Embed Size (px)
Citation preview

CARE INTERNATIONAL – SOMALIA
NUTRITION SMART SURVEY
FINAL REPORT
BADHAN DISTRICT, SANAG REGION, SOMALIA
OCTOBER 2019

i
ACKNOWLEDGMENT
CARE Somalia would like to pleasantly acknowledge the support of everyone who was
involved in successful execution of the SMART survey in Badhan District, Sanaag Region.
The following played a key role;
▪ OFDA for their financial support to carry out the SMART survey
▪ Ministry of Health for their help in survey planning, coordination and
implementation
▪ Community leaders for good reception and provision of household lists for their
villages
▪ Parents and caretakers for availing their children for assessment as well as for
providing other relevant data for the study
▪ Somalia Cluster’s Assessment and Information Management Working Group for
their technical review and validation of the survey protocol and results.
▪ Care Somalia staff for the management of personnel, logistics planning and field
implementation of the survey
▪ Field supervisors and data collectors for their hard work and dedication during
data collection
Report compiled by:
Epistat Research Consultants

ii
TABLE OF CONTENTS
ACKNOWLEDGMENT ................................................................................ I
LIST OF TABLES .................................................................................... III
LIST OF FIGURES .................................................................................. IV
LIST OF ANNEXES .................................................................................. IV
ACRONYMS AND ABBREVIATIONS ................................................................ V
EXECUTIVE SUMMARY ............................................................................. VI
1.0 INTRODUCTION ................................................................................ 1
1.1 Background .................................................................................. 1
1.2 Health and nutrition situation ............................................................ 2
1.3 Justification of the survey ................................................................ 2
1.4 Survey objectives ........................................................................... 3
1.4.1 Specific Objectives .................................................................... 3
1.5 Survey location and timing ................................................................ 3
2.0 METHODOLOGY ................................................................................ 4
2.1 Study design ................................................................................. 4
2.2 Target group ................................................................................ 4
2.3 Data and data collection methods ....................................................... 4
2.4 Sample size determination ................................................................ 5
2.4.1 Anthropometry sample size .......................................................... 5
2.4.2 Summary of sampling methods ...................................................... 6
2.5 Organization of the survey ................................................................ 6
2.5.1 Recruitment and Composition of survey teams ................................... 6
2.5.2 Training of the survey teams ........................................................ 7
2.5.3 Field Data Collection ................................................................. 7
2.6 Data Management .......................................................................... 7
2.6.1 Data Quality Control .................................................................. 7
2.6.2 Data Collection Tools ................................................................. 8
2.6.3 Data Entry and Analysis .............................................................. 8
3.0 RESULTS- BADHAN DISTRICT ................................................................. 9
3.1 Anthropometric Results.................................................................... 9
3.1.1 Distribution by age and sex .......................................................... 9
3.1.2 Prevalence of Wasting (WHZ) ...................................................... 10

iii
3.1.3 Prevalence of Acute Malnutrition by MUAC ...................................... 12
3.1.4 Prevalence of Underweight (WAZ) ................................................ 14
3.1.5 Prevalence of Stunting (HAZ) ...................................................... 15
3.1.6 Mean z-scores, Design Effects and excluded subjects ......................... 16
3.2 Child morbidity and immunization coverage ......................................... 16
3.2.1. Child Morbidity ..................................................................... 16
3.2.2 Health seeking behaviour .......................................................... 17
3.2.3 Child immunization, vitamin a supplementation, and deworming ........... 18
4.0 CONCLUSION ................................................................................. 20
5.0 RECOMMENDATIONS ......................................................................... 21
6.0 ANNEXES ...................................................................................... 22
LIST OF TABLES
Table 1: Summary of Main Survey Results ..................................................... vi
Table 2: Survey target group ..................................................................... 4
Table 3: Data and collection methods .......................................................... 4
Table 4: Sample size determination ............................................................ 5
Table 5: Summary of survey completeness .................................................... 9
Table 6: Distribution of age and sex of sample ............................................... 9
Table 7: Prevalence of acute malnutrition based on weight-for-height z-scores (and/or
oedema) and by sex ............................................................................. 11
Table 8: Distribution of acute malnutrition and oedema based on weight-for-height z-
scores .............................................................................................. 12
Table 9: Prevalence of acute malnutrition by age, based on weight-for-height z-scores
and/or oedema ................................................................................... 12
Table 10: Prevalence of acute malnutrition based on MUAC cut off's (and/or oedema)
and by sex......................................................................................... 13
Table 11: Prevalence of underweight based on weight-for-age z-scores by sex ....... 14
Table 12: Prevalence of stunting based on height-for-age z-scores and by sex ........ 15
Table 13: Mean z-scores, Design Effects and excluded subjects ......................... 16

iv
LIST OF FIGURES
Figure 1: Badhan Seasonal Calendar ............................................................ 3
Figure 1: Age and sex pyramid ................................................................. 10
Figure 2: Distribution of WHZ z-scores for the surveyed population ..................... 11
Figure 3: Prevalence of acute malnutrition by age, based on MUAC cut offs and/or
edema ............................................................................................. 14
Figure 4: Common illnesses reported ......................................................... 17
Figure 5: Health seeking behavior ............................................................. 17
Figure 6: Vitamin A Supplementation, Deworming and measles vaccination ........... 19
LIST OF ANNEXES
Annex 1: List of sampled clusters ............................................................. 22
Annex 2: Badhan District Plausibility report ................................................. 23
Annex 3: Badhan District Standardization test report ...................................... 24
Annex 4: Badhan District calendar of events, 2019 ......................................... 27

v
ACRONYMS AND ABBREVIATIONS
AIMWG Assessment and Information Management Working Group
CHW Community Health Worker
CI Confidence Interval
CMAM Community Management of Acute Malnutrition
DEFF Design Effect
ENA Emergency Nutrition Assessment
FSNAU Food Security and Nutrition Analysis Unit
GAM Global Acute Malnutrition
HAZ Height for Age Z-score
HH/s Household/s
IDPs Internally Displaced Persons
IMCI Integrated Management of Childhood Illnesses
IPC Integrated Phase Classification
IYCF Infant and Young Child Feeding
KAP Knowledge, Attitudes and Practices
LCL Lower Confidence Limit
MIYCN Maternal, Infant and Young Child Nutrition
MOH Ministry of Health
MUAC Mid Upper Arm Circumference
ODK Open Data Kit
OFDA Office of Foreign Disaster Assistance
OTP Outpatient Therapeutic Programme.
PPS Probability proportional to size
SAM Severe Acute Malnutrition
SD Standard Deviation
SMART Standardized Monitoring and Assessment of Relief and
Transitions
TEM Technical Error of Measurement
TSFP Targeted Supplementary Feeding Program
UCL Upper Confidence Limit
VAS Vitamin A Supplementation
WASH Water, Sanitation and Hygiene
WAZ Weight for Age Z-Score
WHO World Health Organization
WHZ Weight for Height Z- Score

