Embed Size (px)
Citation preview
11FK.235.Os7.PHC (Nov-16)
Name: ______________________________________________________
£I have an ileostomy
£I have a colostomy
Please bring this booklet with you to the hospital when you come for your surgery.
Caring For Your OstomyWhat You Should Know
2
IntroductionWe encourage you to use this booklet as one essential component of your ostomy resources. We do not expect you to learn everything while you are in the hospital. While you are here we will do our best to provide you with the knowledge you need to care for yourself after an ostomy.
Caring For Your Ostomy - What You Should Know© 2016 Providence Health Care
The information in this book has been adapted from a number of sources – our thanks to all.References available upon request.
In particular, we would like to acknowledge the Canadian Association of Enterostomal Therapists (CAET).
And thanks also to members, past and present, of the PHC Wound Ostomy team -Pam Bocquentin, Neal Dunwoody, Aleza Moyer, B.J. Paproski, Corina Tezcan,
Bethany Thomas, Pam Turnbull and Gwen Varns
Edited by Hedda EybenIllustrations & layout by Gary Cody
If you have suggestions for improving this book, please write to:[email protected]
We also encourage you to take time before your surgery to identify some
people you can talk to about your feelings. You are also welcome to discuss your thoughts and concerns with an ostomy nurse.
An ostomy nurse has special education so they can answer your questions and direct you to the right resource.
3
Table of contentsThe digestive tract. . . . . . . . . . . . . . . . . . . . . . . . . . . . .1What is a stoma? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2Types of stomas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Comparing ileostomy and colostomy (table) . . . . . .4Before your ostomy surgery . . . . . . . . . . . . . . . . . . . .6After surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6Going home from hospital. . . . . . . . . . . . . . . . . . . . . .7Support after you go home . . . . . . . . . . . . . . . . . . . . .7 - follow up (surgeon, community care nursing, ostomy nurse) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7Learning to care for your ostomy . . . . . . . . . . . . . . . .8 What is a pouching system? . . . . . . . . . . . . . . . . . . . .8 How long can I wear my pouch, and when should I change it? . . . . . . . . . . . . . . . . . . . . . . . . .9 When I change my pouch, how do I clean the skin and my stoma? . . . . . . . . . . . . . . . . . . . . . . .10Emptying your pouch . . . . . . . . . . . . . . . . . . . . . . . .11Bathing and showering . . . . . . . . . . . . . . . . . . . . . . .11Choosing your pouching system . . . . . . . . . . . . . . .12Supplies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12 Paying for your supplies . . . . . . . . . . . . . . . . . . . .12 BC Fair Pharmacare Plan. . . . . . . . . . . . . . . . . . . .12 Extended health benefits . . . . . . . . . . . . . . . . . . . .13 Ordering supplies . . . . . . . . . . . . . . . . . . . . . . . . . .13 Supplier information . . . . . . . . . . . . . . . . . . . . . . .13Considerations for daily living . . . . . . . . . . . . . . . . .14 Going out and about . . . . . . . . . . . . . . . . . . . . . . .14 Activities after surgery (first 6 to 8 weeks). . . . .14 Activities after surgery (after 8 weeks) . . . . . . .14 Going back to work . . . . . . . . . . . . . . . . . . . . . . . .14 When to get help after discharge . . . . . . . . . . . . . . .15
4
Skin irritation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15Preventing skin irritation. . . . . . . . . . . . . . . . . . . . . .16Treating skin irritation . . . . . . . . . . . . . . . . . . . . . . . .16Crusting technique, instructions. . . . . . . . . . . . . . . .16 Parastomal hernias . . . . . . . . . . . . . . . . . . . . . . . . . . .17 What is a parastomal hernia? . . . . . . . . . . . . . . . .17 Are you at risk for a parastomal hernia? . . . . . .17 What are signs of a parastomal hernia? . . . . . . .18 What should I do if I think I have a hernia?. . . .18 How do I prevent a parastomal hernia? . . . . . . .18Exercises to prevent a parastomal hernia . . . . . . . .19 Living with a parastomal hernia. . . . . . . . . . . . . . . .20Dietary considerations . . . . . . . . . . . . . . . . . . . . . . . .20 Ileostomy patients: food blockages . . . . . . . . . . . . .22 - signs of a partial and complete blockage chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22Dehydration. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23 What is dehydration? . . . . . . . . . . . . . . . . . . . . . .23 How to know when you are dehydrated . . . . . .23 How to prevent dehydration . . . . . . . . . . . . . . . .24Ileostomy: medications . . . . . . . . . . . . . . . . . . . . . . .24Colostomy irrigations. . . . . . . . . . . . . . . . . . . . . . . . .25 What to wear . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25Changing weight and your ostomy system . . . . . .25 Swimming and hot tubs. . . . . . . . . . . . . . . . . . . . . . .25 Intimacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26 Travel. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26 Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29“To do” list before coming to hospital for surgery . . . . . . . . . . . . . . . . . . . . . . . . back cover
Table of contents, continued
1
descending colon
sigmoid colonrectum
ascending colon
small bowel
anus
transverse colon
esophagus
stomach
large bowel
small bowel
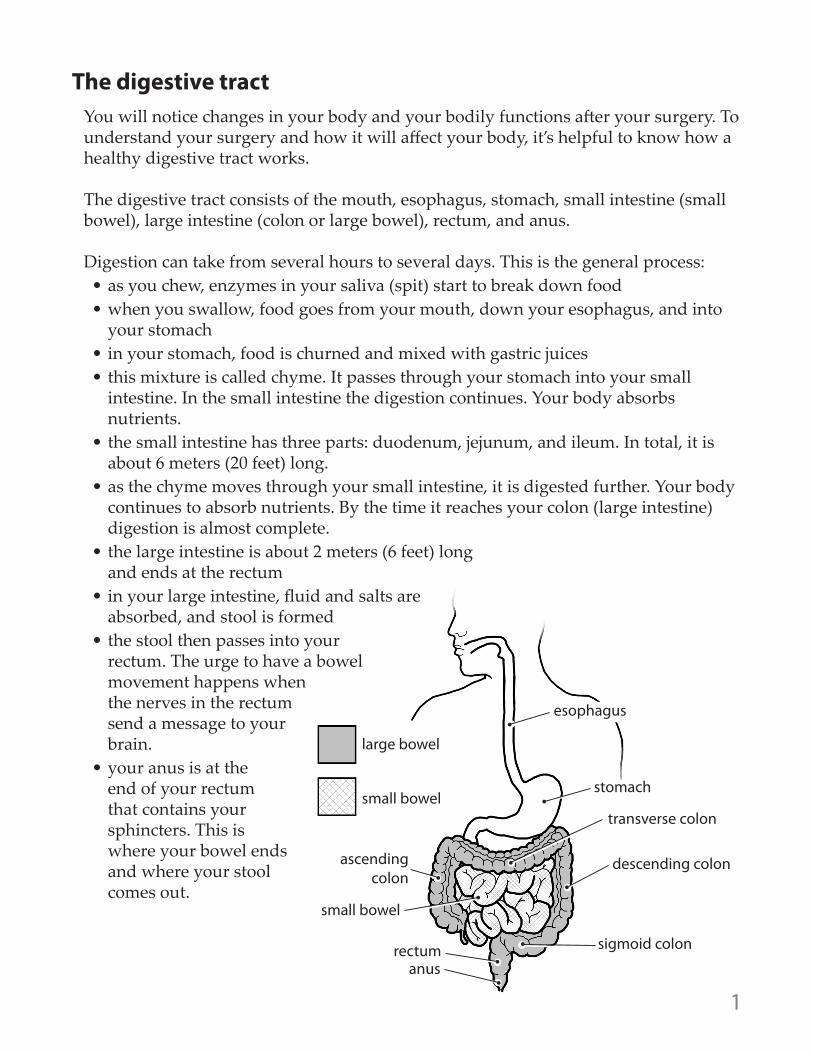
The digestive tract You will notice changes in your body and your bodily functions after your surgery. To understand your surgery and how it will affect your body, it’s helpful to know how a healthy digestive tract works.
The digestive tract consists of the mouth, esophagus, stomach, small intestine (small bowel), large intestine (colon or large bowel), rectum, and anus. Digestion can take from several hours to several days. This is the general process:• as you chew, enzymes in your saliva (spit) start to break down food• when you swallow, food goes from your mouth, down your esophagus, and into
your stomach• in your stomach, food is churned and mixed with gastric juices• this mixture is called chyme. It passes through your stomach into your small
intestine. In the small intestine the digestion continues. Your body absorbs nutrients.
• the small intestine has three parts: duodenum, jejunum, and ileum. In total, it is about 6 meters (20 feet) long.
• as the chyme moves through your small intestine, it is digested further. Your body continues to absorb nutrients. By the time it reaches your colon (large intestine) digestion is almost complete.
