Embed Size (px)
Citation preview

siology 62 (2006) 185–192www.elsevier.com/locate/ijpsycho
International Journal of Psychophy
Cardiovascular reactivity during performance under social observation:The moderating role of task difficulty
Guido H.E. Gendolla ⁎, Michael Richter
FPSE, Department of Psychology, University of Geneva, 40, Bd. du Pont d'Arve, CH-1211 Geneva 4, Switzerland
Received 2 February 2006; received in revised form 9 March 2006; accepted 11 April 2006Available online 5 June 2006
Abstract
An experiment with N=40 university students investigated the impact of social observation on cardiovascular reactivity during performance ona computer-based letter detection task. The study was conducted in a 2 (social observation: no vs. yes)×2 (task difficulty: easy vs. difficult)between-persons design. In accordance with engagement-related predictions about the role of social observation in active coping, the merepresence of an experimenter who observed participants during task performance increased the reactivity of systolic blood pressure when the taskwas difficult, but not when the task was easy. Without social observation, reactivity was modest in both the easy and the difficult conditions.Reactivity of diastolic blood pressure described the same pattern as systolic blood pressure. Results are interpreted as evidence for an effort-relatedanalysis of cardiovascular reactivity based on the principles of motivational intensity theory.© 2006 Elsevier B.V. All rights reserved.
Keywords: Cardiovascular reactivity; Social observation; Active coping; Mental effort
1. Introduction
Reactions of the autonomic nervous system during taskperformance under social observation have been of interestsince Zajonc (1965) proposed that the presence of othersincreases the level of “drive” or “general arousal” and thusmoderates task performance (see Hull, 1943). After decadeswith modest evidence of social observation effects onautonomic nervous system activity (see Geen and Bushman,1989) there is now accumulating evidence of effects on onespecific autonomic parameter: cardiovascular arousal (e.g.,Hartley et al., 1999; Pruyn et al., 1985; Schwerdtfeger, 2004;Smith et al., 1997, 2000; Wright et al., 2002, 1995). Weinvestigated social observation effects on cardiovascularreactivity from a specific theoretical perspective—an applica-tion of Wright's (1996) integration of Obrist's (1981) activecoping approach with Brehm's theory of motivational intensity(Brehm and Self, 1989) to performance conditions that involvethe performer's self (Gendolla, 2004). According to Wright's(1996) integrative analysis, the impact of the sympathetic
⁎ Corresponding author.E-mail address: [email protected] (G.H.E. Gendolla).
0167-8760/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.ijpsycho.2006.04.002
nervous system on the heart and the vasculature respondsproportionally to subjective task difficulty as long as success ispossible and worthwhile. Especially, systolic blood pressure hasbeen found to respond reliably to task demand (e.g., Bongard,1995; Gendolla and Krüsken, 2001a, 2002a,b; Gerin et al.,1995; Light, 1981; Lovallo et al., 1985; Obrist, 1981; Sherwoodet al., 1990; Smith et al., 1997, 2000). Evidence for effects ondiastolic blood pressure and heart rate (Gendolla, 1999;Gendolla and Richter, 2005; Obrist, 1981; Schwerdtfeger,2004) is existent but less consistent—presumably becausesystolic blood pressure is more systematically influenced bysympathetic discharge to the heart than diastolic blood pressureand heart rate (Brownley et al., 2000).
Wright and colleagues have demonstrated that cardiovascu-lar reactivity in the context of task performance increasesproportionally to the extent of subjective demand until a fixeddifficulty level exceeds a person's abilities (i.e. active coping istoo difficult and thus impossible) or the amount of necessaryeffort for active coping is not justified by the importance ofsuccess (see Wright, 1996; Wright and Kirby, 2001 for reviews).Furthermore, the integrative analysis suggests that the impor-tance of success directly determines cardiovascular reactivitywhen task difficulty is unfixed, i.e. when people are asked to

186 G.H.E. Gendolla, M. Richter / International Journal of Psychophysiology 62 (2006) 185–192
“do their best” or select a performance standard on their ownrather than trying to attain a fixed standard.
Wright's integrative analysis has been successfully applied tocardiovascular effects of explicit social evaluation—a variablethat is closely related to, but not identical with social obser-vation. In studies by Wright et al. (1995) social evaluation wasmanipulated by explicitly telling half the participants that at leastone other person in a control room would evaluate their per-formance on a remote computer monitor. Participants then per-formed a mental challenge that was either easy or unfixed interms of task difficulty. Results showed stronger systolic bloodpressure increases in the social-evaluation/unfixed-difficultycondition than in the other three conditions. Wright et al. (1998)conducted a study that manipulated five fixed task difficultylevels and explicit social evaluation—half the participants weretold that a camera would monitor and present their performanceto judges in a control room. In the social evaluation condition,systolic, diastolic, and heart rate reactivity increased with taskdifficulty until the task became so difficult that success wasimpossible. Without social evaluation, cardiovascular reactivitywas modest in all five difficulty conditions. These results sup-port the idea that explicit social evaluation justified the requiredeffort in the moderately difficult and difficult conditions. In stillanother study that involved a task with unfixed task difficulty,Wright et al. (2002) found that social evaluation only augmentedcardiovascular reactivity when participants believed that theywere observed by a high status observer (faculty member), butnot when they believed they were observed by a low statusobserver (student). Social evaluation had no impact in an easycondition.
