Embed Size (px)
Citation preview

Carti lage Grafting inNasal Reconstruction
Sara Immerman, MDa, W. Matthew White, MDb,Minas Constantinides, MDb,*KEYWORDS
� Cartilage grafting � Nasal reconstruction � Composite grafts� Cutaneous malignancy
Oneof themostcommon locations for skincancer isthenose; theunique3-Dstructureof thenoseposesa challenge for reconstruction. Nasal defects afterresections of cutaneous malignancies arefrequently disfiguring and distressing to patients.Without proper reconstruction, it is nearly impos-sible to hide these aesthetic and functional defor-mities. The goals of nasal reconstruction aretwofold. First, the surgeon must restore the func-tional and breathing capacity of the nose andmain-tain or regain the structural integrity of the defectsite.Second, thesurgeonmust strive foranaesthet-ically pleasing result that is in harmony with rest ofthe face in terms of texture, color, and form.
The nose may be divided into layers for thepurpose of planning reconstruction: (1) cover(skin, subcutaneous tissue, and muscle); (2) struc-ture (upper and lower lateral cartilages, septum,nasal bones, and tip-supporting mechanisms);and (3) internal lining (vestibular skin and nasalmucosa). This article focuses on reconstructionof oncologic defects involving the nasal coveringand structure, emphasizing the use of cartilagegrafting in such repair.
Critical analysis of a defect should precedereconstruction of any wound. The defect’s size,including depth, and location have an impact onnasal function. When the depth is such that nativestructural support has been removed, the defectuniformly requires reconstruction with compositeor cartilaginous grafting. During the analysis stage,the location of the defect is also of utmost impor-tance. The alar rim is one of the free margins that
a Department of Otolaryngology, New York UniversityYork, NY 10016, USAb Division of Facial Plastic and Reconstructive Surgery, DSchool of Medicine, 530 First Avenue, Skirball Institute,* Corresponding author.E-mail address: [email protected]
Facial Plast Surg Clin N Am 19 (2011) 175–182doi:10.1016/j.fsc.2010.10.0061064-7406/11/$ e see front matter � 2011 Elsevier Inc. Al
represent an immobile landmark. Normal woundhealing and contracture tend to pull the alar rimup and create a notch deformity; thus, appropriateplanning is necessary.
The patient’s age, general health, and aestheticgoals must be included in the decision-makingprocess. A thorough medical history, includingprior skin cancer, nasal surgery, and head andneck irradiation, should be completed. Both headand neck irradiation and intervening scars maycompromise skin flap vascularity. The use oftobacco products cannot be overlooked becauseit increases the risk of skin flap and graft failure.Although the mechanism of the harmful effects ismultifactorial, the nicotine causes vasoconstric-tion of cutaneous blood vessels with resultantdecreased tissue oxygenation.1
After resection ofmalignancy, often large defectsare left where the structural integrity of the nose hasbeendisrupted toget adequatemargins. In casesofskin, soft tissue, and cartilage losses, the recon-struction requires a graft that restores the forcesof the nasal infrastructure but also withstands thesubstantial mass of soft tissue that may betransferred.
Grafting materials may be categorized as autog-enous tissue, alloplasts, and homografts. Thesenior author Constantinides, favors the use ofautogenous materials for nasal reconstruction.Autogenous material is advantageous for severalreasons1: it has superior long-term survival,2 isreadily available in the head and neck region, andhas flexibility when inside the nose.3 It has proved
School of Medicine, 550 First Avenue, NB-5EV, New
epartment of Otolaryngology, New York University7, 7U, New York, NY 10016, USA
l rights reserved. facialplastic.theclinics.com

Immerman et al176
a safe, effective, and reliable grafting material thatdoesnotstimulate an immune response.Asa result,autogenous grafts have low rates of extrusion.Autogenous tissue can cause donor site morbidity,however, and potentially resorb over time.2,3
Although most commonly seen with rib grafts,warping remains the most feared complicationwhen using any autogenous graft.4,5 Situationsarise, however, when harvesting such tissue maybe deleterious to a patient or is not in sufficientquantity to correct a given defect. Under thesecircumstances, homografts are a viable alternative.Alloplastic materials also have been used withvarying success to augment the nose and serve asa secondary, less acceptable alternative toautografts.6
There have been many reconstructive methodsdescribed to restore nasal defects after skin tumorexcision, including primary repair, healing bysecondary intention, skin grafts (split and full thick-ness), local flaps, composite grafts, free cartilagegrafts, and microvascular free flaps.7,8 Split-thickness and full-thickness skin grafts can beapplied in cases where the defects are superficial,but often the defect left by removal of the tumor istoo deep to achieve satisfactory results.7 Localskin flaps serve as another reconstructive optionfor coverage of a defect of the nose. Not only arethey associated with surgical ease and shorteroperating time but also they match the color andtexture of nasal skin.9 Donor sites for local flapsfor facial skin defects usually provide the bestoption for reconstruction. Potential drawbacks,however, include additional facial scars, whichmay be difficult to camouflage, and the possibilityof additional procedures (two stages of repair). Inaddition, dog-ears or a trapdoor phenomenoncan result from local flaps requiring a secondprocedure to create a desired outcome.9,10 Micro-vascular free flap reconstruction requires addi-tional training and expertise, long operative time,and substantial effort. Discussion of this type ofreconstruction is beyond the scope of this article.
