-
8/4/2019 Case 7_Newborn With Respiratory Distress
1/10
Case 7: Newborn with Respiratory Distress
Details of the delivery are always important in assessing a
newborn. In
this case, "fair" glucose control, unknown Group B strep
status,prematurity, and C-section delivery all point to possible
causes of
respiratory distress.
Maternal diabetes is a risk factor for respiratory distress
syndrome andother difficulties. Maternal group B strep infection is
a risk factor forneonatal sepsis. Prematurity predisposes to
respiratory distress
syndrome (RDS) caused by lung immaturity and lack of
surfactant,
but most infants born at 36 weeks' gestational age do not have
RDS.C-section delivery predisposes to transient tachypnea of the
newborn.
Additional risk factors that were NOT present in this case
include
- Premature rupture of membranes 18 hours, a risk factor
forneonatal sepsis
- Meconium in the amniotic fluid, a risk factor for
meconiumaspiration syndrome.
Ms. Mason is taking no medications and has no history of other
druguse. While possible this is unlikely based on the history.
Infants who aspirate meconium in utero or at the time of
deliveryoften present with symptoms of respiratory distress,
including
tachypnea. There was no meconium in the amniotic fluid making
thisan unlikely diagnosis.
Asthma is not a diagnoses in the neonatal period, making
thisdiagnosis unlikely.
Pulmonary embolism is very rare in children and usually is a
resultof a clotting disorder. Pulmonary embolism is only seen in
neonates
who have a predisposing condition such as the placement of a
centralvenous catheter. Adam does not have this risk factor making
this
diagnosis unlikely.
Proceed to the next card and rank the items in the
differential
diagnosis.
The most likely diagnosis for Adam is Transient Tachypnea of
the
Newborn or TTN. Transient tachypnea of the newborn is the result
of
delayed clearance of lung fluid following birth.
Respiratory distress syndrome is the result of
lung-surfactantdeficiency and is the most common cause of
respiratory distress in
premature infants.
Congestive Heart Failure (CHF) in infants is most often caused
by a
congenital heart defect.
Hypothermia should be considered in the differential diagnosis
of a
tachypneic newborn.
Pneumothorax is relatively uncommon, but is always an
importantconsideration in an infant with respiratory distress.
Neonatal sepsis can present initially with tachypnea and
progress tomore severe illness rapidly. Prolonged rupture of the
membranes, not
present in this case, is associated with an increased incidence
of
neonatal sepsis. Neonatal sepsis is often due to Group B Beta
Strep,usually transmitted from the mother during labor. We do not
know
whether the mother was a GBBS carrier. This is an
importantdiagnosis to consider, especially in premature
infants.
-
8/4/2019 Case 7_Newborn With Respiratory Distress
2/10
The Apgar score describes the condition of the newborn
infantimmediately after birth and, when properly applied, is a tool
for
standardized assessment. It provides a mechanism to record
fetal-to-neonatal transition.
The Apgar score alone correlates poorly with the future
neurologicaloutcome of the term infant. This is because the Apgar
score is affected
by gestational age, maternal medications, resuscitation,
andcardiorespiratory and neurologic conditions that may be present
in the
infant. Low Apgar scores at 1 and 5 minutes alone are not
conclusive
markers of an acute intrapartum hypoxic event. Poor
neurologicoutcome is better associated with documented asphyxia,
and that is
why it is important to obtain arterial blood gases to look for
metabolicacidosis. There is a need for health care professionals to
be consistent
in assigning an Apgar score during a resuscitation.
A neonate's birth weight is a good indicator of the health of
the
intrauterine environment. Plotting the weight against
gestational agehelps to identify infants with abnormal growth and
allows the
anticipation of potential problems associated with each
group.
Adam's birth weight is above the 90th percentile for his
presumed 36-week gestational age. If gestational age assessment
confirms that he is
indeed 36 weeks, he would be classified as large for gestational
age(LGA). This is the term used to identify those newborns with
birth
weight above the 90th percentile. Although many LGA infants
are
constitutionally large, the most important pathologic etiology
is
maternal diabetes mellitus. You will need to defer the
gestational ageassessment until his clinical condition stabilizes,
but you must beaware of potential clinical problems associated with
being LGA:
- Large infants often must be delivered by C-section, by
forceps, orvacuum extraction (all of which have associated
complications)
- Birth injuries are more common, such as fractured clavicle,
brachialplexus injury, and facial nerve palsy
- Hypoglycemia is especially common in LGA infants born to
diabeticmothers
Newborns who are appropriate for gestational age (AGA) have
birthweights between the 10th and 90th percentiles.