In summary, these findings indicate that explicit social eval-uation–especially by a high status person–influences car-diovascular reactivity during task performance by augmentingthe value of success. Consequently, cardiovascular reactivity isrelatively strong when people work on an unfixed or difficultchallenge and believe to be evaluated by a remote high statusobserver. However, when task difficulty is fixed and easy or sohigh that success is impossible, cardiovascular reactivity is onlymodest, because only low effort is necessary (easy task) orpeople disengage (impossible task). Also a study by Kelseyet al. (2004) is compatible with the above reported findings forunfixed difficulty conditions. This study found shorter pre-ejection period (indicating increased heart contractility) andhigher heart rate during a mental arithmetic task under thecondition of social evaluation compared to no evaluation. Socialevaluation was manipulated by videotaping participants andgiving the explicit information that the recordings would beappraised. However, that study only contained an unfixed dif-ficulty condition. Thus, the results could also be interpreted asshowing that social evaluation increases cardiac reactivity ingeneral (cf. Cottrell, 1968).
In summary, the studies discussed so far are conclusive forthe effects of explicit social evaluation on cardiovascular re-activity during task performance. However, a number of issueshave remained open. One unresolved question concerns the roleof test anxiety. It is possible that the explicit social evaluationeffects in the Wright et al. and Kelsey et al. studies were carried
by highly test anxious participants. These individuals couldhave been especially responsive to the social evaluation mani-pulation and consequently, potential motivation was higher forthem than for the less test anxious participants. Furthermore, theso far discussed studies give no insight into the effects of meresocial observation by a physically present person. All studiesused an explicit evaluation manipulation, but none involved aphysically present observer. Finally, the cardiovascular reactiv-ity effects of tasks with fixed difficulty under social evaluationreported byWright et al. (1998) have not been replicated to date.Especially, a study on social observation effects during perfo-rmance on fixed easy vs. fixed difficult tasks would be of highinterest—these are the difficulty levels of concern in otherprominent theoretical analyses (Baron, 1986; Cottrell, 1968;Zajonc, 1965).
The explicit social evaluation studies leave it also open inhow far they are compatible with evidence of social presenceeffects on autonomic reactivity out of the context of task per-formance. Cacioppo et al. (1990) found that being observedresulted in increased skin conductance in response to a presentedorienting tone. Vrana and Rollock (1998) reported (among otherautonomic indices) heart rate increases caused by a minimalsocial encounter with an experimenter entering the laboratoryand taking participants' pulse. This suggests that the mere pres-ence of another person can increase autonomic reactivity, whichwould be compatible with the ideas of Zajonc (1965). If aphysically present person has the same effects in a task per-formance situation is still unclear.
2. The present experiment
We conducted a study that (1) included fixed easy and difficultconditions, (2) controlled test anxiety, and (3) manipulated socialevaluation implicitly with a physically present or absent observerwithout explicitly mentioning evaluation aspects. Participantsworked on a computer-based letter detection task. During per-formance, half the participants were observed by the experiment-er; the other participants performed under private conditions. Taskdifficulty was manipulated simultaneously with social observa-tion. Half the participants tried to attain a fixed low performancestandard in the letter detection task (easy condition); the other halftried to attain a fixed high performance standard (difficult con-dition). Cardiovascular measures were taken during habituationand task performance.
In basic accordance with the assumption that being observedduring task performance induces a state of evaluation appre-hension (Cottrell, 1968) we expected that a physically presentobserver should suffice to make success relatively important(i.e. to augment potential motivation). Consequently, we anti-cipated similar effects of social observation as those Wrightet al. (1998) have found for explicit social evaluation: socialobservation should lead to relatively strong cardiovascular re-activity during performance of a difficult task that necessitatesrelatively high mental effort. By contrast, social observationshould not increase cardiovascular reactivity when task dif-ficulty is low and does not necessitate the mobilization of highresources. It is of note that the present logic does not predict that

1 It is of note that the mere presence of a “blind” observer, i.e. a person whowas merely present but could not evaluate the performance of the participantwas not of interest in the present study.
187G.H.E. Gendolla, M. Richter / International Journal of Psychophysiology 62 (2006) 185–192
social observation itself increases cardiovascular arousal, whichis predicted by other approaches (Baron, 1986; Cottrell, 1968;Zajonc, 1965).
3. Method
3.1. Participants and design
Forty university students (35 women, 5 men, average age23 years) with various majors (psychology excluded) were ran-domly assigned in a 2 (social observation: no vs. yes)×2 (taskdifficulty: easy vs. difficult) between-persons design. All res-pondents received a small monetary reward (corresponding to 4USD) for participation. Participants' body mass index–whosecontrol is recommended in studies on cardiovascular psychophy-siology, because it can be associated with stronger cardiovascularreactivity during active coping (Shapiro et al., 1996)–did notdiffer across the experimental conditions (p'sN0.20; averageM=21.59, S.D.=2.73).
3.2. Apparatus and physiological measures
The cardiovascular measures were obtained with a computer-aided monitor (Par Electronics Physioport III) equipped withsoftware for the detection of inflation errors and movementartifacts. Systolic blood pressure (millimeters of mercury [mmHg]) and diastolic blood pressure (mm Hg) were determined byoscillometry; heart rate (beats per minute [bpm]) was determinedby tabulation of oscillations during inflation of the cuff. A bloodpressure cuff was placed over the brachial artery above the elbowof participants' nondominant arm. The cuff was inflated auto-matically and assessed values were stored on computer disk.One cardiovascular measure took approximately 35 s.
