Embed Size (px)
Citation preview

924 | CANCER DISCOVERY August 2018 www.aacrjournals.org
REVIEW
CARs versus BiTEs: A Comparison between T Cell–Redirection Strategies for Cancer Treatment Clare Y. Slaney 1 , 2 , Pin Wang 3 , Phillip K. Darcy 1 , 2 , and Michael H. Kershaw 1 , 2
ABSTRACT The redirection of T cells against tumors holds much promise for the treatment of cancer. Two main approaches for T-cell redirection involve their genetic modifi ca-
tion with chimeric antigen receptors (CAR), or the use of recombinant proteins designated bispecifi c T-cell engagers (BiTE). These approaches have demonstrated dramatic effects in patients with hemato-logic cancers, although limited effect against solid cancers. Here, we review and compare the successes and challenges of these two types of immunotherapies, with special focus on their mechanisms, and discuss strategies to improve their effi cacy against cancer.
Signifi cance : CAR and BiTE cancer therapies have generated much excitement, but although the thera-pies are potentially competitive, information directly comparing the two is diffi cult to obtain. Here, we present the fundamentals of each approach and compare the range and level of functions they can elicit from T cells, and their effi cacy against cancers. Cancer Discov; 8(8); 924–34. ©2018 AACR.
1 Cancer Immunology Program, Peter MacCallum Cancer Centre, Melbourne, Victoria, Australia. 2 Sir Peter MacCallum Department of Oncology, Univer-sity of Melbourne, Parkville, Victoria, Australia. 3 National Key Laboratory of Medical Immunology and Institute of Immunology, Second Military Medical University, Shanghai, China. Corresponding Authors: Michael H. Kershaw, Peter MacCallum Cancer Cen-tre, 305 Grattan Street, Melbourne, Victoria 3000, Australia. Phone: 613- 8559-7092; Fax: 613-8559-5039; E-mail: [email protected] ; and Clare Y. Slaney, [email protected] doi: 10.1158/2159-8290.CD-18-0297 ©2018 American Association for Cancer Research.
INTRODUCTION Immunotherapy that utilizes the body’s immune system
against tumors is a promising fi eld of cancer research. In recent years, exciting technologies and platforms have been developed for the intricate design and production of anticancer immune reagents using antibodies in the form of single-chain variable fragments (scFv; Fig. 1 ). The scFv technology has been adopted and used in some promising cancer immunotherapies, includ-ing bispecifi c T-cell engager (BiTE) and chimeric antigen receptor (CAR). Both strategies use scFv to direct cytotoxic T lymphocytes (CTL) to specifi c surface antigens on cancer cells to facilitate a polyclonal T-cell response to tumor antigens.
A BiTE is a recombinant bispecifi c protein that has two linked scFvs from two different antibodies, one targeting a cell-surface molecule on T cells (for example, CD3ε) and the other targeting antigens on the surface of malignant cells. The two scFvs are linked together by a short fl exible linker ( Fig. 1 ). By binding to tumor antigens and T cells simultane-
ously, BiTEs mediate T-cell responses and killing of tumor cells. Importantly, the T-cell/target cell adherence facilitated by BiTE is independent of MHC haplotype ( 1 ).
A variety of formats for bispecifi c antibodies have been developed in addition to BiTEs, including bispecifi c IgG, dia-bodies, and conjugates, which have been the subject of some comprehensive recent reviews ( 2, 3 ). BiTEs have the advan-tages of relatively simple recombinant production and puri-fi cation, and a molecular weight enabling tissue penetration. BiTEs have also advanced through the regulatory framework, gaining FDA approval for certain indications, and will be the focus of this review.
The other area that has a high level of excitement for using scFv technologies is the CAR T-cell approach for adoptive cell transfer. A CAR is a synthetic receptor comprising an extra-cellular tumor antigen recognition domain, which is fused to the CD3ζ chain for intracellular signaling and contains one or more costimulatory domains ( Fig. 2 ). The binding of scFv to tumor cells triggers the T-cell receptor (TCR) intracel-lular domain and leads to T-cell responses against antigen-expressing cells.
Various molecular formats of CAR have been developed, differing in their extracellular, transmembrane, and cytoplas-mic domains, which have been the subject of some previous excellent reviews ( 4 ). In this review, we focus on CARs in which the predominant cytoplasmic signaling domains are derived from CD3ζ and the costimulatory molecules CD28 or CD137, which endow T cells with signifi cant antitumor activ-ity, and which have received FDA approval for the treatment of some hematologic malignancies.
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

CAR T-cell and BiTE Therapies for Cancers REVIEW
August 2018 CANCER DISCOVERY | 925
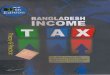
Figure 1. The design of a BiTE. A, Schematic representation of the derivation and structure of a BiTE generated from two antibodies, with specificity for a T-cell activation molecule and a tumor-associated antigen (TAA). B, Schema of a BiTE gene used to produce the recombinant BiTE protein. Linkers were constructed between VH and VL domains of the scFv and between the two scFvs. C, A BiTE creates an immunologic synapse by binding simultane-ously to a tumor cell, via TAA, and a T cell, via CD3.
Light chain
Heavy chain
Variable
Constant
Antigenbinding site
Antigenbinding site
IgG1 IgG2
Linkers
BiTE
scFv
VH VL VH VLLinker Linker Linker
IgG1 scFv IgG2 scFv
A
B
C T cell
CD3
BiTE
Tumor cell
TAA
Anti-CD3 scFv
Anti-TAA scFv
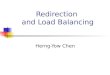
Figure 2. The design of a CAR T cell. A CAR comprises an extracellular domain, which is an scFv targeting TAA. The scFv is followed by a hinge of varying length and flexibility (CD8 as an example) and various combina-tions of endodomains that provide T-cell activation signals, such as CD3ζ, and a costimulation signal, such as CD28. TM, transmembrane.
Extracellular domain (scFv)
Hinge and TM domains CARTCR
Tumor cell
Signaling domains
TAA
Recent advances and positive clinical results from BiTE and CAR T-cell therapies have generated hope and excite-ment. However, both therapies are facing similar dilemmas, such as toxicity concerns in hematologic cancers and a lack of response in solid cancers. In this article, we review and compare the recent progress in the application of BiTE and CAR T-cell therapies, summarize the current understanding of their anticancer mechanisms, and discuss strategies to improve their efficacy against cancers (Table 1).
MECHANISM KEY POINTST-cell Types
T-cell populations are made up predominantly of two cell subsets, expressing either CD4 or CD8. The main function of CD8+ T cells is considered to be cytolysis of tumor cells, whereas CD4+ T cells secrete cytokines to regulate immune responses. In the CAR T-cell approach, CD4+ T cells and CD8+ T cells are usually mixed and genetically modified with CAR and infused back to the patients in clinical trials. Although there is no doubt that CD8+ CAR T cells are the major players in killing cancer cells, CD4+ T cells armed with a CAR can also be activated via CAR and showed cytolytic activities. Although CD4+ CAR T cells eradicated leukemia cells more slowly, these CD4+ CAR T cells persisted longer in vivo (5).
Clinical trials, mixing CAR-equipped CD4+ and CD8+ T cells at a fixed ratio in treating patients, have generated remarkable responses. A study using a defined ratio of CD4+:CD8+ CAR T cells treating refractory B-cell acute lymphoblastic leukemia (B-ALL) achieved bone marrow disease remission in 27 of 29 evaluable patients (6). In that study, 27 patients received a 1:1 ratio of CD4+:CD8+ CAR T cells, whereas 2 patients received alternate ratios. Of the 2 patients receiving alternate ratios, one relapsed and one achieved minimal residual disease. The low patient numbers and intratrial differences in treatment regimens did not allow a statistically meaningful comparison between patients receiving a 1:1 and other ratios. Interest-ingly, a similar approach using a defined mixture of CD4+ and CD8+ CAR T cells in patients with relapsed/refractory B-cell non-Hodgkin lymphoma (NHL) achieved 64% com-plete responses (7). This was comparable with other studies using CAR T cells of variable composition (8, 9), although differences in doses and treatment regimens did not allow a direct comparison of efficacy.
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

Slaney et al.REVIEW
926 | CANCER DISCOVERY August 2018 www.aacrjournals.org
In addition to cell subsets, T cells can exist in several dif-ferentiation states that have different functional abilities. T cells can be classifi ed into naïve T cells (T N ) and four main antigen-experienced or activated subtypes: stem cell memory (T SCM ), central memory (T CM ), effector memory (T EM ), and effector (T EFF ) T cells. It is now evident that less differentiated CAR T cells have better effi cacy in vivo . In CD19-CAR–treated patients with relapsed/refractory B-cell malignancies, the fre-quency of T SCM cells within the transferred lymphocytes cor-related with their in vivo expansion and persistence during the fi rst 6 weeks after infusion ( 10 ). Preclinical studies showed that T SCM cells had greater resistance to cell death caused by repetitive encounter with antigen and had better migration ability to secondary lymphoid organs ( 10 ). It is proposed that T CM are capable of self-renewal and give rise to shorter-lived T EM and T EFF cells that are incapable of self-renewal ( 11 ). Therefore, although T EM and T EFF can be present at high fre-quency at the peak of the anticancer immune response, their persistence is poor. Accordingly, strategies favoring the gen-eration and preservation of T SCM and T CM have been applied in the CAR T-cell therapy fi eld ( 12 ).