An infant with low birth weight may be premature, but low
birth
weight may also result from many other causes. Newborns with
birth
weights below the 10th percentile for gestational age are
classified assmall for gestational age (SGA) or intrauterine growth
restricted
(IUGR). The terms SGA and IUGR are both used in the
literature,although the newer literature tends to favor the term
intrauterine
growth restriction (IUGR). The SGA baby has unique
potentialproblems, which may include:
- Temperature instability (hypothermia)- Hypoglycemia because of
inadequate glycogen stores
- Polycythemia and hyperviscosity
-
8/4/2019 Case 7_Newborn With Respiratory Distress
3/10
Persistent pulmonary hypertension of the newborn
Persistent pulmonary hypertension of the newborn (PPHN) is
theresult of elevated pulmonary vascular resistance to the point
that
venous blood is diverted to various degrees through fetal
channels (the
ductus arteriosus and foramen ovale) into the systemic
circulation and
bypasses the lungs, resulting in systemic arterial
hypoxemia.
Link to adiagram illustrating this blood flow.
PPHN can result from several conditions, including
meconiumaspiration syndrome, diaphragmatic hernia, hypoplastic
lungs, and in
utero asphyxia. The following findings may indicate that an
infant has
PPHN:
- Tachypnea
- Tachycardia- Respiratory distress, with findings such as
expiratory grunting andnasal flaring
- Generalized cyanosis
- Low oxygen levels, even while receiving 100% oxygen
All of the tests listed above should be considered in the
evaluation of acyanotic newborn.
Arterial blood gases help in determining the oxygenation,
ventilation,
and acid-base status of the infant. Knowing the pCO2 is very
helpful in
understanding the cause of the cyanosis.
The CBC with differential count is useful to rule out
neutropenia,leukopenia, abnormal immature-to-total-neutrophil
ratio, and
thrombocytopenia as signs of sepsis.
A chest radiograph is an integral part of the initial assessment
of the
newborn with respiratory distress. The size and the shape of the
heartmay yield some clues to the diagnosis. The appearance of the
lungs
may suggest pneumonia, meconium aspiration, RDS, etc.
Normalinspiratory films should have eight or more intercostal
spaces of lung
fields on both sides.
An echocardiogram is the gold standard in the diagnosis of
congenital
cardiac lesions and persistent pulmonary hypertension of the
newborn.An echocardiogram is indicated when there is persistent
cyanosis and
no indication of lung disease, or when there are other signs
suggesting
a heart defect, such as a murmur, an abnormal ECG or a chest
X-rayshowing an abnormal cardiac contour.
An oxygen challenge test (hyperoxia test) is a valuable tool
that can
help differentiate between cardiac and pulmonary etiology in
infantswho are cyanotic. In brief, oxygen will increase the PaO2 of
an infant
whose cyanosis is caused by a respiratory condition, but will
not
significantly increase the PaO2 if a cardiac lesion causes
cyanosis. Thistest is described in some detail in the article by
Sasidharan.
Physical examination is critical to identify heart murmurs
and
respiratory findings that might be the cause of the
cyanosis.
Remember, however, that some murmurs may not be present early
inlife because of the elevated pulmonary vascular pressure.
http://app2.med-u.org/player/app/extern_temp/152409.htmlhttp://app2.med-u.org/player/app/extern_temp/152409.htmlhttp://app2.med-u.org/player/app/extern_temp/152409.html
-
8/4/2019 Case 7_Newborn With Respiratory Distress
4/10
Pulse oximetry detects the oxygen saturation in the blood.
The findings of tachypnea, retractions and grunting are
classicalsymptoms of respiratory distress from any cause.
Intercostal and
subcostal retractions reflect the increased work of breathing
due to
decreased lung compliance, either due to primary lung pathology
oredema. Grunting occurs at the end of expiration, and is the
audiblesound of air being expelled through a partially closed
glottis as the
infant attempts to increase transpulmonary pressures, increase
lung
volumes, and improve gas exchange. For Adams case,
physicalexamination helps rule out some of these possibilities.