FREE CARTILAGE GRAFTS
Free cartilage to reconstruct the nose after tumorremoval can be harvested from the septum,concha, or rib. Thesecartilagegraftswith their over-lying perichondrium can provide valuable structuralsupport that may have been lost after tumorremoval. Structural grafting is necessary for tworeasons. First, it is needed to provide rigidity to thesidewall or dorsum, thus preventing collapse andnasal obstruction. Secondly, it creates or maintainsform, especially along the alar rim and tip. Septumand rib grafts are hyaline cartilage, which is strong
and stiff yet pliable, and thus can be carved toprovide rigid scaffolding for reconstruction.
Septum
Septal cartilage is the graft of choice for recon-structive rhinoplasty surgeons. It is easily acces-sible during surgery without the morbidity of anadditional donor site. It is a relatively straightstiff graft that is more robust than auricular carti-lage so is easier to carve and shape precisely.After tumor removal, the straight septal cartilageis ideally used for the middle vault and the nasalsidewall areas. It can also be used, however, fornasal tip grafting, strut grafts, batten grafts,lateral crural grafts, spreader grafts, shield tipgrafts, and buttress grafts.11 Thus, septal carti-lage is versatile and valuable for reconstructivesurgeons. The thin nature of the quadrangularplate means that stacking of septal grafts maybe needed to recreate enough volume; however,the septal cartilage thickens posteriorly. Unlikemany investigators, the authors have foundthat septal cartilage is ideal for all areas ofreconstruction, including the tip and alae (Figs.1 and 2). Although it is flat, its strength andresiliency can lend great advantage to restoringvarious missing components of the tip.Discussion of the technique for septoplasty
harvest is beyond the scope of this article, butregardless of the approach, the amount ofseptal cartilage to be removed should bedictated by the amount of cartilage requiredfor surgery. It should be remembered that least1.5 cm of both dorsal and caudal septal carti-lage struts should remain in place to adequatelysupport the nose. If more cartilage is neededthan can be safely obtained from the nasalseptum, alternative sources of autologenousdonor cartilage are sought.
Auricular Cartilage Grafts
