Embed Size (px)
Citation preview

Caroline Ryan, MA (SW)Aging Care Connections
Thank you to The Practice Change Fellows Program, The Atlantic Philanthropies
and The John A. Hartford Foundation
Safe Discharge Home: A Community Response to Rapid
Reintegration of Observation Patients
The number of patients classified under “observation status” in Illinois hospitals has increased 900% over the past ten years
The existing aging service system is not well equipped to respond to the immediate needs of observation patients post-discharge
Safe Discharge Home improves the ability of the community to rapidly respond to the needs of observation patients as they transition from hospital to home

Aging Care Connections◦Non-profit social service organization◦Designated as a Care Coordination Unit and Elder Abuse
Unit by the State of Illinois
Adventist La Grange Memorial Hospital◦ 223 bed community hospital in La Grange, IL
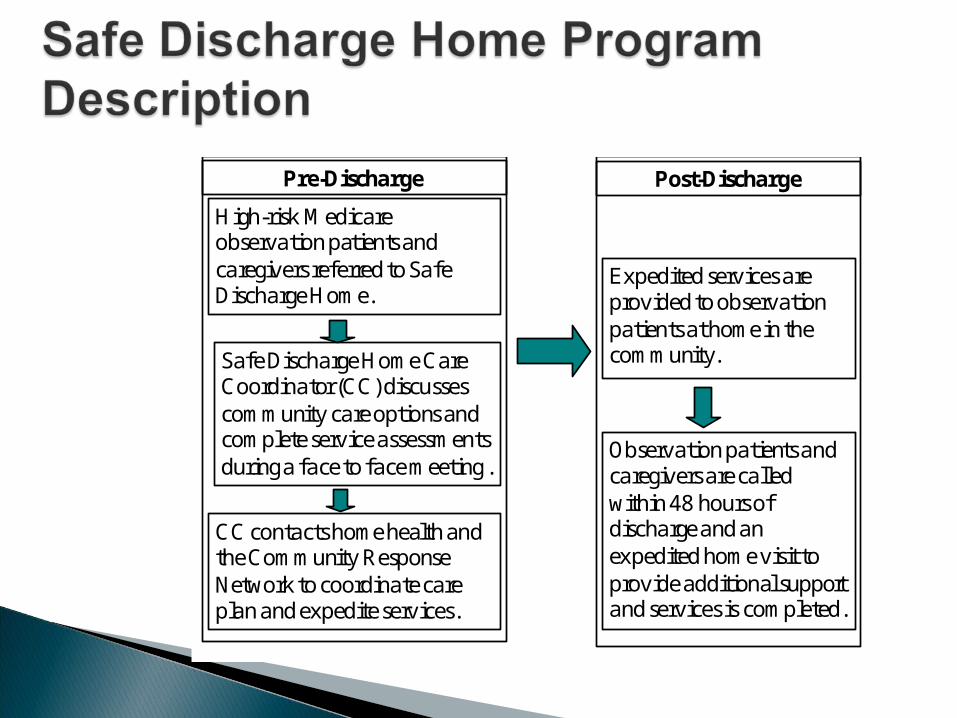
High-risk Medicare observation patients and caregivers referred to Safe Discharge Home.
Safe Discharge Home Care Coordinator (CC) discusses community care options and complete service assessments during a face to face meeting .
CC contacts home health and the Community Response Network to coordinate care plan and expedite services.
Expedited services are provided to observation patients a t home in the community.
Observation patients and caregivers are called within 48 hours of discharge and an expedited home visit to provide additional support and services is completed.
Pre-Discharge Post-Discharge
Community Response Network Requirements
◦Licensed service providers
◦Capacity and willingness to expedite services
◦MOU

Type of Service Providers◦14 Private Homemaker Service Providers
◦5 State Contracted Respite Providers
◦4 Pharmacies that deliver
◦3 Home Visit Physician Organizations
◦3 Home Hair Care Agencies
◦3 Private Meal Providers
◦2 Volunteer Organizations
◦2 Medicaid Waiver Providers
◦1 Adult Day Care Center
◦1 Durable Medical Equipment Lending Closet

76% over the age of 75
44% living alone
96% unmet psychosocial needs
92% frail
80% at risk for nursing home placement
79% eligible for state subsidized services
Reduced length of stay
Reduced number of Emergency Room visits and hospital readmissions within 48 hours and 30 days of discharge
Reduced time between discharge and start of community services
Increased patient and caregiver satisfaction
September 2009 – May 2010◦ Program protocols and evaluation methodology developed with ALMH and IRB
approval obtained◦ Aging Care Connections staff trained to coordinate transitions for observation
patients in Safe Discharge Home◦ Community Response Network formed and referral system developed
June 2010 – July 2011◦ Safe Discharge Home implemented at ALMH◦ Ongoing Community Response Network Meetings◦ Monthly measurement of patient and caregiver satisfaction◦ Quarterly collection of readmission and length of stay data
August 2011◦ Report summarizing program results submitted to ALMH and the Illinois
Department on Aging◦ Successful components integrated into Aging Resource Center Program and
presented to Illinois Transitional Care Consortium

Private/Public Partnership◦Hospital Savings Reducing length of stay through Safe Discharge
Home could save the hospital approximately $300,000 per year
Reduced ER visits Reduced readmissions within 30 days
◦Community Contribution Funding through billable assessments

Nurse case managers charged with monitoring the status of all observation patients at the hospital were originally going to serve as the referral source◦ The hospital social workers also want control of program
referrals
Clinical judgment vs. risk criteria?




























![The Hartford republican. (Hartford, KY) 1903-03-06 [p ]](https://img.pdfslide.us/doc/110x75/61a0afc1d05d2f067c3828b5/the-hartford-republican-hartford-ky-1903-03-06-p-.jpg)