Similar to CAR T-cell therapy, BiTE therapies involve poly-clonal T-cell responses, which are independent of MHC and TCR recognition and costimulation. It has been demon-strated that when incubated with BiTEs, both CD8 + and CD4 + T cells can be activated and induce target tumor cell death, with CD8 + cells killing faster than CD4 + T cells ( 13 ). In contrast to CAR T-cell therapy, where less differentiated
T cells showed better effi cacy, in BiTE treatment, antigen-experienced T-cell subsets mediate BiTE-induced tumor cell death, whereas naïve T cells are not activated when engaged by BiTE ( 1 ). In an early study, Bargou and colleagues reported that following injection of the anti-CD19 BiTE blinatu-momab in patients with relapsed and refractory NHL, T cells were redistributed and activated. T cells transiently declined in numbers within 24 to 48 hours, as the T cells adhered to blood vessels endothelium and/or extravasated. T cells then returned to baseline numbers with an activated phenotype, driven by an expansion of CD4 + and CD8 + T EM cells. T-cell lev-els eventually exceeded pretreatment levels, and this increase was due to the expansion of T EM cells, but not naïve T cells ( 14 ). Despite some differences in the optimal cell phenotype for each approach, both therapies mediated tumor cell killing independent of MHC and provide an opportunity to redirect T-cell cytotoxicity to tumor cells.
T-cell Cytotoxicity CAR T cells can induce target tumor cell death through the
formation of synapses, cytokine secretion, perforin/granzyme B release and/or death receptor ligation. Interestingly, CAR-mediated immune synapse formation has been reported to differ from the traditional TCR-induced synapse, in that the CAR-induced synapse has a much smaller actin ring and diffuse distribution of LCK . In addition, the microtubule-organizing center is distant from the immune synapse in comparison with the classic TCR-induced synapse, which is
Table 1. Comparison of CAR T cells and BiTEs
CAR T cell BiTEStructure A synthetic gene construct encoding an scFv against
tumor antigen linked to activation and costimulatory motifs.
A recombinant protein composed of two linked scFvs; one binds to CD3 on T cells and the other to target a tumor antigen on tumor cells.
Effector cell types Engineered CD8 + and CD4 + T cells ( 5 ). Less-differentiated subsets displaying better antitumor activity in vivo (T SCM and T CM ; ref. 10 ).
Endogenous CD8 + and CD4 + T cells ( 13 ). Antigen-experienced T EM but not T N effective ( 14 ).
Immune synapse Atypical ( 15 ). Typical ( 17–19 ).
Serial killing Yes ( 16 ). Yes ( 22 ).
Killing mechanisms Perforin and granzyme B ( 16 ), Fas/Fas-L, or TNF/TNF-R. Perforin and granzyme B ( 17 ).
Traffi cking Active. Traffi cking of CAR T cells involves comprehen-sive interactions between various molecules and cell–cell interactions ( 57 ).
Passive. Biodistribution depends on factors related to rates of diffusion through vascular endothelium, fl uid fl ow rates, and interaction with target.
Toxicity CRS, neurotoxicity, B-cell aplasia ( 31, 49 ). CRS, neurotoxicity, B-cell aplasia ( 62, 64 ).
Clinical applications Pretreatment lymphodepleting regime using cyclophos-phamide and fl udarabine.
Premedicate with acetaminophen and an H1-antihista-mine. One infusion.
No lymphodepletion regime required. Premedi-cate with dexamethasone. Repeat administra-tion necessary, including continuous i.v. infusion regimens.
FDA approval Yescarta was approved to treat adult patients with relapsed/refractory large B-cell lymphoma in 2017.
Kymriah was approved to treat patients up to 25 years of age with refractory/relapsed B-ALL in 2017.
Blinatumomab was approved to treat relapsed/refractory B-ALL in 2014 and 2017.
Other characteristics Individually produced for each patient. “Off the shelf” reagents.
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

CAR T-cell and BiTE Therapies for Cancers REVIEW
August 2018 CANCER DISCOVERY | 927
proximal to the LCK accumulation. The adhesion molecule LFA1 does not accumulate at the synapse, which could result in rapid detachment from the dying tumor cells, thereby enabling CAR T cells to act rapidly (15). In fact, CAR T-cell serial killing (one T cell kills multiple targets) requires a sig-nificantly shorter time than TCR-mediated serial killing of cancer cells (16).
Similar to CAR T cells, it has been reported that, when incubated with BiTEs, both CD8+ and CD4+ T cells could be activated to kill target tumor cells in vitro, via perforin and granzyme B (17), although roles for TNF and FAS do not appear to have been investigated. However, initial studies suggest that differences exist between the synapse formed between T cells and target cells when mediated by BiTEs compared with CARs. The linkage of tumor cells and T cells by BiTE leads to the formation of cytolytic synapses that are similar to the ones formed during regular cytotoxic T-cell recognition (17–19). Once activated, these T cells start to proliferate and also upregulate the expression of activation markers, such as CD69 and CD25 (20). Although the reason for the difference in synapses formed by CARs and BiTEs is not clear, it potentially arises because BiTEs engage the natu-ral CD3 complex, whereas CARs do not.
Both the size and the position of the epitope to the cell surface determine the extent of BiTE-mediated cancer cell killing (21). Activated T cells kill the target cancer cells via triggering apoptosis, as evidenced by caspase 3/7 activation, PARP cleavage, DNA fragmentation, and membrane blebbing (17). Similar to CAR T cells, it has been shown that BiTEs can induce serial killing by T cells, with one T-cell able to kill sev-eral target cells (22). However, unlike CAR-redirected T-cell function, BiTE-redirected function is sensitive to the dose of BiTE administered. Although this may have advantages in tuning the response to avoid an overreaction and potential toxic levels of cytokine, an excess of BiTE may completely coat CD3 and target antigen separately, thereby reducing the opportunity for coengagement of T cells and target cells (23–25).
Although direct cancer cell lysis is seen as the most potent means to reduce cancer burden by T cells, large amounts of cytokines can be secreted by both CAR- and BiTE-redirected means (26). These effector cytokines have the potential to change the tumor microenvironment and induce endog-enous antitumor immunity. This potential was evident in a study that demonstrated the ability of CAR T cell–secreted cytokines to change the recruitment and activation of endog-enous macrophages and create a favorable milieu for antican-cer immune response (27). Interestingly, studies using both BiTEs and CARs suggest that cytokines secreted upon target cell ligation can contribute to lysis of antigen-negative tumor cells in close proximity to the antigen-specific engagement, so-called bystander lysis (28, 29), although this is not always the case for all target antigens (30).
T-cell Numbers and PersistenceThe resolution of malignant disease requires large num-
bers of responding T cells and their continued action over prolonged time periods. In the case of CAR T cells, these requirements are best achieved by expansion in vivo and long-term engraftment following transfer. In some hematologic
malignancies, CAR T cells have been demonstrated to expand up to, or even exceeding, 1,000-fold (31, 32) and to reach greater than 20% of circulating lymphocytes (33). In clini-cal studies targeting CD19 on B-cell malignancies, absolute counts of circulating CAR T cells can vary among patients, but still achieve levels from several thousand per mL of blood up to several hundred thousand per mL (8, 34, 35).
In the case of BiTEs, a large pool of antigen-experienced T cells can be exploited to provide substantial numbers of redi-rected T cells, with less reliance on expansion. Nevertheless, increased numbers of circulating T cells have been demon-strated following BiTE administration, suggesting expansion of the pool of T cells with the potential to respond against tumor cells. Increases of the order of 2- to 4-fold in circulat-ing T cells have been described (14, 36, 37). However, because the number of antigen-experienced T cells (able to respond independently of costimulation) comprises only a propor-tion of total T cells, the actual level of expansion of respond-ing T cells is likely several folds higher than that reflected in increases in total circulating T cells.
