Embed Size (px)
Citation preview

CA
RO
LIN
E
BIL
LIN
GS
LE
Y, M
DT
heg
os
An
nu
al
Meetin
gJu
ne 1
, 20
14
OncoFertility Fertility Preserving Options & Outcomes in Gynecologic
Cancers

Objectives
Back
gro
un
d
Pre
vale
nce
of U
S p
op
ula
tion
aff
ecte
d
Etio
log
y of ca
nce
r treatm
en
t-rela
ted
fe
rtility failu
re
Ch
em
oth
era
py
Rad
ioth
era
py
Su
rgery
Options for fertility preservation Embryo cryopreservation Oocyte cryopreservation Ovarian tissue cryopreservation Oophoropexy GnRH analogue co-treatment
Candidates for fertility preservation
Breast cancer Cervical cancer Endometrial cancer Ovarian cancer

Gynecologic cancer incidence in reproductive age women
Bleyer A et al. Cancer Epidemiology in Older Adolescents and Young Adults 15 to 29 Years of Age, Including SEER Incidence and Survival: 1975-2000. National Cancer Institute, NIH Pub. No. 06-5767. 2006

Gynecologic cancer incidence in reproductive age women
Diagnosis and treatment of cancer often poses a threat to fertilityCancer Site
2014 Estimates
Diagnosis
New cases
Death Percentage under age 44 (2007-2011)
Projection of women to be diagnosed under age of 44
Endometrial 52,630 8,590 7.2% 3,789
Cervical 12,360 4,020 38.7% 4,783
Ovarian 21,980 14,270 12.1% 2,659
Vulvar 4,850 1,030 8.7% 421
SEER database, 5/2014 (http://seer.cancer.gov)

Etiology of cancer treatment-related fertility failureChemotherapy
High Risk (>80%)
Intermediate Risk Low/no risk (<20%) Unknown(examples)
CyclophosphamideIfosphamide
Cisplatin/Carboplatin
Methotrexate Taxanes
Cholarambucil Adriamycin 5-Fluorouracil Oxaliplatin
Melphalan Imatinib (TKI) Vincristine
Busulfan Bevacizumab Bleomycin
Nitrogen mustard Actinomycin D
Procarbazine Mitomycin

Etiology of cancer treatment-related fertility failureRadiation
Ova
rian
dam
ag
e
Rad
iatio
n to
xicity varie
s with
the
cell cycleH
igh
est in
G a
nd
M cycle
sO
ocyte
s are
particu
larly a
ffecte
dD
ose
rela
ted
red
uctio
n in
the
prim
ord
ial fo
llicle p
ool
Leth
al D
ose
Dose
>6
Gy u
sually ca
use
s irre
versib
le g
on
ad
al fa
ilure1
LD
L5
0 <2 G
y2
Dep
en
den
t on
ag
e, e
xten
t, typ
e/lo
catio
n a
nd
fractio
natio
n
sched
ule
1Howell et al, 1998. 2Wallace et al, 1989, 2003.
Age Dose of Radiotherapy
Birth 20.3 Gy
10 years 18.4 Gy
20 years 16.5 Gy
30 years 14.3 Gy
Cancer Radiation Dosage
Cervical Adjuvant Definitive
45-50 Gy45 Gy, boost to 54-60 Gy
Endometrial WPRT VcBT
45-50 Gy21 Gy
Vulvar Adjuvant Definitive
45-50 Gy54-60 Gy