Auricular cartilage is readily available and can beharvested easily with minimal cosmetic deformity.It gives good support but, despite its similar thick-ness compared with the upper and lower cartilagesof the nose, it is softer and more pliable than septalcartilage.11,12 Like septal cartilage, auricular carti-lage is versatile.13 It can be used as a substitutefor septal cartilage when the septum has been har-vested previously. Due to its more brittle nature,however, it can be more difficult to sculpt thanseptal cartilage.11 This is especially true in olderpatients, so extra care should be taken during har-vesting and subsequent manipulation.Conchal grafts can be used as a single layer
implant or sutured together to increase girth and
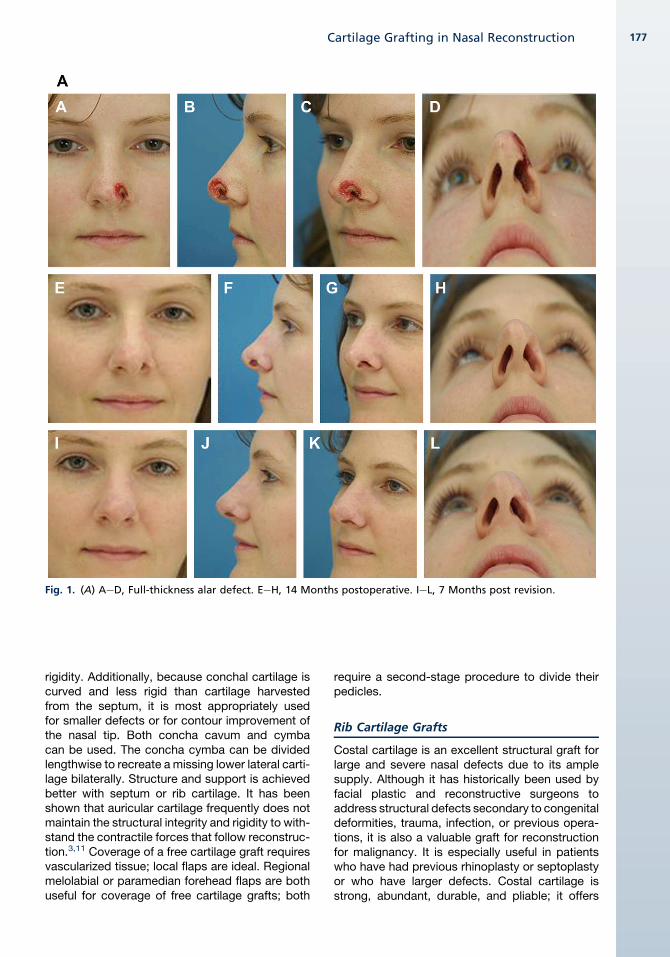
Fig. 1. (A) AeD, Full-thickness alar defect. EeH, 14 Months postoperative. IeL, 7 Months post revision.
Cartilage Grafting in Nasal Reconstruction 177
rigidity. Additionally, because conchal cartilage iscurved and less rigid than cartilage harvestedfrom the septum, it is most appropriately usedfor smaller defects or for contour improvement ofthe nasal tip. Both concha cavum and cymbacan be used. The concha cymba can be dividedlengthwise to recreate a missing lower lateral carti-lage bilaterally. Structure and support is achievedbetter with septum or rib cartilage. It has beenshown that auricular cartilage frequently does notmaintain the structural integrity and rigidity to with-stand the contractile forces that follow reconstruc-tion.3,11 Coverage of a free cartilage graft requiresvascularized tissue; local flaps are ideal. Regionalmelolabial or paramedian forehead flaps are bothuseful for coverage of free cartilage grafts; both
require a second-stage procedure to divide theirpedicles.
Rib Cartilage Grafts
Costal cartilage is an excellent structural graft forlarge and severe nasal defects due to its amplesupply. Although it has historically been used byfacial plastic and reconstructive surgeons toaddress structural defects secondary to congenitaldeformities, trauma, infection, or previous opera-tions, it is also a valuable graft for reconstructionfor malignancy. It is especially useful in patientswho have had previous rhinoplasty or septoplastyor who have larger defects. Costal cartilage isstrong, abundant, durable, and pliable; it offers
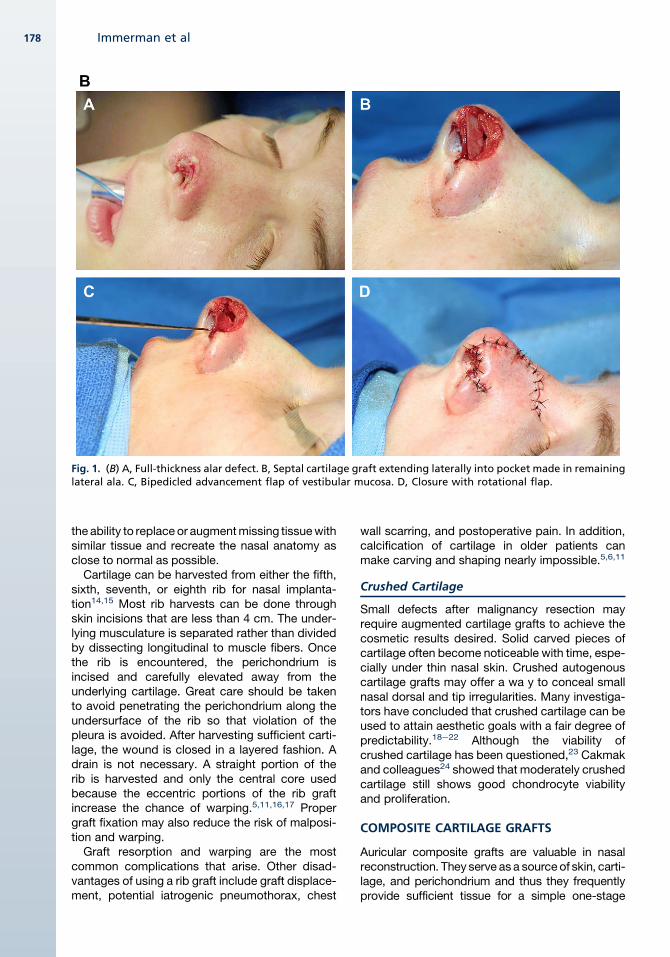
Fig. 1. (B) A, Full-thickness alar defect. B, Septal cartilage graft extending laterally into pocket made in remaininglateral ala. C, Bipedicled advancement flap of vestibular mucosa. D, Closure with rotational flap.