vi
EXECUTIVE SUMMARY
CARE has been providing emergency relief and lifesaving assistance to the Somali people
since 1981. Since then, its programs have evolved to include water and sanitation, Food
security and livelihood, Nutrition and Education. CARE Somalia is currently operational
in the northern regions of Puntland and Somaliland1. The nutrition program being
implemented in 21 villages of Badhan and Lascanod Districts aims to address high
malnutrition rates through treatment of Acutely Malnourished Children, pregnant and
lactating women, referral and treatment of severely malnourished cases with medical
complication as well as community based IYCF programs for improving IYCF practices
in the community.
With financial support from the Office of Foreign Disaster assistance (OFDA), CARE
Somalia conducted a SMART survey in Badhan District in October 2019. The goal of the
survey was to determine a district representative prevalence of acute malnutrition in
Badhan district. The survey was also a follow up to the last FSNAU Post Deyr 2019 survey
and its findings will be used to inform for baseline/continuation of the project beyond
2019
The SMART survey adopted a cross-sectional study design applying two-stage cluster
sampling based on the probability proportional to population size (PPS). The first stage
involved the selection of 36 clusters/villages by the ENA software while the second
stage involved the selection of 16 households in each of the sampled clusters to be
surveyed through simple random sampling. The survey targeted 522 children from 564
households for the anthropometric survey as determined by ENA for SMART (July 19,
2015 update). Eventually, a total of 552 households from 36 clusters were surveyed
with 689 children 6-59 months included in the survey. The key findings of the survey
are shown in the table below;
Table 1: Summary of Main Survey Results
SUMMARY OF SURVEY RESULTS, OCTOBER 2019
INDICATOR N n % 95% CI
ANTHROPOMETRIC RESULTS (6-59 MONTHS) WHO 2006
Wasting (WHZ)
Prevalence of global malnutrition
(<-2 z-score and/or oedema)
678 91 13.4 10.5 – 17.0
Prevalence of moderate malnutrition (<-2
z-score and >=-3 z-score, no oedema)
80 11.8 9.0-15.4
1 https://www.care-international.org/where-we-work/somalia

vii
Prevalence of severe malnutrition (<-3 z-
score and/or oedema)
11 1.6 0.9 – 2.8
Prevalence of GAM by MUAC
Prevalence of global malnutrition (< 125
mm and/or oedema)
689 24 3.5 2.1-5.8
Prevalence of global malnutrition (< 125
mm and >= 115 mm, no oedema)
22 3.2 1.9-5.4
Prevalence of global malnutrition (< 115
mm and/or oedema)
2 0.3 0.1-1.2
Underweight (WAZ)
Prevalence of underweight (<-2 z-score) 685 90 13.1 11.0-15.6
Prevalence of moderate underweight (<-2
z-score and >=-3 z-score)
86 12.6 10.5-14.9
Prevalence of severe underweight (<-3 z-
score)
4 0.6 0.2-1.5
Stunting (HAZ)
Prevalence of stunting (<-2 z-score) 673 83 12.3 9.9-15.3
Prevalence of moderate stunting (<-2 z-
score and >=-3 z-score)
69 10.3 8.3-12.7
Prevalence of severe stunting (<-3 z-
score)
14 2.1 1.2-3.6
CHILD IMMUNIZATION, VITAMIN A SUPPLEMENTATION AND DEWORMING
Measles immunization( 9-59 months) –(
Card and Recall)
660 420 63.6 58.5-69.2
Vitamin A supplementation coverage
children 6-59 months
689 454 65.9 62.3- 69.3
Deworming for Children (12-59 months) in
the last 6 months
615 252 41.0 37.2-45.0
CHILD MORBIDITY AND HEALTH SEEKING BEHAVIOR
Prevalence of reported illness (6-59
months) 14 days mothers/caregivers
recall
689 256 37.2 33.6-40.8
Fever 224 87.5 82.8-91.3
Cough 172 67.2 61.1-72.9
Diarrhea 40 15.6 11.4-20.7
Skin infections 10 3.9 1.9-7.1
Eye infections 1 0.4 0.01-2.7

viii
Other illnesses 24 9.4 6.1-13.6
Health seeking for sick children 129 50.4 44.1-56.7
Main location of health seeking –Private
health facilities
129 36 37.2 28.9-46.2
The findings revealed a nutrition situation which is serious as evidenced by the GAM
prevalence of 13.4% (10.5 – 17.0 95% C.I.) based on the WHO emergency thresholds.
Based on the survey findings, the following actions were recommended to improve
delivery of health and nutrition services in Badhan District;
1) CARE Somalia should continue with nutrition services in Badhan District and scale
up to uncovered locations in order to address the serious levels of malnutrition.
Outreach services need to be considered in volatile or hard to reach areas.
2) Screening for malnourished cases by MUAC at the community level needs to be
enhanced. This will help contain the situation and avoid at risk cases getting
malnourished, while also having moderately malnourished cases treated early.
3) The indicators for Deworming, Vitamin A supplementation and immunization
performed below the WHO targets. There is therefore nee to scale up community
activities to promote the uptake of vitamin A and deworming, as well as promoting
the uptake of other immunization services.
4) Strengthen the routine Vitamin A supplementation and deworming. This should be
given more priority to improve the indicators considering the stability in the area,
coverage and access to the health facilities.
5) Enhance health facility documentation. A training can be conducted on the health
facility staff on documentation of routine activities. This can be accompanied by
periodic data audits and verification exercises.
6) Considering the effect malnutrition has on the younger children, there is need to
strengthen the MIYCN activities in the district, with a key focus on Exclusive
breastfeeding and complimentary feeding, while also improving on poor practices
such as bottle feeding. A significant proportion of 38.5% of the children in the KAP
survey conducted in the area had been bottle fed.
7) A capacity assessment should be done on the public health facilities, including the
lower levels of care in the community with a view of promoting customer service
and promoting services access.

1
1.0 INTRODUCTION
1.1 Background
Badhan district is among the four administrative districts of Sanaag region located on
the north eastern tip of Somaliland neighboring Sool and Togdheer regions. The
population of Sanaag region is estimated at 270,367 (UNDP 2005)2. More than 79% of
the population live in the rural areas predominantly practicing pastoral as the main
source of livelihood with pockets of agro-pastoral areas. Over the years, the region has
experienced recurring droughts and floods which depleted livestock herds adversely
and resulted in urban migration. Approximately, 5,000 people from the region were
displaced due to riverine and flash floods in May 20193. Most of the affected internally
displaced persons (IDPs) have left rural areas in Sanaag, Lower Shabelle, Bakool and
Bay to areas within or outside their region Political instability surrounding
administrative ownership of the region between Somaliland and Puntland remain a huge
challenge to the security and overall humanitarian effort in Badhan District and the
entire Sanaag region.
CARE has been providing emergency relief and lifesaving assistance to the Somali people
since 1981. Its main program activities since then have included projects in water and
sanitation, sustainable pastoralist activities, civil society and media development,
small-scale enterprise development, primary school education, teacher training, adult
literacy and vocational training. CARE Somalia is currently operational in the northern
regions of Puntland and Somaliland4.
Since 2018 CARE has been implementing Nutrition, health and FSL services in Badhan
and Lascanod covering 21 villages. The CARE nutrition program aimed to address the
high malnutrition rates through treatment of Acutely Malnourished Children under 5,
pregnant and lactating women, referral and treatment of complicated cases of SAM and
improving IYCF practices amongst the community through community based IYCF
programs.
CARE International received a grant from OFDA/USAID to carry out humanitarian
assistance in Bari, Galgadud, Mudug, Nugaal, Sanaag, Sool, and Togdheer regions of
Puntland, Galgadud and Somaliland. The interventions happened over 1-year period
from October 2018 to September 2019. The project provided temporary employment,
treatment services for acutely malnourished children and pregnant and lactating
women, basic health services, protection services, safe water to communities including
hygiene promotion as well as provision of WASH Non-Food Items (mainly hygiene kits)
2 UNDP population Figure - 2005 3 Food and Nutrition Analysis Post Gu 2019, Technical Report No xI. 50, august 18, 2019 4 https://www.care-international.org/where-we-work/somalia

