Embed Size (px)
Citation preview

Caregiving and Trauma Spectrum Disorders
Gregory Fricchione MD
Associate Chief of Psychiatry
Director
Benson Henry Institute for Mind Body Medicine
Massachusetts General Hospital
Professor of Psychiatry
Harvard Medical School
Disclosure
• Johns Hopkins University Press--royalties
Objectives
• Review the concepts of stress and resiliency
• Introduce an evolutionary neuromedicine approach to trauma spectrum disorders (TSD)
• Review the diagnoses of TSD, e.g., PTSD and TBI.
• Suggest that trauma represents a separation threat.
• See our caregiving mission as fostering the re-discovery of attachment solutions, which form the foundation for human resiliency and health for our patients, their families and ourselves.
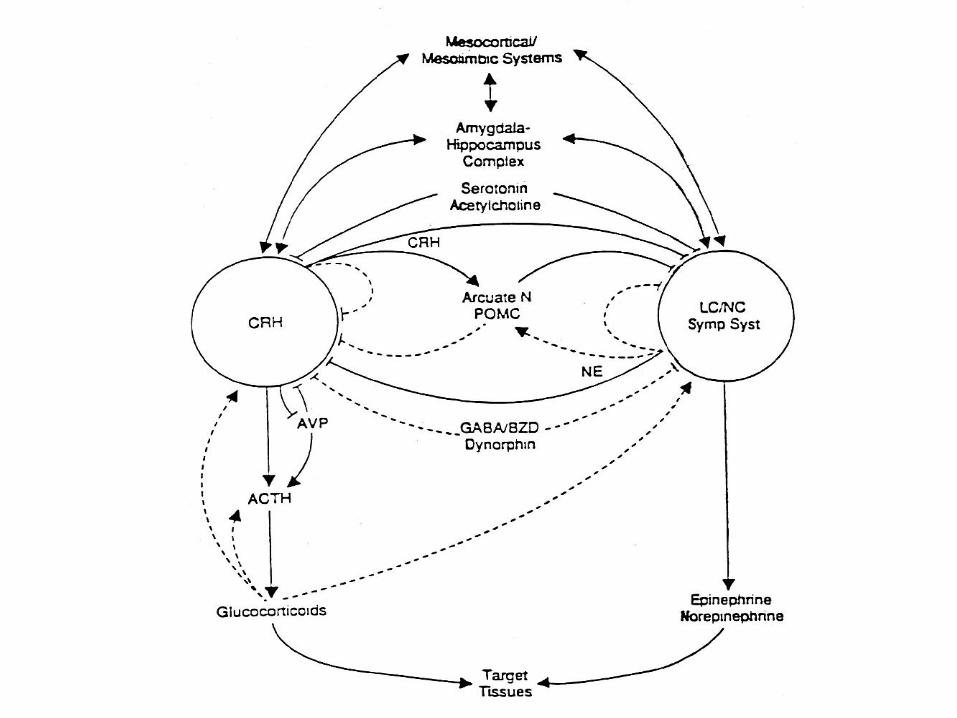
Stress
• Challenge-Stimulus-Hyperarousal, state with physiological, behavioral,
psychological adaptations required of the organism
• Stress Emergency/Fight-Flight Response: amygdala-lateral hypothalamus-locus coeruleus-SNS (Walter B. Cannon 1914, 1915)
• General Adaptation Syndrome: mesolimbic-PVN of hypothalamus-
pituitary adrenal thyroid (Hans Selye 1950s)
Inflammatory Stress Response:
Infection-unrelated inflammatory changes in the microglia of the
mediobasal hypothalamus activates NF-kB metabolic syndrome
(Zhang et al, Nature, 2013)
Chronic social isolation stress activates NF-kB in rat PFC (Zlatkovic and Filipovic, 2013)
• Ghrelin-GH axis can trigger stress-induced vulnerability to enhanced fear memory in the amygdala. (Meyer et al. 2013)
• Distress secondary to acute overwhelming stress or chronic unremitting stress is pathogenic (arousal pathology)
+
PVN LC
Why Brain Evolution?
• Niko Tinbergen (1963): 4 distinct questions when
examining any biological or psychological phenomenon;
always involve mechanism and ontology; function and
evolution:
• How does it work? (mechanism-current)
• How did it develop? (developmental-historical)
• What is it for? (mechanism-current)
• How did it evolve? (developmental-historical)
Primordial Intelligence
• Sense the environment
• Analyze incoming data
• Effect a motor response: to mobilize or
immobilize, to approach or avoid
• Every living thing is a sensory-motor
analyzer-effector. (Cairns-Smith, 1996)
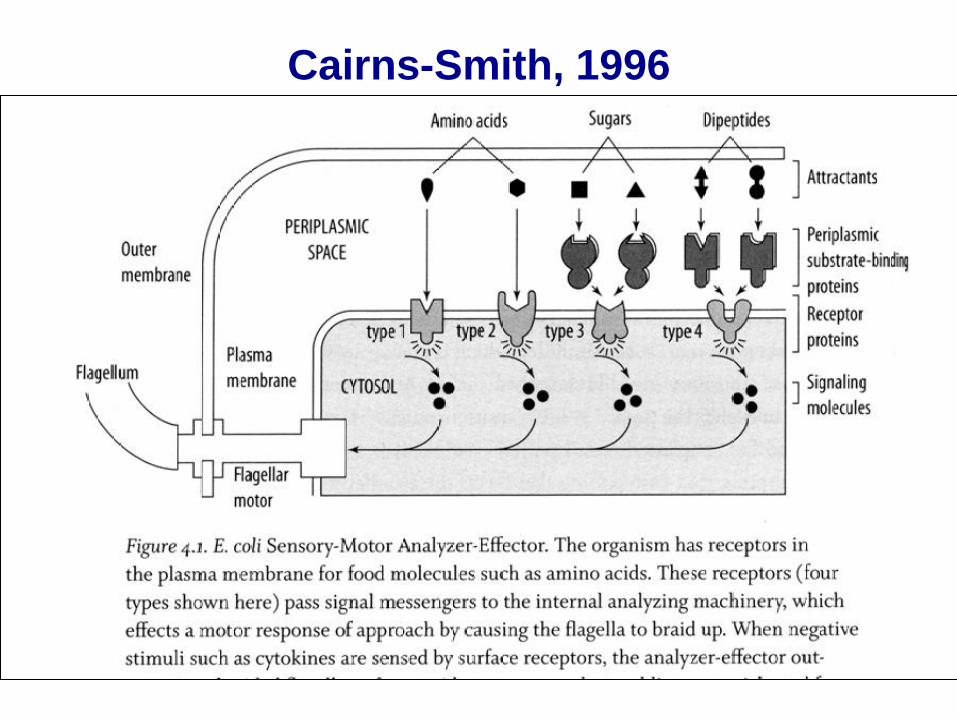
Cairns-Smith, 1996
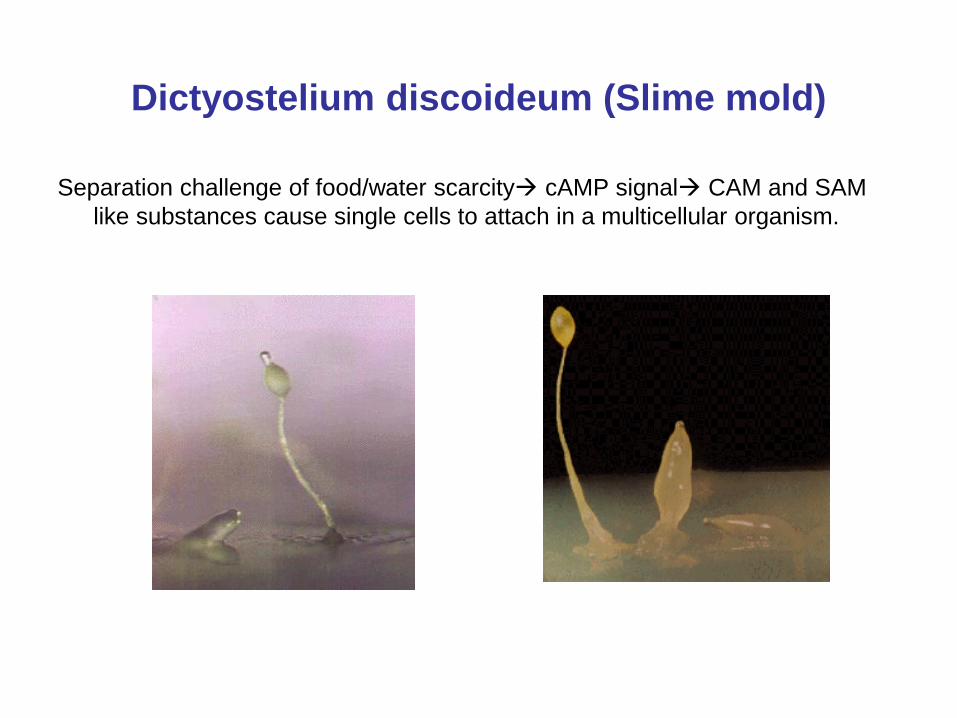
Dictyostelium discoideum (Slime mold)
Separation challenge of food/water scarcity cAMP signal CAM and SAM
like substances cause single cells to attach in a multicellular organism.