• the large intestine is about 2 meters (6 feet) long and ends at the rectum
• in your large intestine, fluid and salts are absorbed, and stool is formed
• the stool then passes into your rectum. The urge to have a bowel movement happens when the nerves in the rectum send a message to your brain.
• your anus is at the end of your rectum that contains your sphincters. This is where your bowel ends and where your stool comes out.
2
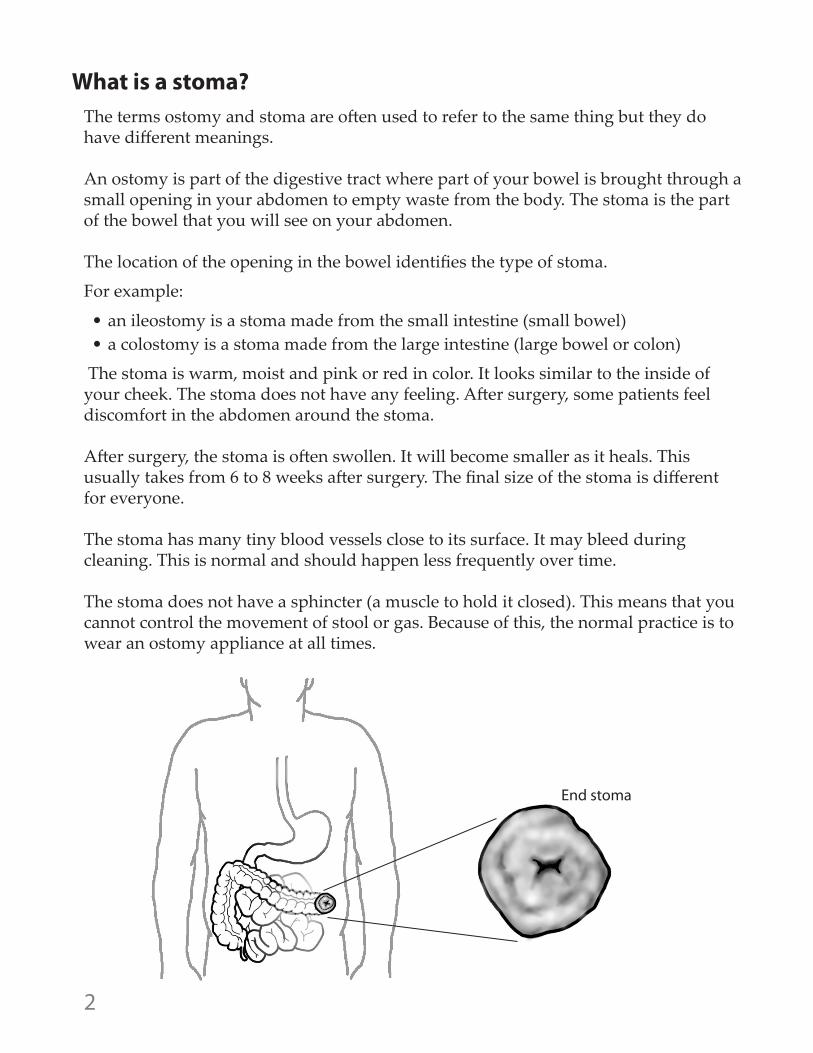
What is a stoma?The terms ostomy and stoma are often used to refer to the same thing but they do have different meanings. An ostomy is part of the digestive tract where part of your bowel is brought through a small opening in your abdomen to empty waste from the body. The stoma is the part of the bowel that you will see on your abdomen.
The location of the opening in the bowel identifies the type of stoma.
For example:
• an ileostomy is a stoma made from the small intestine (small bowel) • a colostomy is a stoma made from the large intestine (large bowel or colon)
The stoma is warm, moist and pink or red in color. It looks similar to the inside of your cheek. The stoma does not have any feeling. After surgery, some patients feel discomfort in the abdomen around the stoma.
After surgery, the stoma is often swollen. It will become smaller as it heals. This usually takes from 6 to 8 weeks after surgery. The final size of the stoma is different for everyone.
The stoma has many tiny blood vessels close to its surface. It may bleed during cleaning. This is normal and should happen less frequently over time.
The stoma does not have a sphincter (a muscle to hold it closed). This means that you cannot control the movement of stool or gas. Because of this, the normal practice is to wear an ostomy appliance at all times.
End stoma
3
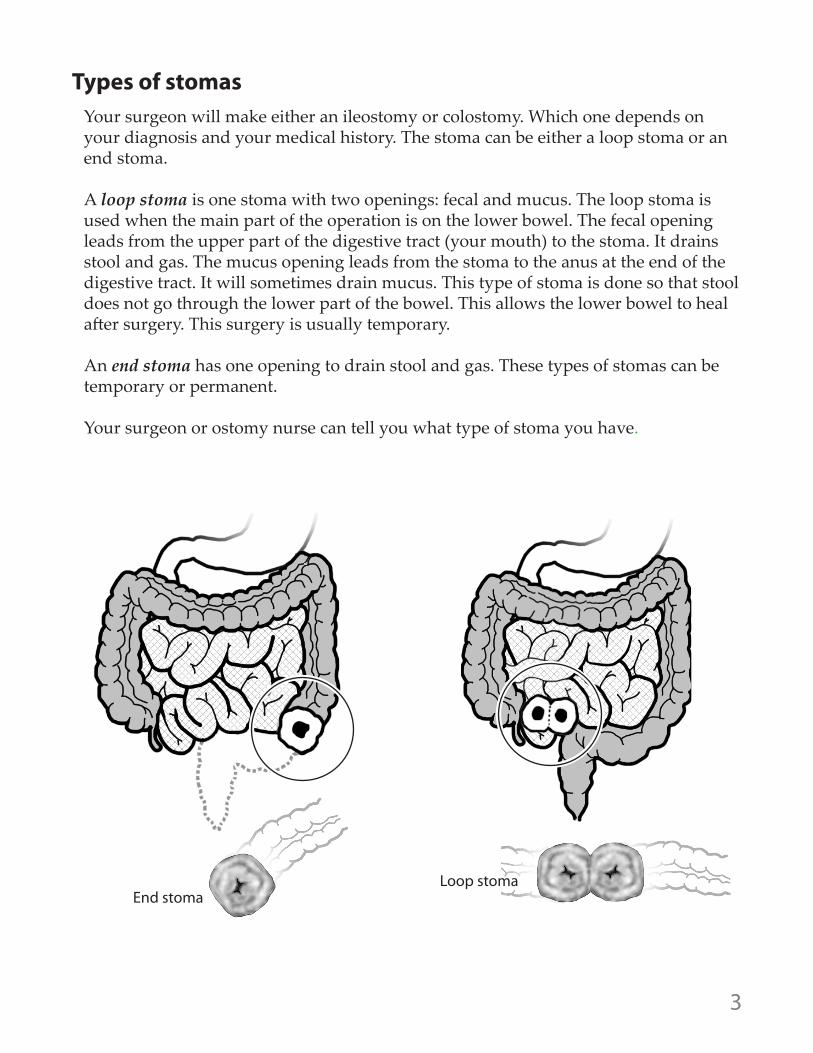
End stomaLoop stoma
Types of stomasYour surgeon will make either an ileostomy or colostomy. Which one depends on your diagnosis and your medical history. The stoma can be either a loop stoma or an end stoma.
A loop stoma is one stoma with two openings: fecal and mucus. The loop stoma is used when the main part of the operation is on the lower bowel. The fecal opening leads from the upper part of the digestive tract (your mouth) to the stoma. It drains stool and gas. The mucus opening leads from the stoma to the anus at the end of the digestive tract. It will sometimes drain mucus. This type of stoma is done so that stool does not go through the lower part of the bowel. This allows the lower bowel to heal after surgery. This surgery is usually temporary. An end stoma has one opening to drain stool and gas. These types of stomas can be temporary or permanent.
Your surgeon or ostomy nurse can tell you what type of stoma you have.