2
to vulnerable households. The project aimed a total reach of 247,671 people for
assistance; equivalent to 22% of the population in IPC 3 and 4 in these regions5.
1.2 Health and nutrition situation
Sanaag region has consistently recorded serious GAM levels. Based on the FSNAU
assessments conducted in the region, the Post Deyr in 2017 recorded a GAM rate of
13.8%, with 12.6% recorded in a similar assessment in 2018. The post Gu 2019 recorded
a GAM rate of 15.8% (11.6-21.1) which showed a deteriorating nutrition situation. In the
absence of large-scale humanitarian assistance, food security is expected to rapidly
deteriorate to emergency IPC Phase 4 in Northern Inland Pastoral, East Golis Pastoral
of Sanaag6.
CARE Somalia, with the support of the ministry of health Puntland are supporting Infant
and Young Child Feeding (IYCF) programming at all levels of the nutrition system in
order to have an integrated and comprehensive approach of delivering basic nutrition
services. With financial support from OFDA/USAID, CARE has been supporting 18 sites
covering 14 villages through 2 mobile teams and 2 static sites.
A baseline IYCF survey was conducted in September 2018 in Sool and Sanag region in
our areas of operation (Badhan, Ceelafweyn, Erigavo, Lascanod). The IYCF end line
study was conducted in Bari, Sool and Sanag region (Bosaso, Badhan, Ceelafweyn,
Erigavo, Lascanod and Taleh) in September 2019. The survey findings showed that
exclusive breastfeeding was at 75.8%, while 84% of the children 6-8 months had been
introduced to complimentary foods on a timely manner. Only 29.6 had continued
breastfeeding beyond 2 years with 58.4% breastfeeding beyond one year. Dietary
diversity was low at 4.5% with a meal frequency of 63%.
1.3 Justification of the survey
CARE had been implementing Nutrition, health and FSL services in Badhan District
aimed to address the high malnutrition rates through treatment of Acutely Malnourished
Children below 5 years of age, pregnant and lactating women, referral and treatment
of complicated cases of SAM and improving IYCF practices amongst the community
through community based IYCF programs.
To understand malnutrition situation, CARE planned and conducted the first SMART
survey to determine district representative prevalence of acute malnutrition in Badhan
5 https://reliefweb.int/job/3305148/terms-reference-tor-smart-survey-sool-and-sanag-regions-drought-response-and-recovery 6 SOMALIA Food Security Outlook, June 2019 to January 2020

3
district. The survey was also a follow up to the last FSNAU Post Deyr 2019 survey report.
The findings of this survey will also be used by CARE to inform for baseline and
continuation of the project into 2020.
1.4 Survey objectives
The overall objective of this survey was to assess the prevalence of acute malnutrition
among children 6-59 months in Badhan District.
1.4.1 Specific Objectives
i) To estimate the current prevalence of acute malnutrition among children aged
6 – 59 Months.
ii) To estimate the coverage of measles vaccination (9-59 months), Vitamin A
supplementation (6-59 months) and deworming (12-59 months)
iii) To assess common morbidity among children 6-59 months based on a 2 weeks’
recall
iv) To draft actionable and localized recommendations based on the findings. Using
assessment for action approach clearly indicating the finding, recommendations
actions, timelines and responsibility and monitoring.
1.5 Survey location and timing
The survey was conducted in Somalia’s Badhan District located in Sanag Region in
October 2019. The survey timing fell on post Gu season as shown in Figure 1 below.
Figure 1: Badhan Seasonal Calendar

4
2.0 METHODOLOGY
2.1 Study design
The SMART survey adopted a cross-sectional study design applying two-stage cluster
sampling based on the probability proportional to population size (PPS). The first stage
involved selection of clusters/villages by the ENA software while the second stage
involved the selection of households to be surveyed through simple random sampling.
2.2 Target group
Based on the objectives of this study, the survey targeted children age 6-59 months.
Table 2: Survey target group
Key Indicators Targeted Population
Prevalence of acute malnutrition Children 6-59 months
Child morbidity and health seeking Children 6-59 months
Vitamin A supplementation Children 6-59 months
Measles immunization Children 9-59 months
Deworming Children 12-59 months
2.3 Data and data collection methods
Table 3: Data and collection methods
Data and collection methods
Anthropometric Data
Age - Health cards and birth certificates were used to determine precise age of the
child. Local calendar of events was used in the absence of documentation for children
6-59 months
Sex – Was recorded as either ‘f’ for female or ‘m’ for male
Weight - Standardized SECA scales were used
Height - Standard height boards were used for taking length and height. Children less
than 24 months were measured lying down and children greater than or equal to 24
months were measured in standing position
MUAC – Was taken using standardized and MOH approved MUAC tape. All children 6-
59 months were measured on the left arm to the nearest 0.1cm or 1.0 mm
Bilateral oedema - All children were checked for oedema; minimal thumb pressure
was applied to the top of the feet for about 3 seconds
Vitamin A supplementation – All children 6-59 months were assessed for Vitamin A
supplementation in the past one year.
Prevalence of child morbidity – this was assessed based on a 2 weeks (14 days) recall
period for all the children 6-59 months

5
Health seeking behavior – For all the children reported ill, the caregivers were
assessed on if and where they sought assistance for their sick children
Measles vaccination – Measles vaccination either by recall or by card was assessed in
all children aged 9-59 months in the survey
Deworming - Supplementation with deworming tablets was assessed in children 12-
59 months in the survey.
2.4 Sample size determination
2.4.1 Anthropometry sample size
The sample size for anthropometric survey was determined using ENA for SMART
software (July 9, 2015 version). As shown below, the population parameters for Badhan
Districts, Sanaag region were used to obtain the number of children and households to
be included in the survey.
Table 4: Sample size determination
Population Parameters Value Rationale/Source
Estimated Prevalence of
GAM (%) 15.8%
Somalia June-July 2019 surveys, FSNAU.
East Golis (Sanag) reported a GAM of
15.8% (11.6-21.1)
Desired precision 4 Reasonable precision in consideration of
estimated GAM and associated resources
Design Effect 1.5 Was adjusted due to high DEFF 2.9
reported for East Golis survey
Children to be included 522
Average HH Size 5.3 Somalia June-July 2019 surveys, FSNAU
% Children under 5s 20%
Adjusted from the Somalia June-July
2019 surveys, FSNAU of 26.8% for East
Golis (Sanag)
%Non-response Households 3% Anticipated Non-Response Rate
Households to be included 564
Number of households per cluster
The number of households to be completed per day in each cluster was determined
according to the time each team could spend conducting the survey excluding travel
time to the field and back, initial introduction and breaks.
The total amount of time available to work in a day was 9 hours (8:00 am – 5:00 pm).
After exclusion of the travelling time, the initial introduction and household and lunch
break, the amount of time left to conduct the survey was 7 hours. The amount of time

