Embed Size (px)
Citation preview

CASE ANALYSIS:
Chronic Tympanomastoid
itis
Submitted by:
Terry Mae L. Sarcia
Group 3
BSN-4B1

Chronic Tympanomastoiditis
Chronic suppurative otitis media or CSOM is a condition where there is persistent inflammation of the middle ear. It is even known as chronic tympanomastoiditis and chronic mastoiditis. It’s characterized by burning pain in ear accompanied by persistent discharge (otorrhoea) from the earwhich may continue for a period of about 2-6 weeks. If the middle ear gets infected it builds uppressure behind eardrum or tympanic membrane which leads to severe earache. The discharge is due to perforation of tympanic membrane (eardrum).
A type of otitis media can also occur without tympanic perforation when middle ear gets filled with fluid without any infection. Acute CSOM is mainly a result of some bacterial, viral or fungal infection which may enter the ear from throat, leading to pus formation in middle ear. It can also be accompanied by severe bleeding. Acute infection causes inflammation and irritation in mucosa of middle ear which generates mucosal ulcerations and breaks down epithelial lining. This disease may even result in hearing loss of varied severity. Usually children under the age of seven are most prone to this disease.

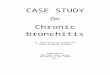
PHYSIOLOGY OF HEARING
The first step is when the pinna collects external sounds that enter through the meatus or ear canal as sound waves. The ear drum begins to vibrate as these sound waves strikes. These vibrations pass through to the three ossicles of the middle ear (hammer, anvil and stapes) where they are amplified. As the transmission proceeds, the vibrations first hit the hammer, then the hammer pushes the anvil, and the anvil hits the stapes.
The vibrations are finally interpreted as sound in the brain after being transmitted and transformed into nerve signals by the cochlea (snail shaped component of the inner ear). This is due to the connectivity of the oval window of the inner ear to the edge of the stapes. When the stapes vibrates, they always transmit the sound vibrations to the inner ear.
SOUND->EXTERNAL AUDITORY CANAL->VIBRATION COMMUNICATED BY OSSICLES->MALLEUS->INCUS-> TRANSMITTED THROUGH THE STAPES-.ROCKS INTO->F. VESTIBULI-> STRETCH ACROSS->MIDDLE EAR->PERILYMPH->ENDOLYMPH OF THE INNER EAR AND THEN TRANSMITTE TO NERVE SIGNALS TO THE BRAIN
SYMPTOMSFollowing are some common symptoms which one might experience while suffering from the disease-
Earache Fever Headaches Mild deafness Discharge from that particular ear Loss of appetite Having difficulty in sleeping. Dizziness Nausea and vomiting Sneezing and coughing
CAUSESCSOM might occur due to any of the causes mentioned below-
Infection caused by some viral, fungal or bacterial pathogens. Some infection in the outer ear left untreated thus spreading to the
inner or middle ear.

Blowing nose so hard that Eustachian material is forced into your middle ear.
Having a persistent head cold. Obstruction of Eustachian tube. Improper treatment of acute otitis media.
Discharge Planning
Medication
Economic Status: Instruct patient to avail of free medication and health services of the AFP medical installation/barangay health centers or if not, instruct patient to buy generic drugs
Treatment:: Advise patient to continue the prescribed medications
Discharge Planning
Health Teaching:
1. Encourage patient to practice proper hygiene in order to reduce the risk for further infection.
2. Maintenance of a healthy lifestyle should be stressed.
3. Instruct patient to avoid exposure to loud music, environment or noise.
4. Discuss importance of continuing medications.
Discharge Planning
Outpatient: Advise patient to return for check-ups
Diet:
1. Eat three balanced meals a day.
2. Advise patient to regularly eat fruits.
3. Instruct patient to increase fluid intake.
Spiritual: Encourage patient to strengthen faith by participating in the mass.
Management
Patients with suspected mastoiditis should be managed in a hospital setting.

Appropriate clinical suspicion and prompt diagnosis are important to reduce the likelihood of complications.
The usual initial therapy is high-dose, broad-spectrum intravenous (IV) antibiotics, given for at least 1-2 days (eg with a third-generation cephalosporin).[1]
Oral antibiotics are usually used after this, starting on IV treatment after 48 hours without fever, and continuing for at least 1-2 weeks.
Paracetamol, ibuprofen and other agents may be given as antipyretics and/or painkillers.
Myringotomy ± tympanostomy tube insertion may be performed in some cases as a therapeutic procedure, or to collect middle ear fluid for culture.
Surgical intervention, usually in the form of mastoidectomy ± tympanoplasty, is suggested if there is:[1]
o Mastoid osteitis.o Intracranial extension.o Abscess formation.o Co-existing cholesteatoma.o Limited improvement after IV antibiotics. Mastoidectomy can be:[1]
o Simple: infected mastoid air cells are removed.o Radical: the tympanic membrane and most middle ear structures are
removed and the Eustachian tube is closed.o Modified: the ossicles and part of the tympanic membrane is preserved. Incision and drainage of a subperiosteal abscess in another procedure
that may be required. Patients with intracranial spread may also need neurosurgical
intervention. In cases with unusual infecting organisms, specialist infectious disease
input may be helpful.
Complications
Conductive and/or sensorineural hearing loss. Osteomyelitis or bone erosion. Extension to the zygoma (zygomatic mastoiditis). Subperiosteal abscess (abscess between the periosteum and mastoid
bone; gives appearance of a protruding ear). Cranial nerve palsies (especially V, VI and VII). Intracranial spread leading to extradural abscess, cerebral
abscess, subdural empyemaand meningitis. Intracranial venous sinus thrombosis (eg lateral sinus thrombosis). Bezold's abscess (spread of pus from mastoid process along the digastric
muscle to other neck muscles).[12]
Petrositis causing Gradenigo's syndrome (VIth cranial nerve palsy + deep trigeminal facial pain + suppurative otitis media).

Carotid artery spasm, arteritis, occlusion, rupture or metastatic septic emboli leading to intracerebral infection (all very rare and associated with the most severe cases).