4
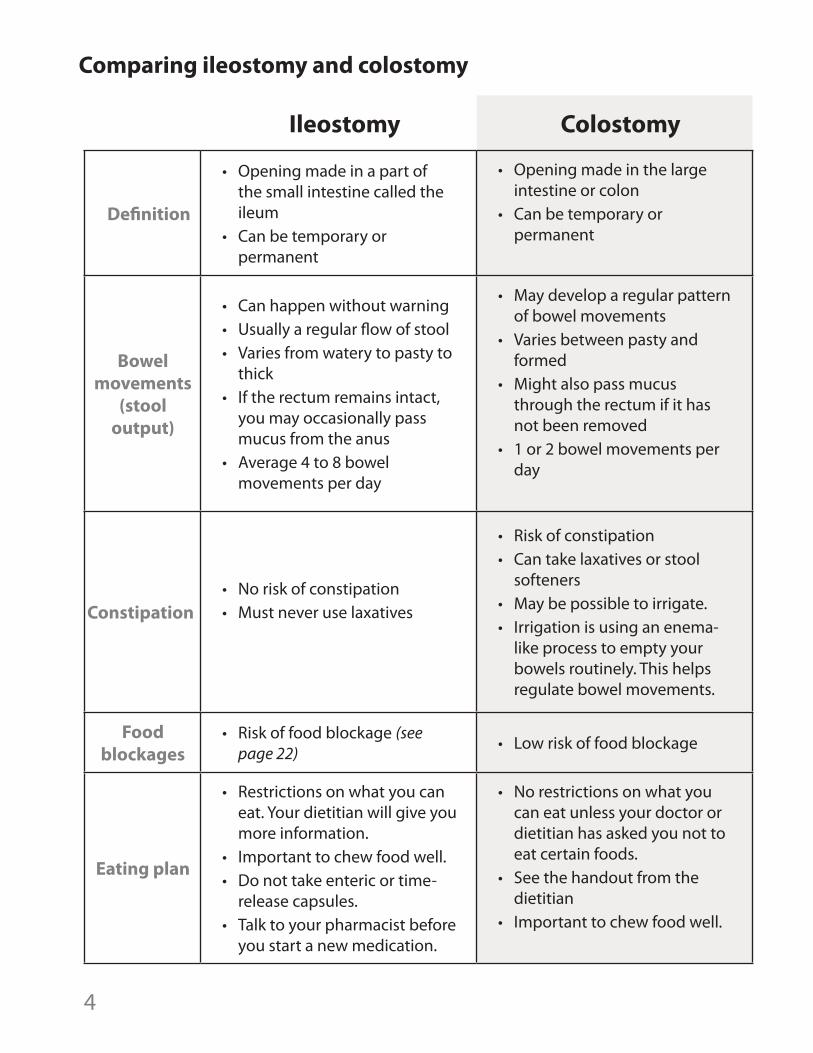
Comparing ileostomy and colostomy
Ileostomy Colostomy
Definition
• Opening made in a part of the small intestine called the ileum
• Can be temporary or permanent
• Opening made in the large intestine or colon
• Can be temporary or permanent
Bowel movements
(stool output)
• Can happen without warning• Usually a regular flow of stool • Varies from watery to pasty to
thick• If the rectum remains intact,
you may occasionally pass mucus from the anus
• Average 4 to 8 bowel movements per day
• May develop a regular pattern of bowel movements
• Varies between pasty and formed
• Might also pass mucus through the rectum if it has not been removed
• 1 or 2 bowel movements per day
Constipation• No risk of constipation• Must never use laxatives
• Risk of constipation• Can take laxatives or stool
softeners• May be possible to irrigate. • Irrigation is using an enema-
like process to empty your bowels routinely. This helps regulate bowel movements.
Food blockages
• Risk of food blockage (see page 22) • Low risk of food blockage
Eating plan
• Restrictions on what you can eat. Your dietitian will give you more information.
• Important to chew food well. • Do not take enteric or time-
release capsules. • Talk to your pharmacist before
you start a new medication.
• No restrictions on what you can eat unless your doctor or dietitian has asked you not to eat certain foods.
• See the handout from the dietitian
• Important to chew food well.
5
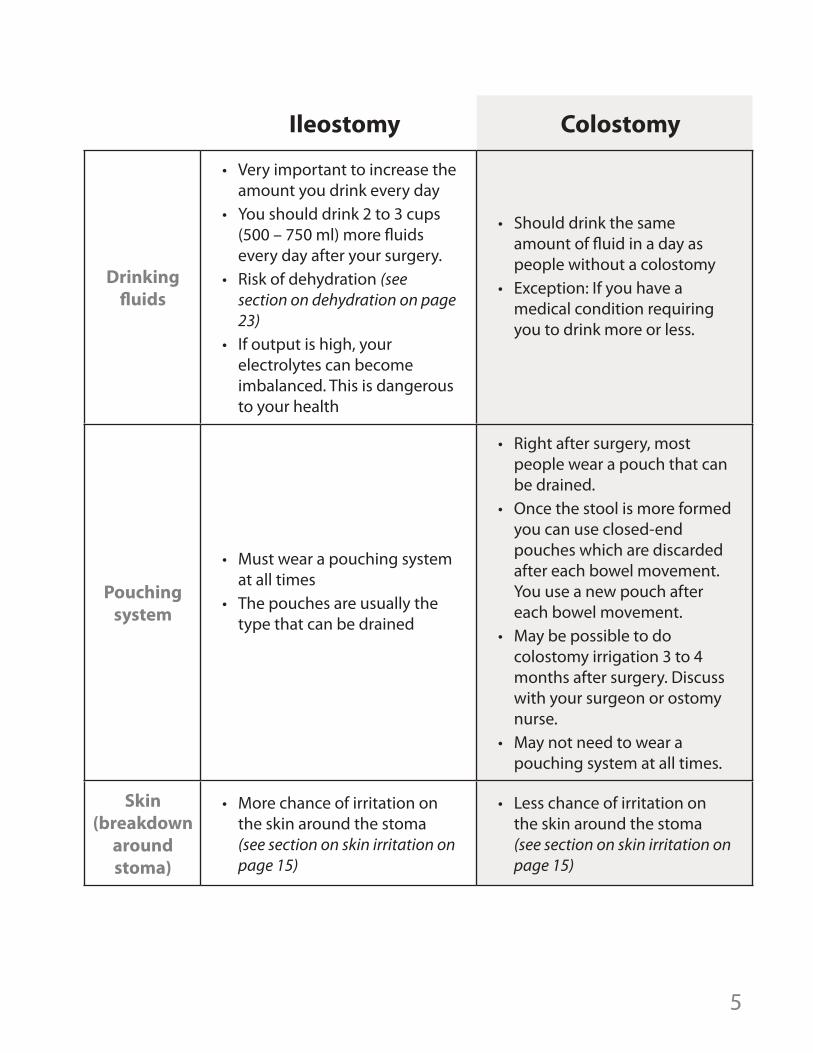
Ileostomy Colostomy
Drinking fluids
• Very important to increase the amount you drink every day
• You should drink 2 to 3 cups (500 – 750 ml) more fluids every day after your surgery.
• Risk of dehydration (see section on dehydration on page 23)
• If output is high, your electrolytes can become imbalanced. This is dangerous to your health
• Should drink the same amount of fluid in a day as people without a colostomy
• Exception: If you have a medical condition requiring you to drink more or less.
Pouching system
• Must wear a pouching system at all times
• The pouches are usually the type that can be drained
• Right after surgery, most people wear a pouch that can be drained.
• Once the stool is more formed you can use closed-end pouches which are discarded after each bowel movement. You use a new pouch after each bowel movement.
• May be possible to do colostomy irrigation 3 to 4 months after surgery. Discuss with your surgeon or ostomy nurse.
• May not need to wear a pouching system at all times.
Skin (breakdown
around stoma)
• More chance of irritation on the skin around the stoma (see section on skin irritation on page 15)
• Less chance of irritation on the skin around the stoma (see section on skin irritation on page 15)
6
Before your ostomy surgeryIf your surgery has been planned, your surgeon’s office may give you some general information with a pre-surgical ostomy kit. The kit will have some information on the surgery, an ostomy appliance and instructions. Many people find it is helpful to read the information and practice with the kit before their pre-admission clinic appointment.
Pre-admission clinic appointmentAt the pre-admission clinic you will meet with an ostomy nurse. They will go over your surgery and answer your questions about life with an ostomy. Some people find it helpful to bring a relative or friend. They can take notes, and help with asking questions.
The ostomy nurse will look at your abdomen to find the best placement of a stoma. They will mark your abdomen using a surgical pen. Your surgeon will use the marking to place your stoma. We will cover the ink mark with a waterproof dressing. If the mark disappears before surgery, please tell the hospital staff on the day of the surgery.
After surgery In the operating room at the end of surgery, we will put a pouching system over the stoma. Nurses and doctors will check your stoma and make sure the pouching system is intact.
Immediately after surgery, the health care team will start working with you on your recovery. We will give you medication to relieve pain. We will help you with deep breathing and coughing exercises. We will show you how to use a “pillow splint” when you cough or sneeze. You are encouraged to move and walk usually within the first 24 hours. We will ask you to chew gum to stimulate your digestive system. You still start by eating fluids only, then easy to digest food, and then your regular diet as tolerated.
Your ostomy will start working slowly after surgery. The first signs that your bowels are starting to work are passing gas and then loose stool through the stoma.
As you start eating solid food, and the bowel adapts to its new shape, the gas should become less noisy. The stool should become more formed.
