Embed Size (px)
Citation preview

Eur J Vasc Endovasc Surg 21, 214–219 (2001)doi:10.1053/ejvs.2000.1292, available online at http://www.idealibrary.com on
Carotid Stump Syndrome: Outcome from Surgical Management
S. M. Kumar1, J. C. C. Wang1, M. C. Barry∗1, L. Farrell1, C. J. Kelly1, P. H. Fitzgerald2,A. Leahy1 and D. Bouchier Hayes1
1 Department of Surgery, Royal College of Surgeons in Ireland and 2 the Non-Invasive Vascular Laboratory,Beaumont Hospital, Dublin 9, Ireland
Objectives: in patients with occluded internal carotid arteries the carotid stump is a potential source of microemboliresulting in the persistence of retinal or cerebral ischaemic symptoms. We report 25 patients who had persistent cerebraland retinal ischaemic symptoms with an occluded ipsilateral ICA and a carotid stump who underwent surgical exclusionof the stump.Methods: between January 1988 and January 1998, 332 patients underwent carotid endarterectomy. Twenty-five patients(20 males: five females; mean age 58.9 (range 44–78 years)) had carotid stump exclusion. Indications for surgery weretransient ischaemic attack (22), amaurosis fugax (eight) and cerebrovascular accident (13). Three patients had undergonecontralateral carotid endarterectomy and 12 had significant contralateral stenosis. Twenty patients were being treatedwith aspirin and four with warfarin at the time of presentation.Results: the diagnosis of carotid stump was made in 22 patients by angiography. In the remaining three patients duplexalone was diagnostic in two patients. In the third case duplex was combined with magnetic resonance angiography (MRA)to confirm the diagnosis. Stump exclusion was carried out by oversewing the ICA origin. All but one patient remainedsymptom free at follow-up.Conclusion: carotid stump syndrome should be considered as a likely clinical entity in patients with an occluded ICAand persisting cerebral and retinal microembolic symptoms. Surgical exclusion of the carotid stump is a safe and effectivemethod of treatment.
Key Words: Carotid stump; External carotid artery; Collateral circulation.
Introduction stump) in the presence of a patent external carotidartery (ECA) with reverse flow in its collateral cir-
The overall risk of major stroke or death from ICA culation.4,5 A previous study from this departmentdescribed the 2-year outcome in a group of six patientsocclusion is 30% with an ipsilateral stroke rate of 3–5%
per annum.1–3 Approximately two-thirds of strokes with carotid stump syndrome.4 Four patients under-went surgery and remained asymptomatic at 2 years.occur ipsilateral to the occluded ICA.1 Transient isch-
aemic attacks (TIA) caused by embolisation from a Of two patients treated with aspirin, one remainedasymptomatic and the other had a fatal cerebro-carotid source should cease when a stenotic lesion in
the ICA progresses to complete occlusion. However, vascular accident pre-operatively. This report de-scribes the surgical management of a further 25a small number of patients with occluded internal
carotid arteries continue to experience ocular or patients.cerebral ischaemic symptoms of an embolic natureeven when a cardiac source of embolism has beenexcluded.
Carotid stump syndrome is defined as the per-sistence of cerebral or retinal ischaemic symptoms after Patients and Methodsocclusion of an ipsilateral ICA. There is a demonstrablepatent proximal remnant of the occluded ICA (carotid Patients with carotid stump syndrome who underwent
surgical excision were identified from a computeriseddatabase. This database was cross-referenced with ca-
∗ Please address all correspondence to: M. C. Barry, Department of rotid duplex scan records, theatre log books and angio-Vascular Surgery, University Hospital Rotterdam, Dijkzigt Hospital,PO Box 2040, 3000 CA Rotterdam, The Netherlands. graphy records.
1078–5884/01/030214+06 $35.00/0 2001 Harcourt Publishers Ltd.

