Embed Size (px)
Citation preview
Carers NSW Biennial ConferenceMarch 2011
Making Caring Countthe cost and value of caring.
Jane HallProfessor of Health Economics
Centre for Health Economics Research and Evaluation
University of Technology Sydney
Outline
• Counting – the importance of unpaid work• Costing - Approaches to costing informal care• Valuing - How should informal care be valued
– Understanding benefits and costs– Some research
• Policy – what we need to know
Counting carers
• 18% Australians have a disability that affects their daily activities– Almost 1 in 5
• 12% Australians are carers for someone with a disability of aged over 60– 1 in 8
• 13% of women and 11% men are carers– 1 in 7-8 women; 1 in 9 men
Source ABS Survey of Disability, Ageing and Carers 2009
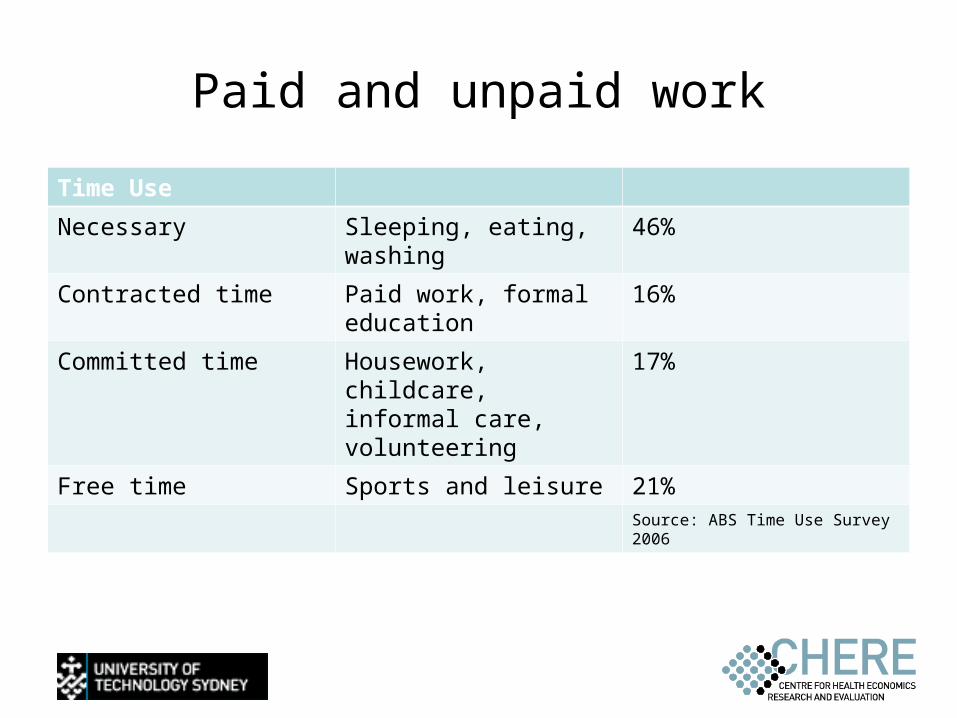
Paid and unpaid work
Time Use
Necessary Sleeping, eating, washing
46%
Contracted time Paid work, formal education
16%
Committed time Housework, childcare, informal care, volunteering
17%
Free time Sports and leisure 21%Source: ABS Time Use Survey 2006
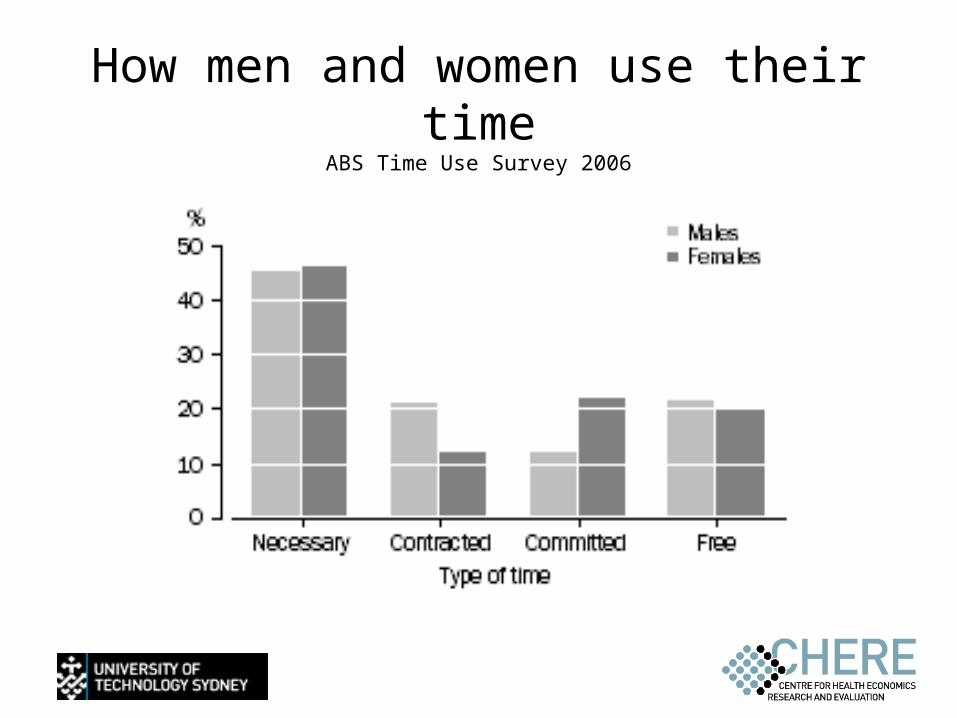
How men and women use their time ABS Time Use Survey 2006
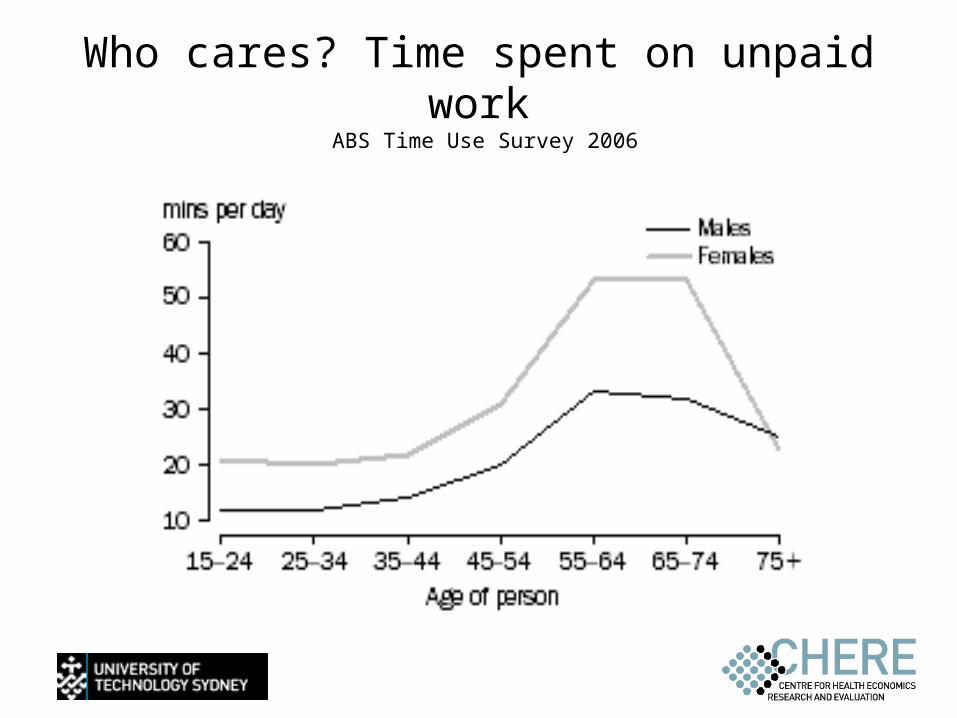
Who cares? Time spent on unpaid work ABS Time Use Survey 2006
Counting for Nothing
• Informal care traditionally seen as a free resource
• So moving from institutions to home care is seen as a cost saving
• But– Time of carers (direct input)
• Van den Berg and Spauwen 2006, and others
– Reduces paid employment or education• Ettner 1996, Carmichael and Charles 2003,
– Reduces pay• Heitmuller and Inglis 2007
Effects of caregiving are complex
Negative• Physical and mental health• Finances• Social life and leisure
Positive• Satisfaction with role• Altruism• Reciprocity
What’s it worth?Approaches to valuing informal care
• Proxy method– Hours of care = what you would have paid for them– Implies perfect substitution– Assumes paid care is available
• Opportunity cost method– Hours of care = what you would have been paid– Ignores difficulty of different tasks– Ignores why carers care
• Both focus on cost not benefit
Why is this important• Many health care programs are assessed by
considering costs and benefits• Ignoring costs and benefits of carers leads to
under estimates and invalid comparisons• Focussing only on costs
– Current methods probably under-estimate
• Benefits or consequences may be positive and negative– Spillover effects– Altruistic gains
Well-being research
• More large scale surveys include a question on happiness or life satisfaction
• Subjective measure of experience• Generally used
– Income, unemployment, family situations, inflation.
