Embed Size (px)
Citation preview
Cardiovascular Outcomes Trials in Diabetes
M. Angelyn Bethel, MDDeputy Director
University of Oxford Diabetes Trials UnitOxford, UK
How did we get here & where are we going?
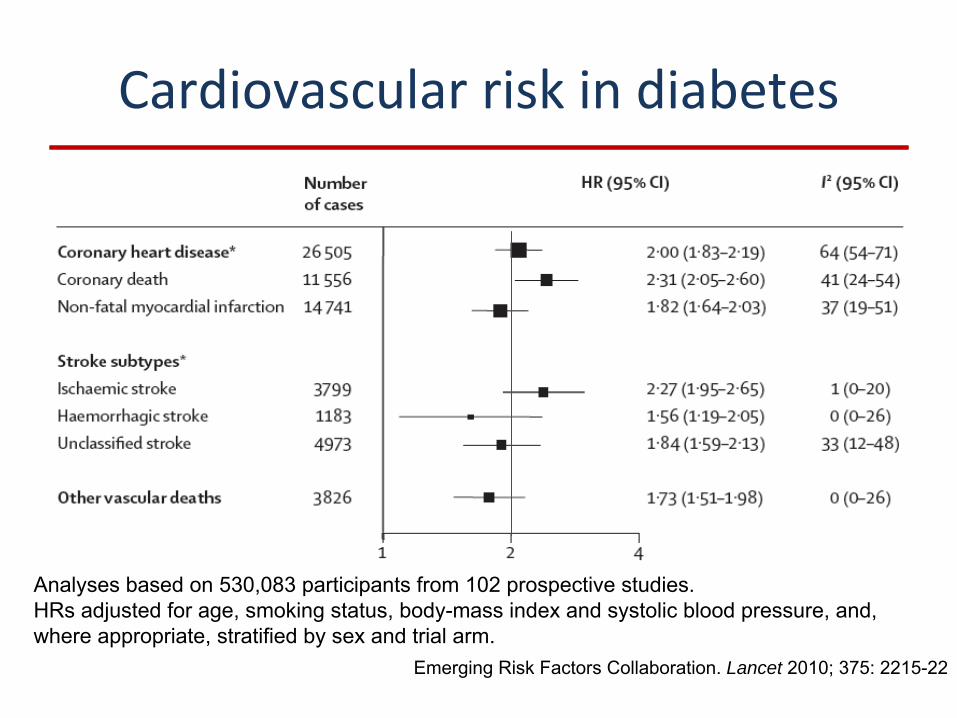
Cardiovascular risk in diabetes
Emerging Risk Factors Collaboration. Lancet 2010; 375: 2215-22
Analyses based on 530,083 participants from 102 prospective studies.HRs adjusted for age, smoking status, body-mass index and systolic blood pressure, and, where appropriate, stratified by sex and trial arm.
Reducing risk for complications
•
Microvascular–
Glucose
–
Blood pressure (esp retinopathy, nephropathy)–
Lipids
–
Smoking cessation•
Macrovascular–
Blood pressure
–
Lipids–
Antiplatelet agents
–
Smoking cessation –
Glucose?
THE ROLE OF GLUCOSE CONTROL IN
MACROVASCULAR DISEASE
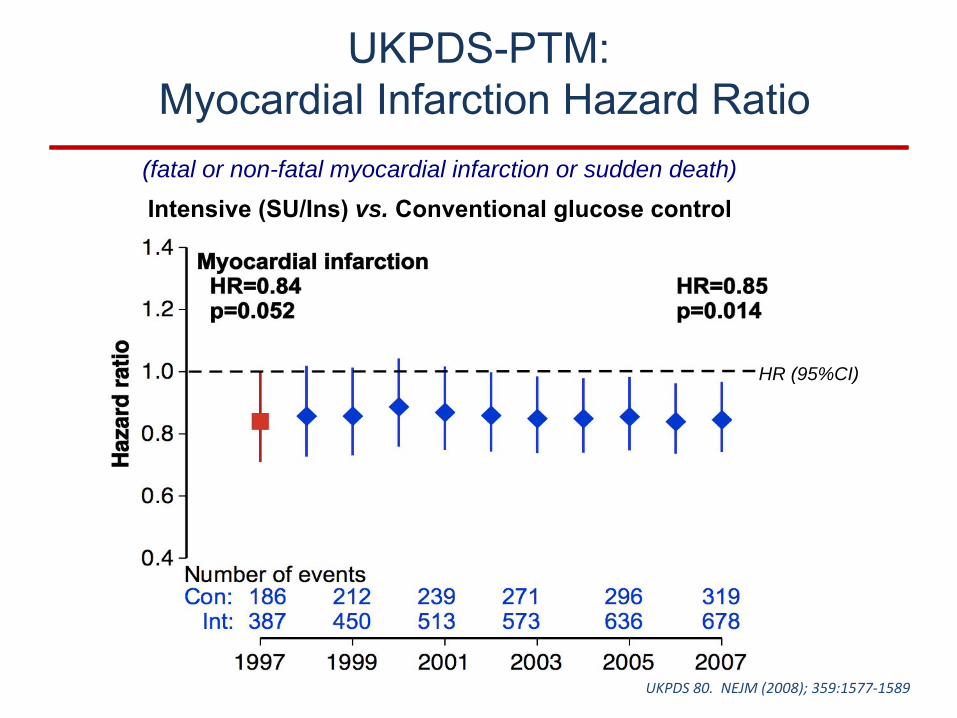