3.3. Letter detection task
Participants performed a letter detection task adopted fromthe d2 mental concentration test (Brickenkamp, 1981). A com-puter program presented for 5 min a random sequence of theletters d and p in the center of a computer screen. Placed aboveand/or below each letter were 1, 2, or no apostrophes. The taskwas to correctly identify all d's that carried 2 apostrophes bypressing a “yes-key” and to indicate all other letters by pressinga “no-key.” One letter was presented per trial. In the easy con-dition each letter occurred for 3 s. Participants were informedabout this presentation time and were instructed to respondcorrectly within this time frame—which was relatively easyaccording to pretests and previous studies that administered thistask (Gendolla and Richter, 2005; Gendolla et al., submitted forpublication). In the difficult condition, the letters were presentedfor 700 ms, which was relatively difficult according to pretests.In both difficulty conditions, the inter-trial interval was 400 ms.All participants were instructed to respond correctly to at least90% of the presented stimuli.
Participants performed 47 training trials to become familiarwith their version of the task. During the training period, thecomputer program gave immediate feedback by alerting after
incorrect responses and by informing that the reaction time wastoo long if participants did not respond within the response timewindow (3 s or 700 ms, respectively). No feedback was givenduring the performance period.
3.4. Procedure
The study was described as an investigation in physiologicalactivity during relaxation and demand. Participants attended thesession individually. The entire experimental procedure wascomputerized—all instructions and questions were displayed onthe computer screen and all responses were made with thekeyboard. After taking a seat in front of the computer screen, theexperimenter–who was hired and unaware of both the hypo-theses and the experimental difficulty condition–attached theblood pressure cuff. After assessment of biographical data (age,major, gender), weight, and height, the session proceeded with a10 min habituation period to determine physiological baselinevalues. During this time participants had the opportunity to readan old issue of a magazine to distract themselves. Cardiovas-cular measures were repeatedly taken in 2 min intervals (i.e. 5measures).
After the habituation period, the computer program displayedgeneral instructions for the letter detection task. After readingthis task information, participants pressed the space button of thecomputer keyboard and the computer displayed the instructionsfor the respective difficulty condition. In the social-observationcondition, the computer display informed participants that theexperimenter would sit next to them during the 5 min taskperformance period to observe them during performance. Nosuch information was given in the no-social-observation con-dition. Then participants performed the training trials and com-pleted a difficulty manipulation check thereafter. Participantsanswered the question “How difficult does successful task per-formance appear to you?” on a scale ranging from very easy (1)to very difficult (9). After this rating, the experimenter took a seatnext to the participant in the social-observation condition. Noinformation concerning the experimenter's status or his potentialfor evaluating the participant was given. During the observation,the experimenter was completely passive to fulfill the basiccriteria of a mere social observation rather than an explicit socialevaluation manipulation. The experimenter sat 0.7 m in a 45°angle left/behind the participant, so that he was easily visible forthe participant but did not disturb task performance. This wasdone to achieve a situation in which the experimenter observedthe participant during task performance and thus induced asituation of implicit evaluation by a physically present observer.As outlined earlier, this should suffice to increase potentialmotivation according to our reasoning.1 In the no-social-obser-vation condition, participants performed alone under privateconditions. During the 5 min of task performance, 3 cardiovas-cular measures were taken in intervals of 2 min, starting 30 safter task onset. Performance was recorded by the computer.

Table 1Cell means and standard deviations (in parentheses) of cardiovascular baselines
Measure No social observation Social observation
Easy Difficult Easy Difficult
Systolic bloodpressure
106.65 (8.99) 114.30 (9.85) 107.65 (14.67) 100.25 (10.50)
Diastolicbloodpressure
69.75 (5.07) 76.30 (7.24) 69.45 (11.44) 64.50 (8.01)
Heart rate 73.25 (3.23) 72.27 (1.53) 71.45 (3.36) 73.10 (2.03)
n=10 in each cell. Systolic blood pressure and diastolic blood pressure are inmillimeter mercury, heart rate is in beats per min.
188 G.H.E. Gendolla, M. Richter / International Journal of Psychophysiology 62 (2006) 185–192
After task performance, participants rated task difficulty a se-cond time on the same 9-point scale and completed a Germanversion (Hodapp et al., 1982) of Spielberger's (1980) TestAnxiety Inventory (TAI) to assess dispositional test anxiety. The20 items (e.g., “I feel confident and relaxed while taking tests“)were rated on scales from “does not apply to me” (1) to “doescompletely apply to me” (4). Finally, the experimenter inter-viewed participants with regard to suspicion, debriefed, and paidthem.
4. Results
4.1. Verbal measures
A 2 (social observation)×2 (task difficulty)×2 (time of mea-sure) mixed model analysis of variance (ANOVA) of the difficultyratings revealed only a highly significant difficultymain effect,F(1,36)=101.11, pb0.001, due to higher ratings in the difficult(M=6.33, S.D.=1.36) than in the easy condition (M=2.38, S.D.=1.11). No other effect approached significance (p'sN0.17). Theratings reliably differed between the difficulty conditions bothbefore (easy:M=2.50, S.D.=1.28; difficult:M=6.45, S.D.=1.47;pb0.001) and after task performance (easy M=2.25, S.D.=1.12;difficult: M=6.20, S.D.=1.61; pb0.001). We computed sumscores for the test anxiety inventory (Cronbach's α=0.88).According to a 2 (social observation)×2 (task difficulty)ANOVA, there were no differences between the experimentalcondition with regard to test anxiety scores (all p'sN0.50; overallM=43.90, S.D.=10.29).