Congenital diaphragmatic hernia is a congenital malformation
resulting from a defect in the development of the diaphragm. It
occurs
in 1 out of every 2,200 to 5,000 live births. The most common
type is
the Bochdelek hernia (a posterolateral hernia) that accounts for
themajority (> 95%) of cases. This defect allows the passage of
organsfrom the abdomen into the chest cavity and severely impairs
lung
development. Most defects occur on the left side. Absent
breathsounds or presence of bowel sounds on one side of the chest
are
important diagnostic clues. Adams physical examination with
the
presence of bilateral normal breath sounds makes this
diagnosisunlikely.
Pneumothorax is caused by a collection of gas in the pleural
space
with resultant collapse of lung tissue. Common risk factors
aremechanical ventilation or underlying lung disease
(especiallymeconium aspiration or severe infant respiratory
distress syndrome).
Absence of breath sounds on one side of the chest in combination
withrespiratory distress is an important diagnostic clue. Adams
physical
examination with the presence of bilateral normal breath
sounds
makes this diagnosis unlikely.
Transposition of the Great Arteries (TGA) is a congenital
heartdefect in which the aorta and pulmonary arteries are
transposed
resulting in respiratory distress and severe cyanosis at shortly
afterbirth as the patent ductus arteriosus closes. One risk factor
for
transposition of the great arteries is being born to a diabetic
mother.
TGA is often associated with other congenital heart defects such
as a
VSD so a murmur may be heard on physical examination.
Adamsnormal cardiovascular examination and absence of cyanosis
makesthis diagnosis unlikely.
Hypothermia can cause tachypnea and may be associated
withneonatal sepsis. Small for gestational age and premature
infants are at
increased risk to develop hypothermia. Adams temperature is
normaland he is an LGA infant making this diagnosis unlikely.
Severe Coarctation of the Aorta may cause respiratory distress
if
there is severe left ventricular outflow tract obstruction.
Classically,diminished pulses in the lower extremities or
asymmetric bloodpressure readings suggest the diagnosis. In
severely ill neonates, there
may be no differences in the pulses because cardiac output is so
poor.
Adams general appearance and normal pulses in all
extremitiesargues against this diagnosis.
Transient tachypnea of the newborn (TTN) - Because Adam islarge
for gestational age, was born by C-section, and his clinical
picture does not fit the other diagnoses well, TTN is a likely
diagnosis
for his respiratory distress.
Infant Respiratory distress syndrome (RDS) remains a
possibility,
but is less likely than TTN in a 36-week gestation infant. A
chest X-
Ray may help to distinguish between TTN and RDS
-
8/4/2019 Case 7_Newborn With Respiratory Distress
5/10
Hypoglycemia may be seen in infants of diabetic mothers due to
the
chronic hyperinsulinemic state that occurred during
gestation.Hypoglycemia may be more pronounced in premature
infants.
Tachypnea is a non specific response to this metabolic
derangement.
This diagnosis remains a possibility for Adam and could
beinvestigated by a serum glucose reading.
Congestive heart failure is unlikely because Adam has a
normal
cardiovascular system with no murmur, normal pulses and
normaloxygen saturation. This constellation of symptoms rules out
most
major cardiac causes of congestive heart failure.
Neonatal sepsis is unlikely (but not impossible) because Adam
has
normal temperature, blood pressure and perfusion. In addition,
his
mother is well without fever suggesting she does not
havechorioamnionitis.
High levels of maternal serum glucose during pregnancy result
in
hyperglycemia in the fetus. This stimulates the fetal pancreatic
betacells and the development of hyperinsulinemia. Maternal insulin
does
not cross the placenta.
Insulin is the primary anabolic hormone for fetal growth. High
levels
in the third trimester result in increased growth of the
insulin-sensitive
organ systems (heart, liver and muscle) and a general increase
in fatsynthesis and deposition. This combination of increased body
fat,
muscle mass, and organomegaly produces a macrosomic (LGA)infant.
Insulin-insensitive organs, such as the brain and kidneys, are
not affected by the elevated insulin levels, and have
appropriate sizefor gestational age.
Control of diabetes during pregnancy is an important predictor
of fetal
outcome, especially with regard to the risk of birth defects.