If your anus and rectum have not been removed, you may still feel the urge to have a bowel movement. Mucus or old stool may be passed from the rectum. This is normal and will continue occasionally.
If your rectum has been removed, you will have an incision and possibly a drainage tube. The nurses will care for this and provide teaching when you are ready for discharge.
7
Going home from hospitalEach person recovers differently after surgery. You will know you are ready to go home when:
• your pain is manageable with pills (oral medication only)• you can eat and drink comfortably• you are able to do your activities of daily living to the same level as before your
surgery• there is no sign of complication• you (or your designated care person) are able to manage your ostomy
Support after you go home
Follow up
1. Surgeon: You will see your surgeon from 2 to 6 weeks after you go home. If you do not have an appointment before you leave the hospital, call your surgeon’s office to make one. Always bring a spare pouching system to any appointments with your surgeon or doctor. They may wish to take off the pouch to check the condition of your stoma. If you have a colostomy, you may wish to discuss the option of bowel irrigation with your surgeon at your follow up visits.
2. Community care nursing: You will have follow up support from community nursing starting 3 or 4 days after you leave the hospital. If you can walk, the community care nurses may ask you to attend a clinic in your area. If you are unable to walk to a clinic, they will arrange a home visit. Community care nursing will continue until you are confident and independent with your ostomy care.
3. Ostomy nurse: The hospital ostomy nurse will help you find an ostomy nurse in your community. This may be through a hospital clinic, an outpatient clinic, a medical supplier or a pharmacy. We recommend that you make an appointment with a community ostomy nurse in 3 to 6 weeks after surgery. You should see the ostomy nurse anytime you have leaking or skin issues. It is also a good idea to see an ostomy nurse at least once each year. They will assess your pouching system to make sure it is still the best option for you. Your community ostomy nurse may also be able to answer your questions regarding the possibility of colostomy irrigation.
8
Learning to care for your ostomyBy the time you leave the hospital, you should know:• how to take care of your ostomy• physical limitations and activity after bowel surgery• diet and fluid requirements• medication requirements • when and where to get ostomy supplies • when and where you can see an ostomy nurse • when you should get help or go to an Emergency Department
Most people are ready to go home in about 3 to 7 days. During this time, we will teach you how to care for your stoma. The ostomy nurse will go over the different pouch systems with you. We will help you select choose the system that will work best for you. You will learn how to empty, and change the pouching system.
The ostomy nurse will help you adapt to having an ostomy. They will teach you how to prevent skin problems around the stoma. You will also learn how to treat skin problems if they develop. Finally, the ostomy nurse will help you order your first set of ostomy supplies and connect you with community resources for continued support.
Many people find it very helpful to have family or a caregiver join these lessons. This is especially helpful if you think you will need help. You, a family member or a caregiver will need to be independent with ostomy care before you leave the hospital.There will be support systems set up for you when you go home. Community nursing support and private ostomy nursing services may be available to help until you are feeling confident and independent with your care. There is more on this in the “Going home from hospital” section of the booklet (page 7).
What is a pouching system?A pouching system or ostomy appliance is used to collect stool and gas. The pouch is designed to control odor. It also protects the skin around the stoma.
There are many types of pouching systems. The ostomy nurse reviews these with you and helps choose the one that will be best for you. Sometimes you have to try different systems to find the one that works best.
9
Pouching systems are odor-proof, water-resistant, lightweight and low profile. They are not noticeable through clothing. They do not break down. They cannot be flushed down the toilet.
The pouching system has two basic parts. The first is the flange (or wafer). This part sticks to the skin. The second part is the pouch (or bag). This part collects the stool.
Pouching systems can be:• drainable or closed-ended• one-piece or two-piece• pre-cut, moldable or cut-to-fit
After your surgery, you will wear a clear pouching system with no filter over your stoma. This allows hospital staff to monitor your stoma and stoma output. The pouching system you go home with may be different.
The stoma usually shrinks for 6 to 8 weeks after surgery. Measure your stoma once a week before cutting the flange. This will help you cut the right size. Once your stoma has finished shrinking, you should see an ostomy nurse to be refitted.
How long can I wear my pouch and when should I change it ?Different people wear the pouching system for different lengths of time. We call this “wear time.” On average the wear time for an ileostomy system is 3 to 5 days. For a colostomy system, it is 5 to 7 days. If you are not experiencing any leaks or skin irritation with your pouching system, you can try wearing it for longer. Most ostomy manufacturers recommend wearing a pouching system for no more than 7 days.
You must change your pouching system at the first sign of a leak to avoid skin issues.
Signs of a leak include:• skin that looks red, raw or weepy• stool on your skin• stool on the back of the flange.
It is impossible to patch a leaking pouching system. It must be changed. If you do not change it the skin around the stoma may be damaged. If you continue to have leaks or skin issues you may need to be refitted for a different type of pouching system by an ostomy nurse.
Flange or wafer
Pouch
10
How long can I wear my pouch and when should I change it?, continued
If your skin becomes red, raw and weepy, your ostomy nurse may recommend a “crusting procedure” (see page 16). You may need to change your pouching system more often until the skin has healed.
You may need to change your pouching system more often:• in hot weather• with increased exercise or sweating• after swimming• after going in a hot tub.
The best time of day to change a pouching system is when the bowel is less active. This is usually first thing in the morning before you eat or drink. You will get to know your body and when the best time is for you.
When I change my pouch, how do I clean the skin and my stoma? As stated above, you will change your pouching system between 3 to 5 days for an ileostomy and 5 to 7 for a colostomy. You should also change it immediately if you suspect it is leaking.
Check your skin every time you change the appliance. It’s also a good idea to check it when you have a shower without your pouch on. The skin around the stoma should look like the skin on the rest of your abdomen. It should not be red or irritated. If you have concerns about the skin around your stoma, make an appointment to see an ostomy nurse.After you remove the pouch, clean your stoma and skin. Use a paper towel and soft cloth and warm water only. Do not use anything else.• Do not use baby wipes or store-bought cleansers. They can leave a residue that
irritates your skin. This residue will also stop the flange from sticking. • Do not use creams or moisturizers (including medicated creams) around the
stoma. They can stop the flange from sticking. • Never use rubbing alcohol. Alcohol strips the natural oils from your skin. This can
lead to skin irritation and skin damage.• There are products specially designed for the skin around the stoma, such as
adhesive remover or ostomy powder. Do not use these unless the ostomy nurse tells you to use them.
11
If you have a lot of hair on the skin around the stoma, you will need to shave. If your skin is smooth the flange will stick better. It will hurt less when you take off the flange. Shaving also helps prevent infection of the hair shaft caused by wearing the flange. An electric razor is the best method for avoiding ingrown hairs. Some people dry-shave using ostomy powder and a disposable razor. You can also do a wet shave with water only. Do not use shaving cream, oil or lotion. They leave a residue that can irritate your skin.
Always pat your skin dry before putting on your pouching system.
Emptying your pouchYou’ll learn how to empty your pouch before you leave the hospital. The nurses will help you until you are able to do it yourself. The more practice you get in the hospital, the more comfortable you will be when you go home.
Empty your ostomy pouches when they are 1/3 to half full. A pouch that is more than half full can pull on the flange and leak. A very full pouch is difficult to empty without a mess.
If you are mobile:• sit on the toilet with your bottom near the back of the seat. You can also sit facing
the back of the toilet. • place some toilet paper in the toilet bowl to prevent splashing• take off the pouch. Hold the drainable end upward and open the pouch.• when you are ready, lower the end of pouch into the toilet bowl and drain the
contents• wipe the inside edge of the pouch with a tissue to clean it. Then wipe the outside
edge before you close it.• close the pouch and reattach it
Bathing and showeringYou can have a bath or shower with your pouching system on. You can also take it off if you prefer. The pouching system is water-resistant when you wear the flange with the pouch attached. It is not water resistant if you wear the flange without the pouch.
After you bathe or shower, dry the outside of the pouching system. Use a towel or a hair dryer on a cool setting.
When you bathe, do not use soap, bath oils or lotions on the skin around your stoma. They may stop your pouching system from sticking.
12
Supplies
Paying for your suppliesOstomy supplies are not covered by British Columbia Medical Services Plan (BCMSP). Supplies can be expensive. Your ostomy nurse will work with you to make sure you have all the information you need about purchasing and paying for your supplies before you go home.
BC Fair Pharmacare PlanBC PharmaCare helps B.C. residents with the cost of eligible prescription drugs, and certain medical supplies and pharmacy services. It provides assistance through several drug plans. The largest is the income-based Fair PharmaCare plan.
Register for Fair Pharmacare before your surgery date. If you don’t, you may have to pay for your supplies.
The BC Fair Pharmacare Plan might pay for some or all of your ostomy supplies. The amount Pharmacare pays depends on your annual income. Pharmacare uses income information from your tax return two years ago. If your current annual income is 10% less than it was two years ago, contact Pharmacare to review the amount the plan covers. You can also ask to have your deductible be spread out over 12 months.