4.2. Cardiovascular baselines
The averages of the last two determinations of systolic bloodpressure, diastolic blood pressure, and heart rate during the habit-uation period constituted the cardiovascular baseline values.2 Cellmeans and standard deviations appear in Table 1. According to 2(social observation)×2 (task difficulty) ANOVAs there weresignificant interaction effects on the systolic and diastolic bloodpressure baselines (p'sb0.04). Later we will deal with theseeffects in analyses of covariance (ANCOVAs). No baselinedifferences between the experimental conditions emerged forheart rate (all p'sN0.12).
4.3. Cardiovascular reactivity
We computed cardiovascular change (delta) scores (Llabreet al., 1991) for each participant by subtracting the baselinevalues from the averages of values obtained during task per-formance.3 Based on our clear predictions about the joint effect
2 We constituted the cardiovascular baseline values from the last twomeasures of the habituation period, because for all parameters the last twomeasures did not differ significantly from one another.3 Cronbach's alphas for the baseline measure were 0.96 (systolic blood
pressure), 0.70 (diastolic blood pressure), and 0.65 (heart rate), respectively.Alphas for the performance measure were 0.97 (systolic blood pressure), 0.93(diastolic blood pressure), and 0.70 (heart rate), respectively.
of social observation and task difficulty on effort-relatedcardiovascular response, we analyzed the reactivity scores–incontrast to the above-mentioned verbal measures that wereanalyzed exploratively without clear hypotheses–with a prioricontrasts that are the most powerful test of predicted patterns ofinteractions (Rosenthal and Rosnow, 1985; Wilkinson and TheTask Force on Statistical Inference, 1999). The a priori contrastcompared the social-observation/difficult cell (contrast weight+3) against the three remaining cells (contrast weights −1).Preliminary ANCOVAs tested for associations between thecardiovascular baseline values and reactivity scores. Theseanalyses found no significant associations between baselinesand reactivity scores for any of the cardiovascular indices (allp'sN0.50). Consequently, we used non-adjusted reactivityscores for these measures. Additional ANCOVAs tested forassociations between the cardiovascular reactivity scores andparticipants' body mass index. However, none of those asso-ciations was significant (all p'sN0.46).
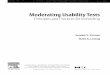
4.3.1. Systolic blood pressure reactivityThe a priori contrast was highly significant, F(1, 48)=8.60,
pb0.006, MSE=45.91, while the test of the residual was not(Fb1). Thus, the contrast captured all significant variance. Asdepicted in Fig. 1 (top panel), the pattern of cell means occurred aspredicted. Focused cell contrasts confirmed that systolic reactivityin the social-observation/difficult cell (M=12.42, S.D.=7.56)wassignificantly stronger than in any of the remaining three cells (allt's [36]N1.74, p'sb0.05).4 Simultaneously, the no-social-obser-vation/difficult cell (M=7.13, S.D.=2.76), the social-observation/easy condition (M=5.28, S.D.=7.25), and the no-social-obser-vation/easy cell (M=3.07, S.E.=8.14) did not differ from oneanother (all p'sN0.18).
4.3.2. Diastolic blood pressure reactivityThe a priori contrast was also highly significant for this mea-
sure, F(1, 36)=15.44 pb0.001, MSE=35.67; the test of theresidual was not, F(2, 36)=2.05, pN0.14, reflecting that the apriori contrast captured all significant variance. Fig. 1 (middlepanel) shows that the pattern of diastolic reactivity correspondedto that of systolic blood pressure. Cell contrasts found that diastolic
4 Given our clear a priori predictions, we applied one-tailed tests for all cellcomparisons with focused follow-up contrasts.

Systolic Blood Presure Reactivity
easy difficult
res
pons
e (m
mH
g)
0123456789
101112131415
observation no-observation
Diastolic Blood Pressure Reactivity
easy difficult
res
pons
e (m
mH
g)
0123456789
101112131415
observation no-observation
Heart Rate Reactivity
easy difficult
res
pons
e (b
pm)
0
1
2
3
4
5
6
7observation no-observation
Fig. 1. Cell means and standard errors of systolic blood pressure reactivity,diastolic blood pressure reactivity, and heart rate reactivity in the experimentalconditions. mm Hg=millimeter mercury, bpm=beats per minute.
5 Cell means were as follows. Performed stimuli: no-social-observation/easy(M=88.50, S.D.=0.53), no-social-observation/difficult (M=269.80, S.D.=0.42),social-observation/easy (M=88.50, S.D.=0.53), social-observation/difficult(M=269.30, S.D.=1.57). Correctly identified stimuli: no-social-observation/easy(M=88.00, S.E.=1.25), no-social-observation/difficult (M=227.20, S.D.=22.74),social-observation/easy (M=87.50, S.D.=1.08), social-observation/difficult(M=224.40, S.D.=24.50). Percentage of errors: no-social-observation/easy(M=0.57, S.D.=1.21), no-social-observation/difficult (M=15.79, S.D.=8.40),social-observation/easy (M=1.13, S.D.=1.40), social-observation/difficult(M=16.69, S.D.=8.93).