UKPDS-PTM: Myocardial Infarction Hazard Ratio
(fatal or non-fatal myocardial infarction or sudden death)
Intensive (SU/Ins) vs. Conventional glucose control
HR (95%CI)
UKPDS 80. NEJM (2008); 359:1577‐1589
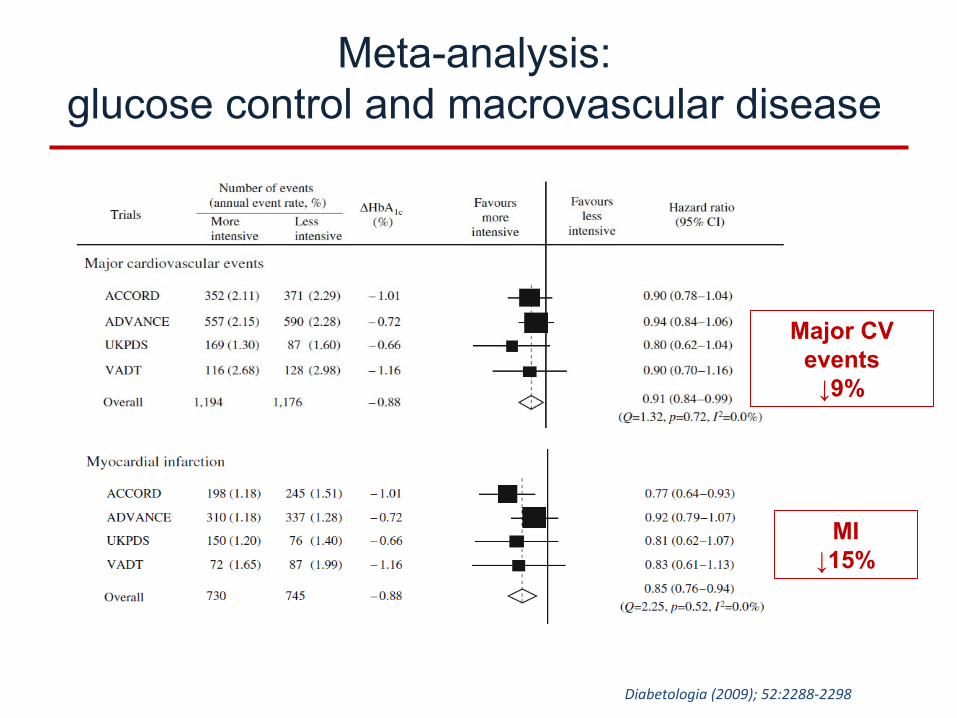
Diabetologia (2009); 52:2288‐2298
Meta-analysis: glucose control and macrovascular disease
Major CV events↓9%
MI↓15%
WHAT IS THE THRESHOLD FOR HARM?
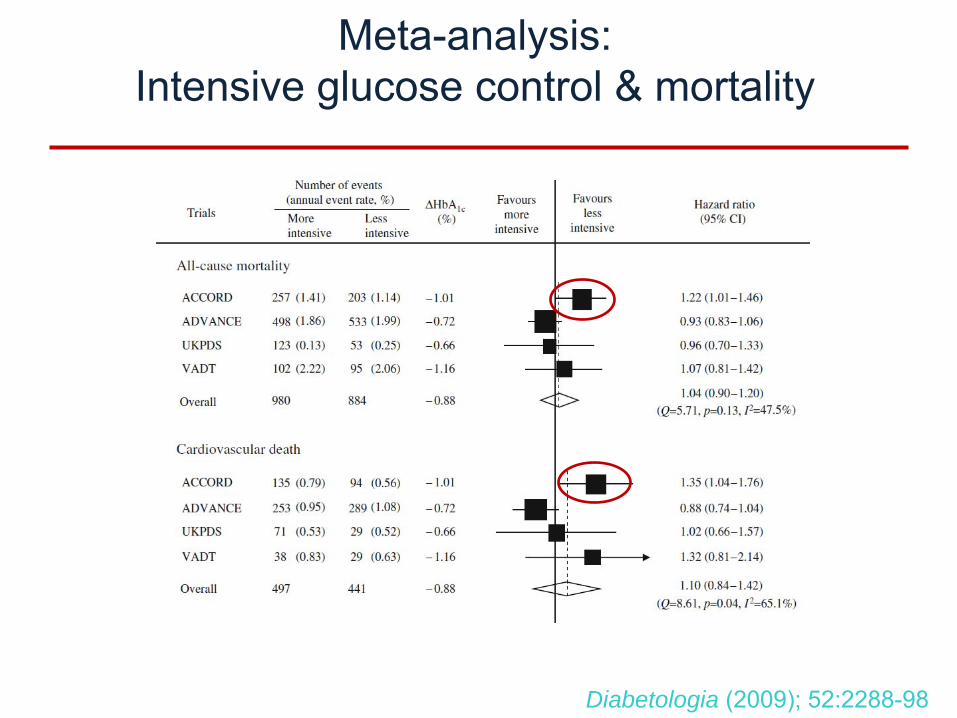
Meta-analysis: Intensive glucose control & mortality
Diabetologia (2009); 52:2288-98
•
Hypoglycemia–
? Adrenergic overdrive
–
? Causal pathway for mortality or macrovascular events
•
Off-target effects of therapeutic choices–
Cardiovascular morbidity?
–
Fractures?–
Cancer?
–
Pancreatitis?
Defining the risks of overtreatment
(unproven)
(unproven)
Real uncertainty about off-target effects
Can a dirt-cheap diabetes drug fight cancer?