6
to be spent conduct the survey in one households was 25 minutes. The details below
were taken into consideration when performing this calculation based on the Badhan
District context:
▪ Departure from the base at 8:00 am and back at 5:00 pm.
▪ Average return travel time for each cluster: 1 hours
▪ Duration for initial introduction and selection of households: 0.5 hours
▪ Time spent to move from one household to the next: 5 minutes
▪ Average time in the household: 20 minutes
▪ Breaks: 1 lunch/prayer break of 0.5 hours
𝑛ℎℎ =(9−1−0.5−0.5)60min
20+5 = 16.8 households (this is rounded down to 16).
Based on this calculation, 16 households were planned per village/cluster to be included
in the survey.
Number of Clusters for Badhan District
The number of clusters for Badhan district was determined by dividing the total
households sample and 16 households (representing one cluster) i.e. number of clusters
=564/16 = 35.3, this was rounded up to 36 clusters.
2.4.2 Summary of sampling methods
First stage Cluster sampling
The first stage involved the selection of 36 clusters in Badhan district using the ENA for
SMART software based on population proportion to size (PPS). This was done using most
recent list of villages with their population sizes.
Second stage sampling
The second stage involved selection of 16 households in each of the 36 sampled clusters.
With the assistance of village leaders, household listing was done on the survey day
followed by simple random sampling using a random number generator mobile
application. Clusters with households above 200 or sparsely populated were segmented
before applying simple random selection of the households.
2.5 Organization of the survey
2.5.1 Recruitment and Composition of survey teams
Care Somalia, with the guidance of the consultant developed the criteria for recruiting
7 survey teams, composed of 1 team leader and 2 data collectors. In total the survey
recruited 21 enumerators to form 7 teams each composed of 3 persons. The selection
process considered key factors such as the level of education, previous experience in

7
conducting surveys, the ability to read and communicate in English and undoubted
fluency in Somali dialects.
2.5.2 Training of the survey teams
The survey teams were trained over a period of 4 days in Garowe town. The training
mainly focused on anthropometric measurements, survey teams, field procedures
translation and back-translation of the questionnaires, data recording using ODK and
second stage sampling. On day 3, standardization test was conducted using 10 healthy
children (6-59 months) to determine enumerators’ precision and accuracy in recording
measurements.
The pre-test was conducted on the fourth day in two non-sampled villages; Badhan-
30ka and Dhanaha. The results from the pre-test were analyzed, feedback shared and
the identified gaps addressed appropriately for each team prior to data collection and
final team formation.
2.5.3 Field Data Collection
The implementation of field data collection was conducted for 7 days. Data was
collected using ODK mobile application. Each team used one mobile phone with two
back-up phones. Close Supervision of the teams was done by the survey consultant,
CARE staff and MOH representative. At the end of each day’s data collection, the survey
manager reviewed all questionnaires for completeness, errors and corrections done
prior to sending the data to the server. Plausibility checks were done on a daily basis
and feedback given to the teams.
2.6 Data Management
2.6.1 Data Quality Control
To ensure data quality, the following measures were put in place;
▪ Review and validation of the protocol and report by the AIMWG
▪ 4-day comprehensive training including standardization and pilot test
▪ Field supervision of the survey teams during data collection by the Ministry of
Health representative, consultant, the CARE program staff
▪ Distribution of enumerator strengths across the teams
▪ Calibration and standardization of the survey equipment
▪ Use ODK platform to collect and organize data
▪ Use of Cluster Control forms for survey outcome for every sampled household
▪ Daily plausibility checks and sharing feedback with the teams every morning
before proceeding to the field
▪ Adequate logistic planning during field work

8
2.6.2 Data Collection Tools
The SMART methodology approved anthropometry tool was used. The guidance of the
Somalia AIMWG was applied designing the additional variables tool. The final tool
combined anthropometry and additional variables (child morbidity, deworming,
measles and vitamin A coverage).
2.6.3 Data Entry and Analysis
The ODK collected was exported into MS Excel, organized and subsequently analyzed.
The anthropometric data was uploaded into ENA for SMART 2011 software (July 9, 2015
version) for quality checks and analysis. Data obtained from additional variables was
reviewed and analyzed using EPI Info 7.

9
3.0 RESULTS- Badhan District
The anthropometric survey in Badhan district targeted 522 children 6-59 months from
564 households. The process of determining clusters led to an adjustment of the
households to 576 households were sampled, after which 5527 households were
surveyed with a cumulative total of 689 children. The summary of the survey
completeness is shown in the table below;
Table 5: Summary of survey completeness
CLUSTERS HOUSEHOLDS CHILDREN 6-59 MONTHS
Planned 36 Planned 564 Planned 522
Surveyed 36 Surveyed 552 Surveyed 689
% surveyed 100% % surveyed 97.9% % surveyed 130%
3.1 Anthropometric Results
All the children aged 6-59 months in the sampled households were included in the
anthropometric survey. This involved taking their requisite measurements (age, sex,
weight, height, MUAC and oedema) to determine their nutritional status based on the
different anthropometric indices.
3.1.1 Distribution by age and sex
There were a total of 689 children in the survey. Among the children, 357 were boys
while 332 were girls hence achieving a boy: girl ratio of 1.1. This shows an equal
representation of both sexes as evidenced by the resulting p-value = 0.3421. The age
ratio of children 6-29 months (younger children) to children 30-59 months (older
children) was 1.02 (The value should be around 0.85). Despite this value showing a
significant difference (p-value = 0.016), the ration was near the expected value of 1.02
the representation of younger and older children in the survey was acceptable.
Table 6: Distribution of age and sex of sample
Boys Girls Total Ratio
AGE (mo) no. % no. % no. % Boy:girl
6-17 91 51.1 87 48.9 178 25.8 1.0
18-29 94 55.3 76 44.7 170 24.7 1.2
30-41 78 49.7 79 50.3 157 22.8 1.0
42-53 74 51.0 71 49.0 145 21.0 1.0
54-59 20 51.3 19 48.7 39 5.7 1.1
Total 357 51.8 332 48.2 689 100.0 1.1
7 There were 24 absent households absent across the 36 clusters

10
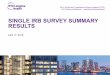
The age and sex distribution is further presented in the graph below, showing an equal
representation of boys and girls in the survey.
Figure 2: Age and sex pyramid
3.1.2 Prevalence of Wasting (WHZ)
Global acute malnutrition (GAM) was defined as <-2 z-scores weight-for-height and/or
oedema and severe acute malnutrition (SAM) was defined as <-3 z-scores weight-for
height and/or oedema.
The survey made exclusions using the SMART flags (WHZ -3 to 3) based on the observed
mean. This is as recommended by the SMART methodology for small scale surveys. The
final sample used for the determination of GAM was 678 children after 11 children were
excluded with z-scores out of range.
Based on the WHZ, the analysis recoded a Global Acute Malnutrition (GAM) rate of 13.4
%( 10.5 - 17.0 95% C.I) and a SAM prevalence of 1.6 %( 0.9 - 2.8 95% C.I.). According the
to the WHO standards, the results indicate a serious nutrition situation in the district.
Boys in the survey were evidently more malnourished than the girls, as depicted by
their respective GAM prevalence in different thresholds.
-100 -80 -60 -40 -20 0 20 40 60 80 100
6-17
18-29
30-41
42-53
54-59
Girls Boys