Carotid Stump Syndrome 215
Demographic data 1. One patient who presented with a stroke and anormal CT brain scan had a MRI brain scan which
Between January 1988 and January 1998, 332 patients showed a cerebral infarct.All patients had echocardiography and holter moni-underwent carotid surgery – 307 carotid end-
arterectomies and 25 carotid stump exclusions. There toring to outrule a cardiac source of emboli. Holtermonitoring detected arrhythmias in two patient butwere 20 male and five female patients (mean age 58.9
years; range 44–78 years). neither was clinically significant.
ResultsPresenting symptoms
Surgical procedureAll 25 patients were symptomatic with amaurosisfugax, transient ischaemic attacks or cerebrovascular
All procedures were carried out under general an-accidents (Table 1). At the time of presentation 20aesthesia. Following exposure of the common, internalpatients were taking aspirin and four patients wereand external carotid arteries and systemic hep-taking warfarin. Indications for warfarin includedarinisation, the common and external carotid arteriesatrial fibrillation (two), arrhythmia with cardiac pace-are clamped. A longitudinal arteriotomy extendingmaker (one) and a past history of pulmonary embolismfrom the CCA towards the ECA is performed. The(one). Three patients had previously undergone contra-ECA is endarterectomised and the internal carotidlateral carotid endarterectomy.stump lumen obliterated with interrupted 6/0 prolenesutures (Fig. 4).
DiagnosisPost-operative complications
The entire extracranial cervical carotid arterial systemwas evaluated using a standard 5–8 MHz pulsed wave One patient developed a right facial paresis and dys-Doppler probe (Acuson Ltd). Flow reversal in the arthria immediately post-operatively. CT brain scanophthalmic artery was assessed using a 10 MHz probe showed a new ipsilateral internal capsular infarct. Itover the ipsilateral orbit or by assessing the ipsilateral is possible that this could have arisen during manipu-supraorbital or supratrochlear arteries as an index to lation of the ECA causing embolisation through thethe direction of flow. Total occlusion of the ICA was ECA if it were a prominent contributor to the affectedshown in all patients, with the presence of a carotid hemisphere. Evacuation of a wound haematoma wasstump being confirmed by the finding of reverse flow required in another patient. Two patients developedin the cul-de-sac of the occluded internal carotid artery post-operative cranial nerve palsies. One patient died 6(Fig. 1). Contralateral carotid artery stenosis was diag- weeks post-operatively following an unrelated surgicalnosed in 12 patients (four had <50% stenosis; four had procedure.50–79% stenosis and four had 80–99% stenosis.
Twenty-two patients underwent carotid angio-graphy or digital subtraction angiography (DSA). One Follow-uppatient had arch aortography carried out. Nineteen of22 carotid angiograms identified a carotid stump in Patients were discharged from hospital after a meanthe occluded ICA (Fig. 2). hospital stay of 8.7 days (range 3–19 days). The mean
Magnetic resonance angiography (MRA) of the ca- follow-up period was 11.9 months (range 6 weeksrotid arteries was performed in eight patients (Fig. 3). to 36 months). Twenty-three patients have remainedIndications for MRA included failed femoral cath- asymptomatic since surgery. One patient suffered aneterisation in three patients. In the remaining five cases ipsilateral deterioration in visual acuity with a retinalMRA findings were being correlated with those of infarct 30 months post-operatively.conventional angiography as part of an ongoing re-search study to validate MRA as a modality for eval-uating the internal carotid artery. All but two patients Discussionhad computerised tomographic brain scans. Thirteeninfarcts ipsilateral to the carotid stump were diag- An occasional finding following complete occlusion of
the ICA is a patent proximal remnant of ICA seen onnosed. Details of these findings are included in Table
Eur J Vasc Endovasc Surg Vol 21, March 2001

S. M. Kumar et al.216
Tab
le1.
Det
ails
of25
pat
ien
tsin
clu
ded
.
