Embed Size (px)
Citation preview
Globalization, Health Inequities, and Structural Transformation: A Culture-Centered Approach to Communication for Social Justice
CARE WHITE PAPER SERIES 2012 VOL. 2
Mohan J. Dutta
Slides fromCDC Plenary Speech Presented at the 2012 National Conference on Health Communication, Marketing, and Media, Atlanta, Georgia. August, 2012.

Globalization, Health Inequities, and Structural Transformation: A Culture-Centered Approach
to Communication for Social Justice Mohan J. Dutta
Slides* from CDC Plenary Speech Presented at the 2012 National Conference on Health Communication, Marketing, and Media,
Atlanta, Georgia. August, 2012.
*Content and layout have been altered for print.
CARE WHITE PAPER SERIES
3
Mohan J. Dutta is Director of CARE and Head of the Department of Communications and New Media at the National University of Singapore.
2
THE CARE WHITE PAPER SERIES IS A PUBLICATION OF THE CENTER FOR CULTURE-CENTERED APPROACH TO RESEARCH AND EVALUATION (CARE),
NATIONAL UNIVERSITY OF SINGAPORE
CARE seeks to: (a) create a strategic research core for the social scientific study of health communication issues in Asia driven by the cultural worldviews of local communities, (b) develop health communication interventions and poli-cies that are culturally-centered via the participatory capacity of local commu-nities to create culturally meaningful and locally responsive health solutions, (c) disseminate the core principles and lessons learned from the culture-centered projects within Asia and across other sectors of the globe, and (d) build health communication research capacity in Asia by creating a training hub for the next generation of health communica-tion theorists, researchers, practitioners, and policymakers across Asia.
ABOUT CAREFunded by a $1.9 million grant from the National University of Singapore, CARE is a global hub for health communica-tion research that uses participatory and culture-centered methodologies to develop community-driven health com-munication solutions.
CARE is driven by the core principle that communities know best the solutions that are relevant to the problems that they identify as critical. CARE works closely with community organizations, policymakers, program planners and evaluators in developing culturally-cen-tered solutions that are envisioned by community members in the grassroots in response to the problems conceptual-ized by them.
Requests for permission to reproduce the CARE White Paper Series should be directed to the Department of Communications and New Media, Faculty of Arts and Social Sciences, National University of Singapore.
DEPARTMENT OF COMMUNICATIONS AND NEW MEDIA11 Computing Drive, AS6 Level 3National University of Singapore
Singapore 117416T (65)6516-4971 W http://www.fas.nus.edu.sg/cnm
Mohan J. Dutta, [email protected]
Copyright of this paper resides with the author and further publication, in whole or in part, shall only be made by authorization of the author.
Design and layout: Daniel Teo, CARE Research Assistant
CARE is online at http://www.care-cca.com.
GLOBALIZATION, HEALTH INEQUITIES, AND STRUCTURAL TRANSFORMATIONCARE WHITE PAPER SERIES
4 5
Slide 1
Slide 2
Slide 3
Slide 4
GLOBALIZATION DEFINED...
GLOBALIZATION
• Globalizationhasbeenmarkedbytheincreasingflowofgoods,labor,andservicesacrossnationalboundaries.
• Time-spaceconvergence.
• Catalyzedthroughpoliticalandeconomicprinciplesoftradeliberalization,privatizationofresources,minimizationofsubsidiesandminimizationofstate-basedprograms.
GLOBALIZATION PRINCIPLES & TRENDS
• Increasingrelianceonexpert-drivenglobalsolutions.
• Increasingrelianceonthelogicsofthemarketforthedeliveryofhealthandhealthcare.
• Public-privatepartnershipsforthedeliveryofhealthsolutions.
• Minimizationofstate-supportedprogramsforthepublic(Education,Health,Food,Water).
• Landacquisitionandlandgrab.
• Privatizationofcollectiveresourcesandknowledge.