For more information or to register for Fair PharmacareTelephone: 1-800-663-7100 or 604-683-7151http://www2.gov.bc.ca/gov/content/health/health-drug-coverage/pharmacare-for-bc-residents
Choosing your pouching systemYour pouching system needs can change over time. While in hospital, your ostomy nurse will suggest a system that works best for your stoma and body type. You may need something different once your stoma and abdomen are healed. If you gain or lose weight, you might need a different system.
See an ostomy nurse if you have problems with leakage, skin irritation or odor. You should also see a nurse if you are getting less than 24 to 48 hours of wear from your pouching system.
Ostomy manufacturers are continually developing new pouching systems and products for skin management. Many manufacturers offer free trials of pouching systems. Ask your ostomy nurse if you are interested in seeing what is new.
13
Extended health benefitsIf you have extended health benefits, these benefits may pay part of the cost. Check with your extended health provider for details about your coverage and how to make a claim.
Other sources of ostomy supply coverage: Let your ostomy nurse know if you get any of these health benefits:
• Veterans Affairs• Non-Insured Health Benefits (NIHB) Program• Income assistance• Disability assistance
You might get some extra help paying for supplies. You may also qualify for a limited amount of free supplies through some of the ostomy manufacturers. Discuss this with your ostomy nurse.
Ordering suppliesYour ostomy nurses will give you options about how to buy your supplies. Before you leave the hospital, they will order a 2 to 4 week supply through a pharmacy, medical supplier or manufacturer based on your preference. Supplies can be delivered to your hospital room or to your home.
We recommend that you see an ostomy nurse from 2 to 4 weeks after discharge. The ostomy nurse will help you buy more supplies. Your stoma and abdomen may change shape after you leave the hospital. We will give you a list of locations where you can see an ostomy nurse.
Supplier informationYou can order ostomy supplies from pharmacies or medical suppliers. Check with your local provider about their services. Many medical suppliers carry a large selection of ostomy products and deliver for free within BC in 1 or 2 business days.
If you prefer to order from a local pharmacy, find out how long it will take to bring in your ostomy system. Sometimes it can take up to two weeks. It is necessary to order your supplies well before you run out.
Some medical suppliers have ostomy nurses who provide free consultation and support for their customers. Call for details or ask your ostomy nurse for more information.
14
Considerations for daily living
Going out and aboutAlways carry a spare pouching system with you or leave one in your car. Many people carry an emergency zipper-lock bag that holds pouching supplies, paper towels and a garbage bag.
Activities after surgery (first 6 to 8 weeks)It is important to increase your activity gradually. For the first 6 to 8 weeks, avoid strenuous activities such as lifting, vacuuming or golfing. Do not lift, pull, or push anything more than 5 to 10 pounds. Do not do any heavy lifting or straining. Light activities such as walking will help your healing. Your surgeon will advise you when you can return to your other activities. If doing something makes you uncomfortable, stop right away.
Talk to your surgeon about any specific limits. Coughing, sneezing, and straining all put pressure on your abdomen. To support your abdominal muscles, hold a pillow or your hands firmly against your abdomen when you cough or sneeze. Regular physical exercise such as walking and swimming will strengthen your abdominal muscles. This kind of exercise is also good for overall health and wellness.
Activities after surgery (after 8 weeks)After your recovery period, you can usually return to the activities you enjoyed before surgery. People with ostomies enjoy all sorts of activities including skiing, golf, tennis, waterskiing, swimming, softball, hiking, etc. There are many devices that you can use to protect your stoma and adapt to various activities. Talk to your ostomy nurse about what is available.
Going back to workYour surgeon will let you know when you can go back to your regular activities. Most people are able to return to work or school 4 weeks after surgery.
If your regular activities involve lifting or physical straining, talk to your ostomy nurse about hernia prevention. You may need to wear a special belt to help prevent a hernia.
15
When to get help after discharge
Go to your nearest hospital emergency department immediately if you notice any of these signs:
• signs of extreme dehydration. These include increased thirst, dry mouth, decreased urine output and fatigue. You may even have leg cramps, muscle cramps and loss of appetite if your electrolytes become imbalanced.
• excessive bleeding from the stoma or where the stoma joins the skin• excessive prolonged output from the stoma (more than 1250 ml or 5 cups in 24
hours)• severe abdominal cramps lasting more than 2 to 3 hours• continuous nausea and vomiting• no ileostomy output for 4 to 6 hours accompanied by cramping and nausea• severe watery discharge lasting more than 5 to 6 hours • severe or unusual odor that may indicate an infection• a deep cut in the stoma• severe swelling of the stoma
If you go to Emergency, always bring a bag of your preferred ostomy supplies. Hospitals carry a very limited range of ostomy supplies, and may not have your specific appliance.
Skin irritation Sometimes the skin around the stoma can become irritated. This can be caused by:
• taking off the pouching system incorrectly• poor fit of the pouching system• leakage of stool under the flange• sensitivity to products• moisture
If you experience skin irritation that does not go away within a week, contact an ostomy nurse for assistance.
Skin can become irritated by touching stool. This is more common for people with an ileostomy. Liquid stool has a high level of digestive enzymes. These enzymes help break down food. When they touch your skin, they start to break it down. This causes irritation and burning. This is less of a problem for people with a colostomy. By the time the stool reaches the large bowel, only a small amount of digestive enzymes remains.
16
Crusting Technique
1. Clean the skin around your stoma with warm water using a soft cloth or paper towel.2. Dry the area with a soft cloth or paper towel. 3. Apply a light dusting of ostomy powder over raw, weeping skin.4. Brush off excess powder with a tissue or paper towel. This keeps the powder from
clumping.5. Blot or spray the irritated skin with skin sealant. (Note: these are special wipes.
They are not the same as alcohol wipes.)6. Wait about 15 to 30 seconds for the area to dry. 7. Repeat these steps a second time.
Change the pouching system every 2 or 3 days until the skin heals. Repeat these steps every time you change the pouch until the skin is healed and healthy. Once your skin is healed, stop using the crusting technique.
Preventing skin irritationIf the skin around your stoma becomes open, red, raw, or weepy, your pouching system may not stick properly. This can lead to leaks which irritate your skin even more. See your ostomy nurse for help with any skin issues.
To prevent irritation, be sure to cut the opening of your flange no more than 2 to 3 mm (1/8 to ¼ inch) larger than your stoma. If the opening is too large, it exposes too much skin to stool. If it is too small, you might not get a good seal and stool could leak under the pouching system. Your ostomy nurse can help you find the right size.
If your pouching system leaks, the best thing to do is to change it as soon as possible. Do not reinforce it. This can trap stool under the flange and cause more irritation. If the problem continues see an ostomy nurse.
Sometimes people need to wear an ostomy belt to keep your pouching system snug to your abdomen. You also may need some accessory products such as wipes, rings, or paste. Talk to your ostomy nurse about what you need.
Treating skin irritationWhen you have raw, open, weeping skin, use the crusting technique described on the next page. This helps create a dry skin surface for the appliance. It also helps your skin to heal under the flange.
Only use the crusting technique when your skin becomes irritated, raw, and moist. Do not use this technique if your skin is red.
17
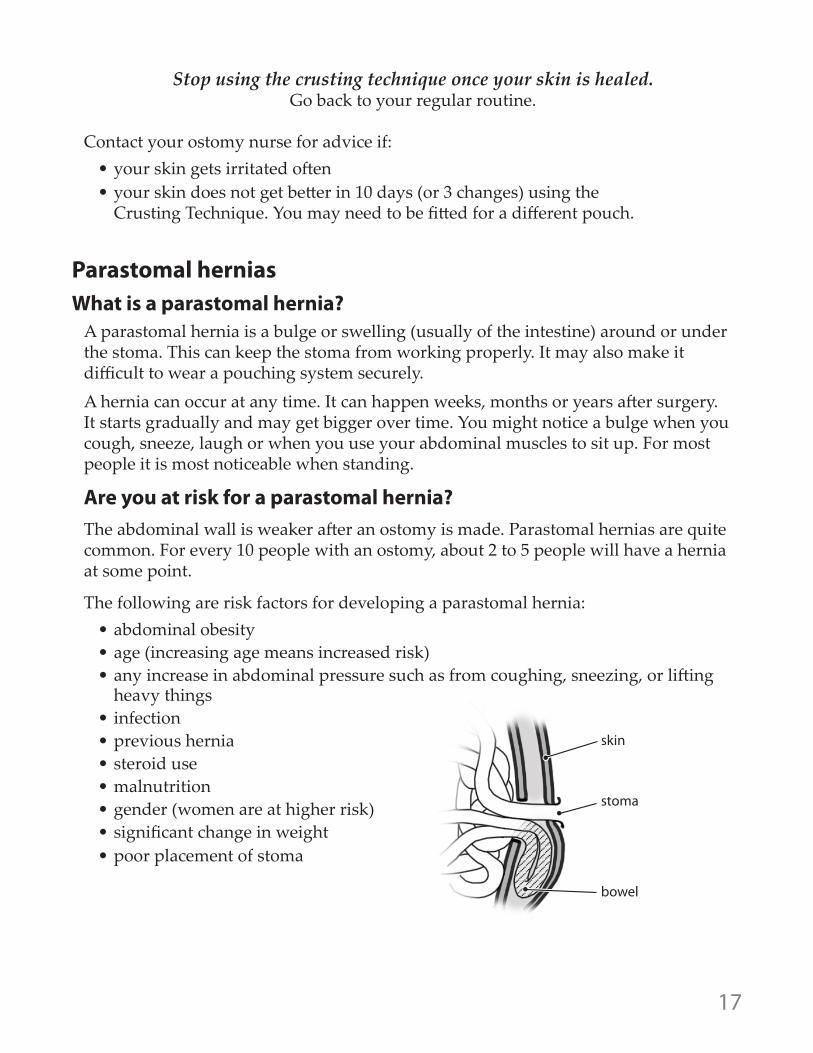
skin
stoma
bowel
Parastomal herniasWhat is a parastomal hernia?