11
Table 7: Prevalence of acute malnutrition based on weight-for-height z-scores (and/or oedema) and by sex
The graphical presentation of the surveyed population shows a resulting mean of -0.79
and a standard deviation of ±1.04. The deviation of the population curve to the left
indicates a population with a poorly nourished population, as compared to the WHO
reference population.
Figure 3: Distribution of WHZ z-scores for the surveyed population
All
n = 678
Boys
n = 353
Girls
n = 325
Prevalence of global malnutrition
(<-2 z-score and/or oedema)
(91) 13.4 %
(10.5 - 17.0
95% C.I.)
(59) 16.7 %
(11.9 - 23.0
95% C.I.)
(32) 9.8 %
(6.6 - 14.5
95% C.I.)
Prevalence of moderate
malnutrition
(<-2 z-score and >=-3 z-score, no
oedema)
(80) 11.8 %
(9.0 - 15.4
95% C.I.)
(54) 15.3 %
(10.6 - 21.6
95% C.I.)
(26) 8.0 %
(4.8 - 13.1
95% C.I.)
Prevalence of severe malnutrition
(<-3 z-score and/or oedema)
(11) 1.6 %
(0.9 - 2.8 95%
C.I.)
(5) 1.4 %
(0.6 - 3.3 95%
C.I.)
(6) 1.8 %
(0.9 - 3.7 95%
C.I.)

12
The survey did not record any oedema case, with only 1.7% of the children classified as
marasmic. This is shown in the table below;
Table 8: Distribution of acute malnutrition and oedema based on weight-for-height z-
scores
<-3 z-score >=-3 z-score
Oedema present Marasmic kwashiorkor
No. 0
(0.0 %)
Kwashiorkor
No. 0
(0.0 %)
Oedema absent Marasmic
No. 12
(1.7 %)
Not severely malnourished
No. 677
(98.3 %)
The analysis of wasting by age groups showed that younger children were more affected
by malnutrition more than the older children for both severe and moderate wasting.
This is the group on transition from exclusive breast feeding and complementary
feeding, hence more vulnerable to the effects of inadequate nutrition. The findings
may also indicate poor child care practices within this group.
Table 9: Prevalence of acute malnutrition by age, based on weight-for-height z-scores
and/or oedema
Severe
wasting
(<-3 z-score)
Moderate
wasting
(>= -3 and <-2
z-score )
Normal
(> = -2 z
score)
Oedema
Age
(mo)
Tota
l no.
No. % No. % No. % No. %
6-17 176 3 1.7 23 13.1 150 85.2 0 0.0
18-29 166 2 1.2 17 10.2 147 88.6 0 0.0
30-41 153 5 3.3 20 13.1 128 83.7 0 0.0
42-53 144 1 0.7 13 9.0 130 90.3 0 0.0
54-59 39 0 0.0 7 17.9 32 82.1 0 0.0
Total 678 11 1.6 80 11.8 587 86.6 0 0.0
3.1.3 Prevalence of Acute Malnutrition by MUAC
In children aged 6-59 months, the Mid-Upper Arm Circumference (MUAC), with simple
cut-offs of MAM (>=115 mm to <125 mm) and SAM (<115 mm has shown to be a better

13
predictor of mortality risk that is associated with malnutrition8. MUAC is used to monitor
malnutrition trends and for admission and discharge in nutrition programmes since its
measurements can be done easily, quickly and affordably
The analysis of GAM by MUAC involved all the 689 children in the survey. This was in
consideration of the MUAC cut offs applied in Somalia, where GAM is defined as MUAC
<125mm and SAM defined as MUAC <115 mm. The results showed a GAM prevalence of
3.5 % (2.1 - 5.8 95% C.I.) and a SAM prevalence of 0.3 % (0.1 - 1.2 95% C.I.). Girls and
boys in the survey were equally malnourished.
Table 10: Prevalence of acute malnutrition based on MUAC cut off's (and/or oedema)
and by sex
All
n = 689
Boys
n = 357
Girls
n = 332
Prevalence of global malnutrition
(< 125 mm and/or oedema)
(24) 3.5 %
(2.1 - 5.8 95%
C.I.)
(11) 3.1 %
(1.5 - 6.2 95%
C.I.)
(13) 3.9 %
(2.0 - 7.6 95%
C.I.)
Prevalence of moderate
malnutrition
(< 125 mm and >= 115 mm, no
oedema)
(22) 3.2 %
(1.9 - 5.4 95%
C.I.)
(10) 2.8 %
(1.4 - 5.4 95%
C.I.)
(12) 3.6 %
(1.8 - 7.3 95%
C.I.)
Prevalence of severe malnutrition
(< 115 mm and/or oedema)
(2) 0.3 %
(0.1 - 1.2 95%
C.I.)
(1) 0.3 %
(0.0 - 2.1 95%
C.I.)
(1) 0.3 %
(0.0 - 2.3 95%
C.I.)
Further analysis of the wasting by MUAC based on the age groups shows that younger
children 6-17 months and 18-29 months were most affected by malnutrition with most
of the severely acutely malnourished children falling in the 6-17 months category. This
may be indicative of a gap in infant and young child nutrition, where the children
transitioning from exclusive breastfeeding to complimentary feeding may not be getting
adequate nutrition. The findings indicate poor IYCF practices in the district.
8 Chiabi, Andreas, et al. "Weight-for-height z score and mid-upper arm circumference as predictors of mortality in children with severe acute malnutrition." Journal of tropical pediatrics63.4 (2016): 260-266

14
Figure 4: Prevalence of acute malnutrition by age, based on MUAC cut offs and/or
edema
3.1.4 Prevalence of Underweight (WAZ)
Underweight refers to inadequate weight relative to age and is measured using weight-
for-age z-scores (WHO 2006). A child can have a low weight-for-age because they are
short, thin or a bit of both and therefore underweight is considered a composite
indicator for stunting and wasting9.
The analysis of underweight involved 685 children after 4 children were excluded with
z-scores out of range. The survey recorded an underweight prevalence of 13.1 %(11.0 -
15.6 95% C.I.) with a severe underwiehgt prevalence of 0.6 % (0.2 - 1.5 95% C.I.). This
indicates an alert nutrition situation based on the WHO classification of underweight10.
Boys in the survey had a higher prevalence of underweight than girls, with a 0.0%
underweight prevalence in girls. This is detailed in the table below;
Table 11: Prevalence of underweight based on weight-for-age z-scores by sex
All
n = 685
Boys
n = 356
Girls
n = 329
Prevalence of underweight
(<-2 z-score)
(90) 13.1 %
(11.0 - 15.6
95% C.I.)
(60) 16.9 %
(13.3 - 21.1
95% C.I.)
(30) 9.1 %
(6.7 - 12.3
95% C.I.)
9 Tanya K and Carmel D. the relationship between wasting and stunting, policy programming and research implications, 1915-1918. "Technical Briefing Paper 12.4 (July 2014): 8-9 10 Alert/medium 10-19.9