Judge sets first hearing for diabetes drug lawsuits
More Evidence Links Fractures to Diabetes
DrugsAvandia, Actos Boost Fracture Risk in Older
Women, Study Finds
Diabetes drug tied to pancreatitis, deaths
Study: Sanofi’s Lantus Insulin Has Possible
Cancer Link
•
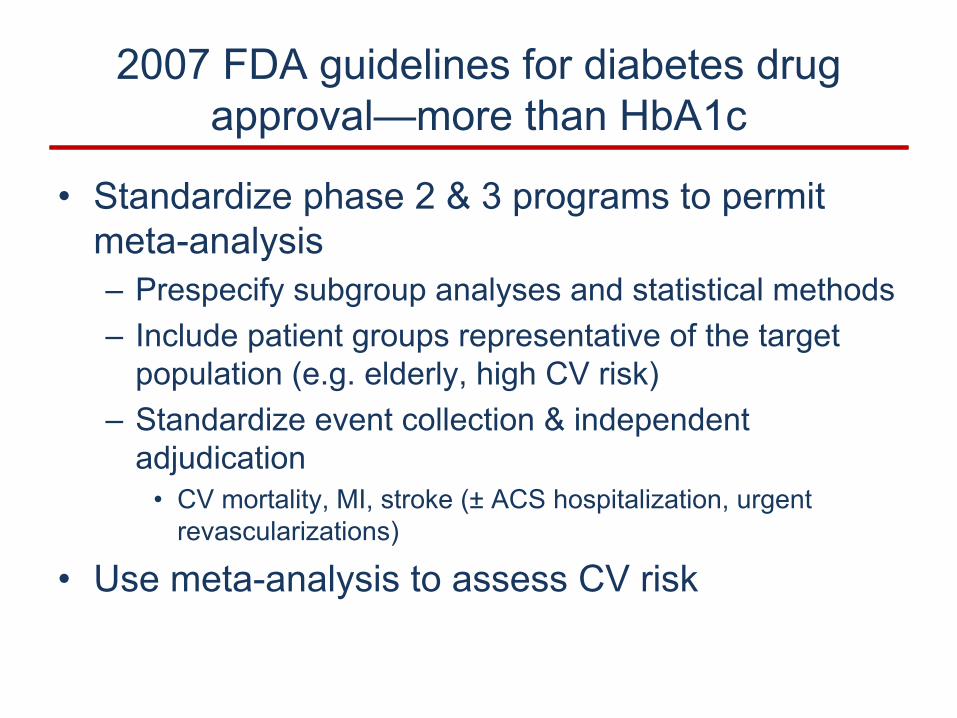
Standardize phase 2 & 3 programs to permit meta-analysis–
Prespecify subgroup analyses and statistical methods
–
Include patient groups representative of the target population (e.g. elderly, high CV risk)
–
Standardize event collection & independent adjudication
•
CV mortality, MI, stroke (±
ACS hospitalization, urgent revascularizations)
•
Use meta-analysis to assess CV risk
2007 FDA guidelines for diabetes drug approval—more than HbA1c
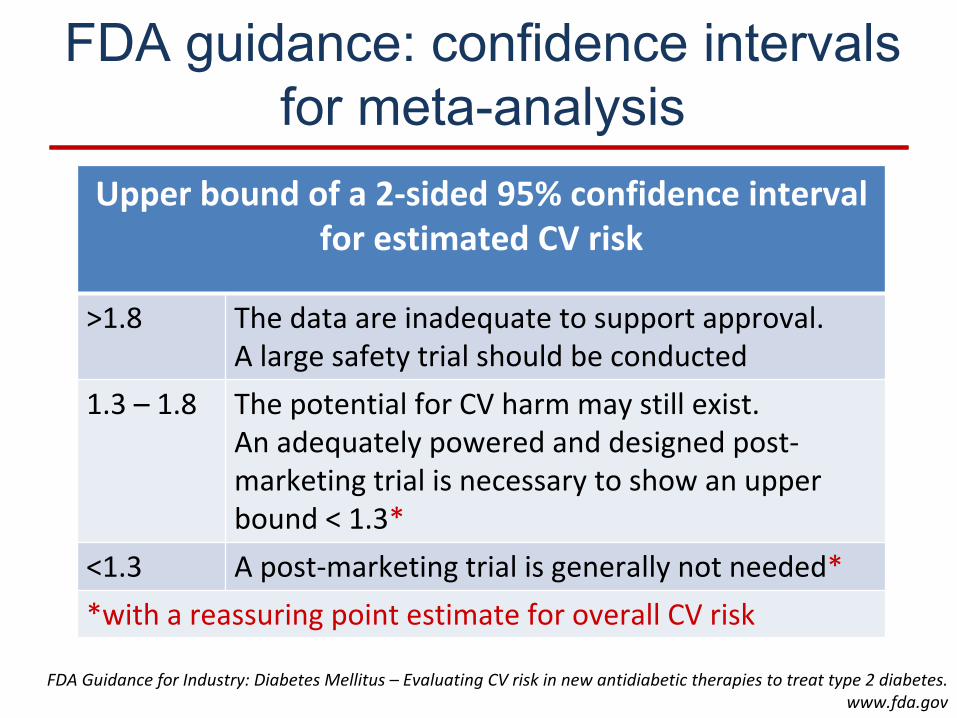
FDA guidance: confidence intervals for meta-analysis
Upper bound of a 2‐sided 95% confidence interval for estimated CV risk
>1.8 The data are inadequate to support approval. A large safety trial should be conducted
1.3 – 1.8 The potential for CV harm may still exist. An adequately powered and designed post‐
marketing trial is necessary to show an upper bound < 1.3*
<1.3 A post‐marketing trial is generally not needed**with a reassuring point estimate for overall CV risk
FDA Guidance for Industry: Diabetes Mellitus –
Evaluating CV risk in new antidiabetic therapies to treat type 2 diabetes.