Pati
ent
M/
FA
geM
edic
atio
nSy
mpt
oms
Freq
uenc
yM
ost
rece
ntC
Tsc
anO
utco
me
Follo
w-u
pno
.(y
ears
)of
sym
ptom
ssy
mpt
oms
find
ings
1M
60A
spir
inIp
sila
tera
l2
2m
onth
spr
e-op
Rig
htip
sila
tera
lpa
riet
alin
farc
tN
ofu
rthe
rsy
mpt
oms
65m
onth
sT
IA/
AF
2M
73A
spir
inIp
sila
tera
l2
1m
onth
pre-
opN
oC
Tsc
anpe
rfor
med
No
furt
her
sym
ptom
s1
mon
thT
IA/
AF
3M
62A
spir
inIp
sila
tera
lT
IA1
1m
onth
pre-
opA
trop
hic
chan
ges
No
furt
her
sym
ptom
s2
wee
ks4
M66
Asp
irin
Ipsi
late
ral
AF
2Im
med
iate
lypr
e-op
Ipsi
late
ral
lacu
nar
infa
rct
No
furt
her
sym
ptom
sD
ied
2m
onth
spo
st-o
p5
M75
Asp
irin
TIA
/co
llaps
e2
Imm
edia
tely
pre-
opB
ilate
ral
fron
topa
riet
alin
farc
tN
ofu
rthe
rsy
mpt
oms
3m
onth
s6
M66
Asp
irin
Vis
ual
loss
left
eye
1Im
med
iate
lypr
e-op
Rig
htoc
cipi
tal
infa
rct
No
furt
her
sym
ptom
s6
mon
ths
7M
66A
spir
inIp
sila
tera
l2
2m
onth
spr
e-op
Ipsi
late
ral
infa
rct
No
furt
her
sym
ptom
s12
mon
ths
TIA
/C
VA8
F72
Asp
irin
Ipsi
late
ral
14
mon
ths
pre-
opIp
sila
tera
lfr
onta
lin
farc
tR
IND
8m
onth
spo
st-o
p3
mon
ths
AF/
RIN
D9
F64
Asp
irin
TIA
/co
llaps
e3
Imm
edia
tely
pre-
opIp
sila
tera
lin
tern
alca
psul
arN
ofu
rthe
rsy
mpt
oms
3m
onth
sin
farc
t10
M58
War
fari
nT
IA1
Imm
edia
tely
pre-
opN
oC
Tsc
anpe
rfor
med
No
furt
her
sym
ptom
s3
mon
ths
11M
67A
spir
inT
IA/
AF
213
mon
ths
pre-
opG
loba
lat
roph
yN
ofu
rthe
rsy
mpt
oms
12m
onth
s12
M43
Asp
irin
TIA
/co
llaps
eM
ulti
ple
Imm
edia
tely
pre-
opN
orm
alN
ofu
rthe
rsy
mpt
oms
12m
onth
s13
M78
Asp
irin
Ipsi
late
ral
CVA
1Im
med
iate
lypr
e-op
Nor
mal
Rec
urre
ntT
IA6
mon
ths
14M
50A
spir
inIp
sila
tera
lA
F1
Imm
edia
tely
pre-
opN
orm
alU
lnar
nerv
epa
lsy
27m
onth
s15
M55
Asp
irin
AF
1Im
med
iate
lypr
e-op
Nor
mal
No
furt
her
sym
ptom
s3
mon
ths
16M
67W
arfa
rin
TIA
/A
F2
Imm
edia
tely
pre-
opN
orm
alN
ofu
rthe
rsy
mpt
oms
6m
onth
s17
F56
War
fari
nIp
sila
tera
lC
VA3
Imm
edia
tely
pre-
opIp
sila
tera
lin
farc
tN
ofu
rthe
rsy
mpt
oms
3m
onth
s18
M44
Non
eIp
sila
tera
lC
VA1
Imm
edia
tely
pre-
opN
orm
alN
ofu
rthe
rsy
mpt
oms
1m
onth
19M
51A
spir
inIp
sila
tera
l2
1m
onth
pre-
opIp
sila
tera
lin
farc
tN
ofu
rthe
rsy
mpt
oms
28m
onth
sT
IA/
CVA
20M
49A
spir
inIp
sila
tera
l1
1m
onth
pre-
opIp
sila
tera
lin
farc
tN
ofu
rthe
rsy
mpt
oms
5m
onth
sT
IA/
CVA
21M
61A
spir