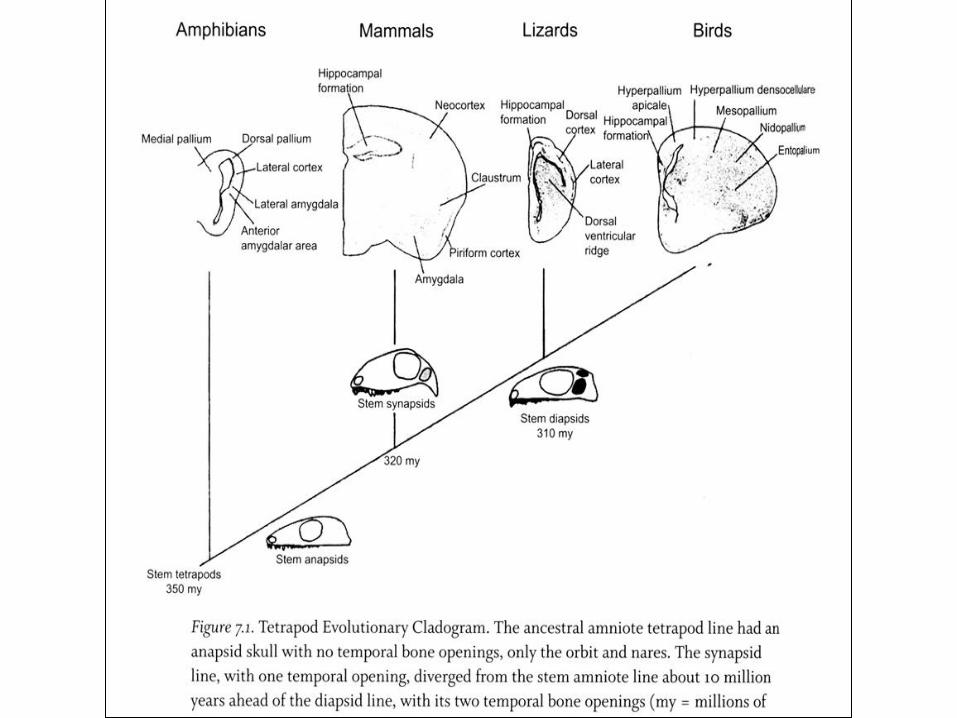
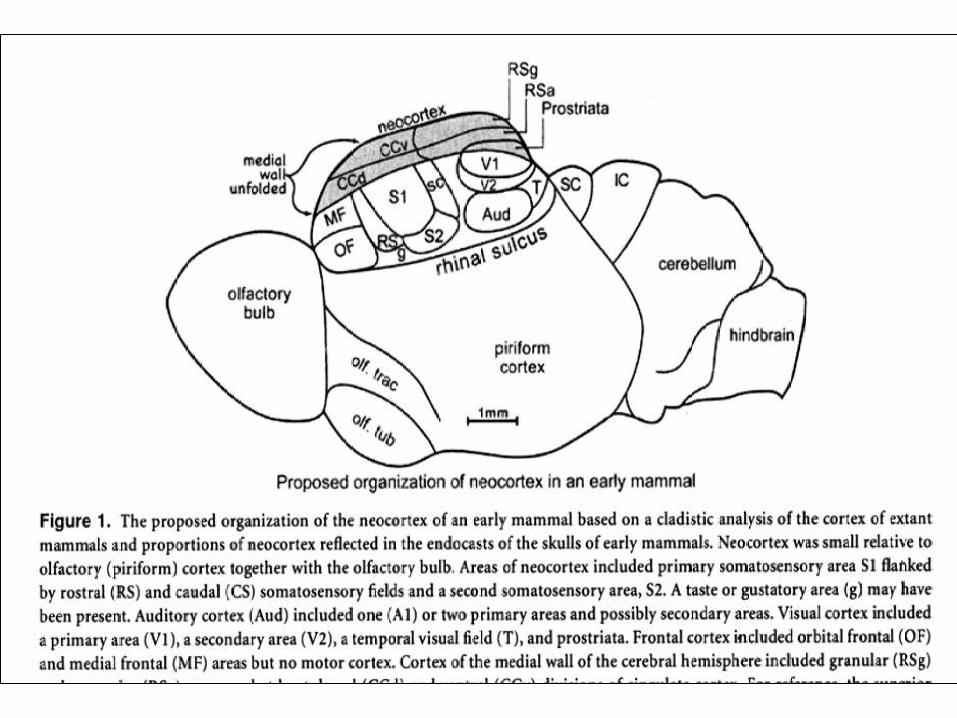
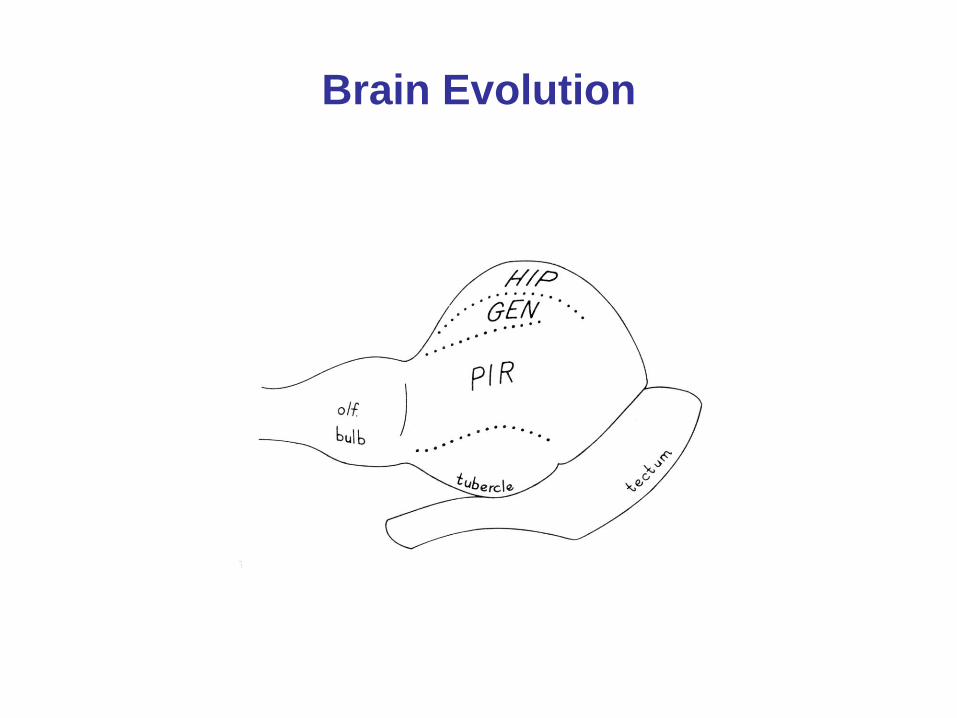
Brain Evolution
Attachment Theory (Bowlby, 1969, 1973, 1988)
• Emotionally significant attachment bonds serve a basic survival function; have a primary status.
• Secure vs. Insecure Attachment (anxious avoidant, resistant, disorganized)
• “The key hypothesis is that variations in the way these bonds develop and become organized during the infancy and childhood of different individuals are major determinants of whether a person grows up to be mentally healthy.” Bowlby, 1988
• “Our environment of evolutionary adaptedness is one of secure base attachment.”
• Suspected that frontal brain areas (vmPFC) are sculpted by these early bonds through epigenetic mechanisms.
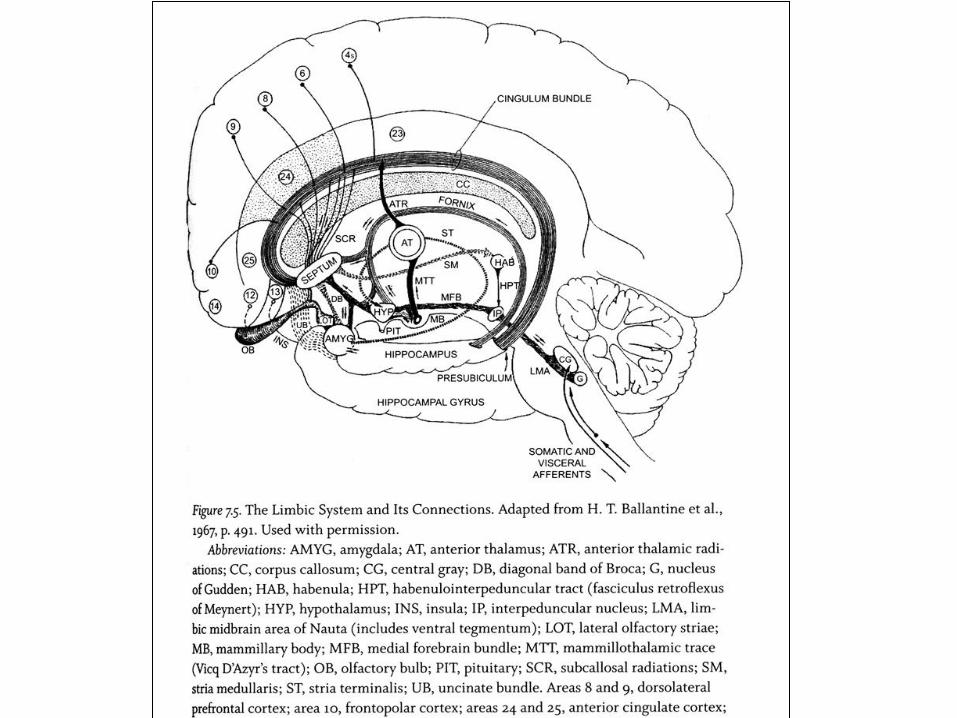
Neurobiological
Attachment Solutions
• Spindle cells (VENs) integrate cognitive inputs with emotional overtones,
overcoming the challenge of separation of cognitive information produced
by cortical regions from emotional information produced by the limbic
system.
• ACC as paralimbic cortex perfectly positioned between limbic system and
neocortex to perform this role. Spindle cells specialized for this attachment
solution function, once they came online, would confer extraordinary
prowess in synthesizing cognition and emotion.
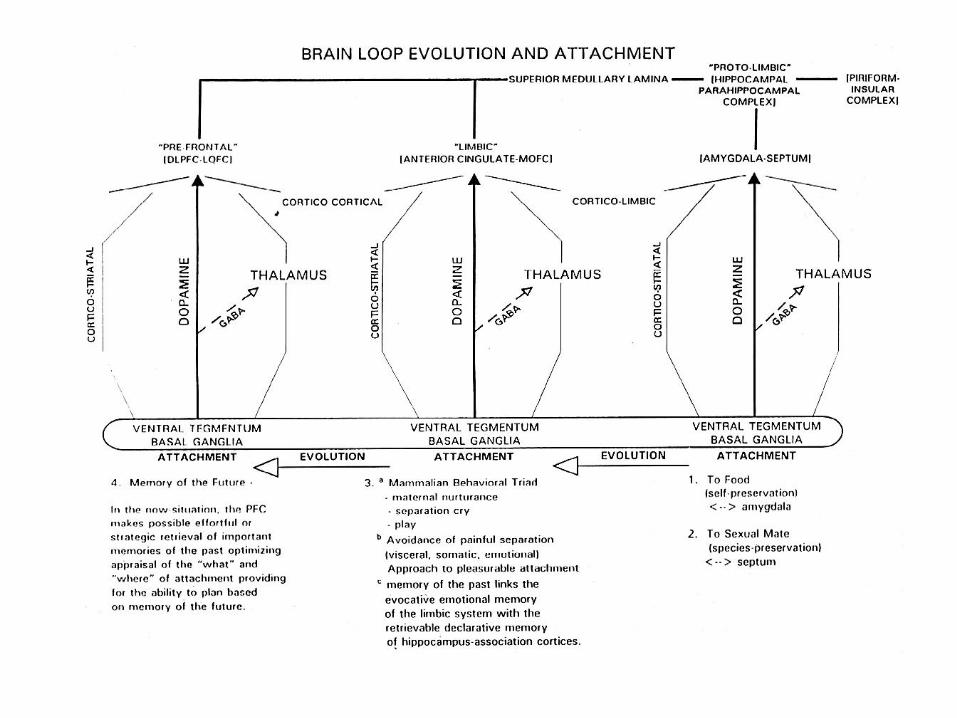
• The ACC-DLPFC–area 10 connections foster the development of self-
control and social insight. The ACC contributes the cognitive-emotional
synthetic analysis required to respond to changing circumstances. Area 10
provides the ability to plan future adaptive responses based on retrieved
memories from the individual’s past experiences.
• DLPFC and “memory of the future” (Ingvar, 1985) or “constructive
episodic simulation” (Schacter, Addis and Buckner, 2008): in league with
MTLMS.
• Affiliative Neuropeptides: oxytocin
Allostasis Sterling and Ayer 1988; McEwen 1998
• “Maintaining stability through change”
• Capacity to adapt or constantly change thereby modifying physiological parameters
in order to adjust to ever shifting environmental conditions.
• At the cellular level, maintenance of healthy mitochondrial reserve capacity.
• The brain does this…
Allostatic Loading • Wear and tear the body experiences due to repeated cycles of allostasis
maintenance. The concept of metabolic energy imbalance.
• Accumulated effects on body of allostatic stress response, as well as inefficient
turning on and shutting off.
• Cognitive constraint hypothesis: depletion of cognitive functioning secondary to
increased decision-making within limited resource model of self-control. Vicious
cycle: overcoming threats and urges and making decisions will deplete mental
resources problem behaviors + poor choices allostatic loading.
• Poverty-related concerns (farmers) consume mental resources leaving less for other
tasks. (Mani et al, Science, 2013)
• Allostatic load diseases include metabolic syndrome, CAD, anxiety and depression
and Alzheimer’s dementia and many others.