www.fda.gov
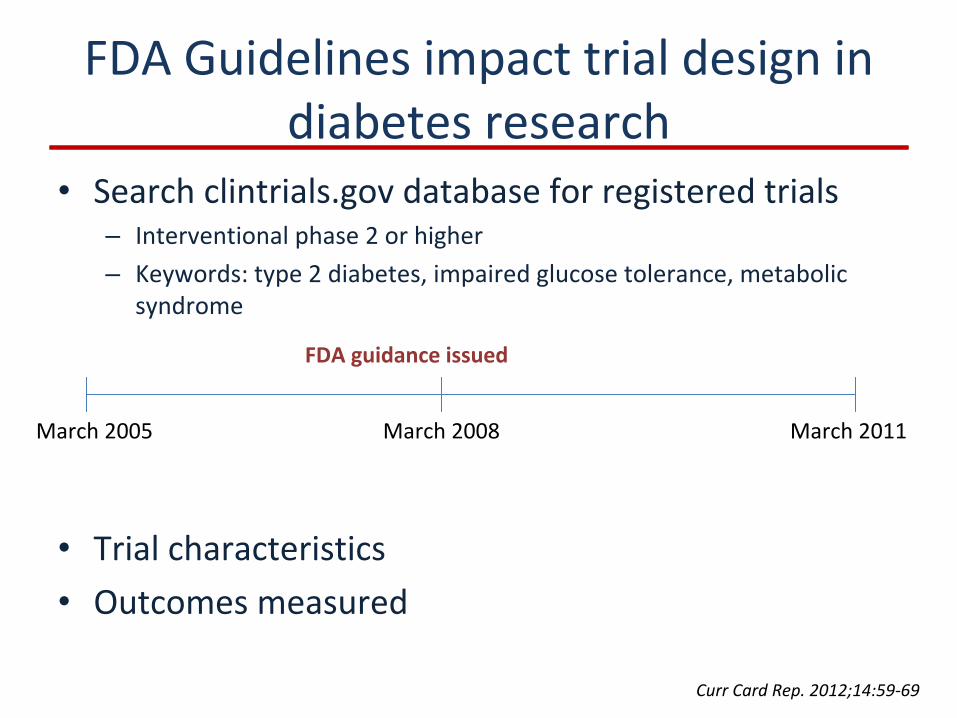
FDA Guidelines impact trial design in diabetes research
•
Search clintrials.gov database for registered trials–
Interventional phase 2 or higher–
Keywords: type 2 diabetes, impaired glucose tolerance, metabolic
syndrome
•
Trial characteristics•
Outcomes measured
March 2008March 2005 March 2011
FDA guidance issued
Curr Card Rep. 2012;14:59‐69
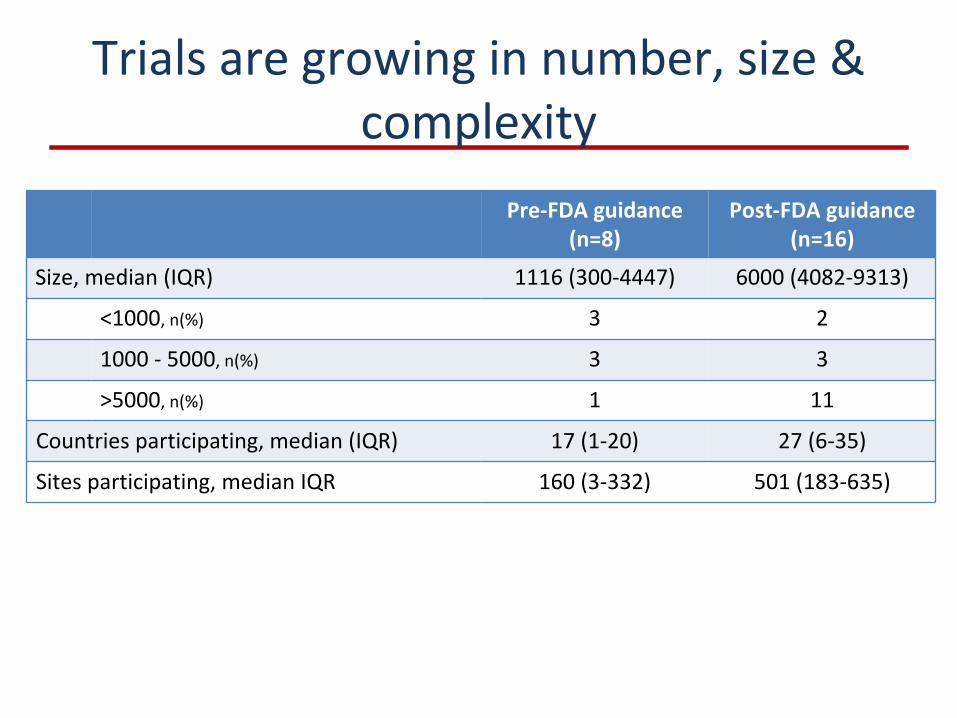
Trials are growing in number, size & complexity
Pre‐FDA guidance(n=8)
Post‐FDA guidance(n=16)
Size, median (IQR) 1116 (300‐4447) 6000 (4082‐9313)
<1000, n(%) 3 2
1000 ‐
5000, n(%) 3 3
>5000, n(%) 1 11
Countries participating, median (IQR) 17 (1‐20) 27 (6‐35)
Sites participating, median IQR 160 (3‐332) 501 (183‐635)
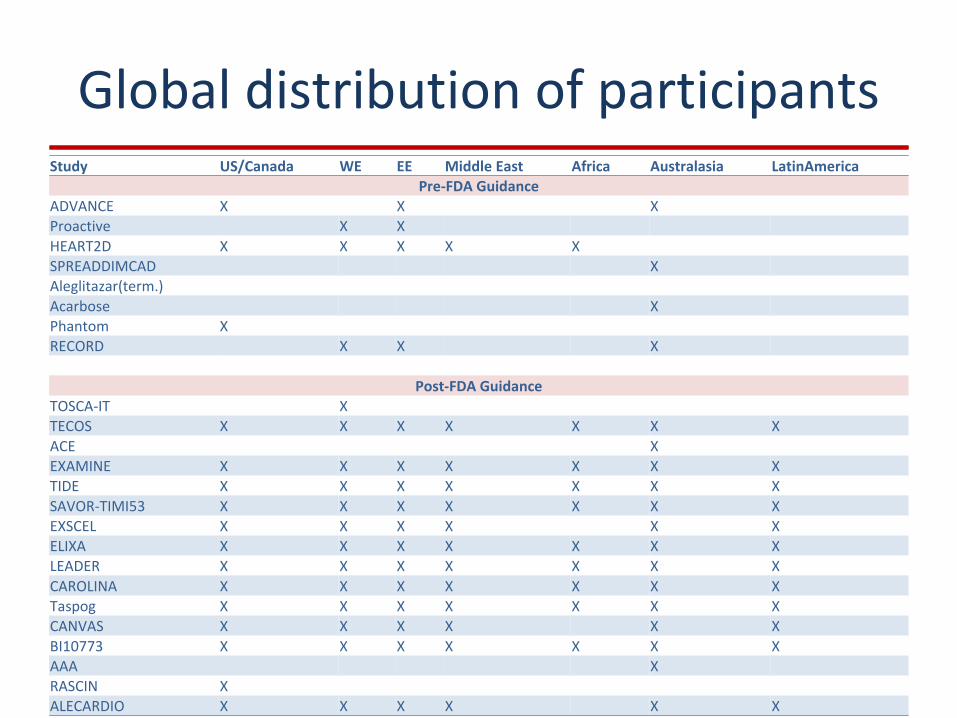
Global distribution of participantsStudy US/Canada WE EE Middle East Africa Australasia LatinAmerica