inIp
sila
tera
lC
VA1
2m
onth
spr
e-op
Ipsi
late
ral
infa
rct
No
furt
her
sym
ptom
s46
mon
ths
22M
54W
arfa
rin
TIA
/C
VAM
ulti
ple
1ye
arpr
e-op
Ipsi
late
ral
infa
rct
No
furt
her
sym
ptom
s3
mon
ths
23F
65A
spir
inT
IA/
CVA
12
mon
ths
pre-
opIp
sila
tera
lin
farc
tN
ofu
rthe
rsy
mpt
oms
6m
onth
s24
M55
Asp
irin
Ipsi
late
ral
311
mon
ths
pre-
opIp
sila
tera
lin
farc
tW
ound
haem
atom
a12
mon
ths
TIA
/A
F/C
VA25
F59
Asp
irin
CVA
12
mon
ths
pre-
opIp
sila
tera
lin
farc
tN
ofu
rthe
rsy
mpt
oms
6m
onth
s
TIA=
Tran
sien
tis
chae
mic
atta
ck;A
F=A
mau
rosi
sFu
gax;
CVA=
Cer
ebro
vasc
ular
Acc
iden
t;R
IND=
Rev
ersi
ble
Isch
aem
icN
euro
logi
cal
Defi
cit.
Eur J Vasc Endovasc Surg Vol 21, March 2001

Carotid Stump Syndrome 217
Fig. 1. Colour-coded Doppler flow study showing a vortex of blue reversed flow in an internal carotid artery stump.
Fig. 2. Digital subtraction angiogram demonstrating patent commonand external carotid arteries. The blind-ending cul-de-sac at theorigin of the internal carotid artery is the carotid stump.
carotid duplex scan, carotid angiography or MRA.1,2,4,5
This region of the ICA is referred to as the “stump”where turbulent flow causes platelet-fibrin aggregationtheoretically leading to microembolisation.
The persistence of cerebral or retinal ischaemicFig. 3. Magnetic resonance angiogram showing a normal left sidedsymptoms after occlusion of an ipsilateral internalextra-cranial carotid circulation. A carotid stump is clearly seencarotid artery has been attributed to both haemo- on the right-hand side with patent common and external carotidarteries.dynamic and embolic factors.1,2,6 The haemodynamic
Eur J Vasc Endovasc Surg Vol 21, March 2001

S. M. Kumar et al.218
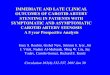
Fig. 4. Illustration of the steps involved in the surgical procedure to exclude the carotid stump. (1) The common, internal and externalcarotid arteries are isolated in the standard fashion through a longitudinal neck incision; (2) a longitudinal arteriotomy extending fromthe common towards the external carotid artery is performed; (3) the external carotid artery is endarterectomised and the internal carotidartery stump obliterated with interrupted 6/0 prolene sutures; (4) the arteriotomy is closed in standard fashion using 5/0 and 6/0 prolene.