Immerman et al178
the ability to replace or augmentmissing tissuewithsimilar tissue and recreate the nasal anatomy asclose to normal as possible.Cartilage can be harvested from either the fifth,
sixth, seventh, or eighth rib for nasal implanta-tion14,15 Most rib harvests can be done throughskin incisions that are less than 4 cm. The under-lying musculature is separated rather than dividedby dissecting longitudinal to muscle fibers. Oncethe rib is encountered, the perichondrium isincised and carefully elevated away from theunderlying cartilage. Great care should be takento avoid penetrating the perichondrium along theundersurface of the rib so that violation of thepleura is avoided. After harvesting sufficient carti-lage, the wound is closed in a layered fashion. Adrain is not necessary. A straight portion of therib is harvested and only the central core usedbecause the eccentric portions of the rib graftincrease the chance of warping.5,11,16,17 Propergraft fixation may also reduce the risk of malposi-tion and warping.Graft resorption and warping are the most
common complications that arise. Other disad-vantages of using a rib graft include graft displace-ment, potential iatrogenic pneumothorax, chest
wall scarring, and postoperative pain. In addition,calcification of cartilage in older patients canmake carving and shaping nearly impossible.5,6,11
Crushed Cartilage
Small defects after malignancy resection mayrequire augmented cartilage grafts to achieve thecosmetic results desired. Solid carved pieces ofcartilage often become noticeable with time, espe-cially under thin nasal skin. Crushed autogenouscartilage grafts may offer a wa y to conceal smallnasal dorsal and tip irregularities. Many investiga-tors have concluded that crushed cartilage can beused to attain aesthetic goals with a fair degree ofpredictability.18e22 Although the viability ofcrushed cartilage has been questioned,23 Cakmakand colleagues24 showed that moderately crushedcartilage still shows good chondrocyte viabilityand proliferation.
COMPOSITE CARTILAGE GRAFTS
Auricular composite grafts are valuable in nasalreconstruction. They serve as a source of skin, carti-lage, and perichondrium and thus they frequentlyprovide sufficient tissue for a simple one-stage
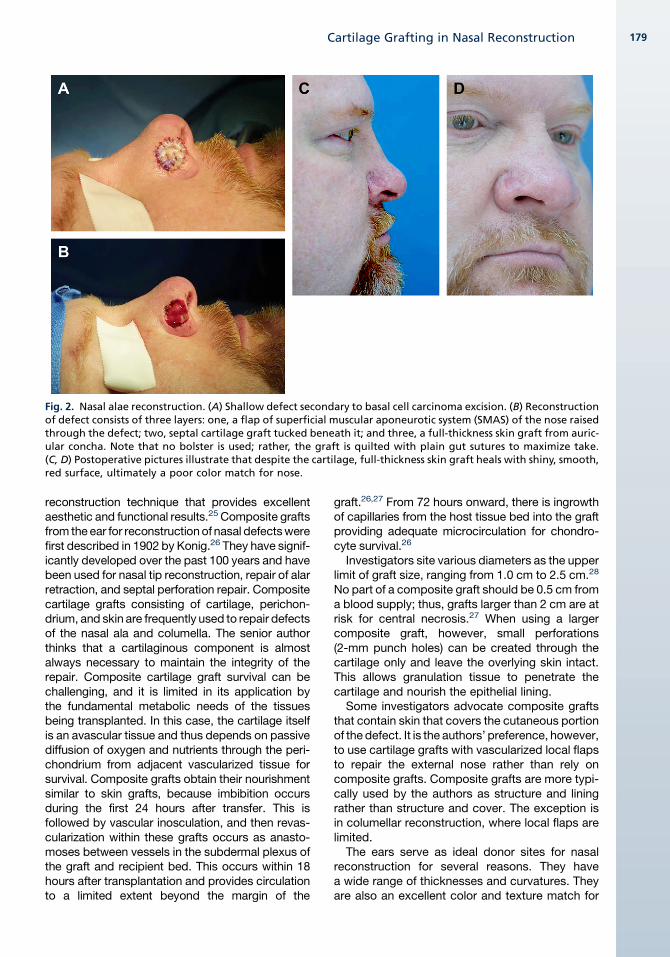
Fig. 2. Nasal alae reconstruction. (A) Shallow defect secondary to basal cell carcinoma excision. (B) Reconstructionof defect consists of three layers: one, a flap of superficial muscular aponeurotic system (SMAS) of the nose raisedthrough the defect; two, septal cartilage graft tucked beneath it; and three, a full-thickness skin graft from auric-ular concha. Note that no bolster is used; rather, the graft is quilted with plain gut sutures to maximize take.(C, D) Postoperative pictures illustrate that despite the cartilage, full-thickness skin graft heals with shiny, smooth,red surface, ultimately a poor color match for nose.