15
Prevalence of moderate
underweight
(<-2 z-score and >=-3 z-score)
(86) 12.6 %
(10.5 - 14.9
95% C.I.)
(56) 15.7 %
(12.4 - 19.8
95% C.I.)
(30) 9.1 %
(6.7 - 12.3
95% C.I.)
Prevalence of severe
underweight
(<-3 z-score)
(4) 0.6 %
(0.2 - 1.5
95% C.I.)
(4) 1.1 %
(0.4 - 3.0
95% C.I.)
(0) 0.0 %
(0.0 - 0.0
95% C.I.)
3.1.5 Prevalence of Stunting (HAZ)
Stunting is defined as a slowing or halting of linear growth or ‘linear growth faltering’.
This is commonly identified by a child falling off the standard growth trajectory
compared to their age as described by the WHO growth standards11. A child is classified
as stunted when their height-for-age is more than two standard deviations below the
WHO Child Growth Standards median.
After exclusion of 16 children whose measurement were out of range, a total of 673
children were included in the analysis of stunting. The survey recording a low stunting12
prevalence of 12.3 %( 9.9 - 15.3 95% C.I.). Boys and girls in the survey were equally
stunted as shown in the table below;
Table 12: Prevalence of stunting based on height-for-age z-scores and by sex
All
n = 673
Boys
n = 348
Girls
n = 325
Prevalence of stunting
(<-2 z-score)
(83) 12.3 %
(9.9 - 15.3
95% C.I.)
(48) 13.8 %
(10.3 - 18.2
95% C.I.)
(35) 10.8 %
(7.6 - 15.0
95% C.I.)
Prevalence of moderate stunting
(<-2 z-score and >=-3 z-score)
(69) 10.3 %
(8.3 - 12.7
95% C.I.)
(38) 10.9 %
(8.1 - 14.6
95% C.I.)
(31) 9.5 %
(6.7 - 13.4
95% C.I.)
Prevalence of severe stunting
(<-3 z-score)
(14) 2.1 %
(1.2 - 3.6 95%
C.I.)
(10) 2.9 %
(1.7 - 4.9
95% C.I.)
(4) 1.2 %
(0.5 - 3.1
95% C.I.)
11 Tanya K and Carmel D. the relationship between wasting and stunting, policy programming and research implications, 1915-1918. "Technical Briefing Paper 12.4 (July 2014): 8-9) 12 WHO classification of stunting , Low <20%

16
3.1.6 Mean z-scores, Design Effects and excluded subjects
The table below presents a summary of the three anthropometric indices as analysed
in the survey. The total number of children 6-59 months included in the survey was 689.
Exclusions were made before analysis for each anthropometric index using the smart
flags, which are based on the observed mean. The final sample used in analysis of
wasting, (WHZ), underweight (WAZ) and stunting (HAZ) is provided in the table below,
with the corresponding mean and the design effect for each index. The standard
deviation for all the indices was within the acceptable range of 0.85 - 1.2 indicating
quality measurements. Details are shown in the table below;
Table 13: Mean z-scores, Design Effects and excluded subjects
Indicator n Mean z-
scores ± SD
Design Effect
(z-score < -2)
z-scores not
available*
z-scores out
of range
Weight-for-Height 678 -0.79±1.04 1.51 0 11
Weight-for-Age 685 -0.89±0.97 1.00 0 4
Height-for-Age 673 -0.69±1.13 1.11 0 16
* contains for WHZ and WAZ the children with oedema.
3.2 Child morbidity and immunization coverage
3.2.1. Child Morbidity
Morbidity data was collected retrospectively based on a two week recall period. All the
caregivers were asked whether their child had suffered any illness and the type of
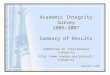
illness two weeks prior to the survey. The findings of the survey show that 37.6% of the
children in the survey had suffered at least one illness two weeks prior to the survey.
Fever and cough were the predominant illnesses, suffered by 87.5% and 67.2% of the
sick children respectively. The other illnesses reported in the survey are shown in the
graph below;

17
Figure 5: Common illnesses reported
3.2.2 Health seeking behaviour
To assess the health seeking behaviour, caregivers were asked what they did the last
time their child was sick. A notable proportioning (49.6%) of the caregivers did not seek
any type of assistance when their child was ill. This may be as a result of the caregivers’
assumption that the illness was not serious enough to warrant any external assistance.
Most of the caregivers who sought assistance preferred private clinics (37.2%) and public
health facilities (27.9%). The other places where the caregivers sought assistance are
shown in the figure below;
Figure 6: Health seeking behavior
87.5%
67.2%
15.6%
3.9%0.4%
9.4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
FEVER COUGH DIARRHOEA SKIN INFECTION EYE INFECTIONSOTHER ILLNESES
I LLNESSES REPORTED
0% 5% 10% 15% 20% 25% 30% 35% 40%
Private clinic
Public health facilities/hospital
Phamarcy/chemist
Shop
CHW/Community Nutrition worker
Traditional healer
Religious leaders
37.2%
27.9%10.1%
10.1%
9.3%
3.1%
2.3%Health Seeking Behaviour

18
3.2.3 Child immunization, vitamin a supplementation, and deworming
WHO recommends that Children be supplemented with Vitamin A at 6 months and
subsequently at 6 months’ intervals until a child reaches 5 years old13. Deworming at
least biannually using single doses of albendazole (400 mg) or mebendazole (500 mg) is
recommended as a public health intervention for all young children 12–23 months of
age, preschool children 1–4 years of age, and school-age children 5–12 years of age14.
To assess the coverage of vitamin A supplementation and deworming, the caregivers
were shown vitamin A (6-59 months) and deworming tablets (12-59 months), which was
meant to aid them recall if their children had received such in the past 12 months and
past 6 months respectively. Measles vaccination was also assessed in all children 9-59
months in the survey based on the EPI card or on recall where the cards were not
available.
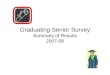
The survey findings show that 65.9% of the children 6-59 months had been
supplemented with vitamin A in the past 12 months, while less than half (44.9% of the
children 12-59 months had been dewormed 6 months prior to the survey. More than half
(63.6%) of the children 9-59 months in the sample had been immunized against measles
with only 4.4% being verified by the EPI card. The routine program data in the district
reported a measles coverage of 62.2%15, which is similar to the coverage found in the
survey. The performance of Vitamin A, deworming and also measles fall below the WHO
recommended coverage of 80%, hence the need to put in place measures for scale up
to achieve the desired public health significance.
13 www.who.int/nutrition/publications/vitamins_minerals/en/index.html 14 Deworming and adjuvant interventions for improving the developmental health and well-being of children in low- and middle-income countries: a systematic review and meta-analysis 15 EPI coverage, Badhan district

19
Figure 7: Vitamin A Supplementation, Deworming and measles vaccination
65.9%
44.9%
63.6%
0%
10%
20%
30%
40%
50%
60%
70%
Vitamin A (6-59 months) Deworming (12-59 months) Measles (9-59 months)
Vaccination and Immunization

