Embed Size (px)
Citation preview

PREVALENCE OF CARDIOVASCULAR RISK FACTORS AMONG RENAL TRANSPLANT RECIPIENTS ATTENDING NEPHROLOGY
CLINICS IN NAIROBI, KENYA
MMED RESEARCH PRESENTATION AT KENYA ASSOCIATION OF PHYSICIANS 17TH SCIENTIFIC CONFERENCE
•Dr James A. A. Wagude•Prof. E.N. Ogola•Prof. S.O. Mcligeyo•Prof. J.K. Kayima•Dr A.J. Were

Introduction
• Transplantation of the human kidney is the treatment of choice for end-stage renal disease (ESRD) patients.
• 50–60% of deaths in renal transplant recipients (RTR) are attributable to cardiovascular disease1. Death from cardiovascular disease is the most common cause of graft loss2.
• Cardiovascular mortality rates among renal transplant recipients (RTR) and chronic kidney disease (CKD) patients are significantly higher than among those in the general population3.
• RTR are at increased risk of cardiovascular disease (CVD) compared with the same risk factors in the general population4.
1. Ojo AO. Cardiovascular complications after renal transplantation and their prevention. Transplantation 2006; 82:6032. Shirali AC, Bia MJ. Management of cardiovascular disease in renal transplant recipients. J Am Soc Nephrol 2008;
3:491.3. Sarnak MJ, Levey AS. Cardiovascular Disease and Chronic Renal Disease: A New Paradigm. Am J Kidney Dis. 2000;
35:S117–S1314. Dimény E. Cardiovascular disease after renal transplantation. Kidney Int, 2002; 61:S78

CVD Risk Factors in CKD Patients5,6,7
Traditional Risk Factors Nontraditional Risk Factors
Older age* ΨMale sex*Hypertension*Higher LDL cholesterol*Lower HDL cholesterolDiabetes mellitus* ΨCigarette smoking*Physical inactivityMenopauseFamily history of CVDLeft ventricular hypertrophy
Proteinuria/albuminuriaHomocysteineLipoprotein (a) and apolipoprotein (a) isoformsAnemiaAbnormal calcium-phosphate metabolismExtracellular fluid overloadOxidative stressInflammation (C-reactive protein)MalnutritionThrombogenic factorsAltered nitric oxide/endothelin balance
5. Menon V, Sarnak MJ. The Epidemiology of Chronic Kidney Disease Stages 1 to 4 and Cardiovascular Disease: A High-Risk Combination. Am J of Kidney Dis 2005; 45:223–232
6. Kasiske BL. Risk factors for accelerated atherosclerosis in renal transplant recipients. Am J Med 1988; 84:9857. Jardine AG, Fellstrom B, Logan JO, et al. Cardiovascular risk and renal transplantation: post hoc analyses of the
Assessment of Lescol in Renal Transplantation (ALERT) Study. Am J Kidney Dis 2005; 46:529
Study Justification
• Kenya with a population of 38.6 million is estimated to have a prevalence of ESRD of 15.6 per million population8,9 .
• 200 patients on dialysis at Kenyatta National Hospital (KNH) with 20 renal transplants performed annually.
• Major cause of mortality in the renal transplant recipients is cardiovascular disease.
• Data was to formulate strategies for cardiovascular risk reduction and management.
8. Kenya National Bureau of Statistics. Population and Housing Census 2009. Government Printer Nairobi, Kenya, 2010
9. Bamgboye EL. End-Stage Renal Disease in Sub-Saharan Africa. Ethn Dis 2006; 16:S2–9

ObjectivesBroad objective:
• To determine the prevalence of cardiovascular risk factors and to analyze for association of these risk factors with patient variables and immunosuppressant drug use in renal transplant recipients in Nairobi.
Specific objectives: 1. To determine the prevalence of cardiovascular risk factors (hypertension,
dyslipidemia, dysglycemia, obesity, proteinuria, decreased glomerular filtration rate, anemia and cigarette smoking) in RTR attending nephrology clinics in Nairobi
2. To document patient variables of age, gender, duration of dialysis pre-transplant, medications used, cause of CKD, pre-existent diabetes or hypertension, and type and number of renal allografts in RTR and analyze for correlations with the cardiovascular risk factors.
3. To document types of and duration of exposure to immunosuppressant drugs used by RTR and analyze for correlations between these drugs and established cardiovascular risk factors in RTR.