189G.H.E. Gendolla, M. Richter / International Journal of Psychophysiology 62 (2006) 185–192
reactivity in the social-observation/difficult cell (M=12.93, S.D.=7.44)was significantly stronger than in each of the remaining threecells (all t's [36]N2.57, p'sb0.01). Simultaneously, the no-social-observation/difficult cell (M=6.08, S.D.=4.26), the social-ob-servation/easy condition (M=5.77, S.D.=5.67), and the no-social-observation/easy cell (M=1.25, S.D.=6.07) did not differsignificantly from one another (all p'sN0.08).
4.3.3. Heart rate reactivityNeither the a priori contrast of the baseline-adjusted reac-
tivity scores (Fb1) nor the test of the residual was significant, F(2, 36)=2.46, pb0.10. Cell means, which are depicted in Fig. 1
(bottom panel), were as follows: no-social-observation/difficult,M=5.32, S.D.=5.63; no-social-observation/easy, M=1.28,S.D.=3.42; social-observation/difficult, M=4.17, S.D.=5.73;and social-observation/easy, M=1.77, S.D.=3.23.
4.4. Task performance
To test if performance effects resembled those of cardiovas-cular reactivity, we applied the same a priori contrast to the totalnumber of attended stimuli, the number of correctly identifiedtargets, and the percentage of errors with reference to the totalnumber of attended stimuli—for the percentage of errors, thecontrast weights were inverted because good performance shouldbe reflected by few errors (see Gendolla and Richter, 2005). Apreliminary analysis revealed that two participants in the social-observation/difficult cell committedmuchmore errors in the letterdetection task than the rest of the sample (exceeding both thegrand mean and the respective cell means for more than 2 S.D.s).We replaced their performance values by the respective conditionmeans (excluding these participants completely did not changethe significance of the effects reported below).
The a priori contrasts were highly significant for all achieve-ment indices, F's(1, 36)N23.04, p'sb0.001. However, for eachindex the residuals were highly significant, too,F's(2, 36)N19.42,p'sb0.001. This indicates that a significant amount of variancewas not explained by the contrast and that the contrast did thus notappropriately reflect the pattern of effects.We tested thereforewithconventional ANOVAs which other effects were reliable. Theseanalyses only found difficulty main effects on all performanceindices, all F's(1, 36)N61.73, p'sb0.001, in the absence of anyother significant effect (all p'sN0.38). Condition means were asfollows: performed stimuli (easy:M=88.50, S.D.=0.51, difficult:M=269.55, S.D.=1.16), correctly identified stimuli (easy:M=87.75, S.D.=1.16, difficult: M=225.80, S.D.=23.05), per-centage of errors (easy:M=0.85, S.D.=1.26, difficult:M=16.24,S.D.=8.45).5
However, reactivity of systolic blood pressure (r's=0.31 to0.38, p'sb0.05) and diastolic blood pressure (r's=0.38 to 0.43,p'sb0.02) were positively correlated with all of these perfor-mance indices. Heart rate reactivity correlated positively withthe total number of attended letters (r=0.34, pb0.04) and thepercentage of committed errors (r=0.51, pb0.001). In summarythis indicates associations between cardiovascular reactivity andperformance in that stronger reactivity was combined with fasterbut also more error prone performance.

190 G.H.E. Gendolla, M. Richter / International Journal of Psychophysiology 62 (2006) 185–192
4.5. Complementary analysis
Because of the above reported large difference between theeasy and difficult conditions regarding the total number ofattended letters, we tested for significant associations between thisvariable and cardiovascular reactivity. If such associations exis-ted, the reported cardiovascular reactivity could be explained bymere motor activity rather than the mobilization of mental effort.Therefore we considered the total number of attended letters ascovariate in the a priori contrasts on systolic blood pressure,diastolic blood pressure, and heart rate. However, the total numberof attended letters was not associatedwith any reactivity index (allp'sN0.50). Consequently, the cardiovascular reactivity effects arehardly attributable to mere physical activity.
We applied the same type of analysis to evaluate the questionif participants' test anxiety could be responsible for the observedcardiovascular reactivity effects. However, the covariate effectsof the TAI scores were not significant for any of three assessedcardiovascular reactivity indices (p'sN0.26). Consequently, theassessed test anxiety could not explain the observed cardiovas-cular reactivity effects. There were also no significant associa-tions between the TAI scores and the cardiovascular baselinevalues (p'sN0.12). Furthermore, the TAI scores were not corre-lated with any of the three performance indices reported above(r's=−0.02 to 0.00, p'sN0.50).
5. Discussion
The present results support our predictions about the impact ofsocial observation on cardiovascular reactivity during task perfor-mance. Drawing on a recent theoretical application of Wright's(1996) integrative analysis to performance conditions that involvethe performer's self (Gendolla, 2004), we had expected that socialobservation during task performance makes success relativelyimportant, because a physically present observer of one's perfor-mance is sufficient to induce a state of social evaluation. However,unlike other approaches that have posited that social observationshould lead to a general increase in autonomic nervous systemactivity (e.g., Baron, 1986; Cottrell, 1968; Zajonc, 1965), wepredicted an interaction effect between social observation and taskdifficulty on one specific type of autonomic arousal—cardiovas-cular response. In support of this reasoning social observationresulted in relatively strong cardiovascular reactivity during taskperformance only when the task was difficult and thus necessitatedhigh resources, but not when it was easy, and only necessitatedrelatively low resources. This was evident for two cardiovascularindices—systolic and diastolic blood pressure.