Etiology of cancer treatment-related fertility failureRadiation
Ute
rine d
am
ag
e
Ob
stetrica
l In
crease
d risk
of S
AB
Seco
nd
trimeste
r pre
gn
an
cy loss
Pre
term
birth
Low
birth
weig
ht
Pla
cen
ta a
ccreta
Risk
s dep
en
den
t on
dose
, site,
ag
e•
Pre
pu
berta
l ute
rus is p
articu
larly
vuln
era
ble
Ch
ildh
ood
Can
cer S
urvivo
r Stu
dy1
Larg
e, m
ultice
nte
r coh
ort
Birth
ou
tcom
es o
f child
hood
rad
iatio
n
survivo
rs com
pare
d to
siblin
g (n
o ra
dia
tion
exp
osu
re) co
ntro
ls
12
64 ca
nce
r survivo
rs
22
01
sing
leto
n ch
ildre
n6
01
siblin
g co
ntro
ls (no ra
dia
tion
)
1
17
5 sin
gle
ton
child
ren
1Signorello et al, J Natl Cancer Inst 2006;26:98:1453
High dose (>500cGy)
Cancer survivors
Sibling controls
Odds ratio
95% CI P value
Preterm birth
50.0% 19.6% 3.5 1.5-8.0 .003
Low birth weight
36.2% 7.6% 6.8 2.1-22.2 .001
Small for gestational age
18.2% 7.8% 4.0 1.6-9.8 .003

Fertility Preserving Options
Options for fertility preservation Embryo cryopreservation (via ovulation induction)
Oocyte cryopreservation
Ovarian tissue cryopreservation
Oophoropexy
GnRH analogue co-treatment

Fertility Preserving Options: Embryo cryopreservation
Defi
nitio
n
Harve
sting
eg
gs, in
vitro fe
rtilizatio
n, a
nd
fre
ezin
g o
f em
bryo
s for la
ter im
pla
nta
tion
Com
men
t
Most e
stab
lished
tech
niq
ue fo
r fertility
pre
serva
tion
in w
om
en
Con
sidera
tion
s
Req
uire
s 10
-14
days o
f ova
rian
stimu
latio
n
from
the b
eg
inn
ing*
of m
en
strual cycle
* Ran
dom
start o
varia
n stim
ula
tion
Ou
tpatie
nt su
rgica
l pro
ced
ure
(eg
g re
trieva
l)
Req
uire
s partn
er o
r don
or sp
erm
Cost (ra
ng
e $
40
00
-80
00
per cycle
, $3
50
for
yearly sto
rag
e fe
es)
Med
icatio
ns
Follicle
stimu
latin
g h
orm
on
e a
nalo
gs
Aro
mata
se in
hib
itors
Sim
ilar n
um
ber o
f eg
gs a
nd
em
bryo
s an
d sim
ilar
pre
gn
an
cy ou
tcom
es 1
Sele
ctive e
strog
en
rece
pto
r inh
ibito
rs
Rate
s
Su
ccess:
Inta
ct em
bryo
s afte
r thaw
ing
have
simila
r im
pla
nta
tion
rate
s as fre
sh e
mb
ryos
59
% p
reg
nan
cy rate1
26
% live
birth
rate1
1Rodriguez-Wallberg et al, Cancer Treatment Reviews. 2012;38:354-361.

Fertility Preserving Options: Oocyte cryopreservation
Defi
nitio
n
Retrie
ving
an
d fre
ezin
g u
nfe
rtilized
eg
gs
thro
ug
h a
vitrifica
tion
pro
cess
Com
men
t
Pre
viou
sly con
sidere
d e
xperim
en
tal
Now
con
sidere
d a
stan
dard
pra
ctic
e p
er A
SC
O
20
13
gu
idelin
es
Con
sidera
tion
s
Req
uire
s 10
-14
days o
f ova
rian
stimu
latio
n
from
the b
eg
inn
ing*
of m
en
strual cycle
* Ran
dom
start o
varia
n stim
ula
tion
Ou
tpatie
nt su
rgica
l pro
ced
ure
(eg
g re
trieva
l)
Cost (ra
ng
e $
40
00
-80
00
per cycle
, $3
50
for
yearly sto
rag
e fe
es)
Med
icatio
ns
Follicle
stimu
latin
g h
orm
on
e a
nalo
gs
(FolliS
tim)
Aro
mata
se in
hib
itors
Sim
ilar n
um
ber o
f eg
gs a
nd
em
bryo
s an
d sim
ilar
pre
gn
an
cy ou
tcom
es 1
S
ele
ctive e
strog
en
rece
pto
r inh
ibito
rs
Rate
s
An
tinori e
t al:
Th
e fe
rtilizatio
n, p
reg
nan
cy, an
d im
pla
nta
tion
rate
s w
ere
92
.9%
, 32
.5%
, an
d 1
3.2
%, re
spective
ly2 T
hre
e h
un
dre
d th
irty-seve
n live
birth
s resu
lting
fro
m 8
57
thaw
ed
cycles (3
9.3
% p
reg
nan
cy rate
) w
ere
rep
orte
d a
cross a
ll cen
ters3
1Loren et al, J Clin Oncol. 2013;31. 2Antinori et al, RBM Online. 2007;14:72–79. 3Rudick et al, Fertil Steril. 2010 Dec;94(7):2642-6.