Pre‐FDA GuidanceADVANCE X X XProactive X XHEART2D X X X X XSPREADDIMCAD XAleglitazar(term.)Acarbose XPhantom XRECORD X X X
Post‐FDA GuidanceTOSCA‐IT XTECOS X X X X X X XACE XEXAMINE X X X X X X XTIDE X X X X X X XSAVOR‐TIMI53 X X X X X X XEXSCEL X X X X X XELIXA X X X X X X XLEADER X X X X X X XCAROLINA X X X X X X XTaspog X X X X X X XCANVAS X X X X X XBI10773 X X X X X X XAAA XRASCIN XALECARDIO X X X X X X
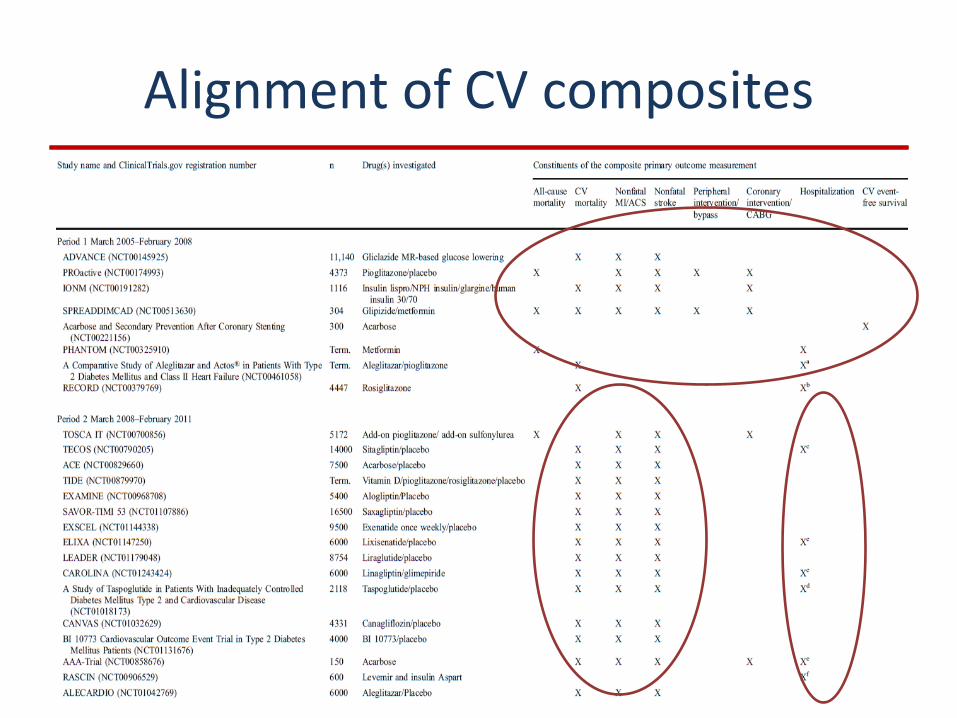
Alignment of CV composites
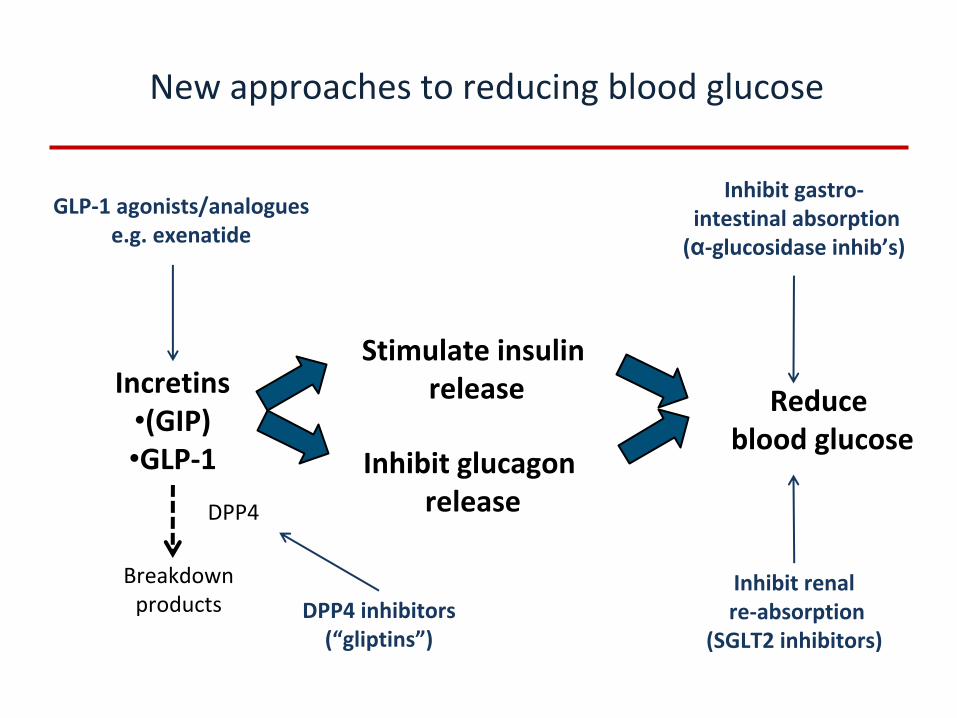
Incretins•(GIP)•GLP‐1
Stimulate insulinrelease
Inhibit glucagonrelease
Reduceblood glucose
DPP4
Breakdownproducts DPP4 inhibitors
(“gliptins”)
GLP‐1 agonists/analoguese.g. exenatide
Inhibit renalre‐absorption
(SGLT2 inhibitors)
Inhibit gastro‐intestinal absorption(α‐glucosidase inhib’s)
New approaches to reducing blood glucose
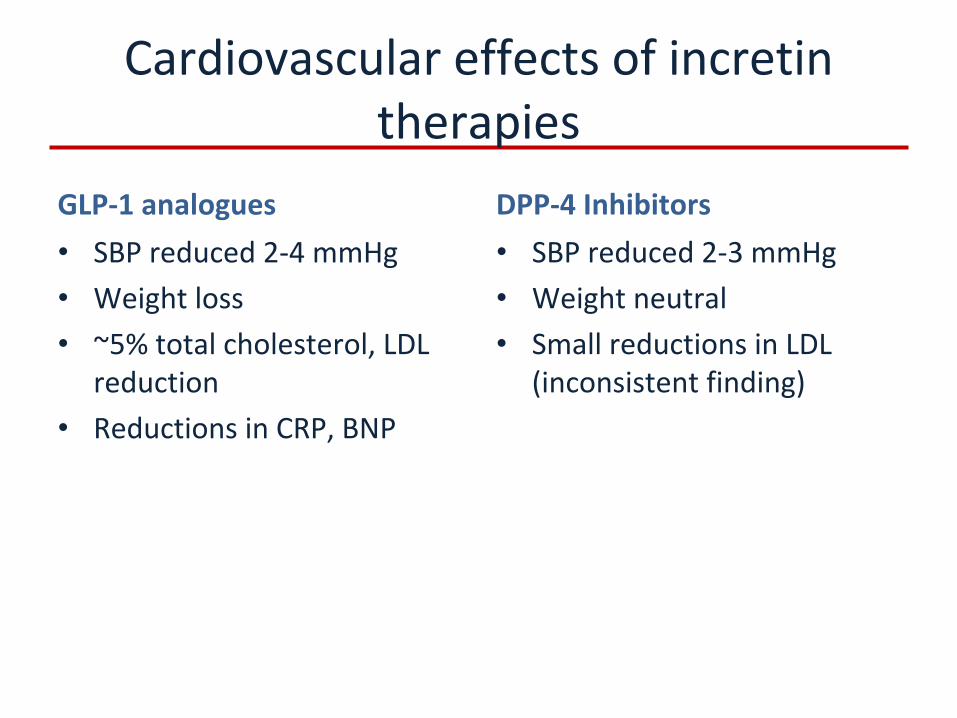