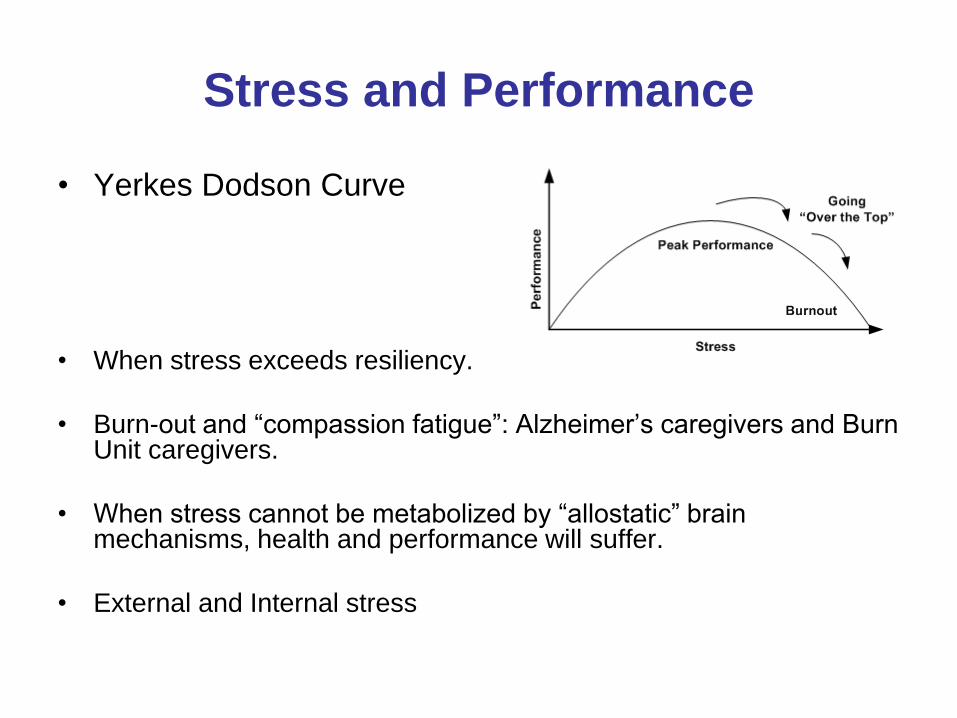
Stress and Performance
• Yerkes Dodson Curve
• When stress exceeds resiliency.
• Burn-out and ―compassion fatigue‖: Alzheimer’s caregivers and Burn Unit caregivers.
• When stress cannot be metabolized by ―allostatic‖ brain mechanisms, health and performance will suffer.
• External and Internal stress
Post Traumatic Stress
• Traumatic events
– Combat
– Rape or other sexual abuse
– Torture
– Criminal Assault
– Accidents
– Natural Disasters
• Traumatic events
reactions
– Intense fear,
helplessness, or horror
(Slide: Tanev 2013)
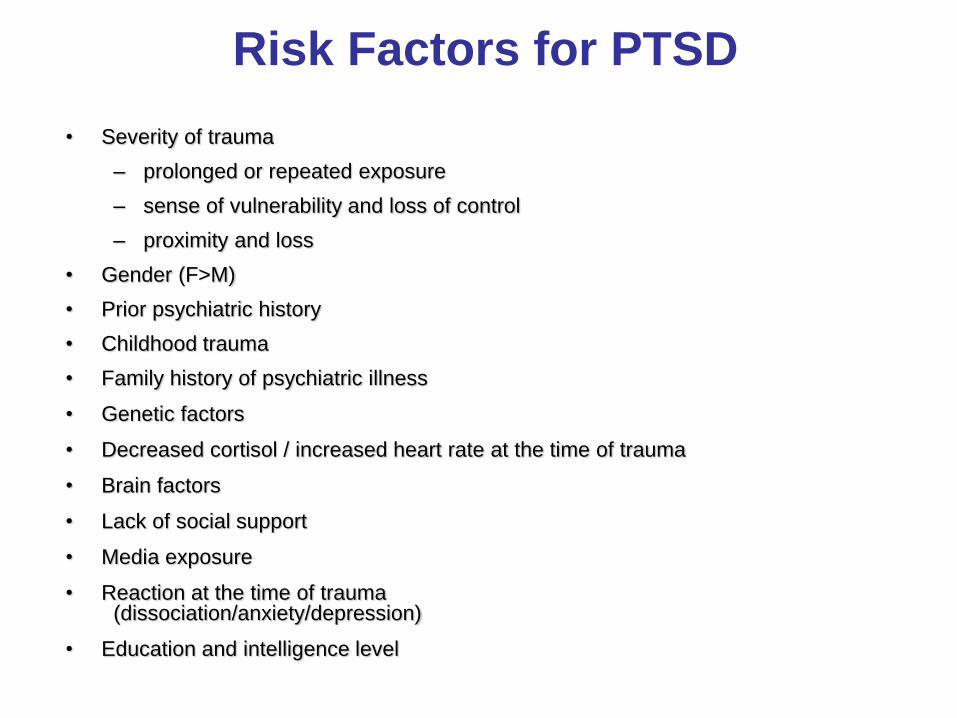
Risk Factors for PTSD
• Severity of trauma
– prolonged or repeated exposure
– sense of vulnerability and loss of control
– proximity and loss
• Gender (F>M)
• Prior psychiatric history
• Childhood trauma
• Family history of psychiatric illness
• Genetic factors
• Decreased cortisol / increased heart rate at the time of trauma
• Brain factors
• Lack of social support
• Media exposure
• Reaction at the time of trauma (dissociation/anxiety/depression)
• Education and intelligence level
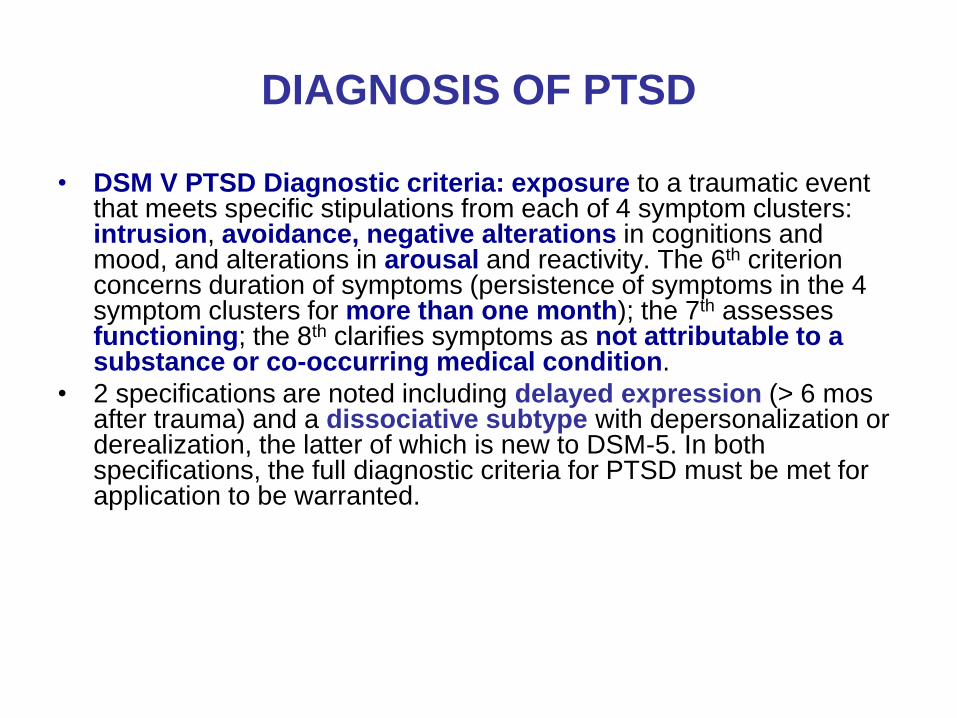
DIAGNOSIS OF PTSD
• DSM V PTSD Diagnostic criteria: exposure to a traumatic event that meets specific stipulations from each of 4 symptom clusters: intrusion, avoidance, negative alterations in cognitions and mood, and alterations in arousal and reactivity. The 6th criterion concerns duration of symptoms (persistence of symptoms in the 4 symptom clusters for more than one month); the 7th assesses functioning; the 8th clarifies symptoms as not attributable to a substance or co-occurring medical condition.
• 2 specifications are noted including delayed expression (> 6 mos after trauma) and a dissociative subtype with depersonalization or derealization, the latter of which is new to DSM-5. In both specifications, the full diagnostic criteria for PTSD must be met for application to be warranted.
PTSD and The Brain
• PTSD may relate to increased amygdala attention to threat cues. (El Khoury-Malhame, 2011)
• Extinction of fear responses to threat cues is impaired in PTSD; dysfunctional activation of fear extinction brain regions, i.e., BLA, hippocampus, ventromedial prefrontal cortex (vmPFC), and dorsal anterior cingulate cortex (dACC). (Milad, 2009)
• PTSD: structural and functional compromise of the ACC, a/w impairment of ability to regulate the amygdala.