TRENDS IN HEALTH INEQUALITIES
• Increasingconcentrationofeconomicresourcesinthehandsoffew:power.
• Increasingeconomicgapswithincountries:GiniCoefficient(China,India,US).
• Risingunemploymentrates,disenfranchisementofthepoor.
• Largegapsinhealthoutcomesbetweenthehavesandhavenots.
6 7
GLOBALIZATION, HEALTH INEQUITIES, AND STRUCTURAL TRANSFORMATIONCARE WHITE PAPER SERIES
Slide 5
Slide 6
Slide 7
Slide 8
NEO-COLONIALISM OF HEALTHIncreasingly,decisionsaremadebyexpertswhoareoutoftouch
withthelivedexperiencesofcommunitiesatthemargins.
Theeconomicsofhealthinterventions:Moneyflowsandpoliticaleconomy.
Communicativeerasuregoeshand-in-handwithmaterialerasure.
CULTURE-CENTEREDAPPROACH
WHAT IS THE CULTURE-CENTERED APPROACH?
Resistingexpert-drivenmodelsby:
• Renderingimpuretheconceptualcategoriesandmethodsofknowledgeproduction.
• Creatingavenuesforlocalcommunitymembersandleaderstoparticipateinandtodevelopsolutionsthatarealignedwiththeirworldviews.
• Examininghowtraditionalhealthcommunicationtheorieshaveerasedtheculturalvoicesofmarginalizedcommunities.
• Buildingdialogicalspacesforengagementwiththesevoicesfromthemargins.
8
CARE WHITE PAPER SERIES GLOBALIZATION, HEALTH INEQUITIES, AND STRUCTURAL TRANSFORMATION
Slide 9
Slide 10
Slide 11
Slide 12
9
TWO CASES:
SONAGACHI SEX WORKERS PROJECT
HEART HEALTH INDIANA
HEALTH IN OUR HANDS: THE SONAGACHI CASE
• CCAwasusedtoexaminehowtwosexworkercommunitiesinthecityofKolkatainWestBengal,Indiaparticipateincreatingandsustainingtheirownhealthpractices,especiallywithrespecttoHIV/AIDS.
• Community-sexworker(CSWer)ledprojectsliketheSonagachiHIV/AIDSInterventionProgram(SHIP)weredesignedtobeparticipatoryinthattheCSWerscoulddecidedwhatwasimportanttothemwhenitcametomattersoftheirhealth.
• Inthiscase,theexpertwasthecommunity,ratherthansomebodyoutsidethecommunity.Theirownexpertiseanddecisionswereregardedascrucialtotheproject.
TAKING OWNERSHIP OF THE PROJECTLocal ownership defines the problem and the scope of solutions to
be implemented in the community.
“...We realized that to get sex workers to use condoms, go for regular check ups, the first thing we needed to do was determine the root of our problems and figure out ways we can address them. You have to live here to really know what’s going on. You can’t just come in, ask questions, and tell us what to do...”-Lakshmi
COMMITMENT TO THE CAUSEPutting the community at the helm of affairs affects the level of
involvement of community members in projects.
“I could spend my valuable time coming to our meetings because I knew that we were there for each other. We made mistakes, but these were our mistakes. We learned from them, and then we did new things, but all along, we were working together to solve our problems.” -Rani
“This [SHIP] is real. The problems are ours and we can solve them. You are not coming to tell us what to do. So here, we can sit together and figure out what works and what doesn’t. And that makes me have faith in this [SHIP].” -Niyoti
10
CARE WHITE PAPER SERIES GLOBALIZATION, HEALTH INEQUITIES, AND STRUCTURAL TRANSFORMATION
Slide 13
Slide 14
Slide 15
Slide 16
11
COLLECTIVE MOBILIZATION
“As individual sex workers, we were vulnerable. The local political leaders, policemen, and our pimps, they harassed us every day. But today we are together, and we have more power because of that.” -Lakshmi
“We take care of the project that we run here. We work with the doctors, we work with the children, we work with our peers and some of our clients. We try to talk to our peers and convince them of the need to come for regular STD tests. We have been trying very hard to impress upon all of us the need to use condoms.” -Jayanti
LESSONS FROM SHIPStructural changes lie at the heart of addressing vulnerabilities
among populations at the margins.