The provision of large numbers of tumor-reactive T cells in the solid-tumor setting presents different challenges for the BiTE and CAR T-cell approaches. Whereas extensive expan-sion and prolonged persistence has been demonstrated for CAR T cells in hematologic cancers, little if any expansion of CAR T cells is usually demonstrated when treating solid can-cers (38–40), except for isolated reports of expansion exceed-ing 100-fold (41, 42). CAR T cells directed against blood cancers may receive further costimulatory signals from cancer cells, or other antigen-positive leukocytes, in a microenviron-ment that is less immunosuppressive than that found in solid tumors. This may explain the observed differences in T-cell expansion in liquid cancers compared with solid cancers. Approaches combining CAR T-cell transfer with vaccines, to provide T-cell support away from the tumor microenviron-ment, are being used to enhance CAR T-cell proliferation and persistence in the solid-tumor setting (43, 44).
Because the BiTE approach is potentially less reliant on T-cell expansion, it may be more successful against solid tumors. However, the success of this approach is dependent on the sustained loading of BiTEs on T cells, which may be compromised during the process of penetration of solid tumors.
Differences between the CAR and BiTE approaches also exist when considering tumor recurrence. CAR T cells are able to engraft long-term and provide an ongoing source of tumor-reactive T cells to respond against recurring tumors, even before they become evident. This has been demonstrated in mouse tumor models, in which mice that rejected a primary tumor also rejected a secondary challenge with tumor cells (43). In contrast, without continuous administration of BiTEs, recurrent tumors have the opportunity to grow large before detection, which may render subsequent treatment with BiTEs less effective.
CLINICAL APPLICATIONSCAR T-cell therapies have generated fantastic responses
in B-cell malignancies and revolutionized the field of cancer immunotherapy. CD19 CAR T-cell therapy has been tested in treating different B-cell malignancies, including NHL (7, 45,
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

Slaney et al.REVIEW
928 | CANCER DISCOVERY August 2018 www.aacrjournals.org
46), chronic lymphocytic leukemia (CLL; refs. 47, 48), and ALL (6, 31, 34, 49, 50). In these trials, the relapsed/refractory patients who had limited treatment options were treated with CD19 CAR T cells, and the treatment generated remarkably high rates of complete responses, over 50% in NHL (7, 8, 46), 90% in ALL (6, 49, 50), and over 70% complete response and/or partial response in CLL (48). In 2017, two CD19 CAR T-cell adoptive transfer treatments were approved by the FDA. Yescarta (axi-cabtagene ciloleucel; Kite Pharma) was approved to treat adult patients with relapsed or refractory large B-cell lymphoma. Kymriah (tisagenlecleucel; Novartis) was approved for the treat-ment of patients up to 25 years of age with refractory/relapsed B-ALL. Preconditioning that depletes endogenous lymphocytes is important for CAR T-cell therapy; without this, significant clinical benefit is rarely observed (51).
Given the remarkable initial response rate observed using CAR T cells in some blood cancers, but a significant relapse frequency at present, the question remains as to whether this form of therapy would be best applied as a stand-alone treatment or as a bridge to stem-cell transplantation. The use of CAR T cells as a bridge to transplant has some attractive features including dramatic reduction in disease burden often to undetectable levels, perhaps enabling a subsequent less-intensive conditioning regimen prior to transplant. In the CAR T-cell setting, transplantation following conditioning would have the added benefit of eliminating CAR T cells to allow recovery of normal B cells, because B-cell aplasia can persist long-term in a substantial proportion of patients with leuke-mia/lymphoma achieving complete responses. This is likely to continue to be an important option for clinicians in the treat-ment of hematologic cancers. However, the increased cost of an additional transplant procedure, together with transplant-related toxicities if using allogeneic donors, indicates that with improvements to cell production and efficacy, and controlled gene expression or inclusion of suicide genes for CAR T cells, a stand-alone approach would be an ultimate goal.
Although highly effective against CD19 B-cell malignan-cies, CAR T-cell therapy did not generate the same potent response against other lymphomas/leukemias. In addition, the loss of CD19 expression in patients can limit the CD19-CAR therapeutic benefit. Recently, a few additional CAR targets have been tested. CD22 in treating patients with ALL who are refractory to CD19 CAR T-cell therapy (52), CD20 in indolent B-cell and mantle cell lymphomas (53), B-cell matu-ration antigen (BCMA) in multiple myeloma (54), and Lewis Y in acute myeloid leukemia (AML; ref. 55) have been tested in the clinic and generated encouraging results.
In solid-cancer clinical trials, CAR T cells have not dem-onstrated the same dramatic effect as seen in hematologic cancers. The reasons are believed to be the solid-tumor immu-nosuppressive microenvironment, impaired T-cell trafficking, and the suboptimal phenotype of the infused CAR T cells (11, 56, 57). A number of tumor antigens have been targeted in solid cancers, such as GD2 in neuroblastoma (58), HER2 in glioblastoma and other solid cancers (40, 59), and EGFRvIII in glioblastoma (60). Interestingly, a recent inspiring study reported that CAR T-cell treatment targeting IL13Rα-2 has successfully eradicated a case of glioblastoma, and the com-plete response lasted several months (61). Although some of the trials have observed some response, the overall outcomes
are less satisfactory than the ones used in blood cancers. There is great enthusiasm to improve CAR T-cell treatment efficacy against solid cancers in preclinical research, and this is discussed in the next section.
Similar to CAR T cells, BiTEs have been used in clinical trials targeting a variety of antigens. Blinatumomab was the first clinically tested and FDA-approved BiTE, receiving accelerated approval in 2014 for the treatment of CD19+ Philadelphia chromosome–negative (Ph−) relapsed and refrac-tory B-ALL. In July 2017, the FDA further approved its use to include the treatment of Philadelphia chromosome–positive (Ph+) relapsed or refractory B-ALL.
A phase II trial (ALCANTARA, NCT02000427) enrolled 45 patients with Ph+ relapsed or refractory B-ALL for the blinatumomab treatment. In this trial, 16 patients (36%) achieved complete remission (CR) or CR with partial hematologic recovery, and the median duration of remis-sion was 6.7 months (62). Thus, blinatumomab has led to promising results for patients with Ph+ relapsed/refractory ALL. A recent phase II trial (TOWER, NCT02013167) com-pared blinatumomab with standard-care chemotherapy in 405 patients with Ph− relapsed and refractory B-ALL. Blinatumomab demonstrated a significant improvement in overall survival (OS) and higher rates of hematologic remission than chemotherapy. The median OS was 7.7 months with blinatumomab compared with 4 months with chemotherapy (63).
Apart from ALL, blinatumomab has also shown promise in treating NHL. The initial clinical studies used short infu-sion of blinatumomab and did not show efficacy but did show toxicities such as cytokine release syndrome (CRS) and neurotoxicity (14). Subsequently, lessons were learned from the ALL studies for continuous infusion of blinatumomab. A clinical trial using continuous infusion of blinatumomab 60 μg/m2/day in NHL (4-fold higher than ALL) has proven to be feasible. In this phase I trial, single-agent blinatumomab showed promising activity with an objective response rate of 69% (24/35 patients; ref. 64).
As with CAR T cells, treatment with BiTEs can lead to high initial response rates but a significant relapse rate, and the use of BiTEs in the hematologic setting offers an option as a bridge to transplantation. As with CAR T-cell therapy, dramatic reductions in disease and complete responses are observed in many patients but, in contrast to CAR T cells where T cells persist long-term, BiTEs require continuous administration to provide protection against disease recur-rence. Therefore, hematopoietic stem-cell transplant follow-ing BiTE therapy may be beneficial. Longer-term follow-up of complete responders receiving BiTEs (or CAR T cells) will be informative to determine the feasibility of using T-cell redi-rection as a stand-alone therapy.
Other tumor antigens have also been explored for BiTE therapy. For example, CD3–CD33 (AMG330) BiTE has been constructed to treat patients with relapsed/refractory AML (NCT02715011).
For treating solid tumors, CD3-coupled BiTEs specific for EPCAM (solitomab), CEA, and prostate-specific membrane antigen (PSMA) have all been tested. Limited responses were observed in treating patients with solid tumors, and toxicity was observed. In a trial using solitomab treating different
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

CAR T-cell and BiTE Therapies for Cancers REVIEW
August 2018 CANCER DISCOVERY | 929
solid tumors, transient elevation of liver enzymes and diarrhea as dose-limiting toxicities were observed. This may be due to the targeting of EPCAM to normal tissue in bowel epithelial and bile ducts. The toxicity precluded further dose escalation (65). Although some tumor response was observed, higher doses were limited by toxicity. New targets, such as gpc3 to treat hepatocellular carcinoma, have also been tested (66).
TOXICITIESCAR T-cell therapy can be associated with some toxicities.
The most commonly observed toxicity is CRS, a systemic response due to elevated levels of cytokines. Studies have dem-onstrated that high levels of 24 serum cytokines, such as IL6 and IFNγ in the first months after CAR T-cell infusion, were associated with severe CRS (67). CRS occurs several hours to 14 days after CAR T-cell infusion, and symptoms include fever, fatigue, anorexia, hypotension, tachycardia, and capil-lary leak, which can be life-threatening. It was demonstrated that the patients with highly elevated levels of IL6 are the ones with maximum CAR T-cell activation and proliferation (49). Anti-IL6 receptor antibody (tocilizumab) that blocks IL6 from binding to its receptor can reverse the life-threatening CRS without inhibiting CAR T-cell treatment efficacy (31).