• ACC volume is smaller a/w combat-related PTSD, broadly consistent with ACC hypofunctionality. (Woodward 2006)
• PTSD is associated with decreased activity in the DLPFC. (Reichert, 2006) (Cohen, 2004)
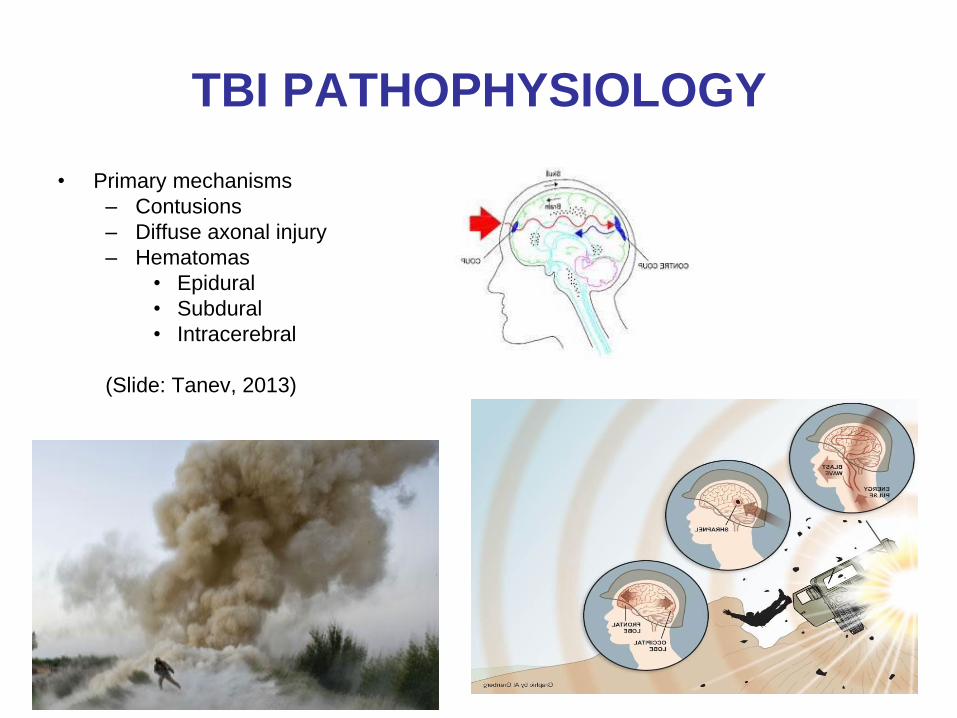
TBI PATHOPHYSIOLOGY
• Primary mechanisms
– Contusions
– Diffuse axonal injury
– Hematomas
• Epidural
• Subdural
• Intracerebral
(Slide: Tanev, 2013)
TBI PATHOPHYSIOLOGY
• Some mechanisms of secondary injury
– Cerebral edema
– Hydrocephalus
– Increased intracranial pressure
– Infection
– Hypoxia
– Neurotoxicity
– Inflammatory response
– Protease activation
– Caspase activation - apoptosis
– Calcium influx
– Excitotoxins
– Free radical release
– Nitric oxide
(Slide: Tanev, 2013)
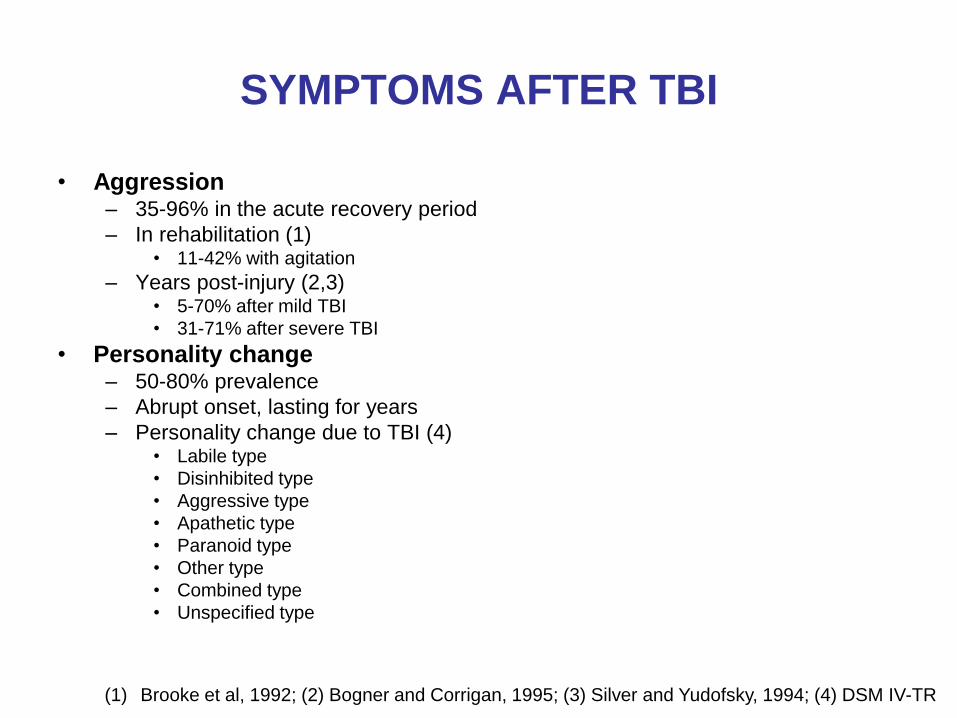
SYMPTOMS AFTER TBI
• Aggression – 35-96% in the acute recovery period
– In rehabilitation (1) • 11-42% with agitation
– Years post-injury (2,3) • 5-70% after mild TBI
• 31-71% after severe TBI
• Personality change – 50-80% prevalence
– Abrupt onset, lasting for years
– Personality change due to TBI (4) • Labile type
• Disinhibited type
• Aggressive type
• Apathetic type
• Paranoid type
• Other type
• Combined type
• Unspecified type
(1) Brooke et al, 1992; (2) Bogner and Corrigan, 1995; (3) Silver and Yudofsky, 1994; (4) DSM IV-TR
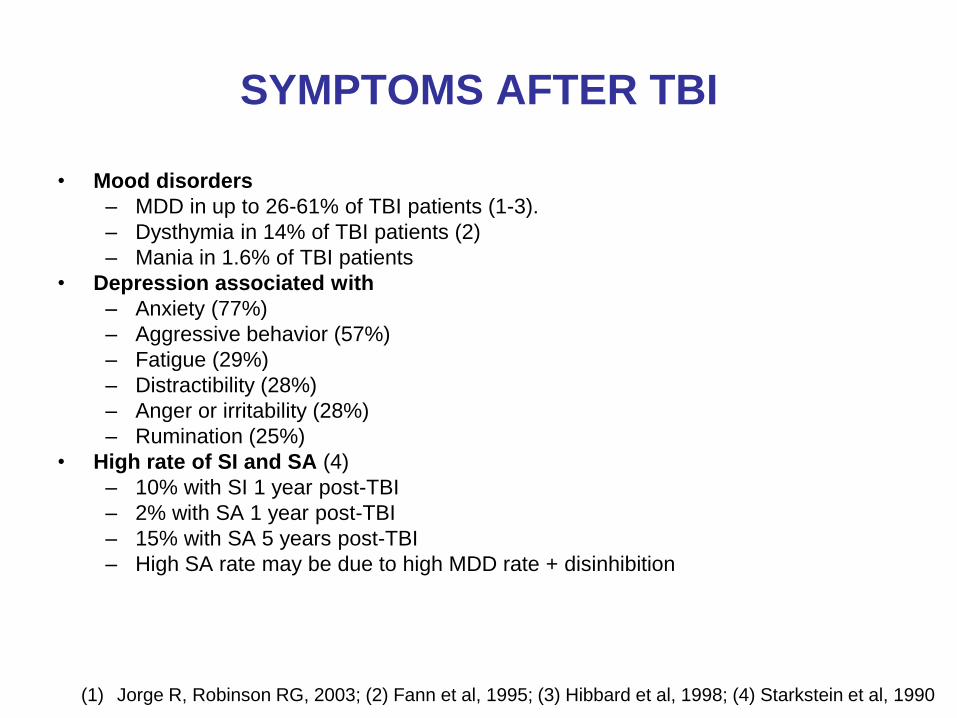
SYMPTOMS AFTER TBI
• Mood disorders
– MDD in up to 26-61% of TBI patients (1-3).
– Dysthymia in 14% of TBI patients (2)
– Mania in 1.6% of TBI patients
• Depression associated with
– Anxiety (77%)
– Aggressive behavior (57%)
– Fatigue (29%)
– Distractibility (28%)
– Anger or irritability (28%)
– Rumination (25%)
• High rate of SI and SA (4)
– 10% with SI 1 year post-TBI
– 2% with SA 1 year post-TBI
– 15% with SA 5 years post-TBI
– High SA rate may be due to high MDD rate + disinhibition
(1) Jorge R, Robinson RG, 2003; (2) Fann et al, 1995; (3) Hibbard et al, 1998; (4) Starkstein et al, 1990
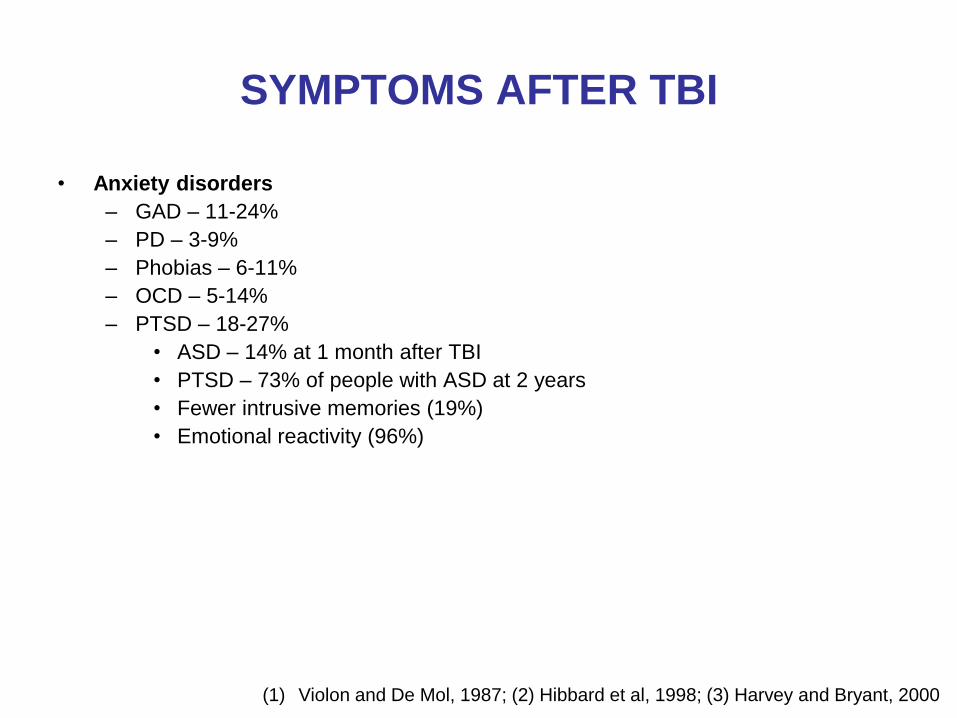
SYMPTOMS AFTER TBI
• Anxiety disorders
– GAD – 11-24%
– PD – 3-9%
– Phobias – 6-11%
– OCD – 5-14%
– PTSD – 18-27%
• ASD – 14% at 1 month after TBI
• PTSD – 73% of people with ASD at 2 years
• Fewer intrusive memories (19%)
• Emotional reactivity (96%)
(1) Violon and De Mol, 1987; (2) Hibbard et al, 1998; (3) Harvey and Bryant, 2000
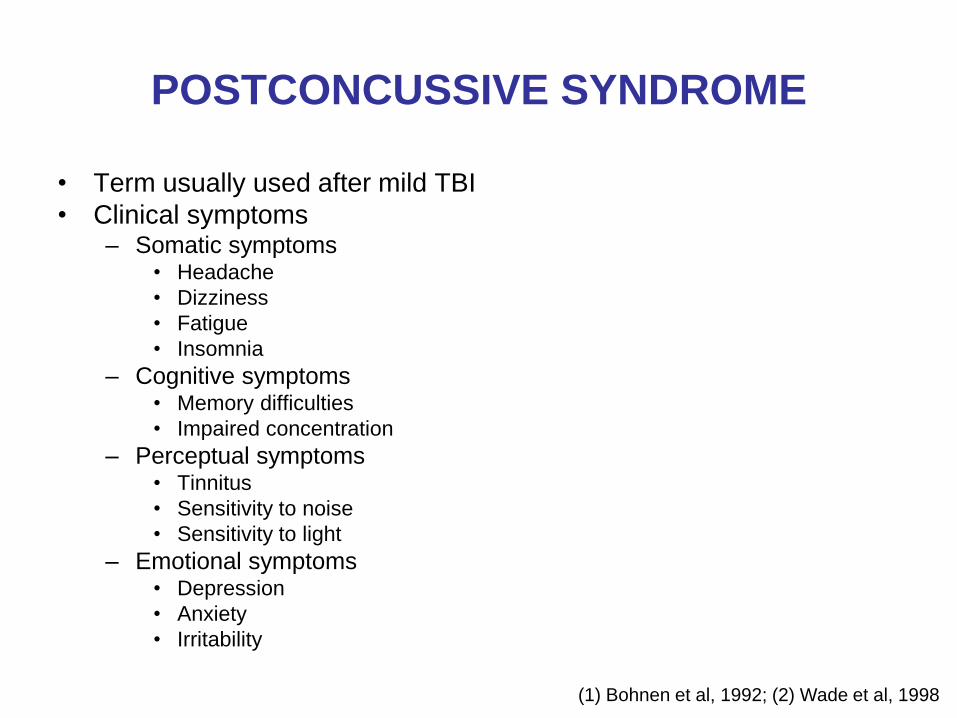
POSTCONCUSSIVE SYNDROME
• Term usually used after mild TBI
• Clinical symptoms – Somatic symptoms
• Headache
• Dizziness
• Fatigue
• Insomnia
– Cognitive symptoms • Memory difficulties
• Impaired concentration
– Perceptual symptoms • Tinnitus
• Sensitivity to noise
• Sensitivity to light
– Emotional symptoms • Depression
• Anxiety
• Irritability
(1) Bohnen et al, 1992; (2) Wade et al, 1998
CO-MORBID PTSD
AND TBI PATHOPHYSIOLOGY
• Challenges in identifying common
pathophysiological mechanisms
– Psychological trauma can be difficult to separate from
biomechanical trauma
– Alteration of consciousness may be difficult to
determine
– The ―Index Event‖ may be difficult to define
– Brain changes may happen in overlapping areas
– Brain changes may be risk factors rather than
consequences of PTSD/TBI
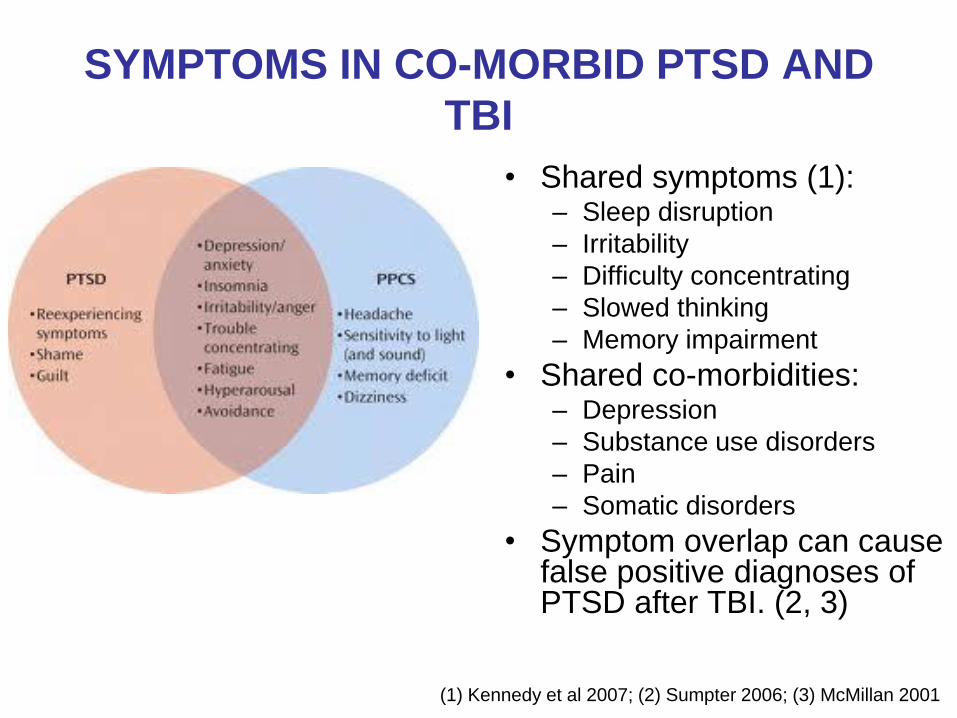
SYMPTOMS IN CO-MORBID PTSD AND
TBI
• Shared symptoms (1): – Sleep disruption
– Irritability
– Difficulty concentrating
– Slowed thinking
– Memory impairment
• Shared co-morbidities: – Depression
– Substance use disorders
– Pain
– Somatic disorders
• Symptom overlap can cause false positive diagnoses of PTSD after TBI. (2, 3)
(1) Kennedy et al 2007; (2) Sumpter 2006; (3) McMillan 2001
COGNITIVE DYSFUNCTION
IN TBI
• Cognitive improvement within the first 6-12 months post injury due to natural regenerative brain processes
• New cognitive baseline after 12 months, which is frequently abnormal and contributes to disability
• Areas of neurocognitive impairment – Slow speed of information processing - most robust
effect size (g=0.47) in mTBI (1)
– Attention
– Executive dysfunction
– Memory problems (2)
(1) Frencham et al, 2005; (2) West et al, 2010
NEUROIMAGING
IN PTSD AND IN TBI
• In veterans with PTSD, there are disruptions in gray and WM areas: – Pregenual ACC and bilateral insulae (1)
– Left amygdala and the frontal lobes (2)
– Prefrontal cortex, posterior angular gyrus (3)
– Corpus callosum is decreased in volume (2, 4)
• TBI involves damage in multiple gray and WM areas: – The hippocampi (5)
– Frontal, parietal, occipital and temporal neocortices (6)
– Mid- and posterior cingulate cortices, corpus callosum, thalamus, (7, 8)
– Caudate nucleus, midbrain and cerebellum (7)
– Volume enlargements in ventricles (7) and sulcal/subdural CSF (9)