Fertility Preserving Options: Ovarian tissue cryopreservation
Defi
nitio
n
Fre
ezin
g o
f ova
rian
tissue a
nd
reim
pla
nta
tion
afte
r can
cer tre
atm
en
t
Reim
pla
nt:
Orth
oto
pic: re
imp
lan
t to th
e m
ed
ulla
ry portio
n o
f th
e re
main
ing
ova
ry, or to
the p
erito
neu
m o
f the
ova
rian
fossa
Hete
roto
pic: to
fore
arm
, ab
dom
inal w
all, ch
est w
all
*No live
birth
s rep
orte
d fo
r hete
roto
pic
Com
men
t
Poor su
rvival o
f ova
rian
strom
a is a
limitin
g
facto
r
Sam
e d
ay o
utp
atie
nt su
rgica
l pro
ced
ure
Con
sidera
tion
s
Con
sidere
d e
xperim
en
tal
Not a
pp
rop
riate
if the risk
of o
varia
n
invo
lvem
en
t is hig
hL
eu
kem
ia
Risk
of re
intro
du
ction
of m
alig
nan
t cells
No re
ports o
f can
cer re
curre
nce
in h
um
an
s1
Rate
s
In w
om
en
wh
o h
ave
survive
d ca
nce
r, at le
ast
24
live b
irths h
ave
been
rep
orte
d u
sing
cryo
pre
serve
d o
varia
n tissu
e1,2
,3
1Loren et al, J Clin Oncol. 2013;31. 2Donnez et al. Fertil Steril. 2013;99:1503-15. 3Fertil Steril 2014 May;101(5):1237-43.
Preparing the tissue for freezing
Transplantation ofovarian tissue
Reimplantation

Fertility Preserving Options: Ovarian tissue cryopreservation
Am
erica
n
Socie
ty of
Rep
rod
uctive
M
ed
icine: 2
014
Com
mitte
e
Op
inio
n1
“an option in patients w
ho m
ust urge
ntly undergo
aggressive
chemotherapy
and/or rad
iation, or
who have m
edica
l conditions requ
iring treatm
ent that m
ay threaten ovarian
function and subseque
nt fertility. O
varian tissue
cryopreservation m
ay be the only
option for prep
ubertal girls und
ergoing such
treatme
nts. H
owe
ver, these
technique
s are still considere
d to be exp
erimen
tal and should
be offere
d to ca
refully
selected patients as an exp
erimen
tal p
roto
col”.
1Fertil Steril. 2014 May;101(5):1237-43.

Fertility Preserving Options: Ovarian transposition (Oophoropexy)
Defi
nitio
n
Su
rgica
l rep
ositio
nin
g o
f ova
ries a
way fro
m a
p
lan
ned
rad
iatio
n fi
eld
Com
men
t
Sam
e d
ay su
rgica
l pro
ced
ure
Mu
st occu
r just p
rior to
rad
iatio
n th
era
py to
p
reve
nt m
igra
tion
of o
varie
s to o
rigin
al
positio
n
May n
eed
rep
ositio
nin
g o
r IVF
to co
nce
ive
Risk
s
Ova
rian
torsio
n
Ch
ron
ic ova
rian
pain
Infa
rction
of fa
llop
ian
tub
e
Need
for re
-op
era
tion
E
ffica
cy
Men
struatio
n5
0%
succe
ss rate1
alte
red
blo
od
flow
to th
e o
vary
scatte
red
rad
iatio
n (p
an
um
bra
) A
ge o
f the p
atie
nt
Dose
an
d e
xten
t of ra
dia
tion
Pre
gn
an
cyVaria
ble
Morice
et a
l2
37
patie
nts
Ova
rian
tran
spositio
n
Ute
rine co
nse
rvatio
n
Ove
rall p
reg
nan
cy rate
: 12
/37
(32
%)
18
pre
gn
an
cies in
12
patie
nts
1Loren et al, J Clin Oncol. 2013;31. 2Morice et al,Hum Reprod. 1998 Mar;13(3):660-3.