Cartilage Grafting in Nasal Reconstruction 179
reconstruction technique that provides excellentaesthetic and functional results.25 Composite graftsfrom the ear for reconstructionof nasal defectswerefirst described in 1902 by Konig.26 They have signif-icantly developed over the past 100 years and havebeen used for nasal tip reconstruction, repair of alarretraction, and septal perforation repair. Compositecartilage grafts consisting of cartilage, perichon-drium, and skin are frequently used to repair defectsof the nasal ala and columella. The senior authorthinks that a cartilaginous component is almostalways necessary to maintain the integrity of therepair. Composite cartilage graft survival can bechallenging, and it is limited in its application bythe fundamental metabolic needs of the tissuesbeing transplanted. In this case, the cartilage itselfis an avascular tissue and thus depends on passivediffusion of oxygen and nutrients through the peri-chondrium from adjacent vascularized tissue forsurvival. Composite grafts obtain their nourishmentsimilar to skin grafts, because imbibition occursduring the first 24 hours after transfer. This isfollowed by vascular inosculation, and then revas-cularization within these grafts occurs as anasto-moses between vessels in the subdermal plexus ofthe graft and recipient bed. This occurs within 18hours after transplantation and provides circulationto a limited extent beyond the margin of the
graft.26,27 From 72 hours onward, there is ingrowthof capillaries from the host tissue bed into the graftproviding adequate microcirculation for chondro-cyte survival.26
Investigators site various diameters as the upperlimit of graft size, ranging from 1.0 cm to 2.5 cm.28
No part of a composite graft should be 0.5 cm froma blood supply; thus, grafts larger than 2 cm are atrisk for central necrosis.27 When using a largercomposite graft, however, small perforations(2-mm punch holes) can be created through thecartilage only and leave the overlying skin intact.This allows granulation tissue to penetrate thecartilage and nourish the epithelial lining.
Some investigators advocate composite graftsthat contain skin that covers the cutaneous portionof the defect. It is the authors’ preference, however,to use cartilage grafts with vascularized local flapsto repair the external nose rather than rely oncomposite grafts. Composite grafts are more typi-cally used by the authors as structure and liningrather than structure and cover. The exception isin columellar reconstruction, where local flaps arelimited.
The ears serve as ideal donor sites for nasalreconstruction for several reasons. They havea wide range of thicknesses and curvatures. Theyare also an excellent color and texture match for
Immerman et al180
the nose and are readily available. Other advan-tages of auricular composite graft for nasal recon-struction include its ease of harvest, simplicity ofreconstruction, single-stage reconstruction, andavailability for use in elderly patients where pro-longed hospitalization and multiple stages areundesirable and excellent survival of grafts(Fig. 3). Free perichondrium can also be harvestedand be used as a camouflaging graft for thin-skinned patients.
Donor Site Considerations
Grafts may be harvested from different areas ofthe auricle. The helical rim, anterior or posteriorconcha, antihelix, and fossa traingularis can allserve as possible graft sites. The specific locationdepends on the defect size, location, and surgeonpreference. The dorsal concha and root of the helixprovide an excellent source of convex grafts,whereas the ventral concha and fossa triangulariscomposite grafts provide an excellent source ofconcave grafts for the nasal wall or columella.Additionally, the concave surface provides a shapesimilar to the native lower lateral cartilage and canbe helpful in reconstruction of the nasal ala. Thehelical crus can be helpful if a strut graft is neces-sary and is among the strongest cartilaginouscomponents of the ear.