mechanism proposes that cerebral hypoperfusion sec- where recurrence of ischaemic symptoms followingexclusion of the proximal stump occurs.ondary to ICA occlusion may lead to cerebroretinal
ischaemic symptoms. Altered cardiac output sec- Intermittent microembolisation from the carotidstump was the most probable cause of persistent isch-ondary to changes in cardiac rhythm and postural
changes have also been implicated. Several mech- aemic symptoms in these 25 patients because throm-botic material was found in the base of the stump ofanisms have been proposed to explain continuing
embolic symptoms in the presence of an occluded the occluded ICA in a number of patients and stumpexclusion resulted in cessation of symptoms in allipsilateral ICA. Documented sources of microemboli
from the extracranial vascular system include: the patients.In thepresenceofsignificantcontralateraldiseaseem-ipsilateral CCA or ECA; the carotid bifurcation via a
patent ECA, the contralateral carotid vessels via the bolisation from the contralateral carotid via the anteriorcommunicating artery is possible. Endarterectomy ofcircle of Willis,7 a patent proximal remnant of the
occluded ICA or distal thrombus occluding the ip- the contralateral carotid stenosis has been re-commended.12,13 This procedure, however, often fails tosilateral ICA. Isolated cases of emboli arising from the
distal tail of the thrombus in the occluded ICA have relieve symptoms because the symptomatic hemi-sphere does not receive significant collateral blood sup-been reported.8–11 This should be considered in cases
with occlusion of both the ipsilateral ICA and ECA and ply from the contralateral carotid artery.14–16 Three
Eur J Vasc Endovasc Surg Vol 21, March 2001

Carotid Stump Syndrome 219
patients in this study had significant (80–99%) stenosis ipsilateral carotid occlusion before the onset of symp-toms. However, the occurrence of symptoms in manyof the contralateral ICA. Cross-circulation was not dem-of the patients on more than one occasion supports ouronstrated on carotid angiography. Two patients hadtheory of an embolic phenomenon. Carotid stump syn-contralateral internal carotid endarterectomy8 days to 1drome should therefore be considered as a likely clinicalmonth before ipsilateral stump exclusion. Both patientsentity in patients with an occluded ICA and persistingcontinued to have TIAs following the endarterectomyipsilateral cerebral and retinal microembolic symp-and subsequent stump exclusion prevented furthertoms.symptoms. The third patient had no further symptoms
following stump exclusion and proceeded to have acontralateral internal carotid endarterectomy 1 month Referencesafter stump exclusion.
If a symptomatic internal carotid artery is ac- 1 Eikelboom BC, Ackerstaff RAG. Preoperative prediction ofcerebral ischaemia due to carotid occlusion. Eur J Vasc Surg 1993;companied by obstructive lesions in the ipsilateral7: 21–24.external carotid artery, as demonstrated by duplex 2 Irvine CD. The significance of one occluded internal carotid ar-
or angiography, external carotid endarterectomy may tery. Editorial. Eur J Vasc Endovasc Surg 1998; 16: 91–93.3 Nicholls SC, Kohler TR, Bergelin RO et al. Carotid artery oc-prove beneficial because the ipsilateral external carotid
clusion: natural history. J Vasc Surg 1986; 4: 479–485.artery is the major source of blood supply to the 4 Cassidy L, Grace PA, Bouchier Hayes D. The carotid stumpsymptomatic hemisphere.17–23 In the current series four syndrome. Eur J Vasc Surg 1992; 6: 368–370.
5 Quill DS, Colgan MP, Sumner DS. Carotid stump syndrome: apatients had moderate (50–79%) stenosis of the ip-colour-coded Doppler flow study. Eur J Vasc Surg 1989; 3: 79–83.silateral external carotid artery, one patient had severe 6 Georgiadis D, Grosset DG, Kennedy RL. Transhemispheric pas-
(80–99%) stenosis of the ipsilateral external carotid sage of microemboli in patients with unilateral internal carotidocclusion. Stroke 1993; 24: 1664–1666.artery and a further two patients had mild (16–49%)
7 O’Mara CS. Surgical significance of the external carotid artery.stenosis of both the ipsilateral external and common In: Bergan JJ, Jao JST, eds. Cerebrovascular Insufficiency. New York:
Grune & Stratton, 1983: 251–273.carotid arteries. These seven patients had en-8 Dandy WE. Results following ligation of the internal carotid ar-darterectomy of these atheromatous lesions before
tery. Arch Surg 1942; 45: 521–533.carotid stump exclusion. 9 Gunning AL, Pickering GW, Robb-Smith AHT, Russell RR.