Neurotoxicity, also termed CAR T cell–related encephalopa-thy syndrome (CRES), has also been reported (31, 48, 49). CRES is typically manifested by symptoms of confusion and delirium and occasionally by seizures and cerebral edema (6, 68). The pathogenesis of neurologic toxicity remains unclear, although it has been proposed that CRES could be due to cytokine-mediated endothelial activation and passive diffusion of cytokines into the brain (69) and/or trafficking of T cells into the central nervous system (CNS; ref. 68). Although CD19 CAR T cells were identified in the cerebrospinal fluid (CSF), levels of the transgene in the brain did not correlate with rates of high-grade CRES events (32). CRES is generally reversible using anti-IL6 receptor and/or corticosteroids (68, 69).
B-cell aplasia is also associated with CD19 CAR T-cell therapy, because CD19 is expressed on normal B cells, but injections of immunoglobulin can be used to maintain levels of circulating antibodies (49). Infections with microorganisms can also occur following CAR T-cell transfer, which was largely due to depletion of endogenous leukocytes by precondition-ing regimens (70). Bacterial infections predominated, which included bacteremia and more localized infections to sites including gastrointestinal tissue. Viral and fungal infections were also experienced. These infections are largely manageable using antibiotics, although some fatalities have resulted.
Although leukodepleting preconditioning is not required for BiTE therapy, toxicities after blinatumomab treatment are common, but mostly manageable. The most frequent adverse effects were CRS and neurologic adverse effects including headache, tremor, aphasia, and seizure (62, 64). These effects might be associated with T-cell migration to the CNS or a transient cytokine storm in serum. Currently, the blinatu-momab treatment dosage and administration schedule is based on body weight, and patients are required to be pre-medicated with dexamethasone, to reduce cytokine produc-tion while retaining cytolytic activity (71, 72). In addition, the treatment of blinatumomab also depleted normal B cells and
plasma precursor cells, resulting in substantial hypogamma-globulinemia. This presents risk of infections, which can be reduced by administration of intravenous immunoglobulin.
RESEARCH IN ENHANCING TREATMENT EFFICACY AGAINST SOLID CANCERS
Both BiTE and CAR T-cell treatment strategies have pro-duced remarkable effects in hematologic malignancies; how-ever, the efficacy for both was generally poor against solid cancers. Considerable effort is being invested in enhancing the treatment efficacy against solid cancers.
For CAR T-cell therapy, the hurdles for treating solid can-cers lie in the combination of the immunosuppressive effect of the tumor microenvironment and inefficient penetration of CAR T cells into tumors. The tumor microenvironment is a complex assortment of cell types including malignant cells, fibroblasts, endothelium, and immunoregulatory cells. Regulatory cell types include myeloid-derived suppressor cells (MDSC), M2 macrophages, and regulatory T cells (Treg; ref. 73). Using a preclinical model, Moon and colleagues demon-strated that CAR T cells were able to slow down tumor growth, but did not cause regression. The reason was the rapid loss of functions of CAR T cells when exposed to the tumor microen-vironment in vivo. Diminished functions included reduction in the ability to secrete cytokines, killing ability, and phospho-ERK expression. When CAR T cells were isolated and rested away from the tumor, their hypofunction was reversed (74).
For targeting the suppressive tumor microenvironment, a number of strategies have been tested. For example, using all-trans retinoic acid (75) or GM-CSF neutralization to dis-rupt MDSC function (76), targeting CD123 on macrophages (77), or fibroblast activation protein on cancer-associated fibroblasts (78) inhibiting adenosine 2A receptors (79) and altering metabolic components such as inhibiting protein kinase A activation (80) all demonstrated enhancement of CAR T-cell treatment efficacy in preclinical models of solid tumors. In addition, there has been great interest in using checkpoint inhibitors as adjuvant therapy for CAR T-cell treatment. Blocking a number of checkpoints, such as PD-1 (81) and LAG3 (82), has been shown to enhance CAR T-cell treatment in solid tumors.
Other strategies that have shown promising results include supplying CAR T cells with cytokine support to enhance their activity within the tumor microenvironment (83). Such approaches include inducing the local release of stimulatory cytokines, including IL12 (84), and transducing the IL7 recep-tor into CAR T cells to provide signal 3 for T-cell support (85). Inhibitory cytokines present in the tumor microenviron-ment can also be harnessed to provide support for T cells. In this approach, T cells are genetically modified with chimeric cytokine receptors. For example, chimeric cytokine receptors composed of the extracellular domain of the IL4 receptor fused to the intracellular domain of the IL7 receptor led to activation and proliferation of T cells in the presence of the normally inhibitory cytokine IL4 (86, 87).
To enhance CAR T-cell infiltration to the tumor bed, effort has been made to modify chemokine receptors on CAR T cells to enhance their migration toward tumors. For example, CAR T cells have been modified to express CCR2b, the chemokine
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

Slaney et al.REVIEW
930 | CANCER DISCOVERY August 2018 www.aacrjournals.org
receptor for CCL2 that is highly expressed by the target tumors (88). To facilitate the penetration into tumors, con-struction of CARs targeting VEGFR2 or αvβ3 integrin over-expressed on tumor vasculature has been reported (89, 90).
Similar to CAR T-cell therapy, the efficacy of BiTEs in treat-ing solid tumors in preclinical models is modest. One of the major hurdles for BiTEs is their short half-life in serum. After injection, BiTEs are rapidly catabolized and cleared from the circulation, leading to a short serum half-life of around 2 hours (91). To overcome the limitation, current approaches include attaching BiTEs to heavy-chain fragments or other novel designs to increase the serum life. A number of these methods significantly increased the BiTE circulation time without hampering its binding to the target cells (92).
The other major hurdle for treating solid tumors using BiTE is the density and types of T cells already in the tumor bed. Small-animal PET and fluorescent imaging studies have demonstrated the penetration of BiTE into solid tumors (93). However, the profiles of the T cells already existing in the tumor are difficult to predict, as the intensity, location, phenotype, and activation phenotypes of these T cells vary dramatically among tumors (94). In addition, preexisting T cells in the tumor may already have an exhausted phenotype or may be Tregs. Approaches in increasing T-cell infiltration into tumor tissue and combinational approaches to reverse T-cell exhaustion and targeting the tumor immunosuppres-sive microenvironment warrant further investigation to boost the efficacy of BiTE against solid cancers.
Recent enthusiasm surrounding BiTEs extends toward their production in vivo. One strategy is to produce geneti-cally modified T cells for making BiTE to overcome the limitations of BiTEs’ short half-life and passive biodistribu-tion. Technologies were developed to generate T cells that secrete BiTEs (ENG-T cells) targeting tumor antigens such as EPHA2 (95), CD123 (96), and CD19 (97). These ENG-T cells can recognize tumor cells in an antigen-dependent man-ner in vitro and in vivo, redirecting T cells to the target cancer cells, and have potent antitumor activity in cancer models (95, 96). Importantly, these ENG-T cells expanded in vivo and increased the production of BiTEs after activation, obviating the need for continuous infusion of engager molecules (95). Interestingly, a recent report compared the efficacy of RNA-electroporated ENG-T cells to the RNA-electroporated CAR T cells and concluded that the ENG-T cells showed more efficacy in the NALM6 leukemia model (98).
Another recent promising strategy is to use an oncolytic virus engineered to express a BiTE. Oncolytic viruses have been tested in the clinic and have demonstrated safety and some anticancer effects. Two recent studies engineered an oncolytic adenovi-rus to secrete an EGFR-targeting BiTE. The BiTE-expressing adenovirus induced a strong T-cell response against cancer cells both in vitro and in vivo (99, 100). The use of oncolytic virus in combination with BiTE or the oncolytic virus secreting BiTE is another strategy for changing the tumor microenvironment. Several oncolytic viruses are currently under development, and whether different strains of these viruses are better than others to be engineered to express and secrete BiTE is yet to be inves-tigated. Post–oncolytic virus administration, large numbers of immune cells infiltrated to the tumors, and the addition of BiTE redirects infiltrating T cells against tumors (101).
Strategies for changing the tumor microenvironment may greatly enhance BiTE treatment efficacy in solid cancers. It was reported that tumors upregulated PD-L1 post–BiTE administration (102) and adding anti–PD-L1 to AMG 330 treatment enhanced killing in vitro (103). Other inhibitor molecules to target include galectin 1, which has been docu-mented to be linked with BiTE resistance (104). Enhancing tumor antigen presentation has also been shown to be a good strategy for enhancing BiTE treatment efficacy. Adding the epigenetic modifier drugs panobinostat and azacitidine increased CD33 expression in some cell lines and enhanced AMG 330–induced cytotoxicity (105).