Cardiovascular effects of incretin therapies
GLP‐1 analogues•
SBP reduced 2‐4 mmHg
•
Weight loss•
~5% total cholesterol, LDL
reduction•
Reductions in CRP, BNP
DPP‐4 Inhibitors•
SBP reduced 2‐3 mmHg
•
Weight neutral•
Small reductions in LDL
(inconsistent finding)
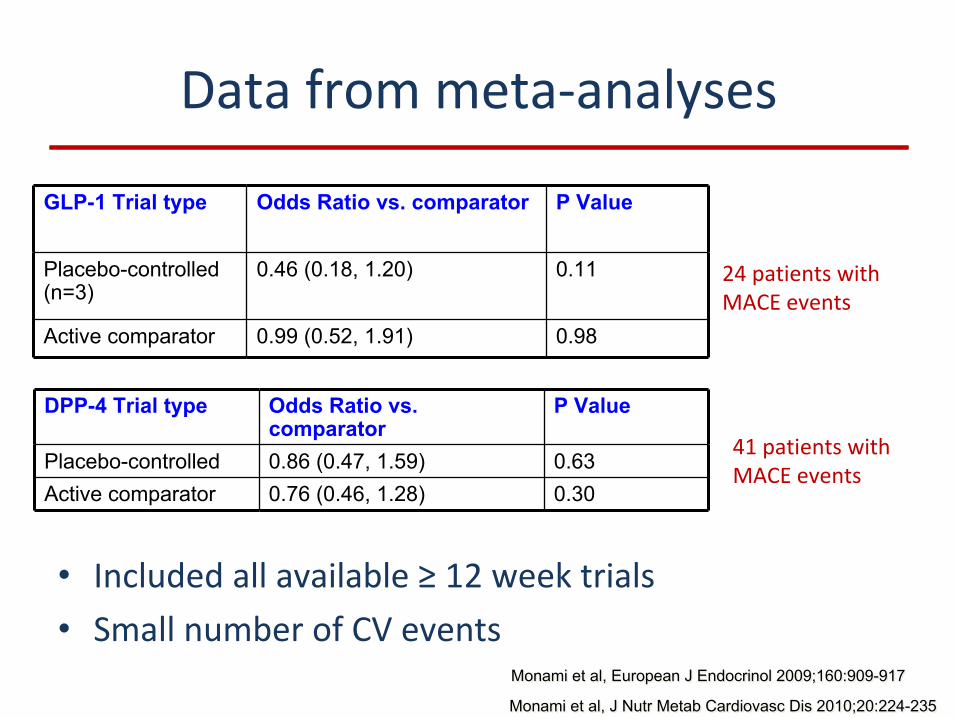
Data from meta‐analyses
•
Included all available ≥
12 week trials•
Small number of CV events
GLP-1 Trial type Odds Ratio vs. comparator P Value
Placebo-controlled (n=3)
0.46 (0.18, 1.20) 0.11
Active comparator 0.99 (0.52, 1.91) 0.98
DPP-4 Trial type Odds Ratio vs. comparator
P Value
Placebo-controlled 0.86 (0.47, 1.59) 0.63Active comparator 0.76 (0.46, 1.28) 0.30
Monami et al, European J Endocrinol 2009;160:909-917Monami et al, European J Endocrinol 2009;160:909-917
Monami et al, J Nutr Metab Cardiovasc Dis 2010;20:224-235Monami et al, J Nutr Metab Cardiovasc Dis 2010;20:224-235