Methods and Patient Selection
Study Design:• Cross-sectional descriptive study between August 2011 and February 2012
Study Population and Sites:• Renal transplant recipients on follow-up at nephrology clinics including KNH
Renal Unit, Parklands Nephrology Centre , KNH and Nairobi Hospital Doctors Plazas
Inclusion Criteria:1. Renal transplant recipients2. Written informed consent 3. Age above 18 years of age
Exclusion Criteria:1. Patients on hemodialysis for any cause.2. Patients with acute kidney failure and acute liver failure
Minimum Sample size:Calculated from other studies to be 87 participants
• Clinical data collected by primary investigator while Lancet laboratory used for investigations.
• All information collected was kept confidential and results disseminated to the patients and physicians.
• Data underwent univariate, bivariate and multivariate testing. A P value less than or equal to 0.05 was considered statistically significant.
Demographic variables:– Age, gender, dialysis duration pre-transplant, cause of CKD if
known, duration of time after transplantation, current medications, number and type of renal transplant, and pre-existent diabetes and hypertension.
Clinical variables:– Obesity, estimated GFR, anemia, proteinuria, smoking,
hypertension , dysglycemia and dyslipidemia.
Methods and Patient Selection

Study Recruitment Flow Chart

RTR CharacteristicsVariable Frequency (Percent), N = 91
Sex
Male 62 (68.1)
Female 29 (31.9)
Site of clinic
KNH Renal Unit 54 (59.3%)
Private nephrology clinics 37 (40.7%)
Transplant donor
Living related 83 (91.2%)
Living unrelated 8 (8.8%)
Cadaveric 0
Previous renal grafts
First 86 (94.5%)
Second 5 (5.5%)
Mean age (years) 44.2 years (SD 12.44)
Mean time after last transplant (months) 29.9 months (SD 38.38)

Prevalence of CVD Risk Factors
Hypertension
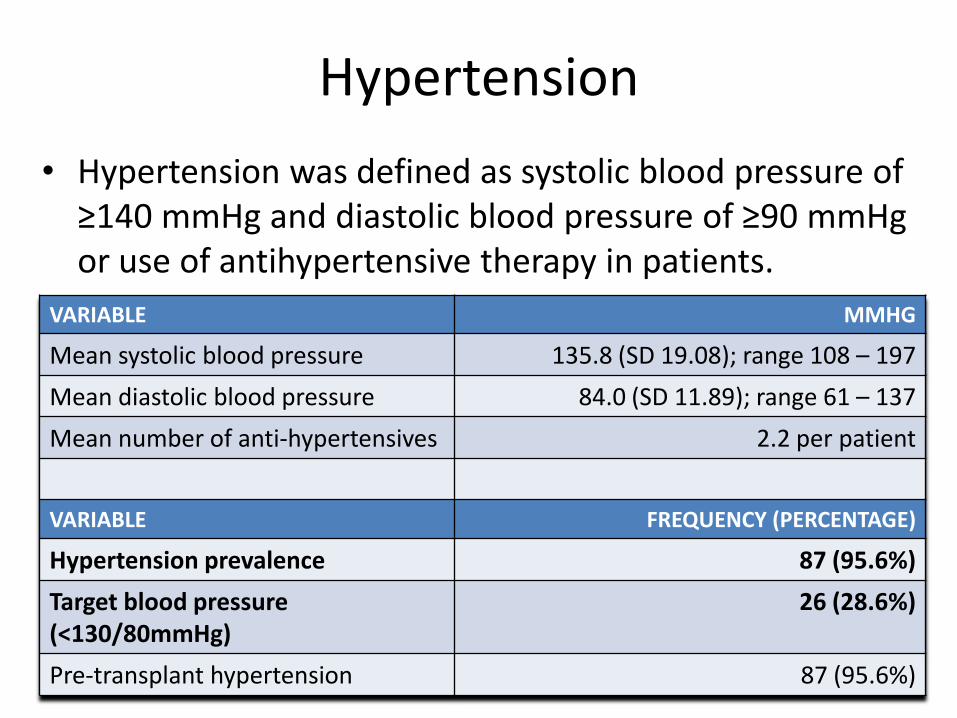
• Hypertension was defined as systolic blood pressure of ≥140 mmHg and diastolic blood pressure of ≥90 mmHg or use of antihypertensive therapy in patients.
VARIABLE MMHG
Mean systolic blood pressure 135.8 (SD 19.08); range 108 – 197
Mean diastolic blood pressure 84.0 (SD 11.89); range 61 – 137
Mean number of anti-hypertensives 2.2 per patient
VARIABLE FREQUENCY (PERCENTAGE)
Hypertension prevalence 87 (95.6%)
Target blood pressure(<130/80mmHg)
26 (28.6%)
Pre-transplant hypertension 87 (95.6%)