• Higher income is associated with higher wellbeing
• So lower wellbeing can valued as drop in income
Wellbeing losses due to caregiving in Australia: current work
• HILDA panel data• Representative sample, surveyed 2001-06• Data set includes
– life satisfaction, – living arrangements, – income, employment, – provision of informal care, – health-related quality of life (SF-6D)
• 16,984 individuals 2,729 carers
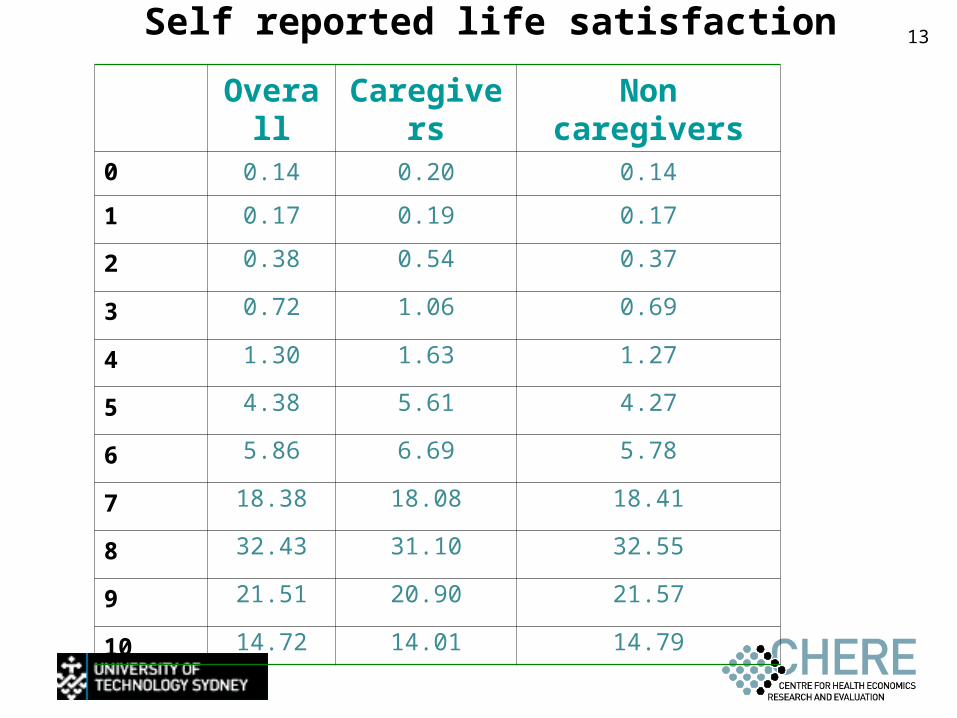
13Self reported life satisfaction
Overall Caregivers Non caregivers0 0.14 0.20 0.14
1 0.17 0.19 0.17
2 0.38 0.54 0.37
3 0.72 1.06 0.69
4 1.30 1.63 1.27
5 4.38 5.61 4.27
6 5.86 6.69 5.78
7 18.38 18.08 18.41
8 32.43 31.10 32.55
9 21.51 20.90 21.57
10 14.72 14.01 14.79
What affects satisfaction?
• Positives– Income– Health – Married/partner– Working part-time
• Negative– Unemployed/Working full-time– Children
Informal care
• Reduces wellbeing by 0.07 (-10 scale)– Small but significant
• Caregiving, not hours of care• Impact
– Income effect $325 per week– Health effect 0.04 QALY
Preferences research:
• Stated preferences: individuals’ choices in hypothetical scenarios tell us about their preferences
• Moves from a rating scale to exploring trade-offs• Allows for ‘non-market’ situations• Increasingly used to explore health and health
care
Assessing carers’ preferences in palliative care: recent research
• Palliative care is a special situation but not often studied
• Sample of informal carers of community palliative care – 82 in descriptive phase– 168 high care (72) and low care (96) in preference
study
• Data collection– Face-to-face interviews– Various methods
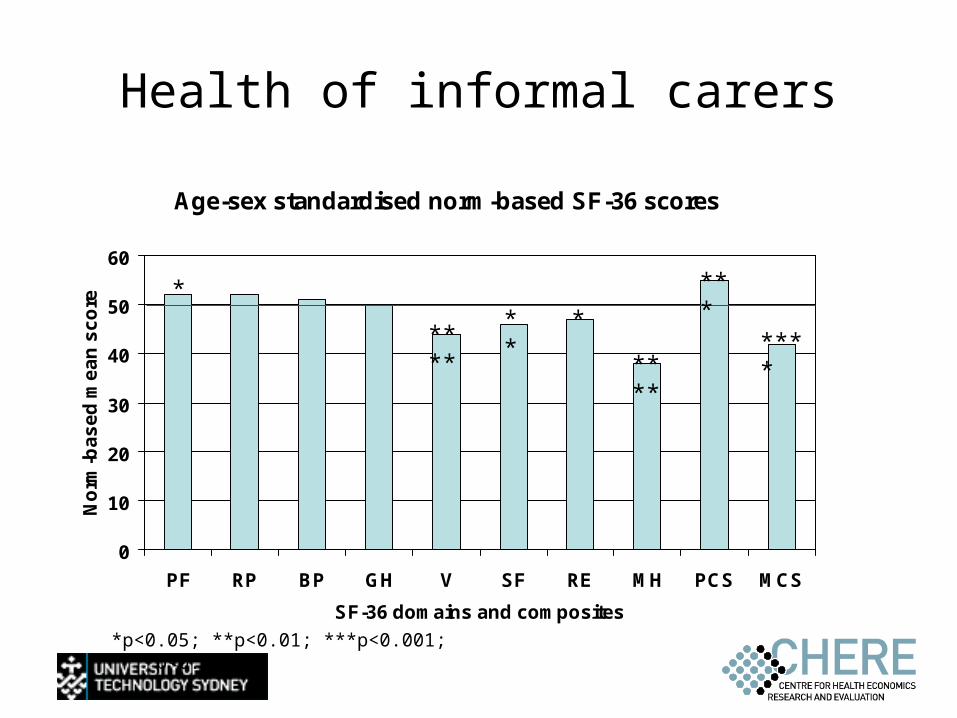
Health of informal carers
Age-sex standardised norm-based SF-36 scores