A few studies directly compared the functional efficacy of the two strategies in their antitumor effect (106). In an early study, Stone and colleagues compared the CAR and BiTE treatment antitumor response in vitro using the same antican-cer scFv against a murine fibrosarcoma epitope, 237. Although both strategies enhanced T cell–mediated antitumor effect, CAR T cells were more potent than the BiTE approach against cancers expressing lower levels of antigens (107). In a recent study, Hoseini and colleagues compared a bispecific antibody (specific for both CD3 and GD2), with a CAR that contained the same anti-GD2 scFv (106). Incubating GD2+ target cancer cells with anti-GD2 CAR T cells for 24 hours led to the deple-tion of the CARhi T cells, and, in contrast, in the presence of BC119, the exposure of untransduced T cells to GD2+ target cancer cells did not deplete the T cells. This GD2-specific CAR T-cell depletion severely compromised CAR T-cell cytotoxic-ity in vitro and impaired their in vivo antitumor efficacy. For treating the GD2+ tumors in immunocompromised mice, BC119 with untransduced T cells conferred rapid shrinkage of the established tumors, whereas CAR T cell–treated tumors showed a delayed regression for 2 weeks. The percentage of tumor-infiltrating lymphocytes (TIL) in the BC119 treatment was higher than that in the CAR T-cell treatment. Interest-ingly, the ratio of CD4+ and CD8+ TILs in BC119-treated mice was nearly equal, whereas the TILs in the CAR T cell–treated mice were nearly all CD8+. The number and composition of TILs could partially explain the superior antitumor effect mediated by BiTE over CAR T-cell treatment. It is note worthy that the above study used immunocompromised mice with adoptive transferred T cells, whereas in the clinic, BiTEs are usually administered without adoptive transfer. The TIL pro-files in immunocompetent mice are poorly studied, albeit a few studies demonstrated that BiTE could suppress tumor progression in these mice (108–110).
In the clinic, it is possible that patients refractory to one therapy respond to the other. For example, in a trial run by Maude and colleagues in 2014, 2 patients refractory to bli-natumomab achieved CR after CD19-CAR treatment (49). This suggests that a lack of response to one immunotherapy against the same target may not preclude a successful therapy outcome with another, even with the same target. In addition, there could conceivably be some benefit from using CAR T cells and BiTEs simultaneously against tumors. A preclinical study targeting the alpha folate receptor using a CAR, while also targeting EGFR using an oncolytic virus encoding a BiTE, led to increased inhibition of tumors (111). This study suggested that combining these approaches, and oncolytic viruses, could address the issues of antigen heterogeneity and
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

CAR T-cell and BiTE Therapies for Cancers REVIEW
August 2018 CANCER DISCOVERY | 931
immunosuppressive microenvironment of solid tumors to enhance antitumor responses.
CONCLUSIONSWe have summarized the current clinical status of the
two immunotherapies BiTE and CAR T-cell treatment, their modes of action, toxicities, and preclinical development. Both platforms have demonstrated excellent efficacy in clinical trials against hematologic malignancies and were recently approved by the FDA for treating B-ALL. With their applica-tions in the clinic, we will understand more about the anti-cancer mechanisms, investigate these treatments as single or combined methods in different situations, and eventually expand their success to other cancers.
Despite the excitement, a few issues still remain to be overcome. Interestingly, both platforms are facing the same dilemma: CRS and neurologic adverse effects and moderate anticancer effects in solid-tumor settings. Substantial effort has been invested in finding strategies for reducing toxicities and enhancing treatment efficacy against solid tumors, such as targeting the immunosuppressive microenvironment and enhancing T-cell infiltration to the tumors. Both treatments warrant further exploration in a wide variety of tumor set-tings.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
AcknowledgmentsThis work was supported by grants from Cure Cancer Australia
(1100199), the Peter MacCallum Cancer Centre Foundation, the National Health and Medical Research Council (NHMRC) of Aus-tralia (1103352 and 1132373), the National Breast Cancer Foun-dation (NBCF) of Australia (IIRS-18-064), and Susan G. Komen (16376637). P.K. Darcy and M.H. Kershaw were supported by NHMRC Senior Research Fellowships. C.Y. Slaney was supported by a postdoctoral fellowship from the NBCF. P. Wang was supported by grants from the National Natural Science Foundation of China (31470871, 81671566, and 31722019).
The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received March 29, 2018; revised May 20, 2018; accepted June 1, 2018; published first July 16, 2018.
REFERENCES 1. Klinger M, Benjamin J, Kischel R, Stienen S, Zugmaier G. Harness-
ing T cells to fight cancer with BiTE(R) antibody constructs—past developments and future directions. Immunol Rev 2016;270: 193–208.
2. Spiess C, Zhai Q, Carter PJ. Alternative molecular formats and thera-peutic applications for bispecific antibodies. Mol Immunol 2015; 67:95–106.
3. Velasquez MP, Bonifant CL, Gottschalk S. Redirecting T cells to hematological malignancies with bispecific antibodies. Blood 2018; 131:30–8.
4. Sadelain M, Brentjens R, Riviere I. The basic principles of chimeric antigen receptor design. Cancer Discov 2013;3:388–98.
5. Yang Y, Lin T, Jacoby E, Qin H, Gardner EG, Chien CD, et al. CD4 CAR T Cells Mediate CD8-like cytotoxic anti-leukemic effects resulting in leukemic clearance and are less susceptible to attenua-tion by endogenous TCR activation than CD8 CAR T cells. Blood 2015;126:100.
6. Turtle CJ, Hanafi LA, Berger C, Gooley TA, Cherian S, Hudecek M, et al. CD19 CAR-T cells of defined CD4+:CD8+ composition in adult B cell ALL patients. J Clin Invest 2016;126:2123–38.
7. Turtle CJ, Hanafi LA, Berger C, Hudecek M, Pender B, Robinson E, et al. Immunotherapy of non-Hodgkin’s lymphoma with a defined ratio of CD8+ and CD4+ CD19-specific chimeric antigen receptor-modified T cells. Sci Transl Med 2016;8:355ra116.
8. Kochenderfer JN, Somerville RPT, Lu T, Shi V, Bot A, Rossi J, et al. Lymphoma remissions caused by anti-CD19 chimeric antigen recep-tor T cells are associated with high serum interleukin-15 levels. J Clin Oncol 2017;35:1803–13.
9. Locke FL, Neelapu SS, Bartlett NL, Siddiqi T, Chavez JC, Hos-ing CM, et al. Phase 1 results of ZUMA-1: a multicenter study of KTE-C19 Anti-CD19 CAR T cell therapy in refractory aggressive lymphoma. Mol Ther 2017;25:285–95.
10. Xu Y, Zhang M, Ramos CA, Durett A, Liu E, Dakhova O, et al. Closely related T-memory stem cells correlate with in vivo expansion of CAR.CD19-T cells and are preserved by IL-7 and IL-15. Blood 2014;123:3750–9.
11. Sadelain M, Riviere I, Riddell S. Therapeutic T cell engineering. Nature 2017;545:423–31.
12. Hurton LV, Singh H, Najjar AM, Switzer KC, Mi T, Maiti S, et al. Tethered IL-15 augments antitumor activity and promotes a stem-cell memory subset in tumor-specific T cells. Proc Natl Acad Sci U S A 2016;113:E7788–E97.
13. Mack M, Gruber R, Schmidt S, Riethmüller G, Kufer P. Biologic properties of a bispecific single-chain antibody directed against 17-1A (EpCAM) and CD3: tumor cell-dependent T cell stimulation and cytotoxic activity. J Immunol 1997;158:3965.
14. Bargou R, Leo E, Zugmaier G, Klinger M, Goebeler M, Knop S, et al. Tumor regression in cancer patients by very low doses of a T cell-engaging antibody. Science 2008;321:974–7.
15. Davenport AJ, Cross RS, Watson KA, Liao Y, Shi W, Prince HM, et al. Chimeric antigen receptor T cells form nonclassical and potent immune synapses driving rapid cytotoxicity. Proc Natl Acad Sci U S A 2018;115:E2068–E76.
16. Davenport AJ, Jenkins MR, Cross RS, Yong CS, Prince HM, Ritchie DS, et al. CAR-T cells inflict sequential killing of multiple tumor target cells. Cancer Immunol Res 2015;3:483–94.
17. Haas C, Krinner E, Brischwein K, Hoffmann P, Lutterbuse R, Schlereth B, et al. Mode of cytotoxic action of T cell-engaging BiTE antibody MT110. Immunobiology 2009;214:441–53.