Dyslipidemia• Dyslipidemia was defined as the presence of at least one
abnormal specific lipid profile or the use of lipid lowering drugs10.
• The mean total cholesterol level was 5.2 mmol/L (SD 1.19), mean triglyceride level 1.71 mmol/L (SD 0.845), mean LDL-cholesterol level 2.9 mmol/L (SD 0.96) and mean HDL-cholesterol level 1.5 mmol/L (SD 0.50).
• 35.2% had no lipid abnormalities while 64.8% had 1 or more lipid profile abnormalities. Only 16 RTRs (17.6%)were on drugs to correct lipid abnormalities.
10. Executive Summary of the Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults. JAMA 2001; 285:2486–2497

Obesity• Body mass index (BMI) was classified as per the WHO guidelines11.
• Abdominal obesity was determined by:– waist circumference – abnormal if ≥94.0 cm in males or ≥80.0 cm in females
– waist-hip ratio – abnormal if ˃0.90 in men or ˃0.85 in women12
11. World Health Organization. Obesity: Preventing and Managing the Global Epidemic. WHO Press; 2000.12. Alberti KGMM, Zimmet P, Shaw J. The IDF Epidemiology Task Force Consensus Group: the metabolic syndrome—a
new worldwide definition. Lancet 2005; 366:1059
VARIABLE MEAN RANGE
BMI (kg/m²) 25.7 (SD 5.74) 16.2 – 54.7
Waist circumference (cm) 91.0 (SD 13.38) 63 – 122
Waist-hip ratio 0.92 (SD 0.075) 0.71 – 1.14
CLASSIFICATION BMI (KG/M²) FREQUENCY (PERCENTAGE)
Underweight <18.5 6 (6.6%)
Normal 18.5 – 24.9 41 (45.1%)
Overweight 25.0 – 29.9 28 (30.8%)
Class I Obesity 30.0 – 34.9 11 (12.1%)
Class II Obesity 35.0 – 39.9 4 (4.4%)
Class III Obesity ≥40.0 1 (1.1%)

Dysglycemia
VARIABLE MMOL/L
Fasting glucose 5.8 (SD 2.55); range 2.5 – 17.9
VARIABLE (N=91) FREQUENCY (PERCENTAGE)
Diabetes mellitus 30 (33.0%)
Impaired fasting glucose (IFG) 15 (16.5%)
Overall dysglycemia (Diabetes and IFG) prevalence 45 (49.5%)
Normoglycemia 46 (50.5%)
Pre-transplant Diabetes mellitus 22 (24.2%)
New Onset Diabetes After Transplantation (NODAT) 8 (8.8%)
•Dysglycemia was defined as follows: •Diabetes – fasting blood glucose ≥ 7.0 mmol/l or the use of antidiabetic therapy•Impaired fasting glucose – fasting blood glucose 5.6 – 6.9 mmol/l while not receiving antidiabetic medication13
13. American Diabetes Association: Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2010; 33:S62–S69

Associations

Immunosuppressant Drug Use
0
10
20
30
40
50
60
70
80
90
100
Prednisolone Mycophenolate Mofetil
Cyclosporine Tacrolimus Azathioprine Everolimus
97.8
89
62.6
28.6
6.62.2
Percentage

Immunosuppressant Drug Use
57.1%25.2%
4.4%3.3%
2.2%7.8%
Drug Combinations
CSA + MMF + Pred
MMF + TAC + Pred
MMF + Pred
AZA + Pred
CSA + Pred
Other combinations*
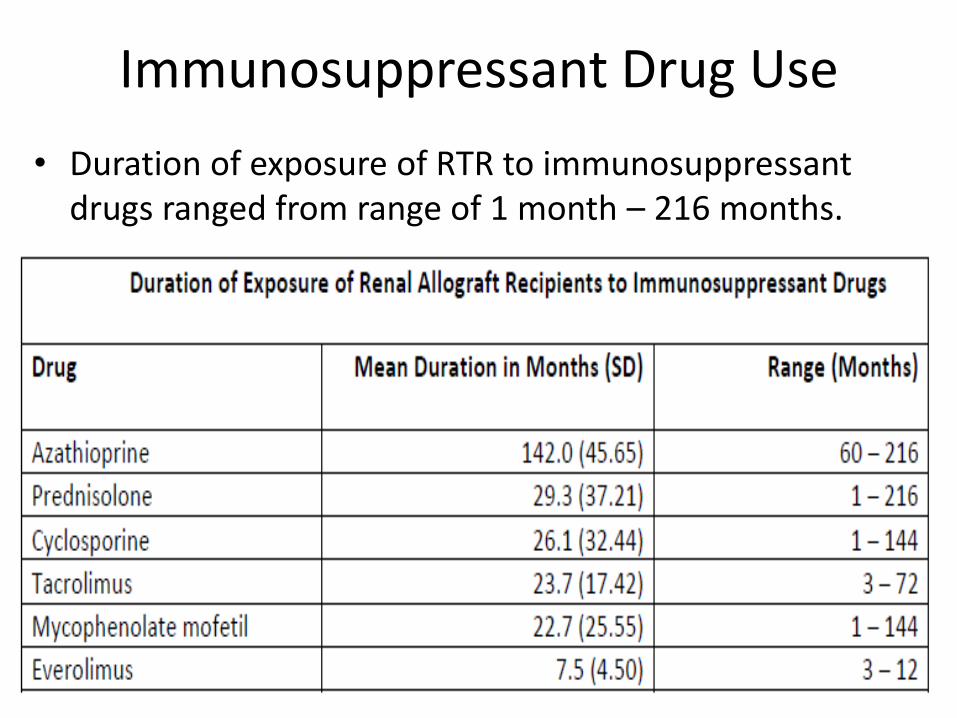
Immunosuppressant Drug Use
• Duration of exposure of RTR to immunosuppressant drugs ranged from range of 1 month – 216 months.

