Embed Size (px)
Citation preview

Carpometacarpal Carpometacarpal Joint ArthritisJoint Arthritis

Carpometacarpal (CMC)Carpometacarpal (CMC)Arthritis Arthritis

Carpometacarpal Joint Carpometacarpal Joint ArthritisArthritis
• Most commonly surgically reconstructed area with OA in arm
• Surgical indications- Refractory to non-operative treatment

CMC Osteoarthritis CMC Osteoarthritis
Affects 16-25% of Affects 16-25% of postmenopausal postmenopausal womenwomen
Causes pain swelling, Causes pain swelling, instability, deformity instability, deformity & loss of motion& loss of motion
Radiographic Radiographic evidence of basal evidence of basal joint arthritis joint arthritis
1 in 4 women1 in 4 women 1 in 12 men 1 in 12 men

CMC Basic ScienceCMC Basic Science Four ArticulationsFour Articulations
1.1.Trapeziometacarpal Trapeziometacarpal TMTM
2.2.TrapeziotrapezoidTrapeziotrapezoid3.3.Scaphotrapezial STScaphotrapezial ST4.4.Trapezium-Index Trapezium-Index
MetacarpalMetacarpal
CMC joint enables CMC joint enables opposition & allows opposition & allows arcs of movement in arcs of movement in 3 planes3 planes
1.1.Flexion-extensionFlexion-extension2.2.Abduction-adductionAbduction-adduction3.3.oppositionopposition

Saddle JointSaddle Joint Minimal osseous Minimal osseous
stability stability Rely on static Rely on static
ligamentous ligamentous constraints to limit MC constraints to limit MC base translationbase translation
5 stabilizing ligaments5 stabilizing ligaments1.1. Anterior obliqueAnterior oblique2.2. Posterior obliquePosterior oblique3.3. Anterior intermetacarpalAnterior intermetacarpal4.4. Posterior Posterior
intermetacarpalintermetacarpal5.5. Dorsal radiocarpalDorsal radiocarpal

EtiologyEtiology
Secondary to excessive basal joint Secondary to excessive basal joint laxitylaxity
Only the TM & ST joint lie along Only the TM & ST joint lie along the longitudinal compression axis the longitudinal compression axis of the the thumbof the the thumb
Radiographic disease most commonly Radiographic disease most commonly affects these 2 jointsaffects these 2 joints

EtiologyEtiology
During opposition axial rotation results in During opposition axial rotation results in increased contact forces between opposing increased contact forces between opposing joint surfaces subjecting the cartilage to joint surfaces subjecting the cartilage to shearshear

Pathophysiologic StagesPathophysiologic Stages
1.1. Cartilage is sheared & wornCartilage is sheared & worn
2.2. Osteophytes in response to inflammationOsteophytes in response to inflammation
3.3. Dorsoradial subluxation of the 1Dorsoradial subluxation of the 1stst MC base MC base
4.4. Excessive laxity & repetitive loadingExcessive laxity & repetitive loading
5.5. MC adopts an adducted posture leading to MC adopts an adducted posture leading to functional deficits as the ability to spread the functional deficits as the ability to spread the hand & palm compromised hand & palm compromised
Opening jarsOpening jars Octave on a pianoOctave on a piano
6.6. Hyperextension at MCP joint as a result of this Hyperextension at MCP joint as a result of this adduction deformityadduction deformity
7.7. Focal pain, diminished pinch strength, & Focal pain, diminished pinch strength, & narrowing of the functional hand widthnarrowing of the functional hand width

Thumb Carpometacarpal Thumb Carpometacarpal Joint ArthritisJoint Arthritis
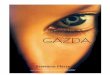
Eaton classification of Radiographic stages of Thumb CMC OA1 - Normal appearance2 - Joint space narrowing osteophytes < 2mm3 - Sclerosis, Subchondral cysts osteophytes > 2mm4 - Pantrapezial arthritis

DemographicsDemographics
IncidenceIncidence Prevalence in postmenopausal womenPrevalence in postmenopausal women
Isolated carpometacarpal – 25%Isolated carpometacarpal – 25% Scaphotrapezial – 2%Scaphotrapezial – 2% Combined - 8%Combined - 8%
Symptomatic ArthritisSymptomatic Arthritis 28% isolated and 55% combined28% isolated and 55% combined
Classification Classification Interrater and intrarater variationof the Eaton Interrater and intrarater variationof the Eaton
ClassificationClassification .6.6

Clinical FindingsClinical Findings
Dorsoradial prominence of the Dorsoradial prominence of the thumb MC base secondary to thumb MC base secondary to subluxation, inflammation, & subluxation, inflammation, & osteophytesosteophytes
Adduction deformity later in Adduction deformity later in diseasedisease
Point tenderness at CMC jointPoint tenderness at CMC joint MCP joint hyperextension & MCP joint hyperextension &
tendernesstenderness Decreased ROMDecreased ROM Pinch strength decreasedPinch strength decreased TM Grind test (axial loading with TM Grind test (axial loading with
MC rotation)MC rotation)