24 patients with
MACE events
41 patients with
MACE events
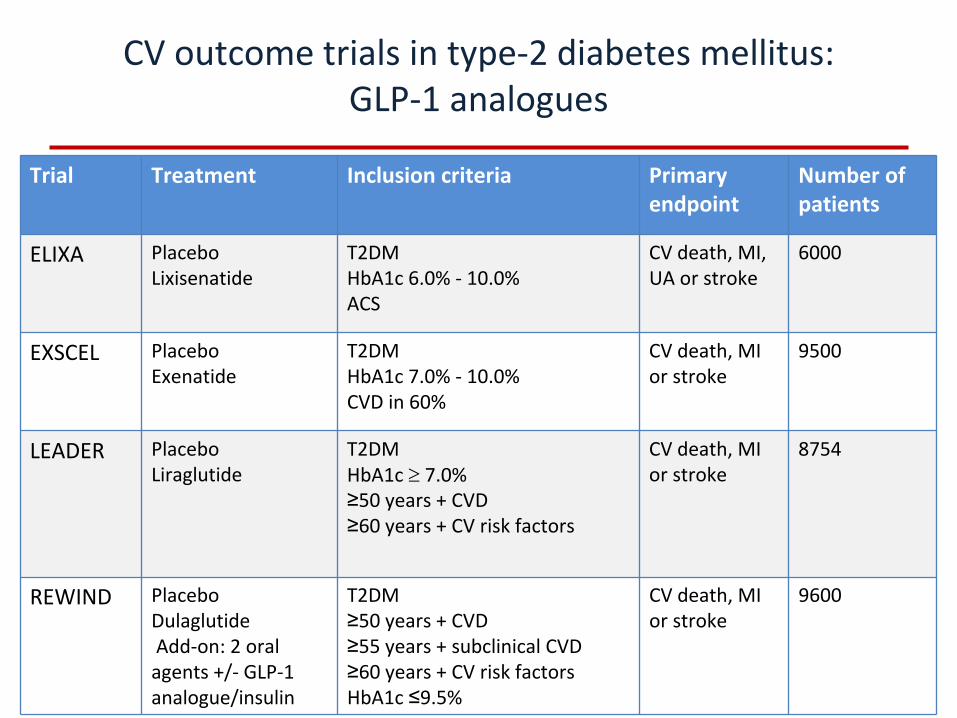
CV outcome trials in type‐2 diabetes mellitus: GLP‐1 analogues
Trial Treatment Inclusion criteria Primary
endpoint
Number of
patients
ELIXA PlaceboLixisenatide
T2DMHbA1c 6.0% ‐
10.0% ACS
CV death, MI,
UA or stroke
6000
EXSCEL PlaceboExenatide
T2DMHbA1c 7.0% ‐
10.0%CVD in 60%
CV death, MI
or stroke
9500
LEADER PlaceboLiraglutide
T2DMHbA1c
7.0% ≥50 years + CVD≥60 years + CV risk factors
CV death, MI
or stroke
8754
REWIND PlaceboDulaglutide Add‐on: 2 oral
agents +/‐
GLP‐1
analogue/insulin
T2DM≥50 years + CVD≥55 years + subclinical CVD≥60 years + CV risk factorsHbA1c ≤9.5%
CV death, MI
or stroke
9600
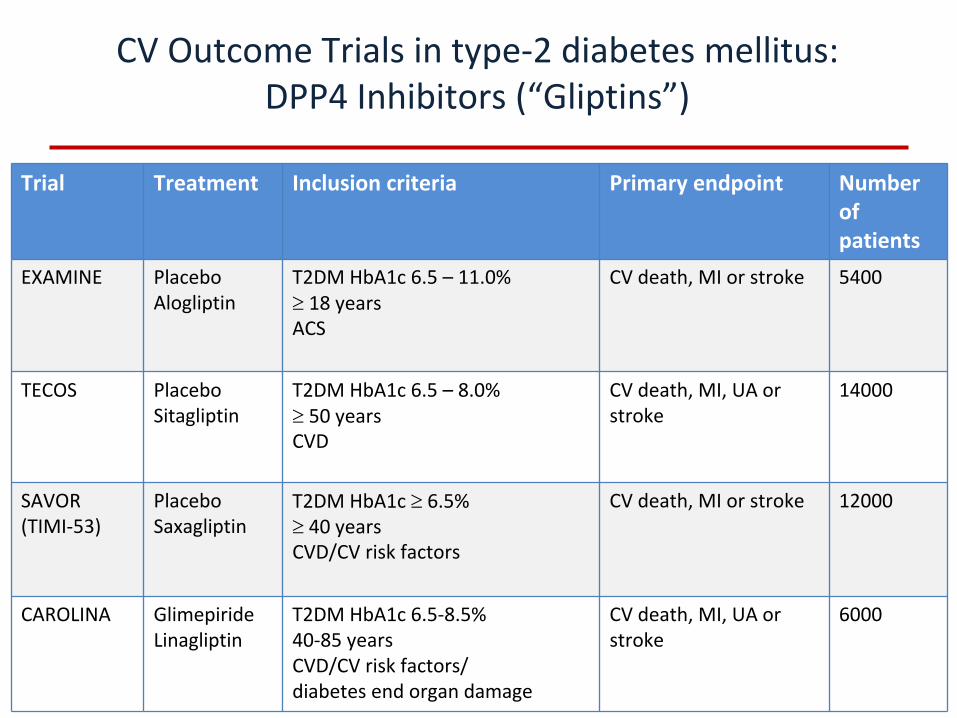
CV Outcome Trials in type‐2 diabetes mellitus: DPP4 Inhibitors (“Gliptins”)
Trial Treatment Inclusion criteria Primary endpoint Number
of
patients