It is of note that the cardiovascular reactivity effects wereindependent of physical activity and metabolic demand due to thekey press rate during task performance, as evident in the lack ofeffects of the number of performed letters (i.e. the number of keypresses) on cardiovascular reactivity. These findings indicate thatcardiovascular reactivity indeed reflected the mobilization ofmental effort in the performed cognitive task (Gaillard andKramer, 2001; Hockey, 1997). It is of additional note that thepresent cardiovascular reactivity effects are hardly explicable asreflecting test anxiety or by the effect that highly test anxious
individuals carried the observed effects: assessed anxiety was notrelated to cardiovascular reactivity. Both of these findings arecompatible with the results of other recent experiments that in-vestigated the roles of ego-involvement (Gendolla and Richter,2005, in press) and self-awareness (Gendolla et al., submittedfor publication)—other variables that involve a performer's self(Gendolla, 2004).
Referring to the effects on the single cardiovascular indiceswe had assessed in this study, results for systolic reactivity fullysupport our predictions. The corresponding effects on diastolicblood pressure were less anticipated. Nevertheless, there is ampleevidence for simultaneous systolic and diastolic adjustmentsduring active coping (e.g., Al'Absi et al., 1997; Gendolla, 1999;Gendolla and Richter, 2005; Gerin et al., 1995; Lovallo et al.,1985; Smith et al., 1990; Wright and Dill, 1993). One reason forthe observed diastolic reactivity could be that myocardial con-tractility is sometimes so strong that it also results in significantincreases in blood pressure between pulse waves, which results incorresponding increases in both systolic and diastolic bloodpressure (e.g., Gendolla andKrüsken, 2001b; Lovallo et al., 1985;Sherwood et al., 1990). Another possibility is that active coping issometimes associated with greater vasoconstriction than vasodi-latation, for instance when active coping elicits only modestsympathetic discharge (Storey et al., 1996). But given that thepresent study did not involve direct measures of contractility andperipheral resistance, these interpretations are tentative and callfor further research. Nevertheless, it should be noted that thesignificant effects on diastolic blood pressure reactivity do notcontradict our predictions. Rather, they complete the predictedeffects on systolic reactivity.
Heart rate was less influenced by the social observation mani-pulation than blood pressure. However, it is of note that heart rateis determined by both sympathetic and parasympathetic arousaland should thus only respond to effort mobilization when thesympathetic impact is stronger—which is not always the case(Berntson et al., 1993; Obrist, 1981). Consequently, heart rate is aless reliable indicator of resourcemobilization than systolic bloodpressure, which is more directly and more systematically relatedto sympathetic discharge to the heart (Brownley et al., 2000;Papillo and Shapiro, 1990). However, given that we have notapplied continuous ECGmeasures to assess heart rate, we have toacknowledge that the lack of effect of the social observationmanipulation on this cardiovascular index could also be explainedby a relatively high measurement error.
On the conceptual level, the present study clarifies someopen issues from studies byWright and colleagues regarding theeffects of explicit social evaluation on cardiovascular reactivity(Wright et al., 1995, 1998, 2002). Those studies left it open ifthe effects of mere social observation by a physically presentperson would be the same as those of explicit social evaluationby another high status person, and if individual differences intest anxiety played a significant role in the determination ofcardiovascular reactivity when performance is socially evalu-ated. According to our findings, explicit social evaluation is notnecessary to boost potential motivation and test anxiety plays nosignificant role in the determination of cardiovascular reactivityunder social evaluation—as the zero-effect of this variable as a

191G.H.E. Gendolla, M. Richter / International Journal of Psychophysiology 62 (2006) 185–192
covariate indicated. Moreover, observers who are physicallypresent during task performance seem to have different effectsthan people who are merely present without a performancecontext (see Cacioppo et al., 1990; Vrana and Rollock, 1998).
Also the observed performance effects deserve some attention.Although previous studies found corresponding effects on car-diovascular reactivity and task performance (e.g., Gendolla andKrüsken, 2002b, Study 2;Gendolla andRichter, 2005) the presentstudy found only difficulty main effects on all performance indi-ces. That is, the manipulation of social observation has affectedcardiovascular reactivity and task performance differently. On theother hand the significant correlations between the cardiovascularreactivity and the number of performed letters and committederrors suggests that the mobilization of mental effort wasassociated with faster but also more erroneous performance.Although the significant correlations between cardiovascular re-activity and the performance measures may support our as-sumption that cardiovascular reactivity reflected the mobilizationof mental effort at least on the within-persons level, it is of notethat effort and performance are not interchangeable constructs. Aspointed out earlier (e.g., Gendolla and Richter, 2005; Richter andGendolla, in press), effort refers to themobilization of resources inorder to carry out instrumental behavior. Achievement (only)describes the outcome of instrumental behavior and is the productof effort, ability, and strategy (Locke and Latham, 1990). In-terestingly, an abundance of studies have identified performanceeffects of social observation in social psychology research (seeBond and Titus, 1983; Guerin, 1986 for reviews) have failed tofind effects on autonomic reactivity—although this variable hasbeen proposed as the mediator between social observation andperformance (Geen and Bushman, 1989). The relationship bet-ween effort, activation, and achievement is obviously complexand remains an important research topic for future research.
Acknowledgement
This research was supported by a Deutsche Forschungsge-meinschaft research grant (Ge 987/3-1) awarded to the firstauthor. We would like to thank Alexander Bertrams and FlorianSchwanengel for their help as hired experimenters.
References
Al'Absi, M., Bongard, S., Buchanan, T., Pincomb, G.A., Licino, J., Lovallo,W.R., 1997. Cardiovascular and neuroendocrine adjustment to publicspeaking and mental arithmetic stressors. Psychophysiology 34, 266–275.