The
incidence of major malformations is directly related to the
First-
Trimester HbA1C level: Infants born to women with HbA1C
levels>12 have at least a 12-fold increase in major
malformations.
When discussing medical problems that are evolving, it is
important to
be clear about what you know and what the next steps in the
evaluation will be. It is difficult to balance the need to
reassure parentsand help them understand the potentially serious
causes of their childssymptoms. Each of the above answer represents
a reasonable
approach but each could be improved.
A. This answer attempts to explicitly reassure Ms. Mason and
provides the most likely cause of his symptoms. Including
comments like I am sure he will be fine, may be prematureand in
most cases should be avoided.
B. This answer explains in lay language what is happening to
Adam and outlines the expected course of the disease howeverit
doesnt acknowledge that there is still significant uncertaintyin
the diagnosis. It does outline that careful observation will be
included but doesnt explain that additional testing will need
to
be done. Leaving this out may cause surprise and anxiety in
theparent when the tests are done.
C. This answer outlines the most likely cause and the next steps
inthe plan. It also explains that more tests will be done
because
uncertainty about the diagnosis exists. It isnt clear what
tests
are being done but does outline that additional
communication
will be happening soon.D. This answer is more complete in the
explanation of the
possible conditions that might be causing the symptoms and
how the tests will help management. It isnt clear what
thetimeline will be for reporting back the new information
which
will be important to include to help Ms. Mason know what to
expect.
-
8/4/2019 Case 7_Newborn With Respiratory Distress
6/10
None of the answers outlined what additional signs would
beworrisome and how Ms. Mason could help watch for them.
Demystifying exactly what you will be monitoring to know if Adam
isimproving will be simultaneously reassuring and will enlist the
parent
as an active partner in their childs care.
The recommendations for feeding infants with respiratory
distressvary, depending on the physician's experience or the policy
of theneonatal unit. There is no evidence from controlled studies
that
feeding a tachypneic infant by mouth is contraindicated,
although
many physicians are reluctant to try this because they feel that
oralfeedings place the infant under greater stress. Many infants
with
respiratory rates of 60-80 per minute tolerate oral feeds, but
some mayneed nasogastric feeding or IV fluids if respiratory
distress worsens
with feeding. Many infants with respiratory rates of > 80 per
minute
will have difficulty with both oral and nasogastric feedings and
will
often require intravenous fluid support.
The use of a nasogastric feeding tube will avoid use of a
bottle, which
may facilitate Ms. Mason's wish to breastfeed.. (After feeding
from abottle, some babies may get frustrated when they breastfeed
because
the milk does not flow as fast from the breast as from a
bottle.)
Link to the AAP's policy on the benefits of breastfeeding.
See the Expert for links to information about breastfeeding and
HIV
and also about transmission of drugs and other chemicals into
humanmilk.
http://pediatrics.aappublications.org/cgi/content/full/112/5/1196
Glucose is the primary substrate for brain metabolism in the
neonate,and even asymptomatic hypoglycemia may have negative
consequences for long-term neurodevelopment.1,2 The
precisedefinition of hypoglycemia in the neonate has been difficult
to
establish because plasma glucose levels often do not correlate
with
symptoms and long-term outcome. A newborn can be
hypoglycemic
yet be entirely asymptomatic. This is why it is important to
screen allnewborns for glucose level and to monitor closely the
glucose levelsof infants of diabetic mothers.
In utero, glucose crosses the placenta, maintaining the fetal
bloodglucose at approximately two-thirds of maternal levels. At
birth,
separation from the placenta results in a decline in the
infant's glucoselevels over the first 1-2 hours of life. Levels
then increase and stabilize
by 3-4 hours at mean levels of 65-71 mg/dL. The infant of a
diabeticmother has hyperinsulinemia and the glucose level
declines
precipitously at birth. Prompt intervention is required to raise
glucoselevels. Both the definition of hypoglycemia and
identification of athreshold value (below) that signals
intervention is indicated have
been revised.3, 4, 5
Currently, most neonatologists attempt to maintain glucose
levels
between 41-50 mg/dL. Proposed Threshold Values for
initialintervention depend on the clinical situation4:
- Asymptomatic infants and infants at risk for hypoglycemia:
-
8/4/2019 Case 7_Newborn With Respiratory Distress
7/10
The glucometer test is a screening test only, and must not be
used toconfirm hypoglycemia. Glucose oxidase reagent strips are
read by
meter (glucometer) or by eye (Dextrostix, Chemstrip) and
measurewhole blood glucose, which is 10-15% lower than plasma
glucose
levels. These reagent strips are widely used as screening tools
for
hypoglycemia and may also be used for ongoing monitoring of
glucose levels. Any reagent-strip reading of whole blood glucose
40 mg/dL). The frequency of
monitoring will depend on the severity of the hypoglycemia and
may
range from every 30 minutes to every 3 hours prior to feeds. If
theblood glucose is not >40 mg/dL with the first enteral
feeding, most
pediatricians would initiate IV dextrose infusions.