A parastomal hernia is a bulge or swelling (usually of the intestine) around or under the stoma. This can keep the stoma from working properly. It may also make it difficult to wear a pouching system securely. A hernia can occur at any time. It can happen weeks, months or years after surgery. It starts gradually and may get bigger over time. You might notice a bulge when you cough, sneeze, laugh or when you use your abdominal muscles to sit up. For most people it is most noticeable when standing. Are you at risk for a parastomal hernia? The abdominal wall is weaker after an ostomy is made. Parastomal hernias are quite common. For every 10 people with an ostomy, about 2 to 5 people will have a hernia at some point.
The following are risk factors for developing a parastomal hernia: • abdominal obesity• age (increasing age means increased risk)• any increase in abdominal pressure such as from coughing, sneezing, or lifting
heavy things • infection• previous hernia• steroid use • malnutrition• gender (women are at higher risk)• significant change in weight• poor placement of stoma
Stop using the crusting technique once your skin is healed. Go back to your regular routine.
Contact your ostomy nurse for advice if:• your skin gets irritated often• your skin does not get better in 10 days (or 3 changes) using the
Crusting Technique. You may need to be fitted for a different pouch.
18
What are signs of a parastomal hernia?• swelling or ‘bulge’ on your abdomen around your stoma. The swelling may flatten
when you lie down and increase while you stand or move around.• a dull aching, heaviness, bloating, or ‘dragging’ sensation around your abdomen
especially with standing • sometimes hernias may not have any symptoms
What should I do if I think I have a hernia? See your ostomy nurse or surgeon. You may need to have the flange refit to the changing shape of your stoma. Talk to your surgeon or your ostomy nurse about clothing that is comfortable, gives support, and can possibly prevent the hernia from getting larger. You may need to be fitted for a hernia belt or binder.
If the hernia becomes painful and hot with reduced stool output, and does not soften and move back into your abdomen when you lie flat, go to the nearest hospital emergency department.
How do I prevent a parastomal hernia? For the first 2 to 3 months after surgery:
• support your abdominal area with a pillow or your hands when you cough or sneeze
• do not lift, push or pull anything that weighs more than 10 pounds • do not do anything that involves heavy lifting or straining
There are things you can do to reduce your risk: • stop smoking• maintain a healthy diet • do regular physical exercise such as walking and swimming• talk to your ostomy nurse about wearing a hernia belt when you do heavy lifting/
work
Included here are specific exercises that strengthen your abdominal muscles (your core). These are key exercises in preventing a parastomal hernia. The ostomy nurse may also recommend other exercises.
You can usually start doing these exercises 2 months after your surgery.
19
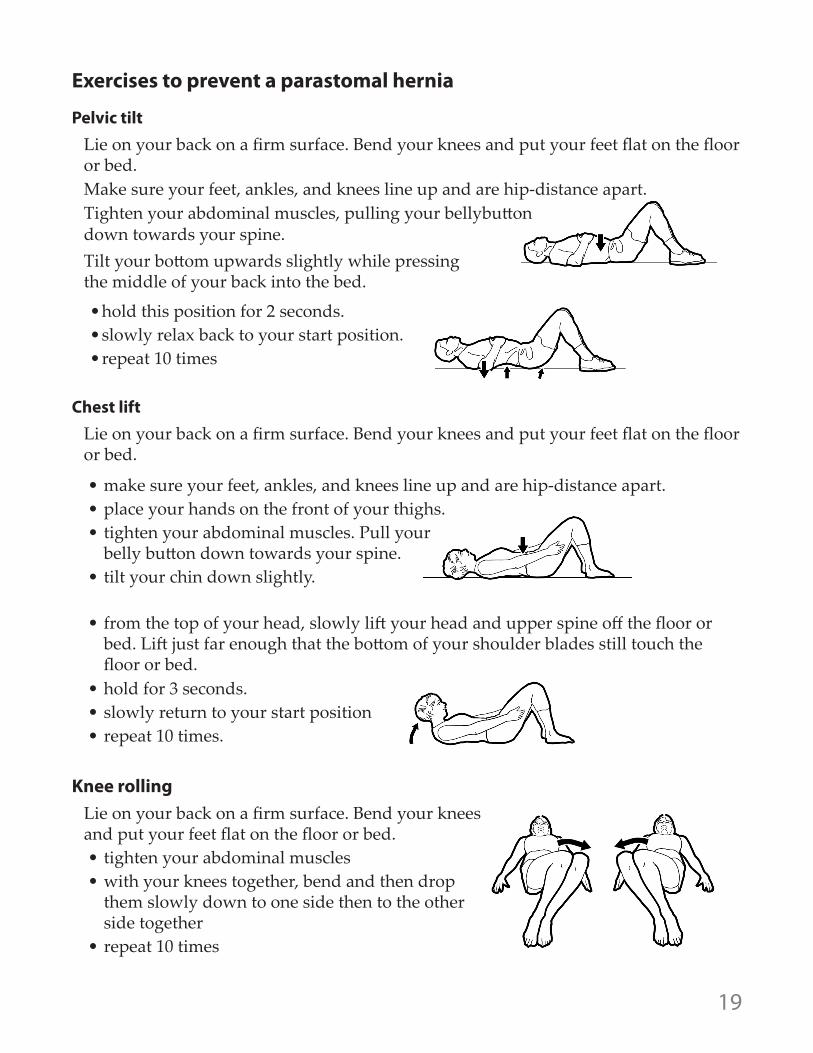
Exercises to prevent a parastomal hernia
Pelvic tiltLie on your back on a firm surface. Bend your knees and put your feet flat on the floor or bed.Make sure your feet, ankles, and knees line up and are hip-distance apart.Tighten your abdominal muscles, pulling your bellybutton down towards your spine. Tilt your bottom upwards slightly while pressing the middle of your back into the bed.
• hold this position for 2 seconds.• slowly relax back to your start position.• repeat 10 times
Chest lift Lie on your back on a firm surface. Bend your knees and put your feet flat on the floor or bed.
• make sure your feet, ankles, and knees line up and are hip-distance apart.• place your hands on the front of your thighs.• tighten your abdominal muscles. Pull your
belly button down towards your spine.• tilt your chin down slightly.
• from the top of your head, slowly lift your head and upper spine off the floor or bed. Lift just far enough that the bottom of your shoulder blades still touch the floor or bed.
• hold for 3 seconds.• slowly return to your start position• repeat 10 times.
Knee rollingLie on your back on a firm surface. Bend your knees and put your feet flat on the floor or bed.• tighten your abdominal muscles• with your knees together, bend and then drop
them slowly down to one side then to the other side together
• repeat 10 times
20
Living with a parastomal herniaFor many people, the stoma will still work properly with a parastomal hernia. Some people may be concerned about the appearance of their parastomal hernia. If your ostomy is temporary your surgeon will often suggest having the hernia surgically repaired when the ostomy is reversed. This decreases the risks from another operation. If your ostomy is permanent your surgeon might suggest you have the hernia surgically repaired.
Call your doctor or ostomy nurse right away if:• you have a large amount of pain or• your bowels have stopped moving (no stool output)
When you have a parastomal hernia, there is a small risk that part of the bowel could become kinked or twisted. This can cause the bowel to be obstructed or perforated. You would need surgery right away to fix this.
Dietary considerationsA dietitian will work with you after surgery. They will teach you about any changes you may need to make to your diet. They will give you an education booklet to take home.