18. Loffler A, Kufer P, Lutterbuse R, Zettl F, Daniel PT, Schwenkenbe-cher JM, et al. A recombinant bispecific single-chain antibody, CD19 × CD3, induces rapid and high lymphoma-directed cytotoxicity by unstimulated T lymphocytes. Blood 2000;95:2098–103.
19. Offner S, Hofmeister R, Romaniuk A, Kufer P, Baeuerle PA. Induction of regular cytolytic T cell synapses by bispecific single-chain antibody con-structs on MHC class I-negative tumor cells. Mol Immunol 2006;43:763–71.
20. Brischwein K, Parr L, Pflanz S, Volkland J, Lumsden J, Klinger M, et al. Strictly target cell-dependent activation of T cells by bispecific single-chain antibody constructs of the BiTE class. J Immunother 2007;30:798–807.
21. Bluemel C, Hausmann S, Fluhr P, Sriskandarajah M, Stallcup WB, Baeuerle PA, et al. Epitope distance to the target cell membrane and antigen size determine the potency of T cell-mediated lysis by BiTE antibodies specific for a large melanoma surface antigen. Cancer Immunol Immunother 2010;59:1197–209.
22. Hoffmann P, Hofmeister R, Brischwein K, Brandl C, Crommer S, Bargou R, et al. Serial killing of tumor cells by cytotoxic T cells redirected with a CD19-/CD3-bispecific single-chain antibody con-struct. Int J Cancer 2005;115:98–104.
23. Amann M, D’Argouges S, Lorenczewski G, Brischwein K, Kischel R, Lutterbuese R, et al. Antitumor activity of an EpCAM/CD3-bispecific
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

Slaney et al.REVIEW
932 | CANCER DISCOVERY August 2018 www.aacrjournals.org
BiTE antibody during long-term treatment of mice in the absence of T-cell anergy and sustained cytokine release. J Immunother 2009;32:452–64.
24. Dreier T, Baeuerle PA, Fichtner I, Grun M, Schlereth B, Lorencze-wski G, et al. T cell costimulus-independent and very efficacious inhibition of tumor growth in mice bearing subcutaneous or leuke-mic human B cell lymphoma xenografts by a CD19-/CD3-bispecific single-chain antibody construct. J Immunol 2003;170:4397–402.
25. Amann M, Friedrich M, Lutterbuese P, Vieser E, Lorenczewski G, Petersen L, et al. Therapeutic window of an EpCAM/CD3-specific BiTE antibody in mice is determined by a subpopulation of EpCAM-expressing lymphocytes that is absent in humans. Cancer Immunol Immunother 2009;58:95–109.
26. Brentjens RJ, Santos E, Nikhamin Y, Yeh R, Matsushita M, La Perle K, et al. Genetically targeted T cells eradicate systemic acute lympho-blastic leukemia xenografts. Clin Cancer Res 2007;13:5426–35.
27. Spear P, Barber A, Rynda-Apple A, Sentman CL. Chimeric antigen receptor T cells shape myeloid cell function within the tumor microenvironment through IFN-gamma and GM-CSF. J Immunol 2012;188:6389–98.
28. Ross SL, Sherman M, McElroy PL, Lofgren JA, Moody G, Baeuerle PA, et al. Bispecific T cell engager (BiTE(R)) antibody constructs can mediate bystander tumor cell killing. PLoS One 2017;12:e0183390.
29. Lanitis E, Poussin M, Hagemann IS, Coukos G, Sandaltzopoulos R, Scholler N, et al. Redirected antitumor activity of primary human lymphocytes transduced with a fully human anti-mesothelin chi-meric receptor. Mol Ther 2012;20:633–43.
30. Henderson MA, Yong CS, Duong CP, Davenport AJ, John LB, Devaud C, et al. Chimeric antigen receptor-redirected T cells display multifunctional capacity and enhanced tumor-specific cytokine secretion upon secondary ligation of chimeric receptor. Immuno-therapy 2013;5:577–90.
31. Grupp SA, Kalos M, Barrett D, Aplenc R, Porter DL, Rheingold SR, et al. Chimeric antigen receptor-modified T cells for acute lymphoid leukemia. N Engl J Med 2013;368:1509–18.
32. Mueller KT, Maude SL, Porter DL, Frey N, Wood P, Han X, et al. Cellular kinetics of CTL019 in relapsed/refractory B-cell acute lymphoblastic leukemia and chronic lymphocytic leukemia. Blood 2017;130:2317–25.
33. Porter DL, Levine BL, Kalos M, Bagg A, June CH. Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia. N Engl J Med 2011;365:725–33.
34. Brentjens RJ, Davila ML, Riviere I, Park J, Wang X, Cowell LG, et al. CD19-targeted T cells rapidly induce molecular remissions in adults with chemotherapy-refractory acute lymphoblastic leukemia. Sci Transl Med 2013;5:177ra38.
35. Kochenderfer JN, Dudley ME, Carpenter RO, Kassim SH, Rose JJ, Telford WG, et al. Donor-derived CD19-targeted T cells cause regression of malignancy persisting after allogeneic hematopoietic stem cell transplantation. Blood 2013;122:4129–39.
36. Topp MS, Kufer P, Gokbuget N, Goebeler M, Klinger M, Neumann S, et al. Targeted therapy with the T-cell-engaging antibody blina-tumomab of chemotherapy-refractory minimal residual disease in B-lineage acute lymphoblastic leukemia patients results in high response rate and prolonged leukemia-free survival. J Clin Oncol 2011;29:2493–8.
37. Nagele V, Kratzer A, Zugmaier G, Holland C, Hijazi Y, Topp MS, et al. Changes in clinical laboratory parameters and pharmacody-namic markers in response to blinatumomab treatment of patients with relapsed/refractory ALL. Exp Hematol Oncol 2017;6:14.
38. Kershaw MH, Westwood JA, Parker LL, Wang G, Eshhar Z, Mavrouka-kis SA, et al. A phase I study on adoptive immunotherapy using gene-modified T cells for ovarian cancer. Clin Cancer Res 2006;12:6106–15.
39. Feng K, Liu Y, Guo Y, Qiu J, Wu Z, Dai H, et al. Phase I study of chi-meric antigen receptor modified T cells in treating HER2-positive advanced biliary tract cancers and pancreatic cancers. Protein Cell 2017 [Epub ahead of print].
40. Ahmed N, Brawley VS, Hegde M, Robertson C, Ghazi A, Gerken C, et al. Human epidermal growth factor receptor 2 (HER2) -specific
chimeric antigen receptor-modified T Cells for the immunotherapy of HER2-positive sarcoma. J Clin Oncol 2015;33:1688–96.
41. Gargett T, Yu W, Dotti G, Yvon ES, Christo SN, Hayball JD, et al. GD2-specific CAR T cells undergo potent activation and deletion following antigen encounter but can be protected from activation-induced cell death by PD-1 blockade. Mol Ther 2016;24:1135–49.
42. Junghans RP, Ma Q, Rathore R, Gomes EM, Bais AJ, Lo AS, et al. Phase I Trial of Anti-PSMA designer CAR-T cells in prostate cancer: possible role for interacting interleukin 2-T cell pharmacodynamics as a determinant of clinical response. Prostate 2016;76:1257–70.
43. Slaney CY, von Scheidt B, Davenport AJ, Beavis PA, Westwood JA, Mardiana S, et al. Dual-specific chimeric antigen receptor T cells and an indirect vaccine eradicate a variety of large solid tumors in an immunocompetent, self-antigen setting. Clin Cancer Res 2017;23: 2478–90.
44. Rossig C, Pule M, Altvater B, Saiagh S, Wright G, Ghorashian S, et al. Vaccination to improve the persistence of CD19CAR gene-modified T cells in relapsed pediatric acute lymphoblastic leukemia. Leukemia 2017;31:1087–95.
45. Schuster SJ, Svoboda J, Chong EA, Nasta SD, Mato AR, Anak O, et al. Chimeric antigen receptor T cells in refractory B-cell lympho-mas. N Engl J Med 2017;377:2545–54.
46. Neelapu SS, Locke FL, Bartlett NL, Lekakis LJ, Miklos DB, Jacobson CA, et al. Axicabtagene ciloleucel cAR T-cell therapy in refractory large B-cell lymphoma. N Engl J Med 2017;377:2531–44.
47. Kalos M, Levine BL, Porter DL, Katz S, Grupp SA, Bagg A, et al. T cells with chimeric antigen receptors have potent antitumor effects and can establish memory in patients with advanced leukemia. Sci Transl Med 2011;3:95ra73.
48. Turtle CJ, Hay KA, Hanafi LA, Li D, Cherian S, Chen X, et al. Dura-ble molecular remissions in chronic lymphocytic leukemia treated with CD19-specific chimeric antigen receptor-modified T cells after failure of ibrutinib. J Clin Oncol 2017;35:3010–20.