Baron, R.S., 1986. Distraction-conflict theory: progress and problems. In:Berkowitz, L. (Ed.), Advances in Experimental Social Psychology, vol. 19.Academic Press, New York, pp. 1–40.
Berntson, G.G., Cacioppo, J.T., Quigley, K.S., 1993. Cardiac psychophysiologyand autonomic space in humans: empirical perspectives and conceptualimplications. Psychol. Bull. 114, 296–322.
Bond, C.F., Titus, L.J., 1983. Social facilitation: a meta-analysis of 241 studies.Psychol. Bull. 94, 265–292.
Bongard, S., 1995. Mental effort during active and passive coping: a dual taskanalysis. Psychophysiology 32, 242–248.
Brehm, J.W., Self, E.A., 1989. The intensity of motivation. Annu. Rev. Psychol.40, 109–131.
Brickenkamp, R., 1981. Test d2, 7th ed. Hogrefe, Göttingen, Germany.
Brownley, K.A., Hurwitz, B.E., Schneiderman, N., 2000. Cardiovascular psy-chophysiology. In: Cacioppo, J.T., Tassinary, L.G., Berntson, G.G. (Eds.),Handbook of psychophysiology. Cambridge University Press, New York,pp. 224–264.
Cacioppo, J.T., Rourke, P.A., Marshall-Goodell, B.S., Tassinary, L.G., Baron,R.S., 1990. Rudimentary physiological effects to mere observation.Psychophysiology 27, 177–186.
Cottrell, N.B., 1968. Performance in the presence of other human beings: merepresence, audience, and affiliation effects. In: Simmel, E.C., Hoppe, R.A.,Milton, G.A. (Eds.), Social facilitation and imitative behavior. Allyn andBacon, Boston, pp. 91–110.
Gaillard, A.W.K., Kramer, A.F., 2001. Theoretical and methodological issues inpsychophysiological research. In: Backs, R.W., Boucsein, W. (Eds.), Engi-neering psychophysiology. Erlbaum, Mahwah, NJ, pp. 31–58.
Geen, R.G., Bushman, B.J., 1989. The arousing effects of social presence. In:Wagner, H., Manstead, A. (Eds.), Handbook of social psychophysiology.Wiley, London, UK, pp. 262–281.
Gendolla, G.H.E., 1999. Self-relevance of performance, task difficulty, and taskengagement assessed as cardiovascular response. Motiv. Emot. 23, 45–66.
Gendolla, G.H.E., 2004. The intensity of motivation when the self is involved:an application of Brehm's theory of motivation to effort-relatedcardiovascular response. In: Wright, R.A., Greenberg, J., Brehm, S.S.(Eds.), Motivational analyses of social behavior. Erlbaum, Mahwah, NJ,pp. 205–244.
Gendolla, G.H.E., Krüsken, J., 2001a. The joint impact of mood state and taskdifficulty on cardiovascular and electrodermal reactivity in active coping.Psychophysiology 38, 539–548.
Gendolla, G.H.E., Krüsken, J., 2001b. Mood state and cardiovascular responsein active coping with an affect-regulative challenge. Int. J. Psychophysiol.41, 169–180.
Gendolla, G.H.E, Krüsken, J., 2002a. The joint effect of informational moodimpact and performance-contingent incentive on effort-related cardiovas-cular response. J. Pers. Soc. Psychol. 83, 271–285.
Gendolla, G.H.E., Krüsken, J., 2002b. Informational mood impact on effort-related cardiovascular response: The diagnostic value of moods counts.Emotion 2, 251–262.
Gendolla, G.H.E., Richter, M., 2005. Ego-involvement and effort: cardiovas-cular, electrodermal, and achievement effects. Psychophysiology 42,595–603.
Gendolla, G.H.E., Richter, M., in press. Ego-involvement and the difficulty lawof motivation: effects on performance-related cardiovascular response. Pers.Soc. Psychol. Bull.
Gendolla, G.H.E., Richter, M., Silvia, P.J., submitted for publication. Self-awareness and the intensity of motivation during self-regulation: studies ofcardiovascular reactivity. Manuscript under review.
Gerin, W., Litt, M.D., Deich, J., Pickering, T.G., 1995. Self-efficacy as amoderator of perceived control effects on cardiovascular reactivity: Isenhanced control always beneficial? Psychosom. Med. 57, 390–397.
Guerin, B., 1986. Mere presence effects in humans: a review. J. Exp. Soc.Psychol. 22, 38–77.
Hartley, T.R., Ginsburg, G.P., Heffner, K., 1999. Self-presentation and cardio-vascular reactivity. Int. J. Psychophysiol. 32, 75–88.
Hockey, G.R.J., 1997. Compensatory control in the regulation of human per-formance under stress and high workload: a cognitive-energetical frame-work. Biol. Psychol. 45, 73–93.
Hodapp, V., Laux, L., Spielberger, C.D., 1982. Theorie und Messung deremotionalen und kognitiven Komponente der Prüfungsängstlichkeit[Theory and measurement of emotional and cognitive components of testanxiety]. Z. Differ. Diagn. Psychol. 3, 169–184.
Hull, C.L., 1943. Principles of Behavior. Appleton-Century-Crofts, New York.Kelsey, R.M., Soderlund, K., Arthur, C., 2004. Cardiovascular reactivity and
adaptation to recurrent psychological stress: replication and extension.Psychophysiology 41, 924–934.