Fertility Preserving Options: GnRH analogue co-treatment
Defi
nitio
n
Use
of h
orm
on
al th
era
pie
s to p
rote
ct ova
rian
tissu
e d
urin
g ch
em
oth
era
py a
nd
rad
iatio
n
thera
py
Com
men
t
Inje
ction
s prio
r to a
nd
du
ring
gon
ad
oto
xic tre
atm
en
ts
Risk
s
Sid
e e
ffects
Eff
icacy
Meta
-an
alysis, 2
01
116
RC
Ts
Con
clusio
n: M
ay b
e b
en
efi
cial
Men
struatio
n:
Incre
ase
d in
ciden
ce sp
on
tan
eou
s men
struatio
n
(OR
3.4
6, C
I 1.1
3-1
0.5
7)
Incre
ase
d in
ciden
ce sp
on
tan
eou
s ovu
latio
n (O
R
5.7
0, 9
5%
CI 2
.29
-14
.20
)
N
O d
iffere
nce
in sp
on
tan
eou
s pre
gn
an
cy rate
OP
TIO
N2
Men
struatio
n:
No d
iffere
nce
betw
een
ova
rian
sup
pre
ssion
an
d
no tre
atm
en
t with
Gn
RH
an
alo
gu
e
AS
CO
2013
Gn
RH
is not a
n e
ffective
meth
od
of
fertility p
rese
rvatio
n
Sh
ou
ld n
ot so
lely b
e re
lied
up
on
for fe
rtility p
rese
rvatio
n
1Bedaiwyi et al, Fertil Steril. 2011;95(3):906. 2Leonard et al, J Clin Oncol. 2010;28: .

Candidates for fertility preservation
Candidates Breast cancer Cervical cancer Endometrial cancer Ovarian cancer

Candidates for fertility preservationBreast Cancer
Bre
ast C
an
cer
23
2,3
40 w
om
en
will b
e d
iag
nose
d in
20141
30
% p
rior to
ag
e 4
4
Tre
atm
en
t
Mu
lti-ag
en
t, main
ly cyclop
hosp
ham
ide
base
d, cyto
toxic ch
em
oth
era
py re
gim
en
s
Tim
ing
6 w
eek in
terva
l from
surg
ery to
ch
em
oth
era
py
Con
cern
s
Horm
on
e re
spon
sive (E
R, P
R)
Op
tion
s
Ovu
latio
n in
du
ction
Aro
mata
se in
hib
itors
SE
RM
s- Tam
oxife
n
Tissu
e cryo
pre
serva
tion
Rare
meta
stasis to
ova
ries
1 http://seer.cancer.gov/csr/ 1975_2011/results_single/ sect_01_table.01.pdf

Candidates for fertility preservationBreast Cancer
Azim
, et a
l 20081
Risk
of le
trozo
le a
nd
FS
H o
n re
curre
nce
21
5 b
reast ca
nce
r patie
nts
Pro
spective
, non
-ran
dom
ized
trial, 2
00
2-2
00
77
9 p
atie
nts : le
trozo
le +
FS
H1
36
patie
nts: co
ntro
ls, no fe
rtility treatm
en
tsM
ean
follo
w u
p a
fter ch
em
oth
era
py: 2
3.4
mon
ths
vs 33
mon
ths (co
ntro
l)
Recu
rren
ce
PF
S: N
o d
iffere
nce
(HR
0.5
6, C
I 95
% .1
7-1
.9)
Con
clusio
nU
se o
f letro
zole
+ F
SH
for o
varia
n stim
ula
tion
does
not a
pp
ear to
incre
ase
the risk
of re
curre
nce
in th
e
short te
rmL
on
ger fo
llow
up
is need
ed
1 Azim AA et al., J Clin Oncol 2008;26:2630–5
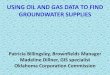
Relapse-free survival in women with breast cancer stimulated withletrozole versus control group. Kaplan-Meier plot (hazard ratio0.56, 95% CI 0.17–1.9).