DiscussionVariable Study Recipients Prevalence Wagude et al
Hypertension Souza et al14 192 86.0% 95.6%
Dyslipidemia Suleiman et al15 78 62.8% 67.0%
Overweight Cofan et al16 2,691 38.0% 30.8%
Obese Cofan et al 2,691 16.0% 17.6%
Diabetes Souza et al 192 23.0% 33.0%
IFG Souza et al 192 23.0% 16.5%
Macroalbuminuria Ibis et al17 130 34.8% 11.0%
Anemia Vanrentergem et al18 4,263 38.6% 22.0%
Impaired graft fxn Souza et al 192 49.5% 16.5%
Smoking Yavuz et al19 226 12% (42%) 3.3%
14. Souza FC, Silva MB, Motta EM, et al. Prevalence of Risk Factors for Cardiovascular Disease in Brazilian Renal Transplant Recipients. Transplant Proceed 2007; 39: 446–448
15. Suleiman B, El Imam M, Elsabigh M, et al. Lipid profile in post renal transplant patients treated with cyclosporine in Sudan. Saudi J Kidney Dis Transpl 2009; 20:312–7
16. Cofán F, et al. Obesity in Renal Transplantation: Analysis of 2691 Patients. Transplant Proceed 2005; 37:3695–369717. Ibis A et al. Early onset proteinuria after renal transplantation. Transplant Proc. 2007;39:938–940 18. Vanrenterghem Y, Ponticelli C, Morales JM, et al. Prevalence and management of anemia in renal transplant recipients: A European
survey. Am J Transplant 2003; 3:835–84519. Yavuz A et al. Cigarette Smoking in Renal Transplant Recipients. Transplant Proceed 2004; 36:108–110

Discussion• The high prevalence of dyslipidemia and obesity in RTR
may be related to the role of steroids in fat redistribution and dyslipidemia as well as dietary indiscretion in patients post-transplantation.
• Bora et al found a higher NODAT prevalence of 16.7% in 78 RTR in India (time post-transplantation 12 months) which may be associated with more frequent use of Tacrolimus (80.8% compared to 28.6% in this study)20.
• Renal transplant recipients with a second graft were significantly more likely to develop NODAT which may be due to prolonged duration of exposure to immunosuppressant agents as well as use of steroids.
20. Bora GS. Risk factors for the development of new-onset diabetes mellitus in a living related renal transplant program. Transplant Proc 2010; 42:4072

Discussion
• Pre-transplant diabetes and insulin use were significantly associated with impaired graft function, though insulin may be confounded by its use in diabetic patients.
• Majority of the RTRs were on Prednisolone which increases long-term risk of developing obesity, glucose intolerance and hypertension.
• Small sample sizes, different immunosuppressant drug formulations, short durations of exposure and differing drug dosages may have contributed to the lack of significant associations.

Recommendations
• RTRs considered as a priority population at high risk for cardiovascular mortality and morbidity in health policy formulation for interventional measures in non-communicable disease.
• Local adaptation and implementation of Kidney Disease Outcomes Quality Initiative (KDOQI) renal transplant recipient guidelines on prevention, screening, treatment and control of specific cardiovascular risk factors.
• Specifically, measures to improve control of blood pressure in hypertensive RTR population need to be adapted locally and disseminated to nephrologists and renal transplant patients.

THANK YOU