The following section applies to both ileostomy and colostomy patients. Special considerations that are specific to your ostomy will be outlined afterward by your dietitian.
Excessive gasIf you find that you have too much gas, you can eat fewer gas-forming foods. You can also eat them at times when gas production is not a concern to you.
Foods that may promote gas formation:• dried peas and beans• melons• eggs• beer and carbonated beverages (pop)• onions and related vegetables• strong cheeses such as Roquefort• vegetables of the cabbage family: broccoli, brussels sprouts,
cabbage, turnip and cauliflower• dairy products (if you are lactose intolerant)
To help decrease gas formation:• chew your food well• do not chew gum• do not use drinking straws• try not to talk with food in your mouth
21
OdorCertain foods can make odors worse. If you have an issue with food-related odors, you may want to avoid these foods. You might also choose to eat them at times when you are less concerned about odor.
Foods that promote odor:• fish• eggs• onions• garlic• dried peas and beans• asparagus• fried foods• vegetables of the cabbage family: broccoli, brussels sprouts,
cabbage, turnip and cauliflower
Some foods can help you control odor:• parsley• yogurt and buttermilk
If odor is a concern, consult with a dietitian, ostomy nurse or your doctor for suggestions.
22
People with a colostomy are not likely to get a food blockage. People with an ileostomy are at higher risk. The small intestine can be slightly narrowed near the stoma. Undigested food can stick in this narrowed place and cause a blockage. This stops the normal passage of stool. It can be very uncomfortable. If the blockage continues it can be a medical emergency.
How to Prevent Blockages: Choosing the right foods can reduce your risk of a blockage. The dietitian will talk to you about what you eat and how you eat. It is important to chew your food well.
Signs of a partial blockage What to do
• thin, clear liquid stool with bad smelling odor (looks like ‘dishwater’)
• cramping• abdominal pain• abdominal swelling
(bloating)• stoma swelling
• remove the flange and replace with a slightly larger opening to accommodate any swelling of the stoma.
• do not eat any solid food. Take only sips of liquids• take a warm bath. This may relax your stomach muscles and
the blockage may dislodge. • massage the area around your stoma• try a ‘knees to chest’ position (fetal position). This may
dislodge the blockage. • if the blockage does not dislodge within 3 to 4 hours, call your
community ostomy nurse or doctor. If you cannot reach them, go to the nearest emergency department.
Signs of a complete blockage What to do
• no stool output for over an 8 hour period during waking hours when eating normally.
• stoma swelling• cramping• abdominal pain• nausea• vomiting
Try the things listed above and:• do not eat or drink anything if you are nauseated or vomiting.• go to the nearest emergency department if your symptoms
do not go away. You may need to have your ileostomy irrigated until the obstruction is passed.
Symptoms of a food blockage include:• no drainage at all• draining only watery fluid• abdominal pain• cramping• swelling of your stoma and
abdomen
The table below outlines signs and symptoms of blockages, and things you can do when you notice them.
Ileostomy patients: food blockages
23
DehydrationIf you have an ileostomy, you have a greater chance of becoming dehydrated.
What is dehydration?Dehydration (sounds like dee-hi-dray-shun) is when a person’s body does not have enough fluids. Your body needs a certain amount of water to work properly. Your body absorbs most of the fluids and electrolytes (like sodium and potassium) it needs in the large intestine. If you have an ileostomy, the stool does not go into the large intestine. Your body cannot absorb the fluids and electrolytes. This means you have a greater chance of becoming dehydrated. Dehydration is not usually a problem with a colostomy.
When you have an ileostomy, it is especially important to pay attention to how much fluid you are drinking. It’s important to avoid dehydration and imbalances in your sodium and potassium levels. These can cause serious side effects like leg cramping, confusion, etc. If you become severely dehydrated, you may need to be treated in an emergency room. In some cases, you may even need to stay in the hospital until the body fluids are back in normal range. To learn more about fluid and electrolyte needs with an ileostomy, please refer to the handout given to you by the hospital dietitian.
How to know when you are dehydratedIf you have mild dehydration you might not notice any symptoms. As dehydration gets worse you may notice you are feeling thirstier.
Other signs:
• dry mouth• headache• feeling tired and jittery• agitation or irritability • cramps in your muscles, especially in your legs• urine is darker than usual. You urinate less often and smaller amounts than
normal.• feeling dizzy when you stand up or sit up
24
Ileostomy: medicationsHaving an ileostomy means that you may need to change some of your medications. It is a good idea to go over all your medications with your doctor and pharmacist. This includes birth control pills and all non-prescription medications. Most medications can be taken safely following ileostomy surgery. Some types of medications may pass into the pouch without being absorbed by your system. This includes time-release or enteric-coated tablets. If you find a pill or a part of a pill in the pouch, contact your doctor or pharmacist. This is important because you may not be fully absorbing your medicine. You may need to take a different medication that can be absorbed.
Never take stool softeners or laxatives. They can result in diarrhea. This can cause severe dehydration and electrolyte imbalance.
Remind your doctor and pharmacist about your ileostomy before you start a new medication. Talk to them if you have any concerns. Carry a list of your prescribed medications with you at all times in case of emergency.
How to prevent dehydrationYou need to drink more fluid than you did before your surgery. Most people need to drink at least 500 to 750 ml (2 to 3 cups) more every day. The exact amount of extra fluid you need to drink depends on your ileostomy output. Please discuss your individual fluids needs with your dietitian especially if you have diabetes, heart disease, kidney disease or issues with fluid retention.
Caffeinated beverages and alcohol actually remove fluids from your body. Do not use them to meet your fluid needs. Sugary beverages (including certain sports drinks, pop and juices) may actually increase your ileostomy output. This can make dehydration worse. Please refer to the handout from the dietitian for more information about what you should drink and how much.
You may want to keep track of how much stool you have in a day to make sure you are not becoming dehydrated. Average ileostomy amounts are 500 to 1000ml/day. If you have more than 1250 ml/day (5 to 6 cups/day) please call your dietitian or your ostomy nurse. They can help you figure out what is triggering your high output. They can also help you get enough fluids and manage your output.
Drink more liquids if you: • have signs of dehydration (see previous page for symptoms)• do activities that make you sweat more than usual • have diarrhoea (looser or higher ileostomy output) • find yourself someplace with hot weather
Dehydration, continued
25
Colostomy irrigationsSome people with a colostomy may choose to manage their output by colostomy irrigation. Irrigation is similar to a regular enema. With irrigation, water is put into the bowel through the stoma. This removes stool from the colon. Irrigation is not appropriate for everyone. Talk to your surgeon to see if it will work for you. If this option is right for you, the ostomy nurse will teach you how to irrigate. Irrigation is not appropriate for people who have an ileostomy.
What to wearPouching systems are lightweight and discreet. Many of them are low profile and not noticeable through clothing. Your pouch will probably not be visible when worn beneath undergarments. It also helps to empty the pouch when it is no more than 1/3 full. Many people find that small changes to their clothing make it more comfortable to wear the pouching system.
These adjustments may include:• avoiding tight belts directly over the stoma.• wearing waistbands above or below the stoma.• adding a soft, absorbent pouch cover to keep plastic away from the skin.• wearing specialty undergarments that cover and support the pouching system.
These are made from soft elastic or Lycra ® for comfort.
There are many clothing options for people with an ostomy. See the Resources section of this booklet or talk to your ostomy nurse about what might be available. Changing weight and your ostomy system
When you gain or lose weight, the shape of your body can change. When your body shape changes, your ostomy system may leak. If this creates a problem with ostomy management, contact an ostomy nurse for advice.
Swimming and hot tubsOnce your incision is completely healed, you can resume swimming, and using hot tubs and saunas. Spending a lot of time in the water can loosen the adhesive seal on your flange. You may need to replace your pouching system more often.
26
IntimacyPeople may have concerns about sexual relationships after an ostomy. An open discussion with your partner will help in your adjustment. If you are comfortable, you can also talk with your surgeon, family doctor or ostomy nurse for advice. If you are not comfortable talking about this issue, you may be able to find tips or support online.
Sexual intimacy may be resumed when you feel physically and emotionally ready. It takes time to adjust to the changes in your body.If the rectum has been removed, there may be nerve damage in the perineal area. This can cause sexual impairment. This may be temporary or permanent. Discuss your concerns with your surgeon.
Here are some things you can do to be more comfortable with intimacy:
• empty your pouch before sexual activity• put on a smaller “mini” pouch or fold and tape your pouch• cover the pouch with a pouch cover, cummerbund, lingerie or an undershirt• try different positions that are comfortable for you and your partner
if you have ongoing concerns, you might find it useful to speak with a professional specializing in sexual counseling. Ask your family doctor or surgeon for a referral.
Travel Travel may require some extra planning. Here are some things to think about:
• take at least twice as many supplies as you would normally use. You may not be able to purchase what you need.