– Diffuse damage to the WM (WM Load) (10)
– Multiple fasciculi: superior longitudinal, uncinate, inferior fronto-occipital, cingulum, corticopontine tract, external capsule (6)
– Internal capsule, supratentorial projection fiber bundles, fronto-temporo-occipital association fiber bundles (11)
– Corpus callosum (6, 11)
(1) Kasai et al, 2008; (2) Karl et al, 2006; (3) Schuff et al, 2010; (4) Villarreal et al, 2004; (5) Ng et al, 2008; (6)
Bendlin et al, 2008; (7) Kim et al, 2008; (8) Yount et al, 2002; (9) Levine et al, 2008; (10) Kraus et al, 2007;
(11) Rutgers et al, 2008
SLEEP IN TBI
• 46% TBI patients have a sleep disorder (1, 2) – 30-70% insomnia symptoms
– 23% sleep apnea
– 11% post-traumatic hypersomnia
– 6% narcolepsy
– 7% periodic limb movements
• Reduced evening melatonin production (3)
• Insomnia neuropsychiatric sequelae of TBI
• Drugs for comorbid issues may interfere with sleep
(1) Ouellet et al, 2004; (2) Castriotta et al , 2011; (3) Shekleton et al, 2010
THERAPY FOR SLEEP DISTURBANCES
IN TBI
• Treatments for sleep problems in TBI – RCT preliminary evidence for Melatonin and
Amitriptyline (1)
– Mixed results for using Modafinil (2, 3)
– Use of benzodiazepines discouraged and atypical GABA agonists cautioned
– Limited data for trazodone and melatonin agonists (4)
– Long-term use of hypnotics may be problematic (7) because of issues of polypharmacy, chronicity of the disorders, altered neuronal milieu, and drug dependency (5, 6)
– CBT could be effective (7)
(1) Kemp et al, 2004; (2) Kaiser et al, 2010; (3) Jha et al, 2008; (4) Larson et al, 2010;
(5) Zeitzer et al, 2009; (6) Seitzer et al, 2009; (7) Ouellet et al, 2004
SLEEP IN PTSD AND CO-MORBID PTSD
AND TBI
• In PTSD – Self-reported sleep problems but unclear if objective indices of
sleep disturbance (1)
– Sleep problems may interfere with recovery (1)
– REM abnormalities, increased respiratory, movement and cognitive arousals (2), more periodic limb movements (3, 4)
– Poor sleep efficiency, decreased slow wave sleep (5), decreased sleep continuity (3, 4)
– Focused therapy of sleep disturbances/nightmares shows good effects (2)
• In PTSD+TBI – Greater severity of sleep disturbances in PTSD with
moderate/severe TBI vs PTSD with mTBI (p<0,05), and in PTSD without TBI (p<0,01) (6)
(1) Babson et al, 2010; (2) Bader et al, 2005; (3) Buljan et al, 2008;
(4) Kim et al, 2007; (5) Yetkin et al, 2010; (6) Simonovic et al 2011
THERAPY FOR SLEEP DISTURBANCES
IN PTSD
• The Standards of Practice Committee of the American Academy of Sleep Medicine reviewed the literature and made the following recommendations (1):
– Pharmacotherapy for PTSD-associated nightmares:
• Prazosin is recommended
• Clonidine may be considered
• The following may be considered, but data low grade and sparse:
– Trazodone, atypical antipsychotic medications, topiramate, fluvoxamine, triazolam and nitrazepam, phenelzine, gabapentin, cyproheptadine, and tricyclic antidepressants.
• No recommendation regarding clonazepam because of sparse data
• Preliminary evidence for eszopiclone (2)
(1) Aurora et al, 2010; (2) Pollack et al, 2011

CBT FOR PTSD
• Review of the literature – Robust evidence--safe and effective in acute and chronic PTSD
following a range of traumatic experiences in adults, children, and adolescents
– Validated and used across many cultures
-- Easily trainable in individual and group settings
– Effective use of Internet-based CBT in PTSD
– Response depends on various factors, including comorbidity and the nature of the study population
– Found to have a preventive role in some studies
– Effect mediated mostly by change in maladaptive cognitive distortions associated with PTSD
– Physiological, functional neuroimaging, and EEG changes c/w response
– Non-response to CBT can be as high as 50%
Kar et al, 2011
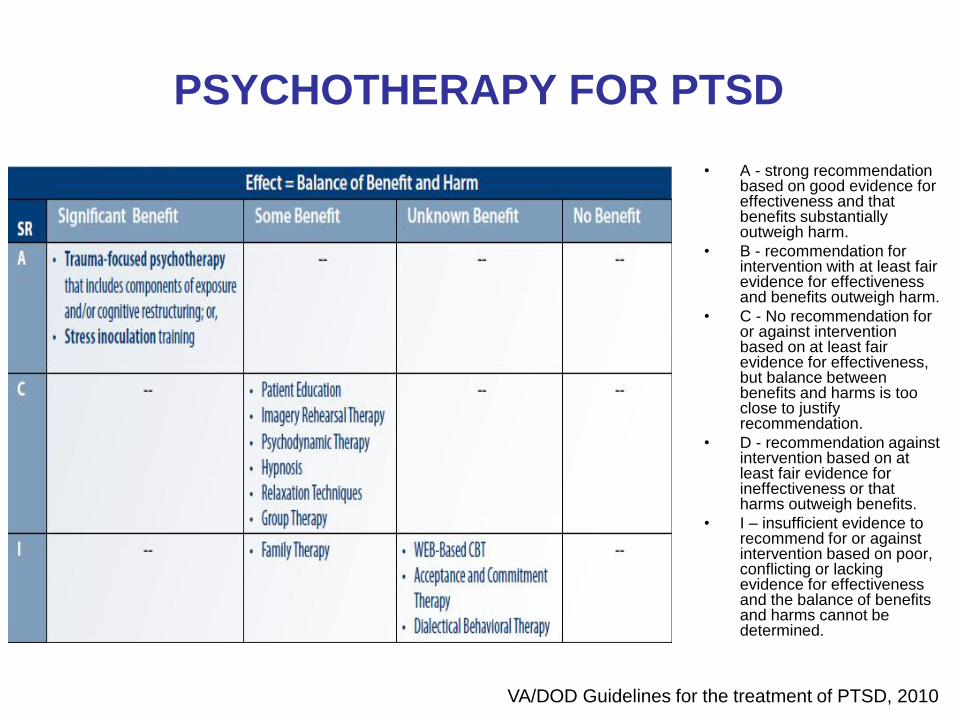
PSYCHOTHERAPY FOR PTSD
• A - strong recommendation based on good evidence for effectiveness and that benefits substantially outweigh harm.
• B - recommendation for intervention with at least fair evidence for effectiveness and benefits outweigh harm.
• C - No recommendation for or against intervention based on at least fair evidence for effectiveness, but balance between benefits and harms is too close to justify recommendation.
• D - recommendation against intervention based on at least fair evidence for ineffectiveness or that harms outweigh benefits.
• I – insufficient evidence to recommend for or against intervention based on poor, conflicting or lacking evidence for effectiveness and the balance of benefits and harms cannot be determined.