49. Maude SL, Frey N, Shaw PA, Aplenc R, Barrett DM, Bunin NJ, et al. Chimeric antigen receptor T cells for sustained remissions in leuke-mia. N Engl J Med 2014;371:1507–17.
50. Maude SL, Laetsch TW, Buechner J, Rives S, Boyer M, Bittencourt H, et al. Tisagenlecleucel in children and young adults with B-cell lymphoblastic leukemia. N Engl J Med 2018;378:439–48.
51. Brentjens RJ, Riviere I, Park JH, Davila ML, Wang X, Stefanski J, et al. Safety and persistence of adoptively transferred autologous CD19-targeted T cells in patients with relapsed or chemotherapy refractory B-cell leukemias. Blood 2011;118:4817–28.
52. Fry TJ, Shah NN, Orentas RJ, Stetler-Stevenson M, Yuan CM, Ramakrishna S, et al. CD22-targeted CAR T cells induce remission in B-ALL that is naive or resistant to CD19-targeted CAR immuno-therapy. Nat Med 2018;24:20–8.
53. Till BG, Jensen MC, Wang J, Qian X, Gopal AK, Maloney DG, et al. CD20-specific adoptive immunotherapy for lymphoma using a chi-meric antigen receptor with both CD28 and 4-1BB domains: pilot clinical trial results. Blood 2012;119:3940–50.
54. Ali SA, Shi V, Maric I, Wang M, Stroncek DF, Rose JJ, et al. T cells expressing an anti-B-cell maturation antigen chimeric antigen receptor cause remissions of multiple myeloma. Blood 2016;128: 1688–700.
55. Ritchie DS, Neeson PJ, Khot A, Peinert S, Tai T, Tainton K, et al. Persistence and efficacy of second generation CAR T cell against the LeY antigen in acute myeloid leukemia. Mol Ther 2013;21:2122–9.
56. Kershaw MH, Westwood JA, Darcy PK. Gene-engineered T cells for cancer therapy. Nat Rev Cancer 2013;13:525–41.
57. Slaney CY, Kershaw MH, Darcy PK. Trafficking of T cells into tumors. Cancer Res 2014;74:7168–74.
58. Louis CU, Savoldo B, Dotti G, Pule M, Yvon E, Myers GD, et al. Anti-tumor activity and long-term fate of chimeric antigen receptor-posi-tive T cells in patients with neuroblastoma. Blood 2011;118:6050–6.
59. Ahmed N, Brawley V, Hegde M, Bielamowicz K, Kalra M, Landi D, et al. HER2-specific chimeric antigen receptor-modified virus-specific T cells for progressive glioblastoma: a phase 1 dose-escalation trial. JAMA Oncol 2017;3:1094–101.
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

CAR T-cell and BiTE Therapies for Cancers REVIEW
August 2018 CANCER DISCOVERY | 933
60. O’Rourke DM, Nasrallah MP, Desai A, Melenhorst JJ, Mansfield K, Morrissette JJD, et al. A single dose of peripherally infused EGFRvIII-directed CAR T cells mediates antigen loss and induces adaptive resistance in patients with recurrent glioblastoma. Sci Transl Med 2017;9:eaaa0984.
61. Brown CE, Alizadeh D, Starr R, Weng L, Wagner JR, Naranjo A, et al. Regression of glioblastoma after chimeric antigen receptor T-cell therapy. N Engl J Med 2016;375:2561–9.
62. Martinelli G, Boissel N, Chevallier P, Ottmann O, Gokbuget N, Topp MS, et al. Complete hematologic and molecular response in adult patients with relapsed/refractory Philadelphia chromosome-positive B-precursor acute lymphoblastic leukemia following treat-ment with blinatumomab: results from a phase II, single-arm, multicenter study. J Clin Oncol 2017;35:1795–802.
63. Kantarjian H, Stein A, Gokbuget N, Fielding AK, Schuh AC, Ribera JM, et al. Blinatumomab versus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med 2017;376:836–47.
64. Goebeler ME, Knop S, Viardot A, Kufer P, Topp MS, Einsele H, et al. Bispecific T-Cell Engager (BiTE) antibody construct blinatu-momab for the treatment of patients with relapsed/refractory non-Hodgkin lymphoma: final results from a phase I study. J Clin Oncol 2016;34:1104–11.
65. Fiedler WM, Wolf M, Kebenko M, Goebeler M-E, Ritter B, Quaas A, et al. A phase I study of EpCAM/CD3-bispecific antibody (MT110) in patients with advanced solid tumors. J Clin Oncol 30:15, 2012 (suppl; abstr 2504).
66. Bi Y, Jiang H, Wang P, Song B, Wang H, Kong X, et al. Treatment of hepatocellular carcinoma with a GPC3-targeted bispecific T cell engager. Oncotarget 2017;8:52866–76.
67. Teachey DT, Lacey SF, Shaw PA, Melenhorst JJ, Maude SL, Frey N, et al. Identification of predictive biomarkers for cytokine release syndrome after chimeric antigen receptor T-cell therapy for acute lymphoblastic leukemia. Cancer Discov 2016;6:664–79.
68. Neelapu SS, Tummala S, Kebriaei P, Wierda W, Gutierrez C, Locke FL, et al. Chimeric antigen receptor T-cell therapy - assessment and management of toxicities. Nat Rev Clin Oncol 2018;15:47–62.
69. Gust J, Hay KA, Hanafi LA, Li D, Myerson D, Gonzalez-Cuyar LF, et al. Endothelial activation and blood-brain barrier disruption in neurotoxicity after adoptive immunotherapy with CD19 CAR-T Cells. Cancer Discov 2017;7:1404–19.
70. Hill JA, Li D, Hay KA, Green ML, Cherian S, Chen X, et al. Infec-tious complications of CD19-targeted chimeric antigen receptor-modified T-cell immunotherapy. Blood 2018;131:121–30.
71. Topp MS, Gokbuget N, Stein AS, Zugmaier G, O’Brien S, Bargou RC, et al. Safety and activity of blinatumomab for adult patients with relapsed or refractory B-precursor acute lymphoblastic leukaemia: a multicentre, single-arm, phase 2 study. Lancet Oncol 2015;16:57–66.
72. Brandl C, Haas C, d’Argouges S, Fisch T, Kufer P, Brischwein K, et al. The effect of dexamethasone on polyclonal T cell activation and redirected target cell lysis as induced by a CD19/CD3-bispecific single-chain antibody construct. Cancer Immunol Immunother 2007;56:1551–63.
73. Binnewies M, Roberts EW, Kersten K, Chan V, Fearon DF, Merad M, et al. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat Med 2018;24:541–50.
74. Moon EK, Wang LC, Dolfi DV, Wilson CB, Ranganathan R, Sun J, et al. Multifactorial T-cell hypofunction that is reversible can limit the efficacy of chimeric antigen receptor-transduced human T cells in solid tumors. Clin Cancer Res 2014;20:4262–73.
75. Highfill SL, Long AH, Orentas RJ, Mackall CL. Neutralization of murine myeloid-derived suppressor cells enhances the efficacy of a chimeric antigen receptor T-cells directed against pediatric solid tumors. J Immunother Cancer 2013;1:P265.
76. Burga RA, Thorn M, Point GR, Guha P, Nguyen CT, Licata LA, et al. Liver myeloid-derived suppressor cells expand in response to liver metastases in mice and inhibit the anti-tumor efficacy of anti-CEA CAR-T. Cancer Immunol Immunother 2015;64:817–29.
77. Ruella M, Klichinsky M, Kenderian SS, Shestova O, Ziober A, Kraft DO, et al. Overcoming the immunosuppressive tumor microenvi-
ronment of hodgkin lymphoma using chimeric antigen receptor T cells. Cancer Discov 2017;7:1154–67.
78. Kakarla S, Chow KK, Mata M, Shaffer DR, Song XT, Wu MF, et al. Antitumor effects of chimeric receptor engineered human T cells directed to tumor stroma. Mol Ther 2013;21:1611–20.
79. Beavis PA, Henderson MA, Giuffrida L, Mills JK, Sek K, Cross RS, et al. Targeting the adenosine 2A receptor enhances chimeric anti-gen receptor T cell efficacy. J Clin Invest 2017;127:929–41.
80. Newick K, O’Brien S, Sun J, Kapoor V, Maceyko S, Lo A, et al. Augmen-tation of CAR T-cell trafficking and antitumor efficacy by blocking protein kinase a localization. Cancer Immunol Res 2016;4:541–51.
81. John LB, Devaud C, Duong CP, Yong CS, Beavis PA, Haynes NM, et al. Anti-PD-1 antibody therapy potently enhances the eradication of established tumors by gene-modified T Cells. Clin Cancer Res 2013;19:5636–46.