0
10
20
30
40
50
60
PF RP BP GH V SF RE MH PCS MCS
SF-36 domains and composites
No
rm-b
as
ed
me
an
sc
ore
*
****** *
****
***
****
*p<0.05; **p<0.01; ***p<0.001; ****p<0.0001.
Impact of caring
• Emotional - negative & positive• Sports/hobbies/interests• Social life/relationships/family• Holidays/travel• Work• Physical health• Finances
Negative emotional impacts
Emotional exhaustion
“I am her nurse, her cook, her driver, her cleaner. In other words I replace everybody including the nurse because I [am] giving her also the injections …. I am completely exhausted, not physically as much as the other way”
Frustration, takes over life
“It’s my father and I love him and I’ll do it, but ….it’s stopping your normal life, like what you normally do and it can become quite frustrating at times. Your life changes completely”
Neglect own emotional health
“I think I don’t look after my emotional well-being well enough. I think that’s one thing that I just let slip. The time thing - can I actually fit in - no I can’t, you know and so that’s when people have given me names of counselors, that’s the sort of thing I push to the back of the priorities”
Positive emotional impacts Satisfaction “Well, I wouldn’t have wanted anyone else to care for her and I think we
believe we’re doing a good job and it helps us you know. At least we know that we’ve done all we can for her. So there is satisfaction yeh”
Giving something back
“My mother’s had a terrible life really as far as family goes so it’s great to give her something back in her lifetime you know”
Benefits of home-care “It gives me pleasure. She is my mother and she looked after me, and