VA/DOD Guidelines for the treatment of PTSD, 2010
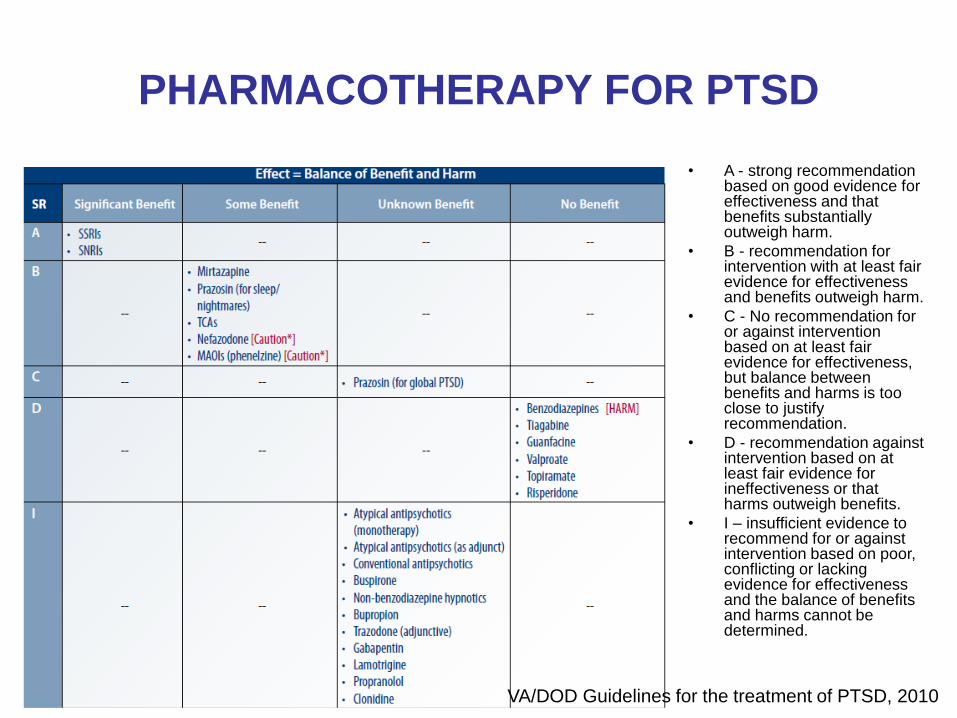
PHARMACOTHERAPY FOR PTSD
VA/DOD Guidelines for the treatment of PTSD, 2010
• A - strong recommendation based on good evidence for effectiveness and that benefits substantially outweigh harm.
• B - recommendation for intervention with at least fair evidence for effectiveness and benefits outweigh harm.
• C - No recommendation for or against intervention based on at least fair evidence for effectiveness, but balance between benefits and harms is too close to justify recommendation.
• D - recommendation against intervention based on at least fair evidence for ineffectiveness or that harms outweigh benefits.
• I – insufficient evidence to recommend for or against intervention based on poor, conflicting or lacking evidence for effectiveness and the balance of benefits and harms cannot be determined.
COGNITIVE REHABILITATION FOR TBI
• Substantial evidence supports cognitive rehabilitation (CR)
– CR best treatment for neurocognitive impairment and functional limitations after TBI
• Comprehensive-holistic neuropsychologic rehabilitation (emphasizing metacognitive and emotional regulation) for cognitive and functional disability in the postacute rehabilitation of moderate or severe TBI
• Recent advances (1)
– Task-specific training of cognitive deficits
– Computer-aided cognitive remediation
– Visual-spatial, visual scanning techniques and body weight-supported treadmill training for motor deficits
• Recommendations for cognitive rehabilitation (2, 3)
– Access to subacute rehabilitation that is holistic
– Trials of medication, especially methylphenidate
– Attention, memory and executive skills retraining can improve abilities to manage workplace tasks/demands
– CBT for improving coping skills, managing cognitive difficulties, and addressing anxiety/depression
Cicerone et al, 2011

PHARMACOTHERAPY FOR COGNITIVE
DEFICITS IN TBI
• A 24-week, RCT, double-blind crossover trial (1). – 18 post acute TBI patients with cognitive impairment.
– Patients randomly assigned to donepezil for 10 weeks and then placebo for 10 weeks OR placebo for 10 weeks followed by donepezil for 10 weeks
– CONCLUSIONS: Donepezil associated with increased neuropsychological testing scores in short-term memory and sustained attention in post acute TBI patients
• A 12 week prospective, double blind, placebo controlled trial (2, 3) – 157 patients > 12 months post-injury
– Rivastigmine 3-6mg per day vs. placebo
– 49% of rivastigmine and 49% of placebo responded by week 12
– CONCLUSIONS: In a subgroup of patients with moderate-severe memory impairment (n=81), rivastigmine significantly better than placebo in improving cognitive measures
1) Zhang et al, 2004
(2) Silver et al, 2006; (3) Silver et al, 2009
PHARMACOTHERAPY FOR COGNITIVE
DEFICITS IN TBI
• Stimulants – Block reuptake of NE and DA
– MPH helps with cognition, rate of recovery (1, 2, 6, 7)
– SE: paranoia, dysphoria, agitation, irritability
– No data for increased seizures with stimulants (3)
• Amantadine up to 400mg per day – DA-ergic action, GABA-ergic, NMDA antagonist
– Improves motivation, concentration, alertness, executive function, behavioral dyscontrol (4, 6, 8)
• In one study, Carbidopa/Levodopa 10/100 to 25/250 qid led to – Better alertness and concentration;
– Decreased fatigue, hypomania and sialorrhea
– Improved memory, mobility, posture and speech (5)
(1) Gualtieri and Evans, 1988; (2) Plenger et al, 1996; (3) Wroblewski et al, 1992; (4) Kraus and Maki, 1997;
(5) Lal et al, 1988; (6) Writer BW, 2009; (7) Willmott C, 2009; (8) Kraus MF, 2005
PHARMACOTHERAPIES FOR CO-
MORBID PTSD AND TBI
• Co-morbid PTSD associated with increased medication adherence (74%) in TBI patients (1)
• Evidence base for pharmacotherapies is scarce.
• Some principles (3): – Absence of data for combined psychotherapy med approaches
– Take a comprehensive approach, consider other psychosocial needs
– Obtain diagnostic clarity and initiate with one agent at a time
– Use longer treatment trials to assess efficacy
– Start with lower doses because of sensitivity to side effects in TBI patients
– No research trials on specific meds. From clinical experience:
Antidepressants: standard approaches may be beneficial
Anticonvulsants: could be useful for treating mood disorders, impulsive anger, irritability and aggression but may exacerbate cognitive deficits
Antipsychotics: very low dose may be helpful for psychotic symptoms complicating this condition
Anxiolytics: caution, usual concerns with benzodiazepines apply
(1) Huggins et al, 2011; (2) Kaplan et al, 2010; (3) McAllister 2009
PTSD, TBI and Risk of Dementia
• Delayed neurological health consequences of environmental insults during military service generally underappreciated.
• PTSD and TBI have been linked to an increased risk of Alzheimer's disease (AD) and other dementias. (Weiner et al, 2013)
• Military risk factors for AD include:
1) tobacco use, TBI, depression, and PTSD
2) vascular risk factors such as obesity and metabolic syndrome, education and physical fitness.
• Degree of combat exposure, Vietnam era Agent Orange exposure and Gulf War Illness may influence risk for AD.
• Conservatively estimated 423,000 new cases of AD in veterans by 2020.
• Mitigation of the potential impact of military exposures on the cognitive function and management of modifiable risk factors through specifically designed programs will be instrumental in minimizing the future impact of AD in veterans
(Veitch et al, 2013)
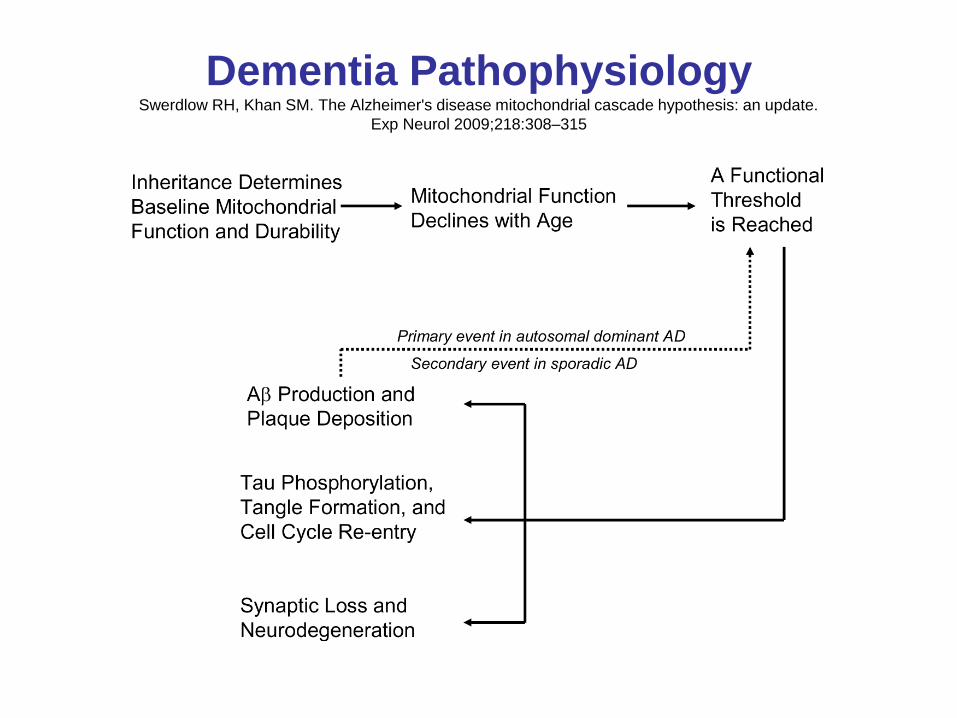
Dementia Pathophysiology Swerdlow RH, Khan SM. The Alzheimer's disease mitochondrial cascade hypothesis: an update.