82. Zhang Y, Zhang X, Cheng C, Mu W, Liu X, Li N, et al. CRISPR-Cas9 mediated LAG-3 disruption in CAR-T cells. Front Med 2017;11:554–62.
83. Shum T, Kruse RL, Rooney CM. Strategies for enhancing adop-tive T-cell immunotherapy against solid tumors using engineered cytokine signaling and other modalities. Expert Opin Biol Ther 2018;18:653–64.
84. Koneru M, Purdon TJ, Spriggs D, Koneru S, Brentjens RJ. IL-12 secreting tumor-targeted chimeric antigen receptor T cells eradicate ovarian tumors in vivo. Oncoimmunology 2015;4:e994446.
85. Shum T, Omer B, Tashiro H, Kruse RL, Wagner DL, Parikh K, et al. constitu-tive signaling from an engineered IL7 receptor promotes durable tumor elimination by tumor-redirected T cells. Cancer Discov 2017;7:1238–47.
86. Leen AM, Sukumaran S, Watanabe N, Mohammed S, Keirnan J, Yanagisawa R, et al. Reversal of tumor immune inhibition using a chimeric cytokine receptor. Mol Ther 2014;22:1211–20.
87. Mohammed S, Sukumaran S, Bajgain P, Watanabe N, Heslop HE, Rooney CM, et al. Improving chimeric antigen receptor-modified T cell function by reversing the immunosuppressive tumor microen-vironment of pancreatic cancer. Mol Ther 2017;25:249–58.
88. Moon EK, Carpenito C, Sun J, Wang LC, Kapoor V, Predina J, et al. Expression of a functional CCR2 receptor enhances tumor localiza-tion and tumor eradication by retargeted human T cells expressing a mesothelin-specific chimeric antibody receptor. Clin Cancer Res 2011;17:4719–30.
89. Chinnasamy D, Yu Z, Kerkar SP, Zhang L, Morgan RA, Restifo NP, et al. Local delivery of interleukin-12 using T cells targeting VEGF receptor-2 eradicates multiple vascularized tumors in mice. Clin Cancer Res 2012;18:1672–83.
90. Fu X, Rivera A, Tao L, Zhang X. Genetically modified T cells target-ing neovasculature efficiently destroy tumor blood vessels, shrink established solid tumors and increase nanoparticle delivery. Int J Cancer 2013;133:2483–92.
91. Zhu M, Wu B, Brandl C, Johnson J, Wolf A, Chow A, et al. Blinatu-momab, a bispecific T-cell engager (BiTE(®)) for CD-19 targeted cancer immunotherapy: clinical pharmacology and its implications. Clin Pharmacokinet 2016;55:1271–88.
92. Liu H, Saxena A, Sidhu SS, Wu D. Fc engineering for developing therapeutic bispecific antibodies and novel scaffolds. Front Immunol 2017;8:38.
93. Warnders FJ, Waaijer SJ, Pool M, Lub-de Hooge MN, Friedrich M, Terwisscha van Scheltinga AG, et al. Biodistribution and PET imag-ing of labeled bispecific T cell-engaging antibody targeting EpCAM. J Nucl Med 2016;57:812–7.
94. Whiteside TL. The tumor microenvironment and its role in promot-ing tumor growth. Oncogene 2008;27:5904.
95. Iwahori K, Kakarla S, Velasquez MP, Yu F, Yi Z, Gerken C, et al. Engager T cells: a new class of antigen-specific T cells that redirect bystander T cells. Mol Ther 2015;23:171–8.
96. Bonifant CL, Szoor A, Torres D, Joseph N, Velasquez MP, Iwahori K, et al. CD123-Engager T cells as a novel immunotherapeutic for acute myeloid leukemia. Mol Ther 2016;24:1615–26.
97. Velasquez MP, Torres D, Iwahori K, Kakarla S, Arber C, Rodriguez-Cruz T, et al. T cells expressing CD19-specific engager molecules for the immunotherapy of CD19-positive malignancies. Sci Rep 2016;6:27130.
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

Slaney et al.REVIEW
934 | CANCER DISCOVERY August 2018 www.aacrjournals.org
98. Liu X, Barrett DM, Jiang S, Fang C, Kalos M, Grupp SA, et al. Improved anti-leukemia activities of adoptively transferred T cells expressing bispecific T-cell engager in mice. Blood Cancer J 2016;6:e430.
99. Fajardo CA, Guedan S, Rojas LA, Moreno R, Arias-Badia M, de Sos-toa J, et al. Oncolytic adenoviral delivery of an EGFR-Targeting T-cell engager improves antitumor efficacy. Cancer Res 2017;77:2052–63.
100. Freedman JD, Hagel J, Scott EM, Psallidas I, Gupta A, Spiers L, et al. Oncolytic adenovirus expressing bispecific antibody targets T-cell cytotoxicity in cancer biopsies. EMBO Mol Med 2017;9:1067–87.
101. Yu F, Wang X, Guo ZS, Bartlett DL, Gottschalk SM, Song XT. T-cell engager-armed oncolytic vaccinia virus significantly enhances anti-tumor therapy. Mol Ther 2014;22:102–11.
102. Kohnke T, Krupka C, Tischer J, Knosel T, Subklewe M. Increase of PD-L1 expressing B-precursor ALL cells in a patient resistant to the CD19/CD3-bispecific T cell engager antibody blinatumomab. J Hematol Oncol 2015;8:111.
103. Krupka C, Kufer P, Kischel R, Zugmaier G, Lichtenegger FS, Kohnke T, et al. Blockade of the PD-1/PD-L1 axis augments lysis of AML cells by the CD33/CD3 BiTE antibody construct AMG 330: reversing a T-cell-induced immune escape mechanism. Leukemia 2016;30:484–91.
104. Zhang P, Shi B, Gao H, Jiang H, Kong J, Yan J, et al. An EpCAM/CD3 bispecific antibody efficiently eliminates hepatocellular carcinoma cells with limited galectin-1 expression. Cancer Immunol Immu-nother 2014;63:121–32.
105. Laszlo GS, Gudgeon CJ, Harrington KH, Dell’Aringa J, Newhall KJ, Means GD, et al. Cellular determinants for preclinical activity of a
novel CD33/CD3 bispecific T-cell engager (BiTE) antibody, AMG 330, against human AML. Blood 2014;123:554–61.
106. Hoseini SS, Dobrenkov K, Pankov D, Xu XL, Cheung NK. Bispecific antibody does not induce T-cell death mediated by chimeric anti-gen receptor against disialoganglioside GD2. Oncoimmunology 2017;6:e1320625.
107. Stone JD, Aggen DH, Schietinger A, Schreiber H, Kranz DM. A sensitivity scale for targeting T cells with chimeric antigen receptors (CARs) and bispecific T-cell Engagers (BiTEs). Oncoimmunology 2012;1:863–73.
108. Amann M, Brischwein K, Lutterbuese P, Parr L, Petersen L, Lor-enczewski G, et al. Therapeutic window of MuS110, a single-chain antibody construct bispecific for murine EpCAM and murine CD3. Cancer Res 2008;68:143–51.
109. Schlereth B, Kleindienst P, Fichtner I, Lorenczewski G, Brischwein K, Lippold S, et al. Potent inhibition of local and disseminated tumor growth in immunocompetent mouse models by a bispecific antibody construct specific for Murine CD3. Cancer Immunol Immunother 2006;55:785–96.
110. Wu MR, Zhang T, Gacerez AT, Coupet TA, DeMars LR, Sentman CL. B7H6-Specific bispecific T cell engagers lead to tumor elimination and host antitumor immunity. J Immunol 2015;194:5305–11.
111. Wing A, Fajardo CA, Posey AD Jr., Shaw C, Da T, Young RM, et al. Improving CART-cell therapy of solid tumors with oncolytic virus-driven production of a bispecific T-cell engager. Cancer Immunol Res 2018;6:605–16.
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297

2018;8:924-934. Published OnlineFirst July 16, 2018.Cancer Discov Clare Y. Slaney, Pin Wang, Phillip K. Darcy, et al. Strategies for Cancer Treatment
Redirection−CARs versus BiTEs: A Comparison between T Cell
Updated version
10.1158/2159-8290.CD-18-0297doi:
Access the most recent version of this article at:
Cited articles
http://cancerdiscovery.aacrjournals.org/content/8/8/924.full#ref-list-1
This article cites 108 articles, 43 of which you can access for free at:
Citing articles
http://cancerdiscovery.aacrjournals.org/content/8/8/924.full#related-urls
This article has been cited by 5 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerdiscovery.aacrjournals.org/content/8/8/924To request permission to re-use all or part of this article, use this link
Research. on August 11, 2020. © 2018 American Association for Cancercancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst July 16, 2018; DOI: 10.1158/2159-8290.CD-18-0297