Mural thrombosis of the internal carotid artery and subsequentCT brain scan did not alter the decision to offer orembolism. QJ Med 1964; 33: 155–195.withhold surgery in any of these patients. Six patients 10 Castainge D, Lhermitte F, Gautier JC, Escourolle R, De-
had normal CT scans but their continuing TIAs while rouesne C. Internal carotid artery occlusion. Brain 1970; 93: 231–258.on antiplatelet or anticoagulant therapy was an in-
11 Finkelstein S, Kleinman GM, Cuneo R, Baringer JR. Delayeddication for angiography. stroke following carotid occlusion. Neurology 1980; 30: 84–88.We describe a little reported syndrome which was 12 Fields WS. Selection of stroke patients for arterial reconstructive
surgery (Editorial). Am J Surg 1973; 125: 527–529.managed with minimal morbidity. Carotid stump ex-13 Thompson JE, Talkington CM. Carotid endarterectomy. Am Surgclusion poses fewer technical difficulties than carotid 1976; 184: 1–15.14 Fields WS, Malenikov V, Meyer JS. Joint study of arterial oc-endarterectomy. The risk of peroperative embolic
clusion. JAMA 1970; 211: 1993–2003.stroke should be much smaller. However, theoretically15 FieldsWS,LemakNS.Joint studyofextracranialarterialocclusion
hypoperfusion during the period of ECA clamping and internal carotid artery occlusion. JAMA 1976; 235: 2734–2738.16 Toole JF, Yuson CP, Janeway R et al. Transient ischaemic attacks: acould predispost to an ischaemic stroke if that cerebral
prospective of 225 patients. Neurology (Minneap) 1978; 28: 746–753.hemisphere is entirely dependent on the ECA for17 Le Pere RH, Hardy RC. Surgical improvement of collateral cir-
perfusion. The surgical technique described involves culation of the brain. Tex Med 1966; 62: 55–58.18 Diethrich EB, Liddicoat JE, McCutchen JJ, DeBakey ME. Sur-exclusion of the lumen of the ICA via the ECA and
gical significance of the external carotid artery in the treatment ofrequires minimal dissection of the ICA. An alternative cerebrovascular insufficiency. J Cardiovasc Surg 1968; 9: 213–223.approach would be to disconnect the ICA entirely at 19 Jackson BB. The external carotid as a brain collateral. Am J Surg
1967; 113: 375–378.the bifurcation thereby removing the carotid stump.20 Ehrenfield WK, Hoyt WF, Wylie EJ. Embolisation and transientIt must be borne in mind that one-third of patients blindness from carotid atheroma. Arch Surg 1966; 93: 781–784.
who develop ICA occlusion will die or have disabling 21 Connolly JE, Steimer EA. Endarterectomy of the external carotidartery. Arch Surg 1973; 106: 799–802.symptoms.1 Therefore, a knowledge of the timing be-
22 LordRSA.Late survivalaftercarotidendarterectomy for transienttween ICA occlusion and the onset of cerebral or retinal ischaemic attacks. J Vasc Surg 1984; 1: 512–519.
23 Burnbaum MD, Selhorst JB, Harbison JW, Brush JJ. Amaurosisembolic symptoms is important to the definitive dia-fugax from disease of the external carotid artery. Arch Neurol 1977;gnosis of the carotid stump syndrome. Given the lim-34: 532–535.
itations of a retrospective study, it was not possible toascertain in this report the presence of asymptomatic Accepted 9 December 2000
Eur J Vasc Endovasc Surg Vol 21, March 2001