• protect your supplies from heat and/or cold• keep some supplies in your carry-on luggage in case your checked luggage is lost• contact the Canadian Association of Enterostomal Therapists (CAET) or the
United Ostomy Association of Canada (UOAC) about available resources in the area you plan to visit (See Resource List)
• observe water precautions. If you cannot drink the water, do not use the water to irrigate your colostomy.
• if flying, ask for an aisle seat near the washroom• print a copy of the United Ostomy Association Travel Card and carry it with
you when you travel. This card is a discreet way of communicating your privacy needs at airports, airplanes or border crossings.
• when riding in a vehicle, protect the stoma from the seat belt. You can put a small pillow or soft foam padding over the stoma to protect it.
27
GlossaryAbdomen - stomach, stomach area, belly,
tummy
Absorb - to take in or soak up
Anus - normal opening through the rectum where stool leaves the body
Blockage - when the bowel is blocked either with waste or the bowel is twisted or pinched off
Bowel - also called intestine and colon. It is the part of the digestive tract that lies between the stomach and the anus. There are two parts, the small intestine and the colon (large bowel). Often these words are used interchangeably
Bowel movement - the waste left after your body has absorbed nutrients and fluids from what you eat and drink. Also called stool or feces
Colon - part of your digestive system called the large bowel or large intestine (sounds like coal-on)
Colostomy - from ‘colon’, meaning large bowel, and ‘ostomy’, meaning opening
Dehydration - condition resulting from excessive fluid loss
Digestion - to digest or breakdown food so it can be used by the body
Electrolytes - minerals your body needs to work properly. For example: sodium, potassium, calcium and magnesium are all electrolytes
End stoma - a single ostomy with one opening to drain feces. Can be permanent or temporary
End stoma with rectal stump - where the lower part of colon is closed and left in place. This part of the colon is stapled or sewn closed. The piece left is called a rectal stump. If temporary, a second surgery is done to reconnect the two ends. This second surgery is also called a Hartmann’s resection
Esophagus - the tube that carries food, fluids, and saliva (spit) from your mouth to your stomach
Enzymes - substances in the mouth, stomach and small intestine that break down food. Stool contains these enzymes. If the stool stays on your skin the enzymes in it will irritate your skin
Diverticulitis - a diverticulum is an abnormal little pouch in the lining of any hollow organ of the body. In the colon (large bowel), these may become inflamed and cause diverticulitis. This condition may require surgery
Fecal - containing feces or stool
Feces - waste from the bowel. Also called bowel movements, stool, or excrement
Hernia - when a part of an internal organ bulges through a weak area of muscle
Ileostomy - from ‘ileum’ (ill-ee-uhm), meaning small bowel, and ‘ostomy’, meaning opening
28
Inflammatory bowel disease - inflammation of the bowel. Symptoms vary, depending on the area of the bowel affected and the degree of inflammation. Both ulcerative colitis and Crohn’s disease are inflammatory bowel diseases
Irrigate - to run water into or through something. Related to colostomy, this is a way to regulate bowel movements. It allows you to empty the bowel at a set time by running water into the bowel through the stoma
Large intestine - also called the large bowel. This is the last part of your digestive system, between the small intestine and the anus. This is where your body absorbs water from food waste
Loop stoma - a single ostomy with two openings. Feces comes out of one opening and mucus comes out of the other. Usually temporary
Ostomy - a surgically created opening into the digestive or urinary system. The opening diverts stool or urine from its normal route. Sometimes the word ostomy is used as a shortened version for the word colostomy
Ostomy nurse - nurses who have special education to help them work with patients who have an ostomy. Also called enterostomal therapy nurses, ET nurse, wound ostomy continence nurse (WOCN), or stoma nurse
Perineal - the area between the genitals and the anus (rectum)
Pouching system - flange and pouch. These are used to contain the output from the colostomy
Reflexes - nerve messages which you cannot control. These messages are sent by something that triggers them. For example, when doctor taps your knee with a small hammer-like tool, your knee will jump upwards. This is a reflex
Small intestine - also called the small bowel. This is the longest part of your digestive system. It does most of the digesting and absorbing of food
Sphincter - ring of muscles around the anus that holds stool in the large bowel
Stoma - the part of the bowel that is seen outside the body after ostomy surgery
Stool -waste from the bowel. Also called bowel movements, feces, or excrement
Stool output - amount of waste from the bowel
Trauma - injury or damage (e.g. a broken arm or ruptured spleen)
Glossary, continued
29
Resources Useful ostomy websites
United Ostomy Association of Canada • http://www.ostomycanada.ca/ • Handbook for New Ostomy patients
o United Ostomy Association Vancouver Chapter www.vcn.bc.ca/ostomyvr
o United Ostomy Association Fraser Valley www.geocities.com/coqcon
o Vancouver United Ostomy Association: http://uoacvancouver.weebly.com/
United Ostomy Association Travel Cardhttp://www.ostomy.org/Ostomy_Travel_Tips.html
Canadian Medic Alert® Foundation Inc.
• Toll Free (English): 1-800-668-1507• Toll Free (French): 1- 800-668-6381• Web Site: www.medicalert.ca
Canadian Association for Enterostomal Therapy (CAET)
• Phone: 905-270-8433• Web Site: www.caet.ca
Canadian Society of Intestinal Research (Bad Gut Society)
• Toll free: 1-800-600-4875• Web Site: www.badgut.com
Colorectal Cancer Association of Canada• www.ccac-accc.ca
Crohn’s and Colitis Foundation of Canada
• Toll free: 1-800-387-1479• Web Site: www.ccfc.ca• Friends of Ostomates Worldwide
(FOW)• www.fowc.ca
International Association for Medical Assistance to Travellers
• Phone: 1-416-652-0137• Web Site: www.iamat.org• International Ostomy Association• www.ostomyinternational.org
J-Pouch Group the Source for J-Pouch Surgery
• www.j-pouch.orgJ-Pouch Unite and J-Pouch Group are support groups on Facebook
Meet an Ostomate
• http://www.meetanostomate.org/
Ostomy Land: Ostomy Support Community
• ostomyland.com (and facebook page)
Information on Sexuality
• www.uoaa/org/ostomy_info/pubs/ uoa_sexuality_en.pdf
30
Ostomy supplies: manufacturer websitesManufacturer’s websites can be a wealth of knowledge. They provide the information you would expect about their product lines. But they also provide education, educational links, resources and information on up and up-coming events.
• www.coloplast.ca• www.convatec.ca• www.cymedostomy.com• www.hollister.com • www.marlenmfg.com• www.nu-hope.com• www.salts.co.uk
Colo-Majic Liners
• Colo-Majic liners work with most 2 piece ostomy pouching system. • 1-866-611-6028• http://www.colomajic.com/
Hernia Support Belt
• http://nu-hope.com/
Osto-EZ-Vent
• The Osto-EZ-Vent is an additional vent that allows for quick release of air build-up in a non-filter ostomy pouching system.
• http://www.kemonline.com/content/home/
Ostomy clothing
Intimate Moments www.intimatemomentsapparel.com (based in the USA)
Joeies Custom Ostomy Garment http://joeies.com/ (based in Vancouver, BC)
Ostomy Secretshttps://www.ostomysecrets.com/ (based in the USA)
Stealth Belthttp://stealthbelt.com/ (based in the UK)
Vegan Ostomy Clothingwww.veganostomy.ca (based in Canada)
Weir Comfeeshttp://weircomfees.com/ (based in Canada)
31
Notes
A
P P ROVEDPATI
ENTThis material has been reviewed and approved by patients, families and staff.
32
This material is for informational purposes only. It does not replace the advice or counsel of a doctor or health care professional. Providence Health Care makes every effort to provide information that is accurate and timely, but makes no guarantee in this regard.
You should consult with, and rely only on the advice of, your physician or health care professional. The information in this document is intended solely for the person to whom it was given by the health care team.
For more copies, go online: http://phc.eduhealth.ca or email: [email protected]
and quote catalogue no. FK.235.Os7.PHC ©Providence Health Care
www.providencehealth.bc.ca
“To do” list before coming to hospital for surgery
£ Read this booklet and write down any questions
£ Check your medical coverage for ostomy supplies. Sign up for Fair Pharmacare if you have not already. (see page 12). Ostomy supplies are not covered by the British Columbia Medical Services Plan (BCMSP). After surgery, the hospital will provide your supplies until you go home.
£ Pack a bag to bring to hospital. Bring:
£ comfortable clothes with loose waistbands
£ slippers with non-slipping tread (optional but recommended)
£ this booklet
If you already have an ostomy,
£ please bring your ostomy supplies with you
£ If you received an ostomy pre-surgical practice kit please review the materials in the kit. Practice with the ostomy appliance. Write down any concerns or questions. You can talk to your ostomy nurse at the hospital.