Candidates for fertility preservationCervical Cancer
Cervica
l Can
cer
12
,36
0 w
om
en
will b
e d
iag
nose
d in
2
01
41
Tre
atm
en
t
Early S
tag
e:
Rad
ical su
rgery, lym
ph
ad
en
ecto
my
Possib
le a
dju
van
t chem
ora
dia
tion
Con
cern
s
Ova
rian
invo
lvem
en
t2,3
SC
C: 0
.5-0
.79
%A
den
oca
rcinom
a: 1
.7%
-5.3
1%
1http://seer.cancer.gov/csr/ 1975_2010/results_single/ sect_01_table.01.pdf, 2Sutton et al, Am. J. Obstet. Gynecol. 1992;166:50–53, 3Shimada et al, Gynecol Oncol. 2006;101(2):234-7. 4Lu et al, Gynecol Oncol. 2013;04:470.

Candidates for fertility preservationCervical Cancer
Op
tion
s
Su
rgica
lR
ad
ical tra
chele
ctom
y, lym
ph
ad
en
ecto
my
Vag
inal
Lap
aro
scop
ic or ro
botic
1http://seer.cancer.gov/csr/ 1975_2010/results_single/ sect_01_table.01.pdf, 2Sutton et al, Am. J. Obstet. Gynecol. 1992;166:50–53, 3Shimada et al, Gynecol Oncol. 2006;101(2):234-7. 4Lu et al, Gynecol Oncol. 2013;04:470.
Reconstruction of the uterine corpus to upper vagina after the cerclage is placed
The intent of the radical abdominal trachelectomy was to resect the cervix, upper 1–2 cm of the vagina, parametrium, and paracolpos in a similar manner to a type III radical abdominal hysterectomy but sparing the uterine corpus

Candidates for fertility preservationCervical Cancer
Radical abdominal trachelectomy—the cervical tissue and parametria are separated from the fundus

Candidates for fertility preservationCervical Cancer
The uterus is reattached to the vaginal apex

Candidates for fertility preservationCervical Cancer
The reconstructed fundus with remaining blood supply from the intact utero-ovarian ligaments—uterine serosa without evidence of fundal ischemia

Candidates for fertility preservationCervical Cancer
Ob
stetric o
utco
mes
>250
live b
irths h
ave
been
rep
orte
d1
Pla
nte
et a
l, 20082
, 20113
Su
rvival o
utco
mes
Recu
rren
ce
Morta
lity
1Lu et al, Gynecol Oncol. 2013;04:470. 2Plante et al, Gynecol Oncol. 2008;111:S105. 3Plante et al, Gynercol Oncol. 2011;121:290-7.
Plante 2008N=256 pregnancies
Plante 2011 N=106 pregnancies
1st trimester loss 18% 20%
2nd trimester loss 8.6% 3%
3rd trimester delivery
62% 73%
Preterm delivery <37 weeks<32 weeks
28%12%
18%4%
Term delivery 40% 55%

Candidates for fertility preservationCervical Cancer
On
colo
gic o
utco
mes
Pla
nte
et a
l, 20081
, 20112
Recu
rren
ce risk
facto
rs:
20
08
•L
esio
ns la
rger th
an
2
cms (2
9 vs 1
%)
•P
rese
nce
of LV
SI (1
2 vs
2%
)
20
11
•L
esio
ns la
rger th
an
2
cms
1Plante et al, Gynecol Oncol. 2008;111:S105. 3Plante et al, Gynercol Oncol. 2011;121:290-7.
Plante 2008N=603 patients (%)
Plante 2011N=125 patients (%)
Recurrence rate 27 (4.5%) 6 (4.8%)
Death from disease (%)
15 (2.5%) 2 (1.6%)
Abandoned VRT 10-12% 4 (11%)
5 year PFS 96%