20
4.0 conclusion
The nutrition situation in Badhan district is serious as evidenced by the GAM prevalence
of 13.4% (10.5 – 17.0 95% C.I.) based on the WHO emergency thresholds. A nutrition and
food security assessment had been conducted in East Golis (Sanaag) where Badhan
district is included, which showed a GAM of 15.8% (11.6-21.1). The area has consistently
recorded serious nutrition levels based on the GAM prevalence from the FSNAU
assessments. The Post Deyr Food security and nutrition assessment conducted in 2017
recorded a GAM rate of 13.8%, with 12.6% recorded in a similar assessment in 2018.
GAM prevalence by MUAC was low 3.5% (2.1- 5.8 95% CI) as compared to the prevalence
by WHZ. This is expected as MUAC is more sensitive at high specificity levels than WHZ
for identifying children at high risk of death. It is worth noting that MUAC and WHZ do
not always identify the same children as having SAM hence the difference in the
prevalence of malnutrition by the 2 criteria16. The 2 criteria should be used in
management of acute malnutrition, with MUAC being the most effective for screening
children at the community level.
Based on the SMART survey results, the younger children (6-29 months) were the most
affected by acute malnutrition as compared to the older children. Malnutrition at such
an early age can be attributed to the fact that infants have high nutrient requirements
and are more susceptible to infection especially at this age when they are being
introduced to solid and semi-solid foods. The high rates of wasting in this group may be
suggestive of inadequate nutrition and care practices within this group, hence a need
to enhance child care practices through MIYCN programs in the district. The prevalence
of underweight was alert at 13.1% (11.0 - 15.6 95% C.I.) while the prevalence of stunting
was low at 12.3% (9.9 – 15.3, 95% C.I).
The assessment of child morbidity showed a morbidity rate of 37.6%, with the main
illnesses reported being fever and cough at 81.5% and 67.2% respectively. It is however
concerning that almost half (49.6%) of the caregivers with sick children did not seek
any kind of assistance when the children were sick. This may be due to factors like the
caregivers not prioritizing some illnesses, distance to the health facilities or the
caregivers not well informed on when and where to seek assistance when the child is
sick. Private facilities were the most preferred by the caregivers (37.2%) as compared
to the public health facilities (27.9%). The cost associated with the private facilities,
and the low preference to public health facilities may be a contributing factor for some
caregivers not seeking treatment for their sick children.
Although vitamin A supplementation was below the WHO recommended threshold of
80%, it was commendable that 65.9% of the children had been supplemented at least
16 Grellety E, Golden MH. Weight-for-height and mid-upper-arm circumference should be used independently to diagnose acute malnutrition: policy implications. BMC Nutr. 2016;2:10.

21
once in the past 12 months. Deworming was low at 44.9% for children 12-59 months
while measles vaccination was 63.6%. measles vaccination was majorly confirmed by
recall, hence the need to improve on the documentation of vaccinations through the
EPI program, as well as documenting the births, which will help in timely and effective
immunizations. There is a need to improve the awareness on immunizations and
vaccinations so as to reach levels which can bring a public health significance.
5.0 Recommendations
1) CARE Somalia should continue with nutrition services in Badhan District and scale
up to uncovered locations in order to address the serious levels of malnutrition.
Outreach services need to be considered in volatile or hard to reach areas.
2) Screening for malnourished cases by MUAC at the community level needs to be
enhanced. This will help contain the situation and avoid at risk cases getting
malnourished, while also having moderately malnourished cases treated early.
3) The indicators for Deworming, Vitamin A supplementation and immunization
performed below the WHO targets. There is therefore nee to scale up community
activities to promote the uptake of vitamin A and deworming, as well as promoting
the uptake of other immunization services.
4) Strengthen the routine Vitamin A supplementation and deworming. This should be
given more priority to improve the indicators considering the stability in the area,
coverage and access to the health facilities.
5) Enhance health facility documentation. A training can be conducted on the health
facility staff on documentation of routine activities. This can be accompanied by
periodic data audits and verification exercises.
6) Considering the effect malnutrition has on the younger children, there is need to
strengthen the MIYCN activities in the district, with a key focus on Exclusive
breastfeeding and complimentary feeding, while also improving on poor practices
such as bottle feeding. A significant proportion of 38.5% of the children in the KAP
survey conducted in the area had been bottle fed.
7) A capacity assessment should be done on the public health facilities, including the lower
levels of care in the community with a view of promoting customer service and promoting
services access.

22
6.0 Annexes
Annex 1: List of sampled clusters
Village name Population size Cluster Number
Badhan-Geeldoora 1 1272
1
Badhan-Geeldoora 2 2
Badhan-Waaberi 1 2915
3
Badhan-Waaberi 2 4
Badhan-Horseed 1 3074
5
Badhan-Horseed 2 6
Badhan-Horseed 3 7
Badhan-Iftin 1 2385
8
Badhan-Iftin 2 9
Badhan-Iftin 3 10
Mindigale 1 2862
11
Mindigale 2 12
Ceelbuh 1 2385
13
Ceelbuh 2 14
Ceelbuh 3 15
Rad 1 1590
16
Rad 2 17
Laako 1166 18
Cawsane 1 2385
19
Cawsane 2 20
Gumar 1219 21
Xarka-Dheere 636 22
Mindhicir 1272 23
Haylaan 1 2385
24
Haylaan 2 25
Haylaan 3 26
Caadsaaran 1590 27
Dooxadheer 1060 28
Faracad 689 29
Hadaftimo 1 4134
30
Hadaftimo 2 31
Hadaftimo 3 32
Gurmalle 398 33
Qoyan 636 34
Gooraan 795 35
Habarshiro 1113 36

23
Badhan-Golis 1034 RC
Jiicanyo 636 RC
Bendersamo 636 RC
Hadaftimo 4134 RC
Badhan-30ka 530 Pretest
Dhanaha 795 Pretest
Annex 2: Badhan District Plausibility report
Plausibility check for: SOM_102019_CARE_BADHAN.as
Standard/Reference used for z-score calculation: WHO standards 2006
(If it is not mentioned, flagged data is included in the evaluation. Some parts of this plausibility
report are more for advanced users and can be skipped for a standard evaluation)
Overall data quality
Criteria Flags* Unit Excel. Good Accept Problematic Score
Flagged data Incl % 0-2.5 >2.5-5.0 >5.0-7.5 >7.5
(% of out of range subjects) 0 5 10 20 0 (1.6 %)
Overall Sex ratio Incl p >0.1 >0.05 >0.001 <=0.001
(Significant chi square) 0 2 4 10 0 (p=0.341)
Age ratio(6-29 vs 30-59) Incl p >0.1 >0.05 >0.001 <=0.001
(Significant chi square) 0 2 4 10 4 (p=0.016)
Dig pref score - weight Incl # 0-7 8-12 13-20 > 20
0 2 4 10 0 (5)
Dig pref score - height Incl # 0-7 8-12 13-20 > 20
0 2 4 10 2 (10)
Dig pref score - MUAC Incl # 0-7 8-12 13-20 > 20
0 2 4 10 0 (6)
Standard Dev WHZ Excl SD <1.1 <1.15 <1.20 >=1.20
. and and and or
. Excl SD >0.9 >0.85 >0.80 <=0.80
0 5 10 20 0 (1.04)
Skewness WHZ Excl # <±0.2 <±0.4 <±0.6 >=±0.6
0 1 3 5 0 (0.14)
Kurtosis WHZ Excl # <±0.2 <±0.4 <±0.6 >=±0.6
0 1 3 5 0 (-0.17)
Poisson dist WHZ-2 Excl p >0.05 >0.01 >0.001 <=0.001
0 1 3 5 0 (p=0.054)
OVERALL SCORE WHZ = 0-9 10-14 15-24 >25 6 %
The overall score of this survey is 6 %, this is excellent.