Exp Neurol 2009;218:308–315
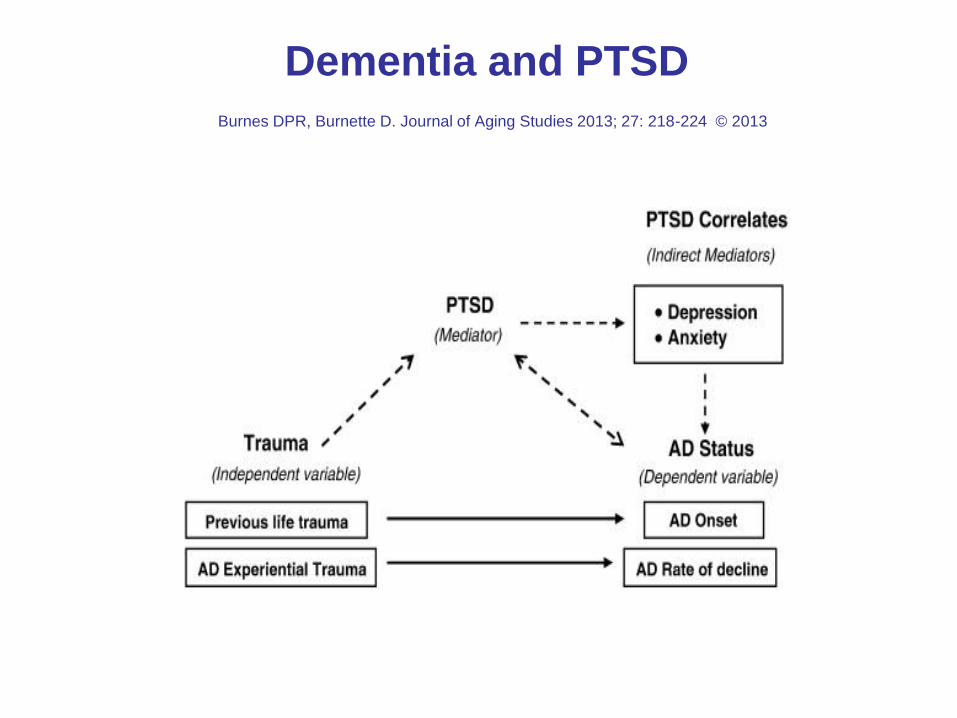
Dementia and PTSD
Burnes DPR, Burnette D. Journal of Aging Studies 2013; 27: 218-224 © 2013
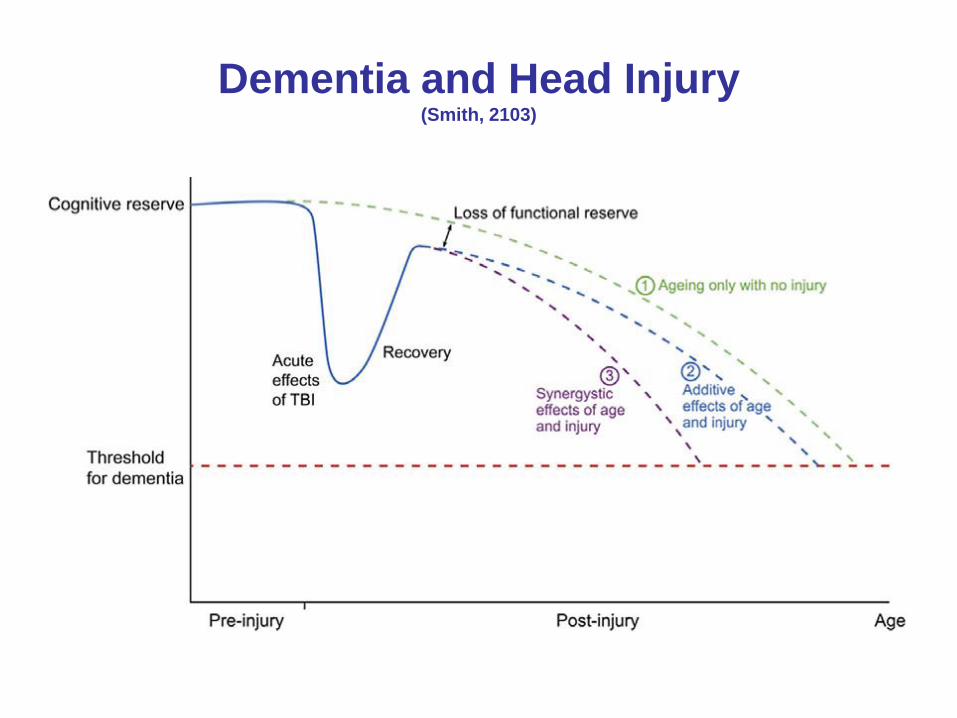
Dementia and Head Injury (Smith, 2103)
Allostatic Load Reduction:
Health Promotion
and Illness Prevention
• Tertiary
• Secondary
• Primary
• Behavioral Risk Factors for Chronic Non-Communicable
Diseases
• Self-care and Care-giving
• Resiliency Medicine
Resiliency: Neural Mechanisms
• Definition: good adjustment across different domains in the face of significant adversity. (Luthar, Cicchetti and Becker, 2000) This will be reflected in better energy dynamics and cognitive reserve—reducing mitochondrial expenditure/building mitochondrial reserve capacity.
• [a] Fear Responsiveness: effective behaviors despite fear (Charney 2004)
• [b] Adaptive Social Behavior: altruism, bonding and teamwork (Charney 2004)
• [c] Reward and Motivation: hedonia, optimism, learned optimism, meaning (Charney 2004)
• Molecular adaptations within the mesolimbic brain reward circuitry (MFB) and Stress Systems are associated with vulnerability and resiliency (Krishnan et al, 2007) ---BDNF; 5-HTTLPR; CRF/NPY; DHEA/cort and NPY/NE
Resiliency Medicine at BHI: Stress Buffering
and Health Strengthening for Caregivers
and Care-receivers
• Relaxation Response/Mindfulness (Focused Attention;
Insight/Open Monitoring) [a]
• Cognitive Behavior Therapy [a]
• Social Support and Pro-social Behavior [b]
• Positive Psychology [c]
• Belief and Conscious Expectation [c]
• Exercise: running enhances local inhibitory mechanisms
in the hippocampus (Schoenfeld et al, 2013) [a]
• Diet: modulation of mitochondrial reserve capacity;
microbiome and stress
• Sleep: modulation of mitochondrial reserve capacity
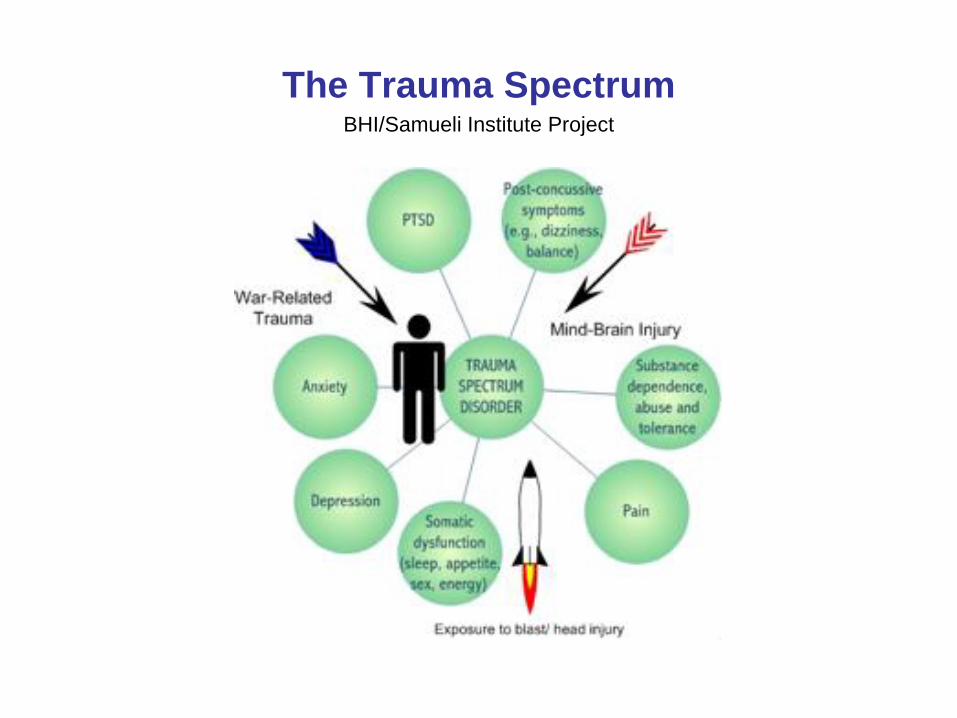
The Trauma Spectrum BHI/Samueli Institute Project
BHI Military Trainings
• Battle Rhythm and Beyond (BRB) Bavaria Soldier 360 Total Fitness Course; Mind Body Train the Trainers program; 2009
• U.S. Army MRAA TATRC Grant Subcontract 2011D001892 Relaxation Response Training for PTSD Prevention in Soldiers (SPIRIT SMART) 09/01/10-08/31/12; Ft Bliss Training May 2012
• US Naval Medical Center, Mind Body Medicine Clinic Planning Consultation; San Diego Training (SPIRIT SMART) March 8, 9, 2013
• NICoE Collaborations: planning stages--genomics and biomarker research on intervention outcomes; train the trainers program for NICoE satellites

Mindfulness
• Non-judgmental attention to experiences in the present moment to
achieve self-awareness and transcendence in everyday life (Kabat-Zinn,
1994) (Vago and Silbersweig, 2012)
• Start with Focused Attention (empty mind of everyday thinking to
stabilize the mind and decrease mental proliferation and focus on a
single point, e.g, breath, word, phrase, prayer) to elicit relaxation
response.
• Move to Insight/Open Monitoring (no object of focus but receptive
in nonjudgmental way to all physical and mental phenomena that
arise).
• Can then add ethical value qualities (loving-kindness, compassion,
forgiveness) OR can do visual imagery and add hypnotic
suggestion for analgesia for example.
• Achieving relaxation response promotes the physiological and
somatic markers of secure attachment.
Resiliency
“During my first flight in 2001, there were 18
mice on board. All of them, with one exception,
clung to the inside of the mesh during the entire
mission. One mouse, smaller than the rest,
seemed to enjoy the experience and effortlessly
floated around the cage….We all watched him
as he enjoyed the feeling of being weightless.”
Astronaut Mark Kelly
Human Resiliency
Stress
----------------------------- = Allostatic =
Resiliency Factors Load
– relaxation response
– mindfulness
– social support/pro-sociality
– cognitive skills
– positive psychology
– spiritual connectedness
– exercise
– nutrition
– sleep hygiene
– healthy habits
Mind Body Medicine Equation
Vulnerability to Illness
Mitochondrial Resiliency
Mitochondrial stress (oxidative)
+ Genetic vulnerability
_________________ = propensity to illness
Mitochondrial resiliency
+ Genetic endowment
e.g.,
Epel ES, Blackburn EH, Lin J, Dhabhar FS, Adler NE, Morrow JD, Cawthon RM. Accelerated telomere shortening in response to life stress. Proc Natl Acad Sci U S A. 2004;101:17312-17315.)
Evolutionary Resiliency
Separation Threats
---------------------------- = Propensity to Illness
Attachment Solutions
The Mammalian Behavioral Triad: separation cry, maternal nurturance
and play. (MacLean, 1990)
Transcriptome: PBMCs and Brain
• Possible that PBMC gene expression can be used to construct
useful profiles of brain disorders (Woelk et al, 2011)
• Peripheral blood expression levels of many genes are moderately
c/w gene expression levels in other tissues including brain. (Sullivan et
al, 2006; Rollins et al 2010; Kohane and Valtchinov 2012)
• Possible proxy phenomenon to identify promising PBMC biomarkers
for neuropsychiatric disorders including PTSD.
• Glatt et al, 2013 Am J Med Gen: pre-trauma PBMC GEP
(particularly activation of cell mediated immune genes) differed
between trauma exposed Marines who developed PTSD and those
who did not.