my kids. It’s the least I can do. It is better for her to be at home. I can give her extra care and comfort. I know what she likes. I can play her special music, arrange her so she is comfortable, cook and serve her food I know she likes”
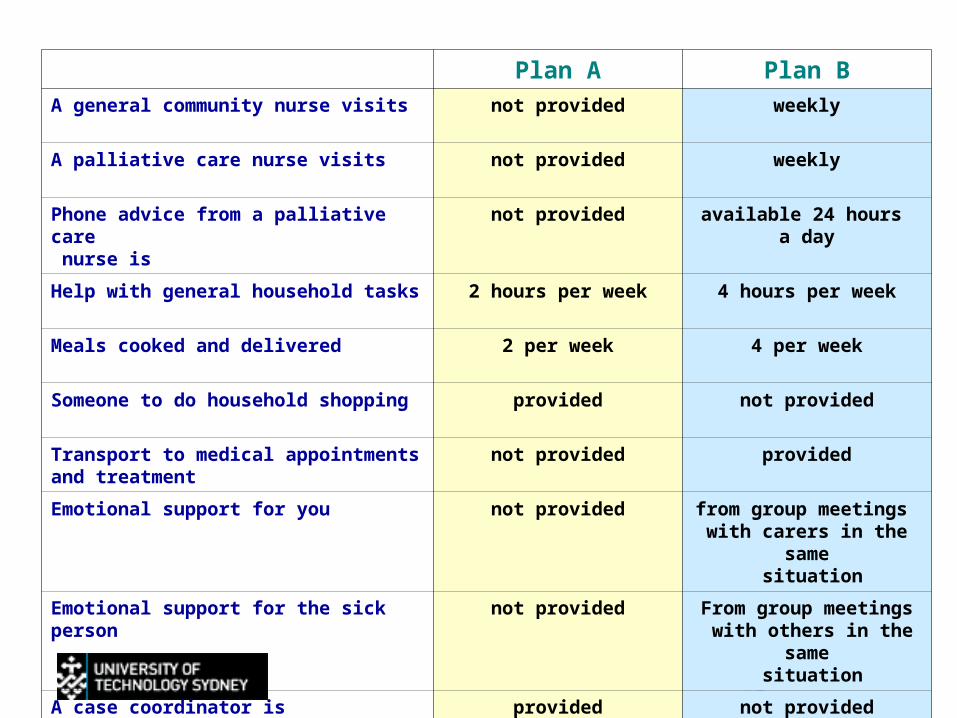
Plan A Plan BA general community nurse visits not provided weekly
A palliative care nurse visits not provided weekly
Phone advice from a palliative care nurse is
not provided available 24 hours a day
Help with general household tasks 2 hours per week 4 hours per week
Meals cooked and delivered 2 per week 4 per week
Someone to do household shopping provided not provided
Transport to medical appointments and treatment
not provided provided
Emotional support for you not provided from group meetings with carers in the same
situation
Emotional support for the sick person not provided From group meetings with others in the same
situation
A case coordinator is provided not provided
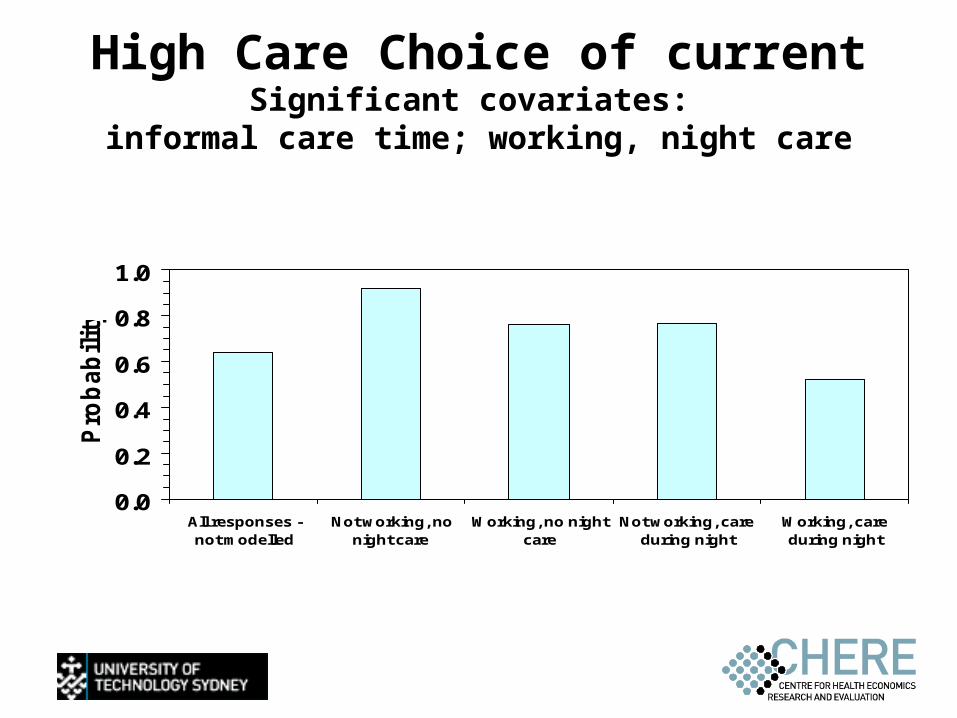
High Care Choice of currentSignificant covariates:
informal care time; working, night care
0.0
0.2
0.4
0.6
0.8
1.0
All responses -not modelled
Not working, nonight care
Working, no nightcare
Not working, careduring night
Working, careduring night
Pro
bab
ilit
y
Summary
• Informal carers value– Palliative Care nurse visits– 24 hour access to PC nurse phone advice– Community nurse visits
• High Care– Personal care assistant, shopping & home respite
• Low Care– Domestic help, transport, emotional support carer & a case
coordinator
• Threshold effects• Carers don’t want to be replaced!
Conclusion
• Importance of counting– Out of the count, out of mind
• Value of caring activity– The right values are needed to evaluate policy
• Impact of caring– Understanding needed to make good policy