Thumb Carpometacarpal Thumb Carpometacarpal Joint ArthritisJoint Arthritis
•Differential diagnosis
• De Quervain’s (1st compartment) tenosynovitis• Radial sensory neuritis• 2nd compartment dorsal tenosynovitis• Arthritis
• Metacarpophalangeal• Scaphtrapeziotrapezoid• Radiocarpal

InvestigationInvestigation
Standard radiographic views of thumb (AP, Standard radiographic views of thumb (AP, lateral, oblique)lateral, oblique)
Provocatory views (lateral pinch)Provocatory views (lateral pinch) Bone scanBone scan Rule out other diagnosisRule out other diagnosis
1.1. Carpal tunnelCarpal tunnel
2.2. DeQuervains TenosynovitisDeQuervains Tenosynovitis
3.3. Trigger ThumbTrigger Thumb

Treatment OptionsTreatment Options Non-OperativeNon-Operative
Activity modificationActivity modification Anti-Inflammatory medicationsAnti-Inflammatory medications Splinting (Thumb spica)Splinting (Thumb spica)
Study 114 thumbsStudy 114 thumbs Long thumb spica for 3-4 weeks continuously, Long thumb spica for 3-4 weeks continuously,
then lessthen less Stage 1 & 2 – 67% improved Stage 1 & 2 – 67% improved Stage 3 & 4 – 54 % improvedStage 3 & 4 – 54 % improved At 6 months 55 % improvement in symptom At 6 months 55 % improvement in symptom
severityseverity

Various SplintsVarious Splints

Intra-Articular steroid Intra-Articular steroid injectionsinjections
25 gauge from 25 gauge from dorsoradial direction dorsoradial direction while traction on while traction on thumb (0.5 ml of thumb (0.5 ml of steroid +/- local steroid +/- local anaesthetic)anaesthetic)
Ultrasound guidedUltrasound guided

Ann Rheum Dis 2004;63:1260-1263
Intra-articular injectionIntra-articular injection
StudyStudy Double blind randomized controlled trial of 5 mg Double blind randomized controlled trial of 5 mg
triamcinolone vs salinetriamcinolone vs saline 40 patients with OA40 patients with OA Assessments @ 4, 12, 24 weeks for joint Assessments @ 4, 12, 24 weeks for joint
tenderness, physician, patient global assessmentstenderness, physician, patient global assessments
ResultsResults No clinical benefit in moderate to severe arthritisNo clinical benefit in moderate to severe arthritis Research should focus on the outcome of the first Research should focus on the outcome of the first
presentation of painpresentation of pain

Treatment OptionsTreatment OptionsSurgicalSurgical
Indicated if pain persists & is Indicated if pain persists & is severe enough to limit patients severe enough to limit patients function & ADL’s…never for function & ADL’s…never for deformity alonedeformity alone
GenerallyGenerally1.1. Osteotomy of thumb metacarpalOsteotomy of thumb metacarpal
2.2. Resection arthroplasty with or without Resection arthroplasty with or without interposition of autologous materialinterposition of autologous material
3.3. ArthrodesisArthrodesis

Osteotomy of the Osteotomy of the MetacarpalMetacarpal
Designed to offset the subluxing forces on Designed to offset the subluxing forces on the base of the MCthe base of the MC
Usually closing wedgeUsually closing wedge

Thumb Carpometacarpal Joint Thumb Carpometacarpal Joint ArthritisArthritis
Appearance of excised trapeziumCourtesy of Donald H. Lee, MD

Volar Ligament Volar Ligament ReconstructionReconstruction
Stage IStage I : : addresses laxity of addresses laxity of the volar oblique the volar oblique ligamentligament
Radial ½ of FCR is Radial ½ of FCR is passed through passed through hole made in MC hole made in MC basebase
Anchored with Anchored with appropriate appropriate tension tension

Ligament Reconstruction Ligament Reconstruction Tendon Interposition Tendon Interposition
(LRTI)(LRTI) Stage II / IIIStage II / III / IV / IV disease disease Removal of the involved joint Removal of the involved joint
partial trapeziectomy Stage II / IIIpartial trapeziectomy Stage II / III Total trapeziectomy Stage IVTotal trapeziectomy Stage IV
Slip of FCR to stabilize lax volar Slip of FCR to stabilize lax volar oblique ligament.oblique ligament.
End of FCR then coiled and inserted End of FCR then coiled and inserted into defect to maintain length and into defect to maintain length and provide painless mobility.provide painless mobility.