Light, K.C., 1981. Cardiovascular responses to effortful active coping: impli-cations for the role of stress in hypertension development. Psychophysiology18, 216–225.
Llabre, M.M., Spitzer, S.B., Saab, P.G., Ironson, G.H., Schneiderman, N., 1991.The reliability and specificity of delta versus residualized change as measure

192 G.H.E. Gendolla, M. Richter / International Journal of Psychophysiology 62 (2006) 185–192
of cardiovascular reactivity to behavioral challenges. Psychophysiology 28,701–711.
Locke, E.A., Latham, G.P., 1990. A Theory of Goal setting and Performance.Prentice Hall, Englewood Cliffs, NJ.
Lovallo, W.R., Wilson, M.F., Pincomb, G.A., Edwards, G.L., Tompkins, P.,Brackett, D.J., 1985. Activation patterns to aversive stimulation in man:passive exposure versus effort to control. Psychophysiology 22, 283–291.
Obrist, P.A., 1981. Cardiovascular Psychophysiology: A Perspective. PlenumPress, New York.
Papillo, J.F., Shapiro, D., 1990. The cardiovascular system. In: Cacioppo, J.T.,Tassinary, L.G. (Eds.), Principles of Psychophysiology. Cambridge Uni-versity Press, New York, pp. 465–512.
Pruyn, A.T.H., Aasman, J., Wijers, D., 1985. Social influences on mentalprocesses and cardiovascular reactivity. In: Orlebeke, J.F., Mulder, G., vanDoornen, L.P.J. (Eds.), Psychophysiology of Cardiovascular Control:Methods, Models, and Data. Plenum, New York, pp. 865–877.
Richter, M., Gendolla, G.H.E., in press. Incentive effects on cardiovascularreactivity in active coping with unclear task difficulty. Int. J. Psychophysiol.
Rosenthal, R., Rosnow, R.L., 1985. Contrast Analysis. Cambridge UniversityPress, New York.
Schwerdtfeger, A., 2004. Predicting autonomic reactivity to public speaking:don't get fixed on self-report data! Int. J. Psychophysiol. 52, 217–224.
Shapiro, D., Jamner, L.D., Lane, J.D., Light, K.C., Myrtek, M., Sawada, Y.,Steptoe, A., 1996. Blood pressure publication guidelines. Psychophysiology33, 1–12.
Sherwood, A., Dolan, C.A., Light, K.C., 1990. Hemodynamics of blood pres-sure responses during active and passive coping. Psychophysiology 27,656–668.
Smith, T.W., Baldwin, M., Christensen, A.J., 1990. Interpersonal influence asactive coping: effects of task difficulty on cardiovascular reactivity. Psycho-physiology 27, 429–437.
Smith, T.W., Nealey, J.B., Kircher, J.C., Limon, J.P., 1997. Social determinantsof cardiovascular reactivity: effects of incentive to exert influence andevaluative threat. Psychophysiology 34, 65–73.
Smith, T.W., Ruiz, J.M., Uchino, B.N., 2000. Vigilance, active coping, andcardiovascular reactivity during social interaction in young men. HealthPsychol. 19, 382–392.
Spielberger, C.D., 1980. Test anxiety inventory (“Test attitude inventory”).Preliminary professional manual. Consulting Psychology Press, Palo Alto,CA.
Storey, P.L., Wright, R.A., Williams, B.J., 1996. Need as a moderator of thedifficulty-cardiovascular response relation: the case of fluid deprivation.J. Psychophysiol. 10, 228–238.
Vrana, S., Rollock, D., 1998. Physiological response to a minimal socialencounter: effects of gender, ethnicity, and social context. Psychophysiology35, 462–469.
Wilkinson, L., The Task Force on Statistical Inference, 1999. Statistical methodsin psychology journals. Am. Psychol. 54, 594–604.
Wright, R.A., 1996. Brehm's theory of motivation as a model of effort and cardio-vascular response. In: Gollwitzer, P.M., Bargh, J.A. (Eds.), The Psychology ofAction: Linking Cognition andMotivation to Behavior, pp. 424–453. Guilford,New York.
Wright, R.A., Dill, J.C., 1993. Blood pressure responses and incentive appraisalsas a function of perceived ability and objective task demand. Psychophys-iology 30, 152–160.
Wright, R.A., Kirby, L.D., 2001. Effort determination of cardiovascular res-ponse: an integrative analysis with applications in social psychology. In:Zanna, M.P. (Ed.), Advances in Experimental Social Psychology, vol. 33.Academic Press, New York, pp. 255–307.
Wright, R.A., Tunstall, A.M., Williams, B.J., Goodwin, J.S., Harmon-Jones, E.,1995. Social evaluation and cardiovascular response: an active copingapproach. J. Pers. Soc. Psychol. 69, 530–543.
Wright, R.A., Dill, J.C., Geen, R.G., Anderson, C.A., 1998. Social evaluationinfluence on cardiovascular response to a fixed behavioral challenge: effectsacross a range of difficulty levels. Ann. Behav. Med. 20, 277–285.
Wright, R.A., Killebrew, K., Pimpalapure, D., 2002. Cardiovascular incentiveeffectswhere a challenge is unfixed: demonstrations involving social evaluation,evaluator status, and monetary reward. Psychophysiology 39, 188–197.
Zajonc, R.B., 1965. Social facilitation. Science 149, 269–274.