Breast milk is the ideal nutrient for the newborn human. It
provides alower renal solute load than formula, has several
anti-infective and
anti-allergic properties, and fosters mother-infant bonding.
Separationof mother and infant poses a challenge for the
successful
establishment of breastfeeding. This most often happens with the
birth
of a premature infant, or an infant requiring special care, such
as
Adam. Adam's ability to breastfeed will be determined by letting
hismother put him to the breast as soon as possible. If he
cannotsuccessfully breastfeed because of his tachypnea, it will be
important
that Ms. Mason begin pumping her breasts as soon as possible
after
delivery. This will initiate milk production and ensure an
adequatesupply when Adam is able to feed at the breast. In the
meantime,
Adam would be fed expressed breast milk, supplemented with
formulaas needed while breast milk volumes are low in the first
2-48 hours
after birth. Pumping breast milk is also psychologically helpful
formothers at a very stressful time: Breast milk is the single
thing that no
one else can provide for their infants.
A - CBC with differential is appropriate because respiratory
distressmay be caused by sepsis.
D - Serum or plasma glucose level is important to confirm
theglucometer reading.
E - Tachypnea may be the only sign of early sepsis or
pneumonia.
G - Lumbar puncture is part of the evaluation for any newborn
in
whom sepsis or meningitis is suspected. It is important to
rememberthat the very young infant with sepsis and/or meningitis
may have no
localizing signs and only subtle clinical symptoms, such
astemperature instability, lethargy, and poor feeding. See: Heath,
PT,
Yusoff NK, Baker CJ. Neonatal Meningitis.Arch Dis Child Fetal
andNeonatalEd 2003;88(3):173-178.
H - Blood gas or pulse oximetry monitoring should be considered
in
-
8/4/2019 Case 7_Newborn With Respiratory Distress
8/10
this case because of the tachypnea, which can be a manifestation
ofrespiratory distress. Measurement of ABGs is used to assess
oxygenation (PaO2), retention of carbon dioxide (PaCO2), and
acid-base states (pH and HCO3). If respiratory distress is mild,
the infant
pink in color, and the infant is not otherwise at risk, blood
gas
determination is not essential. Other risk factors for hypoxemia
would
include shock, severe sepsis, CNS depression, and perinatal
asphyxia.This infant has none of these risk factors. See:
Brouillette RT,Waxman DH. Evaluation of the Newborn's Blood Gas
Status. Clinical
Chemistry 1997;43(1):215-221.
I - Chest X-ray is important because of the tachypnea and
respiratory
distress.
Other laboratory tests are not indicated at this time:
B & C - Determination of serum electrolytes and calcium is
notrecommended early after birth because the newborn's levels
reflect the
mother's status as well as the effect of medications
administered to themother during labor. Results at age 12-24 hours
are more indicative of
the infant's status.
F - A urine culture in the early neonatal period (birth to 3
days old) is
of little value. It may be more useful for an infant 4 days or
older whois suspected of having late-onset sepsis.
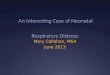
The CXR findings are typical of TTN, with "wet" looking lungs,
no
consolidation, and no air bronchograms (which would
indicaterespiratory distress syndrome). There is no evidence for
a
diaphragmatic hernia. A repeat chest X-ray will not be needed as
longas Adam shows continued clinical improvement.
X-ray findings similar to those on Adam's films may also be seen
withneonatal pneumonia, but this diagnosis is unlikely in the
absence of
other clinical signs of sepsis. If respiratory symptoms do not
improve,
a repeat chest X-ray should be ordered and intravenous
antibioticsshould be initiated.