Thumb Carpometacarpal Joint Thumb Carpometacarpal Joint ArthritisArthritis
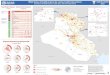
Excisional arthroplasty of trapezium with rolled tendon graft

Tendon Interposition Tendon Interposition ArthroplastyArthroplasty
StudiesStudies 45 patients, follow-up 8 years; pain 45 patients, follow-up 8 years; pain
reduction in 93%, Function 90% of reduction in 93%, Function 90% of opposite hand, function improved in opposite hand, function improved in 90% . 90% . Damen et al, 1996Damen et al, 1996
28 patients, followup 3 years:; pain 28 patients, followup 3 years:; pain reduction very good in > 90%, 87% reduction very good in > 90%, 87% satisfaction, improved functional satisfaction, improved functional mobility but decreased key pinch. mobility but decreased key pinch. Rayan Rayan et al, 1997et al, 1997

Trumble: J Hand Surg, 2000
Partial Trapeziectomy with ligament Partial Trapeziectomy with ligament reconstruction and interposition reconstruction and interposition
costochondral graftcostochondral graft
StudyStudy 41 patients, hemiresection arthroplasty, 41 patients, hemiresection arthroplasty,
FCR, allograft costochondral FCR, allograft costochondral reconstructionreconstruction
ResultResult Absorption Absorption 90% improved 90% improved

Surgical EffectsSurgical Effects
Thumb shorteningThumb shortening In arthritisIn arthritis More after surgeryMore after surgery

ArthrodesisArthrodesis
IndicationsIndications when major correction of the position of the MC when major correction of the position of the MC
required & a procedure to correct MP Joint required & a procedure to correct MP Joint hyperextensionhyperextension
Young heavy labourers Young heavy labourers
Cartilage surfaces debrided, bone graft Cartilage surfaces debrided, bone graft inserted, then K-Wire pinning, screw inserted, then K-Wire pinning, screw (cancellous lag)(cancellous lag)
404000 abduction & 45 abduction & 4500 extension extension Immobilize thumb spicaImmobilize thumb spica

Fulton et al, J Hand Surg 2001
Trapeziometacarpal Trapeziometacarpal ArthrodesisArthrodesis
Study: 49 patients, 7 year followup, Study: 49 patients, 7 year followup, fixation with K wires, use of a bone fixation with K wires, use of a bone graft in mostgraft in most
Results: nonunion – 7%, pain – Results: nonunion – 7%, pain – better, 20-25% developed better, 20-25% developed peritrapezial arthritsperitrapezial arthrits
Recommended in isolated arthritis, Recommended in isolated arthritis, care with thumb positioning, care with thumb positioning, increased laxity of peritrapezial joints increased laxity of peritrapezial joints may cause laxity pain and arthritismay cause laxity pain and arthritis

Chakrabart: J Hand Surg, 1997; Bezwada al 2002.
Carpometacarpal Joint Carpometacarpal Joint ReplacementReplacement
De La CaffiniereDe La Caffiniere Study – 93thumbs in 71 patientsStudy – 93thumbs in 71 patients Results – survival 89% @ 16 years, Results – survival 89% @ 16 years,
avoid in men < 65avoid in men < 65 SiliconeSilicone
84 % satisfaction in pain @ 16 years, 84 % satisfaction in pain @ 16 years, strength improvedstrength improved
6 implant fractures, no frank silicone 6 implant fractures, no frank silicone synovitissynovitis

ArthroplastyArthroplasty
Swanson Silicone ImplantSwanson Silicone Implant Titanium ImplantsTitanium Implants

Additional Surgical Additional Surgical OptionsOptions
Replacement materialsReplacement materials ePTFE (Goretex)ePTFE (Goretex) , , PTFE ( Marlex) PTFE ( Marlex) Tendons – FCR, Abd pollicis longus Tendons – FCR, Abd pollicis longus Ceramic Ceramic Joint Joint

Comparison StudiesComparison Studies
ProcedureProcedure Pain (%)Pain (%) Revision Revision Swanson Swanson 7777 1515HemiarthroplHemiarthroplasty asty (Ashhworth-(Ashhworth-Blatt)Blatt)
3838 5050
Soft tissue Soft tissue arthroplastyarthroplasty
7171 00

Additional Surgical Additional Surgical ConsiderationsConsiderations
Scaphotrapezial arthriritisScaphotrapezial arthriritis Scaphotrapezoid arthritisScaphotrapezoid arthritis Hyperextension of the MCP jointHyperextension of the MCP joint Subluxation of the thumbSubluxation of the thumb Adduction contractureAdduction contracture

Secondary MCPJ DeformitySecondary MCPJ DeformityHyperextensionHyperextension
Less than 30Less than 3000
1.1.Transarticular K-Wire with Transarticular K-Wire with joint in flexion for 4-5 weeksjoint in flexion for 4-5 weeks
2.2.Moving the extensor pollicis Moving the extensor pollicis brevis from base of proximal brevis from base of proximal phalanx to metacarpal shaft phalanx to metacarpal shaft
Greater than 30Greater than 3000
1.1.Arthrodesis (unstable joint)Arthrodesis (unstable joint)
2.2.Volar capsulodesisVolar capsulodesis

EndEnd