Sexworkerscooperativebank
Opportunitiesforskillstraining
Creatingsafespacesforchildren
Collectivelyaddressingstructuraloppressions
HEART HEALTH INDIANA• AffordableCareAct:ComparativeEffectivenessResearch• CreatingComparativeEffectivenessInformationCapacitiesin
CommunitiesattheMargins• LakeandMarionCountiesofIndiana;AfricanAmericans;
HeartDisease
Ethnography In-depth Interviews
Focus Groups Community Workshops
ADVISORY BOARD
PEER LEADERS
Community Organization Academic Partner
Community Stakeholders Media Partners
↔ ↔
↔ ↔
12
CARE WHITE PAPER SERIES GLOBALIZATION, HEALTH INEQUITIES, AND STRUCTURAL TRANSFORMATION
Slide 17
Slide 18
Slide 19
Slide 20
13
VOICES OF PATIENTS“Most definitely need more information and need someone to explain it …you know, they would come in and they would just come and go… and one thing I noticed, they come in with the chart, the notions saying the doctor wants you to be on this, the doctor wants you to be on that, well write this, write that, well that’s what the doctor prescribes. Don’t explain nothing.”
“…you know I haven’t talked to the doctor, when the doctor come in, Ok when they thought I was having a heart attack and they put me in the hospital, I’ve seen a doctor once and I stayed out there for four days and I just talked with the nurses and staff. And when a doctor came in, he just come in and how are you feeling. He didn’t say what I was experiencing, you know, anything like that. You’re doing bet-ter, it wasn’t a heart attack. You can go home. And that was it. So if you did have someone at the hospital or even in doctor office that can take the patient aside and then say why are we doing this, then it would be a great help.”
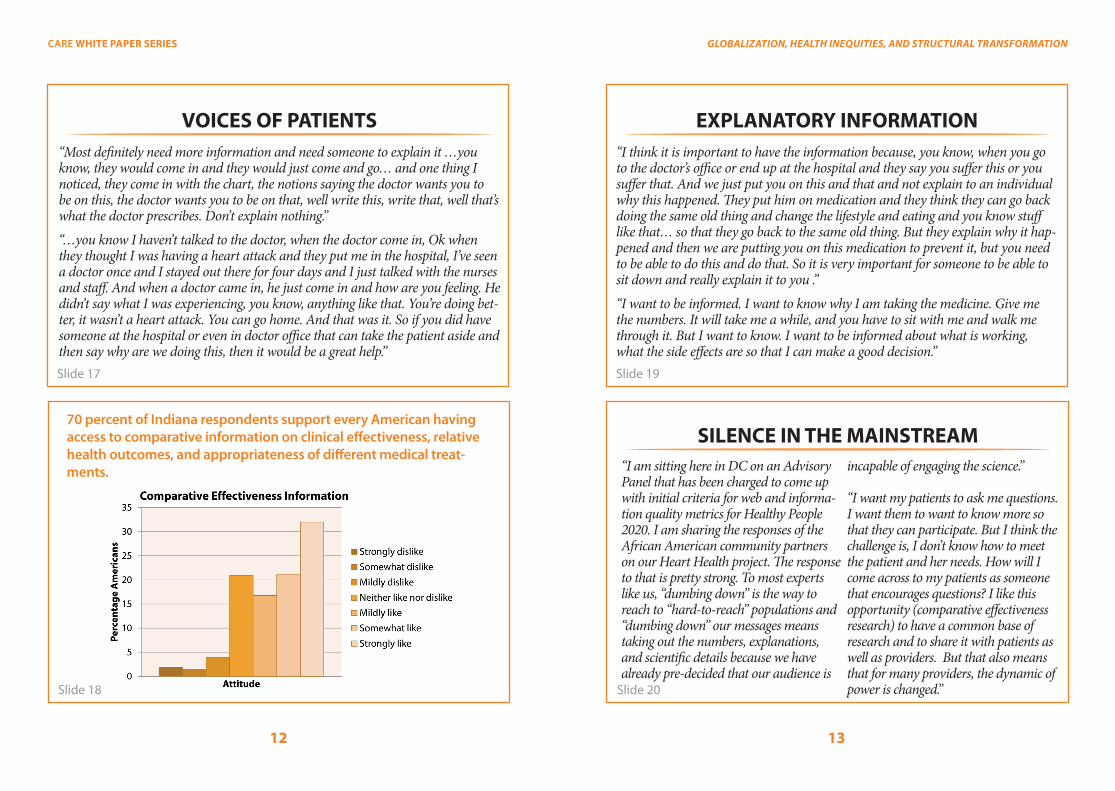
70 percent of Indiana respondents support every American having access to comparative information on clinical effectiveness, relative health outcomes, and appropriateness of different medical treat-ments.