TEN
An infant with respiratory distress syndrome (RDS) would
have
radiographic findings that typically include a diffuse
reticulogranularappearance of the lung fields ("ground glass
appearance") and air
bronchograms. Link to an X-ray showing a newborn
withrespiratorydistress syndrome.
http://app2.med-u.org/player/app/extern_temp/152112.htmlhttp://app2.med-u.org/player/app/extern_temp/152112.htmlhttp://app2.med-u.org/player/app/extern_temp/152112.htmlhttp://app2.med-u.org/player/app/extern_temp/152112.htmlhttp://app2.med-u.org/player/app/extern_temp/152112.html
-
8/4/2019 Case 7_Newborn With Respiratory Distress
9/10
Diaphragmatic hernia most commonly develops on the left side.
Aradiograph shows air-filled loops of bowel in the left side of the
chest,
displacing the heart and mediastinum to the contralateral side.
Link toan X-ray of a newborn with adiaphragmatic hernia.
Developmental Dysplasia of the Hip (DDH) is the current term for
the
condition previously known as Congenital Dislocation of the Hip.
It isnow recognized that dislocation of the hips is a developmental
process
that is not always detectable at birth. In spite of newborn
screeningprograms we continue to see dislocated hips being
diagnosed later in
infancy.
Clinical features of DDH include partial or complete dislocation
orinstability of the femoral head.
Risk factors for DDH include:- Breech position: 30-50% occur in
infants born in the breech position.
- Gender: 9:1 female predominance.
- Family history.
With the goal of decreasing the number of dislocated hips
detectedlater in infancy, the American Academy of Pediatrics has
developed a
Clinical Practice Guideline for primary care providers. The
maincomponents of this guideline are the recognition of risk
factors and
regular hip examinations up to age 18 months. Linkto the
AAPguideline.
All of these factors are important in planning the discharge
of
newborns from the hospital. It is important that the parents
beprepared for the discharge, and that appropriate follow-up is
arrangedin the first week after birth. Any infant discharged from
the nursery
before 48 hours of life must be evaluated by a health care
practitioner
within 48 hours. See the references below for AAP policy
guidelineson hospital discharge, safe transportation of newborns,
breast feeding,
sleeping position and SIDS, and vitamin D supplementation.
The breastfed infant will typically feed on demand every 2-4
hours,feeding 10-15 minutes on each side. Ms. Mason should contact
the
pediatrician if Adam does not have at least 6 wet diapers per
day. Sheshould also observe for development of jaundice over the
next severaldays and contact the physician if it does appear.
The American Academy of Pediatrics recommends that
exclusively
breastfed infants receive a daily dose of 200 IU of Vitamin D,
because
human milk does not provide adequate intake if it is the sole
source ofnutrition. This supplementation should continue until the
infant is
weaned to a formula containing vitamin D. Standard formulas
allcontain at last 400 IU of vitamin D and meet the infant's
needs.
All infants must be transported in a car seat, following the
guidelines
in the AAP SAFE Ride Program/Family shopping guide to car
seats.
The Back to Sleep program has resulted in a significant decrease
in the
incidence of Sudden Infant Death Syndrome. Ensure that parents
areaware of the guidelines. Co-bedding of an infant with an
adult
increases the risk of death by suffocation should the adult
accidentally
roll onto the infant. The AAP recommends that infants not bed
shareduring sleep. Infants may be brought into bed for nursing
or
http://app2.med-u.org/player/app/extern_temp/152114.htmlhttp://app2.med-u.org/player/app/extern_temp/152114.htmlhttp://aappolicy.aappublications.org/cgi/content/full/pediatrics;105/4/896http://app2.med-u.org/player/app/extern_temp/152114.htmlhttp://aappolicy.aappublications.org/cgi/content/full/pediatrics;105/4/896
-
8/4/2019 Case 7_Newborn With Respiratory Distress
10/10
comforting but should be returned to their own bassinet or crib
whenthe parent is ready to return to sleep. The infant should not
be brought
into bed when the parent is excessively tired or using
medications orsubstances that could impair his or her alertness.
The task force
recommends that the infants bassinet or crib be placed in the
parents
bedroom, which will allow for convenient breastfeeding and
contact.
Infants also should not bed share with other children.