24
Annex 3: Badhan District Standardization test report
Standardisation test results Precision Accuracy OUTCOME
Weight subjects
mean SD
max
Technical
error TEM/m
ean
Coef of
reliability
Bias from
superv
Bias from
median result
# kg kg kg TEM (kg) TEM (%) R (%)
Bias (kg)
Bias (kg)
Supervisor 10 12.
7 2.5
0.2 0.07 0.6 99.9 - 0.81
TEM acceptable R value good Bias reject
Enumerator 1 10
12.7
2.5
0.1 0.06 0.5 99.9 -0.01 0.81
TEM acceptable R value good Bias reject
Enumerator 2 10
12.7
2.4
0.2 0.05 0.4 99.9 0 0.81
TEM acceptable R value good Bias reject
Enumerator 3 10
12.7
2.5
1.5 0.36 2.9 97.9 -0.01 0.81 TEM reject
R value acceptable Bias reject
Enumerator 4 10
12.7
2.5
0.7 0.18 1.4 99.5 -0.04 0.77 TEM poor R value good Bias reject
Enumerator 5 10
12.7
2.4
0.1 0.02 0.2 100 0 0.81 TEM good R value good Bias reject
Enumerator 6 10
12.7
2.5
0.1 0.03 0.2 100 0 0.81 TEM good R value good Bias reject
enum inter 1st 6x10
12.7
2.4 - 0.13 1 99.7 - -
TEM acceptable R value good
enum inter 2nd 6x10
12.7
2.4 - 0.23 1.8 99.1 - - TEM poor R value good
inter enum + sup 7x10
12.7
2.4 - 0.16 1.3 99.5 - -
TEM acceptable R value good
TOTAL intra+inter 6x10 - - - 0.25 2 98.9 -0.01 0.8 TEM reject
R value acceptable Bias reject
TOTAL+ sup 7x10 - - - 0.23 1.8 99.1 - - TEM poor R value good
Height subjects
mean SD
max
Technical
error TEM/m
ean Coef of
Bias from
superv Bias from result

25
reliability
median
# cm cm cm TEM (cm) TEM (%) R (%)
Bias (cm)
Bias (cm)
Supervisor 10 92.
3 10.7
3.8 0.91 1 99.3 - -1.11 TEM poor R value good Bias good
Enumerator 1 10
93.2
10.4
19.1 4.33 4.6 82.6 0.93 -0.19 TEM reject
R value reject Bias good
Enumerator 2 10 92
11.3 1 0.35 0.4 99.9 -0.24 -1.35 TEM good R value good Bias good
Enumerator 3 10
92.4 11 1 0.31 0.3 99.9 0.07 -1.04 TEM good R value good Bias good
Enumerator 4 10
91.7
11.5
3.5 0.97 1.1 99.3 -0.57 -1.69 TEM poor R value good Bias good
Enumerator 5 10
92.4
10.9
0.8 0.19 0.2 100 0.14 -0.97 TEM good R value good Bias good
Enumerator 6 10
91.9
10.1
10.1 2.28 2.5 94.9 -0.39 -1.5 TEM reject R value poor Bias good
enum inter 1st 6x10 92
10.8 - 1.62 1.8 97.7 - - TEM reject
R value acceptable
enum inter 2nd 6x10
92.6
10.7 - 2.56 2.8 94.2 - - TEM reject R value poor
inter enum + sup 7x10
92.3
10.6 - 1.91 2.1 96.6 - - TEM reject
R value acceptable
TOTAL intra+inter 6x10 - - - 2.96 3.2 92.3 -0.01 -1.12 TEM reject R value poor Bias good
TOTAL+ sup 7x10 - - - 2.75 3 93.3 - - TEM reject R value poor
MUAC subjects
mean SD
max
Technical
error TEM/m
ean
Coef of
reliability
Bias from
superv
Bias from
median result
# mm mm
mm
TEM (mm) TEM (%) R (%)
Bias (mm)
Bias (mm)

26
Supervisor 10 144
.7 10.6
4.5 1.76 1.2 97.3 - -0.29 TEM good
R value acceptable Bias good
Enumerator 1 10
146.4
10.9 25 5.83 4 71.2 1.64 1.35 TEM reject
R value reject
Bias acceptable
Enumerator 2 10
141.6 11 10 2.91 2.1 93.1 -3.07 -3.35 TEM poor R value poor Bias good
Enumerator 3 10
143.1
10.6 8 1.96 1.4 96.6 -1.57 -1.85 TEM good
R value acceptable Bias good
Enumerator 4 10
145.6
10.4 10 4.25 2.9 83.3 0.89 0.6 TEM reject
R value reject Bias good
Enumerator 5 10
145.2
12.3 6 1.9 1.3 97.6 0.49 0.2 TEM good
R value acceptable Bias good
Enumerator 6 10
146.3
13.1 23 6.23 4.3 77.4 1.59 1.3 TEM reject
R value reject
Bias acceptable
enum inter 1st 6x10
144.8
11.9 - 4.61 3.2 85.1 - - TEM reject
R value reject
enum inter 2nd 6x10
144.6
10.8 - 5.21 3.6 76.6 - - TEM reject
R value reject
inter enum + sup 7x10
144.7
11.2 - 4.48 3.1 84 - - TEM reject
R value reject
TOTAL intra+inter 6x10 - - - 6.48 4.5 67.3 -0.01 -0.29 TEM reject
R value reject Bias good
TOTAL+ sup 7x10 - - - 5.99 4.1 71.4 - - TEM reject R value reject

27
Annex 4: Badhan District calendar of events, 2019
Badhan District Calender of Events
MONTH SEASONS 2014 2015 2016 2017 2018 2019
January
Diraac
57 45 33 21 9
Mawlid War between
alshabab and
puntland
Campaing
Period for
presidency
Tukoraq war
Farmajo visited
Jubaland president
Puntland
election
February 56 44 32 20 8
Death of Prof
Mohamed Tobeel
Daalo airline
explossion
Farmajo
election
March 55 43 31 19 7
Many immigrants
from yemen
Magclay war
Sima drought
Election of
Hassan Khayre
(Prime
minister
April
GU
54 42 30 18 6
Explossion in
Garowe killing UN
staff
Heavy rains
and flooding
Sima drought Tukoraq
war
May 53 41 29 17 5
Sima drought Tukoraq war
Ramadhan
June 52 40 28 16 4
Ramadhan Ramadhan Ramadhan Tukoraq war
Ramadhan
Idd Ul fitri

28
July
Xagaa
51 39 27 15 3
Dabshid Somalia Prime
Minister visited
Puntland
August 50 38 26 14 2
Jubaland
presidential
elections
Idd ul fitri
Garacad Port
Started
September 49 37 25 13 1
Idd al Adha Idd Al Adha Idd Al Adha Idd Al Adha
October
Deyr
48 36 24 12 0
War between
Puntland and
Galmudug
Scobe?Zoobe
(Bomb attack)
Abdiwali Ali visited
Badhan
November 59 47 35 23 11
Qandala war
December 58 46 34 22 10
Bosaso airport
rebuild
Mowlid Mowlid Mowlid