Auricular Defect Reconstruction
Various techniques have been described in theliterature to close the auricular donor site whilemaintaining an aesthetic match of contour and
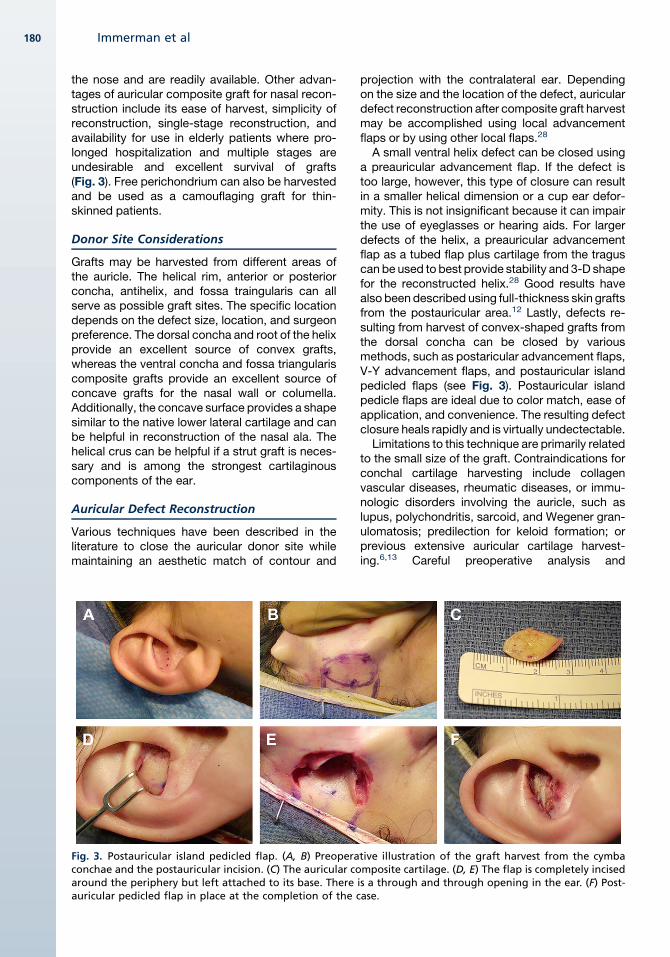
Fig. 3. Postauricular island pedicled flap. (A, B) Preoperaconchae and the postauricular incision. (C) The auricular coaround the periphery but left attached to its base. Thereauricular pedicled flap in place at the completion of the c
projection with the contralateral ear. Dependingon the size and the location of the defect, auriculardefect reconstruction after composite graft harvestmay be accomplished using local advancementflaps or by using other local flaps.28
A small ventral helix defect can be closed usinga preauricular advancement flap. If the defect istoo large, however, this type of closure can resultin a smaller helical dimension or a cup ear defor-mity. This is not insignificant because it can impairthe use of eyeglasses or hearing aids. For largerdefects of the helix, a preauricular advancementflap as a tubed flap plus cartilage from the traguscan be used to best provide stability and 3-D shapefor the reconstructed helix.28 Good results havealso been described using full-thickness skin graftsfrom the postauricular area.12 Lastly, defects re-sulting from harvest of convex-shaped grafts fromthe dorsal concha can be closed by variousmethods, such as postaricular advancement flaps,V-Y advancement flaps, and postauricular islandpedicled flaps (see Fig. 3). Postauricular islandpedicle flaps are ideal due to color match, ease ofapplication, and convenience. The resulting defectclosure heals rapidly and is virtually undectectable.Limitations to this technique are primarily related
to the small size of the graft. Contraindications forconchal cartilage harvesting include collagenvascular diseases, rheumatic diseases, or immu-nologic disorders involving the auricle, such aslupus, polychondritis, sarcoid, and Wegener gran-ulomatosis; predilection for keloid formation; orprevious extensive auricular cartilage harvest-ing.6,13 Careful preoperative analysis and
tive illustration of the graft harvest from the cymbamposite cartilage. (D, E) The flap is completely incisedis a through and through opening in the ear. (F) Post-ase.
Cartilage Grafting in Nasal Reconstruction 181
questioning guide surgeons as to which ear shouldbe used to harvest cartilage. Complete conchalcartilage removal can result in slight medializationof the pinna. Therefore, the more outstanding earshould be harvested. Additionally, if a patient hasa history of sleeping on only one side of the head,the contralateral ear cartilage should be harvested.