Candidates for fertility preservationEndometrial Cancer
En
dom
etria
l Can
cer
It is estim
ate
d th
at 5
2,6
30
wom
en
w
ill be d
iag
nose
d in
20
141
Can
did
ate
s
Early sta
ge u
terin
e ca
nce
r, FIG
O Ia
Low
gra
de h
istolo
gy (e
nd
om
etrio
id)
No m
yom
etria
l invo
lvem
en
t (MR
I)
Tre
atm
en
t
Pro
gestin
M
ed
roxyp
rog
esto
ne
Meg
estro
l ace
tate
Levo
norg
estre
l IUD
Meta
-an
alysis2
R
eg
ressio
n ra
teR
eso
lutio
n o
f 76
% o
f 408 p
atie
nts
Live
birth
rate
:28
% live
birth
rate
Recu
rren
ce ra
te:
41
% o
f 26
7 o
f eva
luab
le p
atie
nts h
ad
re
curre
d
1 http://seer.cancer.gov/csr/ 1975_2010/results_single/ sect_01_table.01.pdf. 2Gallos et al, Am J Obstet Gynecol. 2012;207:(266):e1-2.

Candidates for fertility preservationEndometrial Cancer
Gu
nd
erso
n e
t al, 2
01
21
Med
ical m
an
ag
em
en
t (p
rog
estin
s)
45
stud
ies, 3
91
patie
nts
31
.7 ye
ars o
ld (m
ed
ian
ag
e)
Tre
atm
en
t:
Med
roxyp
rog
este
ron
e (4
9%
), M
eg
ace
(25
%), IU
D (1
9%
)
1Gunderson et al, Gynecol Oncol. 2012;125;477-482.
Initial Response
Complete Response
CR with recurrence
Persistence/progressive disease
Proportion achieving pregnancy
Number of live birth
CAH 85.6% 65.8% 23.2% 14.4% 28/111 (41%)
28
EC 74.6% 48.2% 35.4% 25.4% 89/240 (34.8%)
89
P-value
0.03 0.002 0.03 0.02 0.39 n/a

Candidates for fertility preservationOvarian Cancer
Ova
rian
can
cer
>22,0
00 w
om
en
will b
e d
iag
nose
d in
20
141
15
% w
ill be yo
un
ger th
an
40
Can
did
ate
s
Bord
erlin
e tu
mors
Early sta
ge o
varia
n ca
nce
rsG
erm
cell
Sex co
rd stro
mal
Ep
ithelia
l?
Tre
atm
en
t
Su
rgica
lU
SO
, om
en
tecto
my, w
ash
ing
s, p
erito
neal b
iop
sies, p
elvic a
nd
aortic
lymp
had
en
ecto
my
Pre
serva
tion
of o
ne o
vary, u
teru
s
Park
, et a
l 20
092
Bord
erlin
e o
varia
n tu
mors
Recu
rren
ce R
ate
: 4.9
% (S
OC
) vs 5.1
% (fe
rt sp
arin
g)
Dise
ase
free su
rvival
10
yr DF
S: 9
2%
(SO
C) vs 9
5%
(fert sp
arin
g)
O
vera
ll surviva
l1
0 yr O
S: 9
7%
(SO
C) vs 9
8%
(fert sp
arin
g)
Pre
gn
an
cy3
4 te
rm p
reg
nan
cies
1 http://seer.cancer.gov/csr/ 1975_2010/results_single/ sect_01_table.01.pdf 2 Park et al, Gynecol Oncol. 2009;113:75-82.