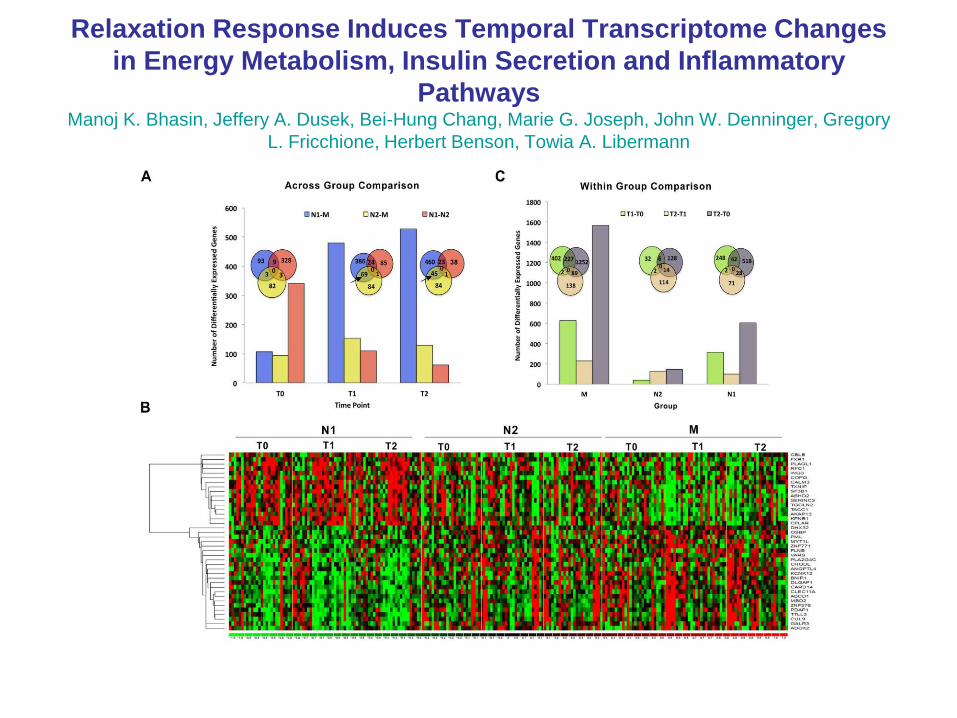
Relaxation Response Induces Temporal Transcriptome Changes
in Energy Metabolism, Insulin Secretion and Inflammatory
Pathways Manoj K. Bhasin, Jeffery A. Dusek, Bei-Hung Chang, Marie G. Joseph, John W. Denninger, Gregory
L. Fricchione, Herbert Benson, Towia A. Libermann
PLoS One, May 2013
Human Well-Being (Fredrickson et al, 2013)
• PBMC transcriptome analysis from subjects with hedonic
(pleasurable needs met) vs. eudaimonic (meaningful other-regarding
purpose) well-being
• Stress-related conserved transcriptional response to adversity
pattern: increased expression of genes associated with NF-kB
induced pro-inflammatory cytokines.
• Those with eudaimonic well being have deactivation of their NF-kB
and activation of anti-viral IRF gene sets.
• Relaxation Response Resiliency Training counter-regulates the
stress-related conserved transcriptional response to adversity
pattern and enhances well-being by recreating the physiological and
somatic markers of secure attachment.
Caregiver Stress
• Today’s need for qualified and well-equipped family caregivers is growing.
• More than 65 million family caregivers in the U.S. provide the largest proportion of care for dependent elderly individuals as well as adults and children with disabilities and chronic illnesses.
• Research has found that family caregivers report frequent stress, high rates of clinical depression and more health problems in general than the non-caregiving population.
RCI Operation Family Caregiver
for Returning Veterans
• Designed to help families of returning OEF/OND/OIF service members suffering with
health issues such as TBI, PTS, and physical disability.
• OFC is a personalized 4-6 month program offered either in-home, by telephone, or
via Skype.
• OFC teaches problem-solving skills to empower family caregivers to deal more
effectively with issues related to caregiving.
• OFC proven to lower depression, decrease health complaints, and reduce burden
and anxiety in family caregivers.
• Participation is free and completely confidential. No personal or medical information is
accessed or shared with others.
• OFC is a translation of an evidence-based intervention (Problem-Solving Training for
Family Caregivers) that has been tested for caregivers of individuals with a range of
mental health conditions associated with TBI and stroke, as well as caregivers of
individuals with disabilities.

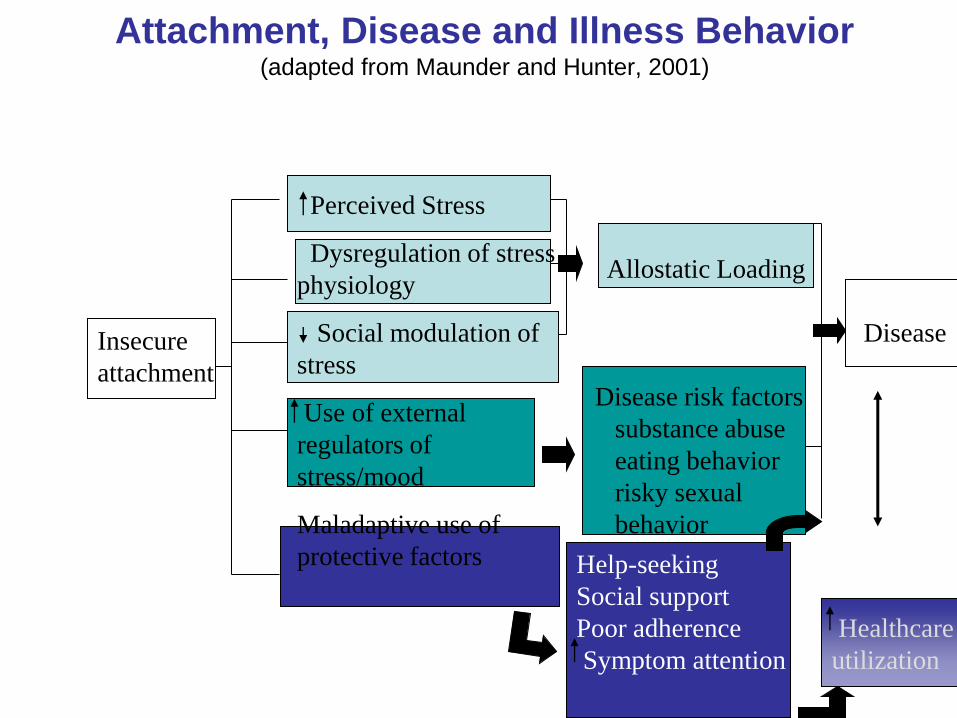
Attachment, Disease and Illness Behavior (adapted from Maunder and Hunter, 2001)
Perceived Stress
Dysregulation of stress
physiology
Social modulation of
stress
Use of external
regulators of
stress/mood
Maladaptive use of
protective factors
Allostatic Loading
Disease risk factors
substance abuse
eating behavior
risky sexual
behavior
Help-seeking
Social support
Poor adherence
Symptom attention
Healthcare
utilization
Insecure
attachment
Disease
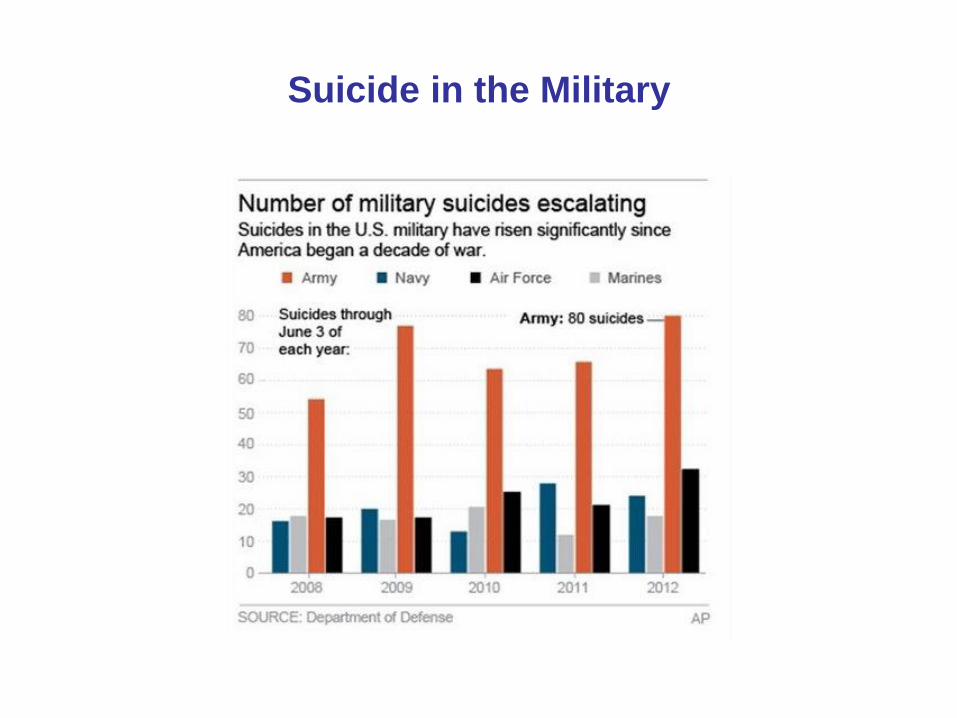
Suicide in the Military
Suicide in the Military
• Suicidality is a separation challenge
• Amygdala and PFC changes
• TBI # and deployment (JAMA, 2013)
• Male sex and mental health issues but not military
specific variables necessarily (JAMA, 8/7/13)
• Disconnectedness
• Moral Injury issue may play a role
• Calls for attachment solutions —professional
caregivers, family and peer caregivers, spirituality and
religion, service dogs, volunteering.
• Resiliency enhancement and self-care
Spirituality and Resiliency
• “Spirituality is the aspect of humanity that refers to the way
individuals seek and express meaning and purpose and
the way they experience their connectedness to the
moment, to self, to others, to nature, and to the significant
or sacred.” (Puchalski et al, 2009, p 887)
• Increase in positive expectations
• Decrease in perceived stress/threat and increase in benign appraisal
• Increase in social support and pro-social behavior
• Increase in Source support
• Downstream benefits for health
Twelve Step Programs
• Sponsor---social support and pro-social behavior
(ACC/MOF)
• Surrender to a power greater than self---spiritual
connectedness
• Power to overcome incentive salience of drug effects on
hedonic pathway.
• Power to dampen dysphoria/negative affect of
withdrawal
• Power to reduce drug craving

Attachment Solution Lessons
from Service Dogs?
• Guardian Angels Medical Service Dogs, Inc.: highly trained service dogs assigned to the Veteran’s Administration (VA) for a multi-year scientific study examining the impacts that service dogs have on veterans with PTSD.
• The Paws for Purple Hearts program: human-dog relationship being studied for measurable clinical impact on the health and well-being of patients, including veterans with PTSD.
• Warrior Canine Connection: anecdotal evidence that service dogs reduce the PTSD symptoms of Warrior-trainers and presence of dogs enhances sense of wellness in NICoE staff and the families of Wounded Warriors. WCC research team plans to investigate physiological, psychological, and behavioral benefits of this program. (Yount et al , 2012)
• Service dogs for ASD: Before the introduction of service dogs, measured a 58% increase in morning cortisol in autistic children after awakening, which diminished to 10% when service dogs were present. Increase in morning cortisol back up to 48% once the dogs were removed (p<0.05). (Viau et al, 2010)
• American Heart Association May 9, 2013 report: owning a dog probably associated with reduced risk of CAD.
The Importance of the Secure Base Effect
for Domestic Dogs (Horn et al, 2013)
• Study showed an owner specific secure
base effect in dogs that extends from
attachment tests to tests of cognitive
functioning.
• Dogs are therefore remarkably like
children; benefit from having their owner
as a secure base for interacting with the
environment.
Quality Care
“It would be nice if all of the data which sociologists
require could be enumerated because then we could run
them through IBM machines and draw charts as the
economists do. However, not everything that can be
counted counts, and not everything that counts can be
counted.”
William Bruce Cameron (1963)
“Ultimately the secret of quality is love.... If you have love
you can then work backward to monitor and improve the
system.”
Avedis Donabedian, MD, MPH (1919-2000)
Implications for Modern Medicine
• Need attachment based medical system that incentivizes attachment solutions
• Need for more community based public health approaches
• Need for research in the new molecular mind body medicine
• Need to recognize the wisdom of the ages-we’ve evolved as organisms that seek resiliency factors (attachment based solutions) that carry with them positive emotions. Doctors heal by promoting these. (Fricchione, 2011)
Summary
• By teaching self care and communitarian ways to reduce stress and enhance resiliency in any stage of the public health continuum, we can promote health, prevent illness and enhance performance.
• Resiliency enhancement necessarily requires enhancement of re-attachment in the face of separation challenges.
• This is because secure attachment is our environment of evolutionary adaptedness and without it we suffer and fail to function.
• The RCI mission has always been dedicated helping others to find attachment solutions in the midst of their separation suffering.