POSTOPERATIVE CARE
Postoperative care is important to graft survival. Itis crucial that patients do not participate in phys-ical activity and do not use tobacco products. Inaddition, there is a normal sequence of colorchanges that should be expected by both thesurgeon and the patient as the graft heals. Initially,the graft appears white and then turns pink atapproximately 6 hours, a cyanotic bluish occursby 24 hours, and then areas of pink color progres-sively appear over the next 3 to 7 days. The graftthen turns cherry red color and lastly a normalskin appearance. Preoperative patient educationof this pattern is critical.
MORBIDITY
Recipient and donor site morbidity is rare. Earlyrecipient site complications are bleeding, swelling,
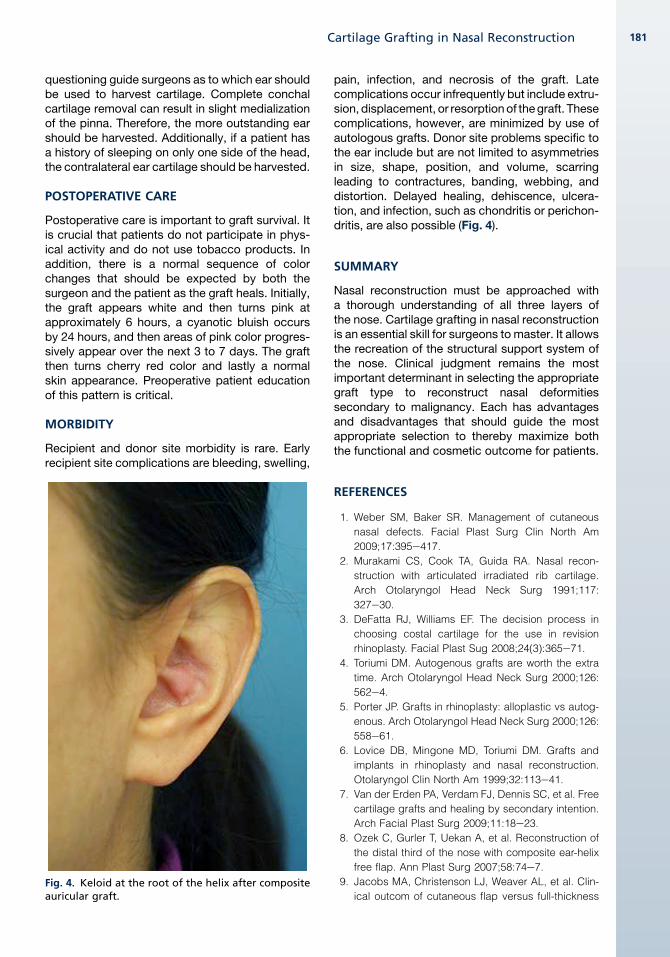
Fig. 4. Keloid at the root of the helix after compositeauricular graft.
pain, infection, and necrosis of the graft. Latecomplications occur infrequently but include extru-sion, displacement, or resorptionof thegraft. Thesecomplications, however, are minimized by use ofautologous grafts. Donor site problems specific tothe ear include but are not limited to asymmetriesin size, shape, position, and volume, scarringleading to contractures, banding, webbing, anddistortion. Delayed healing, dehiscence, ulcera-tion, and infection, such as chondritis or perichon-dritis, are also possible (Fig. 4).
SUMMARY
Nasal reconstruction must be approached witha thorough understanding of all three layers ofthe nose. Cartilage grafting in nasal reconstructionis an essential skill for surgeons to master. It allowsthe recreation of the structural support system ofthe nose. Clinical judgment remains the mostimportant determinant in selecting the appropriategraft type to reconstruct nasal deformitiessecondary to malignancy. Each has advantagesand disadvantages that should guide the mostappropriate selection to thereby maximize boththe functional and cosmetic outcome for patients.
REFERENCES
1. Weber SM, Baker SR. Management of cutaneous
nasal defects. Facial Plast Surg Clin North Am
2009;17:395e417.
2. Murakami CS, Cook TA, Guida RA. Nasal recon-
struction with articulated irradiated rib cartilage.
Arch Otolaryngol Head Neck Surg 1991;117:
327e30.
3. DeFatta RJ, Williams EF. The decision process in
choosing costal cartilage for the use in revision
rhinoplasty. Facial Plast Sug 2008;24(3):365e71.