EXPLANATORY INFORMATION“I think it is important to have the information because, you know, when you go to the doctor’s office or end up at the hospital and they say you suffer this or you suffer that. And we just put you on this and that and not explain to an individual why this happened. They put him on medication and they think they can go back doing the same old thing and change the lifestyle and eating and you know stuff like that… so that they go back to the same old thing. But they explain why it hap-pened and then we are putting you on this medication to prevent it, but you need to be able to do this and do that. So it is very important for someone to be able to sit down and really explain it to you .”
“I want to be informed. I want to know why I am taking the medicine. Give me the numbers. It will take me a while, and you have to sit with me and walk me through it. But I want to know. I want to be informed about what is working, what the side effects are so that I can make a good decision.”
SILENCE IN THE MAINSTREAM“I am sitting here in DC on an Advisory Panel that has been charged to come up with initial criteria for web and informa-tion quality metrics for Healthy People 2020. I am sharing the responses of the African American community partners on our Heart Health project. The response to that is pretty strong. To most experts like us, “dumbing down” is the way to reach to “hard-to-reach” populations and “dumbing down” our messages means taking out the numbers, explanations, and scientific details because we have already pre-decided that our audience is
incapable of engaging the science.”
“I want my patients to ask me questions. I want them to want to know more so that they can participate. But I think the challenge is, I don’t know how to meet the patient and her needs. How will I come across to my patients as someone that encourages questions? I like this opportunity (comparative effectiveness research) to have a common base of research and to share it with patients as well as providers. But that also means that for many providers, the dynamic of power is changed.”