Candidates for fertility preservationOvarian Cancer
Ep
ithelia
l Ova
rian
can
cer?
Can
did
ate
sS
tag
e IA
Sta
ge IC
, gra
de 1
-2, fa
vora
ble
h
istolo
gic typ
e
Sero
us, m
ucin
ou
s, en
dom
etrio
id
Inelig
ible
S
tag
e >
ICG
rad
e III
Un
favo
rab
le h
istolo
gic typ
e
Cle
ar ce
ll •
Poore
r surviva
l
Nam
, et a
l 201
31
918
patie
nts
Recu
rren
ce: 1
09 (1
1.9
%)
Death
: 48
(5.2
%)
O
bste
trical:
17
7 p
atie
nts
24
2 p
reg
nan
cies
21
4 te
rm b
irths (8
8%
), 1 p
rete
rm
(0.4
%)
SA
B ra
te: 2
5/2
42
(10
%)
Ecto
pic ra
te: 2
/42
(0.8
%)
No co
ng
en
ital a
nom
alie
s
1Nam et al, Gynecol Obstet Invest. 2013;76(1):14-24.

American Society of Clinical Oncology (ASCO)Clinical Oncology Clinical Practice Guidelines
20
06
AS
CO
1
Key R
eco
mm
en
datio
ns:
Discu
ssion
of fe
rtility pre
serva
tion
R
efe
r patie
nts w
ho e
xpre
ss inte
rest to
RE
I sp
ecia
listsA
dd
ress fe
rtility pre
serva
tion
early, b
efo
re
treatm
en
t starts
Docu
men
t fertility p
rese
rvatio
n d
iscussio
ns in
th
e m
ed
ical re
cord
An
swer b
asic q
uestio
ns w
heth
er fe
rtility p
rese
rvatio
n m
ay h
ave
an
imp
act o
n su
ccessfu
l ca
nce
r treatm
en
tR
efe
r patie
nts to
psych
oso
cial p
rovid
ers if th
ey
exp
erie
nce
distre
ss ab
ou
t pote
ntia
l infe
rtilityE
nco
ura
ge p
atie
nt to
particip
ate
in clin
ical
trials
20
06
AS
CO
1
Ad
ult F
em
ale
specifi
c reco
mm
en
datio
ns
Pre
sen
t em
bryo
cryop
rese
rvatio
n a
s an
esta
blish
ed
fertility p
rese
rvatio
n m
eth
od
Discu
ss ova
rian
tran
spositio
n (o
op
horo
pexy)
wh
en
pelvic ra
dia
tion
thera
py is p
lan
ned
Info
rm p
atie
nts o
f con
serva
tive g
yneco
log
ic su
rgery a
nd
rad
iatio
n th
era
py o
ptio
ns
Info
rm p
atie
nts th
at th
ere
is insu
fficie
nt
evid
en
ce re
gard
ing
the e
ffective
ness o
f ova
rian
su
pp
ressio
n (G
nR
H a
nalo
gs) a
s a fe
rtility p
rese
rvatio
n m
eth
od
, an
d ca
nn
ot b
e re
lied
u
pon
Info
rm p
atie
nts th
at o
ther m
eth
od
s (ova
rian
tissu
e p
rese
rvatio
n, o
ocyte
cryop
rese
rvatio
n)
are
still exp
erim
en
tal
20
13
AS
CO
2
Reco
mm
en
datio
n ch
an
ges
Oocyte
cryop
rese
rvatio
n is co
nsid
ere
d a
sta
nd
ard
pra
ctice, a
nd
no lo
ng
er
exp
erim
en
tal
1Lee et al, J Clin Oncol. 2006;24:2917-2931. 2Loren et al, J Clin Oncol. 2013 Jul 1;31(19):2500-10.

Summary
Fertility matters, even with a cancer diagnosis Patients are concerned, and want to discuss options
Refer early. At the time of a cancer diagnosis, consider a referral to REI, as time is often limited between diagnosis and treatment
Physicians are not addressing the fertility concerns with patients
OncoFertility Still in its infancy
Additional, long term studies are needed to know the effects of these treatments on cancer recurrence and survival

Thank You
Cuterus- the adorable uterus!