4. Toriumi DM. Autogenous grafts are worth the extra
time. Arch Otolaryngol Head Neck Surg 2000;126:
562e4.
5. Porter JP. Grafts in rhinoplasty: alloplastic vs autog-
enous. Arch Otolaryngol Head Neck Surg 2000;126:
558e61.
6. Lovice DB, Mingone MD, Toriumi DM. Grafts and
implants in rhinoplasty and nasal reconstruction.
Otolaryngol Clin North Am 1999;32:113e41.
7. Van der Erden PA, Verdam FJ, Dennis SC, et al. Free
cartilage grafts and healing by secondary intention.
Arch Facial Plast Surg 2009;11:18e23.
8. Ozek C, Gurler T, Uekan A, et al. Reconstruction of
the distal third of the nose with composite ear-helix
free flap. Ann Plast Surg 2007;58:74e7.
9. Jacobs MA, Christenson LJ, Weaver AL, et al. Clin-
ical outcom of cutaneous flap versus full-thickness

Immerman et al182
skin grafts after mohs surgery on the nose. Dermatol
Surg 2010;36:23e30.
10. Gurunluoglu R, Shafighi M, Gardetto A, et al.
Composite skin grafts for basal cell carcinomadefects
of the nose. Aesthetic Plast Surg 2003;27:286e92.
11. Sajjadian A, Rubinstein R, Naghshineh N. Current
status of grafts and implants in rhinoplasty: part 1.
Autologous grafts. Plast Reconstr Surg 2010;
125(2):40e9.
12. Giberson WG, Freeman JL. Use of free auricular
composite graft in nasal alar/vestibular reconstruc-
tion. J Otolaryngol 1992;21:153e5.
13. Murrell GL. Auricular cartilage grafts and nasal
surgery. Laryngoscope 2004;114:2092e102.
14. Tessier P, Kawamoto H, Matthews D, et al. Taking
long rib grafts for facial reconstruction- tools and
techniques: III. A 2900-case experience in maxillofa-
cial and craniofacial surgery. Plast Reconstr Surg
2005;116(5):38Se46S.
15. Marin VP, Landecker A, Gunter JP. Harvesting rib
cartilage grafts for secondary rhinoplasty. Plast Re-
constr Surg 2008;121(4):1442e8.
16. Mashaver A, Gantous A. The use of autogenous
costal cartilage graft in septorhinoplasty. Otolaryng-
ol Head Neck Surg 2007;137(6):862e7.
17. Vuyk HD, Adamson PA. Biomaterials in rhinoplasty.
Clin Otolaryngol 1998;23:209e17.
18. Breadon GE, Kern EB, Neel BH. Autografts of un-
crushed and crushed bone and cartilage: experi-
mental observations and clinical implications. Arch
Otolaryngol 1979;105:75e80.
19. Huizing EH. Implantation and transplantation in recon-
structive nasal surgery. Rhinology 1974;12:93e106.
20. Guyuron B, Friedman A. The role of preserved
autogenous cartilage graft in septorhinoplasty. Ann
Plast Surg 1994;32:255e60.
21. Rudderman RH, Guyuron B, Mendelsohn G. The
fate of noncrushed and crushed autogenous carti-
lage in the rabbit model. Ann Plast Surg 1994;32:
250e4.
22. Yilmaz S, Ercocen AR, Can Z, et al. Viability of diced,
crushed cartilage grafts and the effects of surgicel
(oxidized regenerated cellulose) on cartilage grafts.
Plast Reconstr Surg 2001;108:1054e60.
23. Bujia J. Determination of the viability of crushed
cartilage grafts: clinical implications for wound
healing in nasal surgery. Ann Plast Surg 1994;32:
261e5.
24. Cakmak O, Buyuklu F, Yilmaz Z, et al. Viability of
cultured human nasal septum chondrocytes after
crushing. Arch Facial Plast Surg 2005;7:406e9.
25. Singh DJ, Bardett SP. Aesthetic management of the
ear as a donor site. Plast Reconstr Surg 2007;120:
899e908.
26. Maves M, Yessenow R. The use of composite auric-
ular grafts in nasal reconstruction. J Dermatol Surg
Oncol 1988;14:994e9.
27. Adams C, Ratner D. Composite and free cartilage
grafting. Dermatol Clin 2005;23:129e40.
28. Haug MD, Rieger UM, Witt P, et al. Managing the ear
as a donor site for composite graft in nasal recon-
struction. Ann Plast Surg 2009;63:171e5.