14
CARE WHITE PAPER SERIES GLOBALIZATION, HEALTH INEQUITIES, AND STRUCTURAL TRANSFORMATION
Slide 21
Slide 22
Slide 23
Slide 24
15
Face-to-FacePeer LeadersCommunity Advocates
New Media
Traditional Media
Meetings with policymakers
Black Expo and Health Fairs
Town-hall meetings
Doctor’s Offices
Churches
Print stories, interviews
Radio stories, interviews
TV stories, interviews
DVDs
Website
YouTube
Mobile Van
Postcards
16
CARE WHITE PAPER SERIES GLOBALIZATION, HEALTH INEQUITIES, AND STRUCTURAL TRANSFORMATION
Slide 25
Slide 26
Slide 27
Slide 28
17
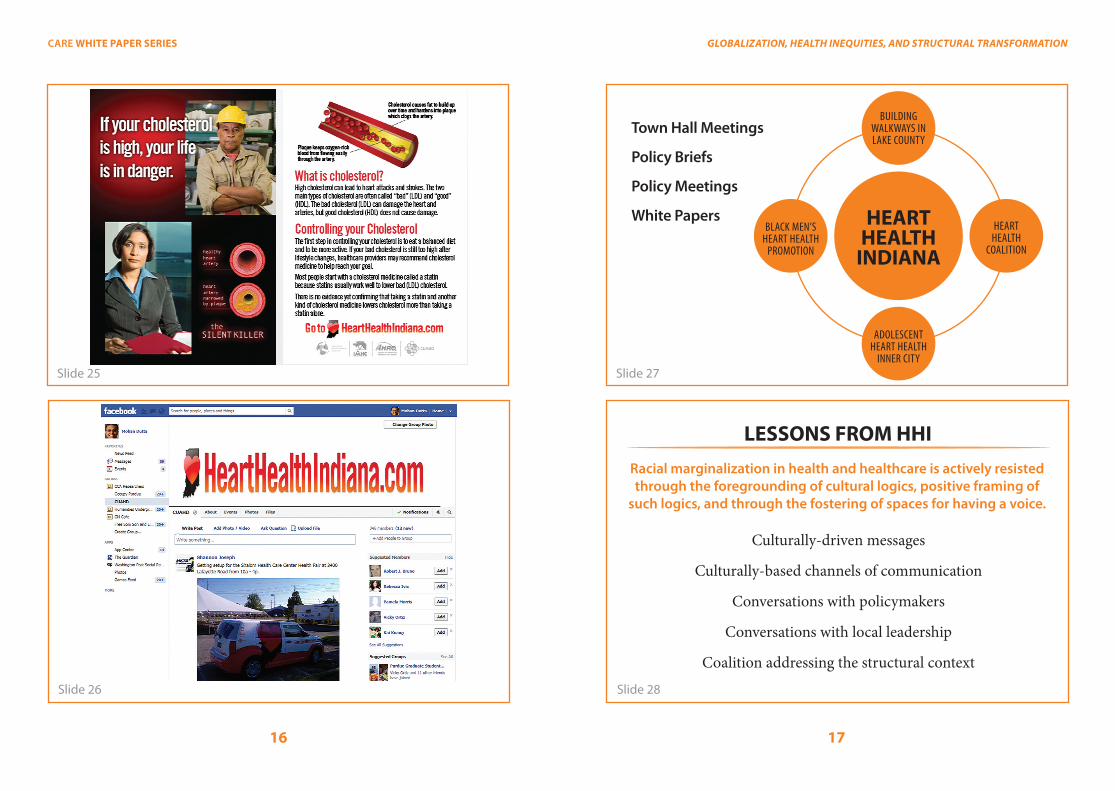
HEARTHEALTH
INDIANA
ADOLESCENT HEART HEALTH
INNER CITY
BLACK MEN’SHEART HEALTH
PROMOTION
HEARTHEALTH
COALITION
BUILDINGWALKWAYS INLAKE COUNTY
Town Hall Meetings
Policy Briefs
Policy Meetings
White Papers
LESSONS FROM HHIRacial marginalization in health and healthcare is actively resisted through the foregrounding of cultural logics, positive framing of
such logics, and through the fostering of spaces for having a voice.
Culturally-drivenmessages
Culturally-basedchannelsofcommunication
Conversationswithpolicymakers
Conversationswithlocalleadership
Coalitionaddressingthestructuralcontext
18
CARE WHITE PAPER SERIES
Slide 29
Slide 30
HEALTH IN OUR HANDS: OUTCOMES
Collectively,theseprojectssuggestthat:
• Collectivemobilizationofthecommunitydoespositivelyaffectthehealthofthecommunity.
• “Thepowertochangeourhealthlieswithus,andnotinthehandsofpeopleoutsideourcommunity.”
• Communitymembersidentifystructuresassitesofchangeandworkcollectivelytowardchallengingthesestructures.
THANK YOU





























