Embed Size (px)
DESCRIPTION
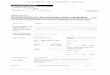
Case 17. * Female, 6 years old. * Annular lesions in both legs from one month. * High erythrocyte sedimentation rate (54 mm). * Reactive C protein: 80 mg/L. * Rheumatoid factor: 21.4 IU/mL. CD4. CD8. Ki67. Case 17 Diagnosis: ?. Case 17 - PowerPoint PPT Presentation
Citation preview

Case 17Case 17

* Female, 6 years old.
* Annular lesions in both legs from one month.

* High erythrocyte sedimentation rate (54 mm).
* Reactive C protein: 80 mg/L.
* Rheumatoid factor: 21.4 IU/mL.











CD4

CD8

Ki67


Case 17Case 17
Diagnosis: ?

Case 17Case 17
Diagnosis: lipoatrophic panniculitis of the ankles in childhood.

1) Gilchrist T.C. et al. John Hopkins Hosp Bull 1916;27:291-294.2) Makai E. Klin Wochenschr 1928;7:2343-2346.3) Cummins L.J. et al. Arch Dermatol Syphil 1938;38:415-426.4) Pinetti P. G Ital Dermatol Siffilo 1941:82:297-340.5) Larkin V de P et al. Am J Dis Child 1944;67:120-125.6) Duperrat B. Med Infant (Paris) 1960;2:5-8.7) Fournier A. et al. Pediatrie 1965;20:595-600.8) Témime P. et al. Bull Soc Franc Dermatol Syphiligr 1968;75:206-207.9) Undeutsch et al. Hautarzt 1970;21:221-225.10) Shelley et al. Arch Dermatol 1970;102:326-329. *11) Stanoeva L. et al. Dermatologica 1972;145:48-55.12) Jablonska S. et al. Acta Derm Venereol 1975;55:135-140.13) Nowińska-Lebiosa H. et al. Przagl Dermatol 1977;64:579-482.14) Taylor G.A. Clin Pediatr (Phila) 1981;20:521-523.15) Edge J. et al. Eur J Pediatr 1986;145:227-229.16) Nelson H.M. Clin Exp Dermatol 1988;13:111-113.17) Moragon M. et al. Eur J Pediatr 1986;145:227-229.18) Winkelmann R.K. J Am Acad Dermatol 1989;21:971-978.19) Roth et al. J Am Acad Dermatol 1989;21:1152-1156.20) Melchiorre L.P. et al. J Rheumatol 2000;27:504-506.21) Martinez A. et al. Br J Dermatol 2000;142:1034-1039.22) Masala M.V. Dermatology 2001;203:81-82.23) Falcini F. et al. Clin Exp Rheumatol 2002;20:432.24) Mirza B. et al. Australas J Dermatol 2006;47:49-52.25) Madasseri A. et al. Clin Exp Dermatol 2006;31:303-305.26) Dimson O.G. et al. J Am Acad Dermatol 2006;54:S40-S42.27) Shen et al. Arch Dermatol 2010;146:877-881.28) Kerns M.J. et al. Pediatr Dermatol 2011;28:142-145. 29) Corredera et al. Pediatr Dermatol 2011;28:146-148.30) Santonja et al. Am J Dermatopathol 2012;34:295-300.31) Fernandez-Flores et al. Am J Dermatopathol 2012: Epub ehead of print.
Reports of localized lipoatrophy invoving the ankles Reports of localized lipoatrophy invoving the ankles and lower legsand lower legs

•Annular lipoatrophy of the ankles•Lipoatrophic and lipophagic panniculitis of childhood•Connective tissue panniculitis•Cytophagic panniculitis•Lipoatrophy annularis

Lipoatrophic panniculitis: after inflammation.
Contrary to lipodystrophy: no previous inflammation
First concept: lipoatrophyFirst concept: lipoatrophy

• Extense variants:• Congenital total.• Acquired total.• Cephalothoracic.• Parcial face-sparing.
• Localized:• Semicircular atrophy of the thighs.• Centrifugalis abdominalis infantilis.
• Annular lipoatrophy of the ankles..
Second concept: localizedSecond concept: localized

Third concept: etiology?Third concept: etiology?
• Previous infections
• Connective tissue disease
Many of these patients have had a history of autoimmune antibodies and autoimmune diseases, such as diabetes and thyroid diseases.

The entity has a well defined clinical The entity has a well defined clinical presentation:presentation:- Recurrent crops of eythematous nodules or plaques involving mainly the legs, especially the ankles but also sometimes accompanying lesions in the arms.
- They develop lipoatrophy.
- Associated laboratory findings:
Elevated ESR.Thrombocytosis.Microcytic anemia.

The entity has a well defined morphology:The entity has a well defined morphology:
- Lobular panniculitis.- Predominance of histiocytes, many of them foamy, including Touton-like lipophages.- Some lymphocytes, neutrophils, plasma cells and eosinophils.
- No necrosis.- No vasculitis.- No mucin

Shelley et al. Arch Dermatol 1970;102:326-329.
“One year after the lesions were initially evidenced, they had become atrophic, with an increase in the venous pattern and hair growth.”
CuriosityCuriosity

ImmunohistochemistryImmunohistochemistry
Umbert I.J. and Winkelmann R.K. Br J Dermatol 1991;124:291-295:
- CD3+. CD4+ (30-40%) with some CD8+.
Martinez A. et al. Br J Dermatol 2000;142:1034-1039:
- Predominance of CD3 lymphocytes.
Santonja et al. Am J Dermatopathol 2012;34:295-300:
- CD4/CD8 even.- High proliferative activity with MIB-1 (early stage?)
(This case also presented lymphocytic rimming)
Fernandez-Flores et al. Am J Dermatopathol 2013;35:524-526.
- Low proliferation rate (MIB-1 10%).- CD4/CD8:70/30%.- No loss of CD2, CD7, CD5.- Groups of PD-1 + cells.