EXAMINE PlaceboAlogliptin
T2DM HbA1c 6.5 –
11.0%
18 yearsACS
CV death, MI or stroke 5400
TECOS PlaceboSitagliptin
T2DM HbA1c 6.5 – 8.0%
50 yearsCVD
CV death, MI, UA or
stroke
14000
SAVOR(TIMI‐53)
PlaceboSaxagliptin
T2DM HbA1c
6.5%
40 yearsCVD/CV risk factors
CV death, MI or stroke 12000
CAROLINA GlimepirideLinagliptin
T2DM HbA1c 6.5‐8.5%40‐85 yearsCVD/CV risk factors/diabetes end organ damage
CV death, MI, UA or
stroke
6000
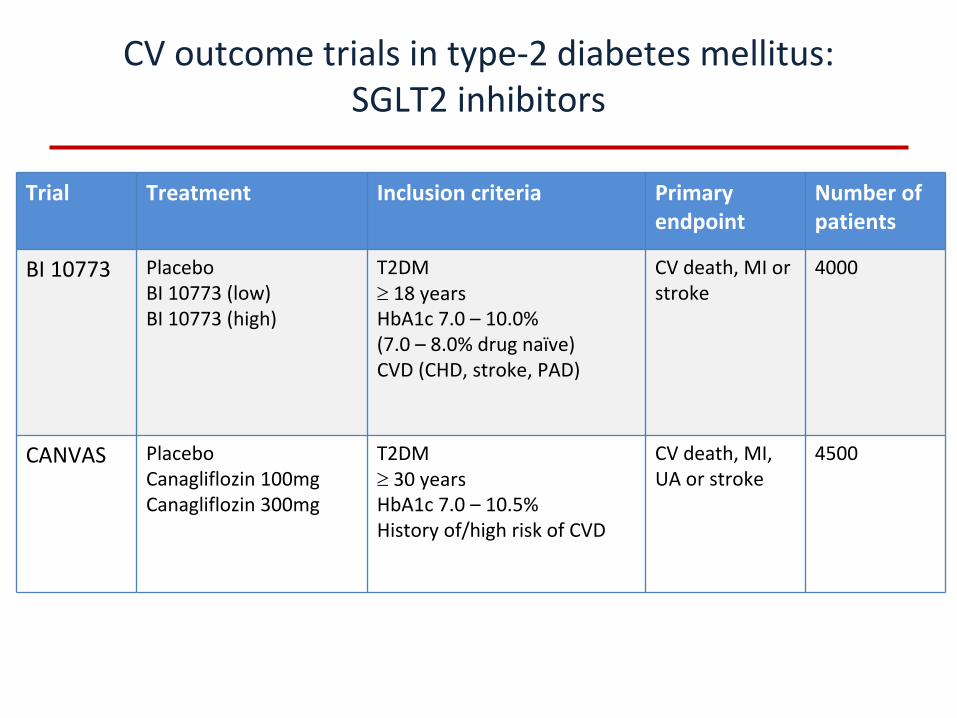
CV outcome trials in type‐2 diabetes mellitus: SGLT2 inhibitors
Trial Treatment Inclusion criteria Primary
endpoint
Number of
patients
BI 10773 PlaceboBI 10773 (low)BI 10773 (high)
T2DM
18 yearsHbA1c 7.0 –
10.0%(7.0 – 8.0% drug naïve)CVD (CHD, stroke, PAD)
CV death, MI or
stroke
4000
CANVAS PlaceboCanagliflozin 100mgCanagliflozin 300mg
T2DM
30 yearsHbA1c 7.0 –
10.5%History of/high risk of CVD
CV death, MI,
UA or stroke
4500
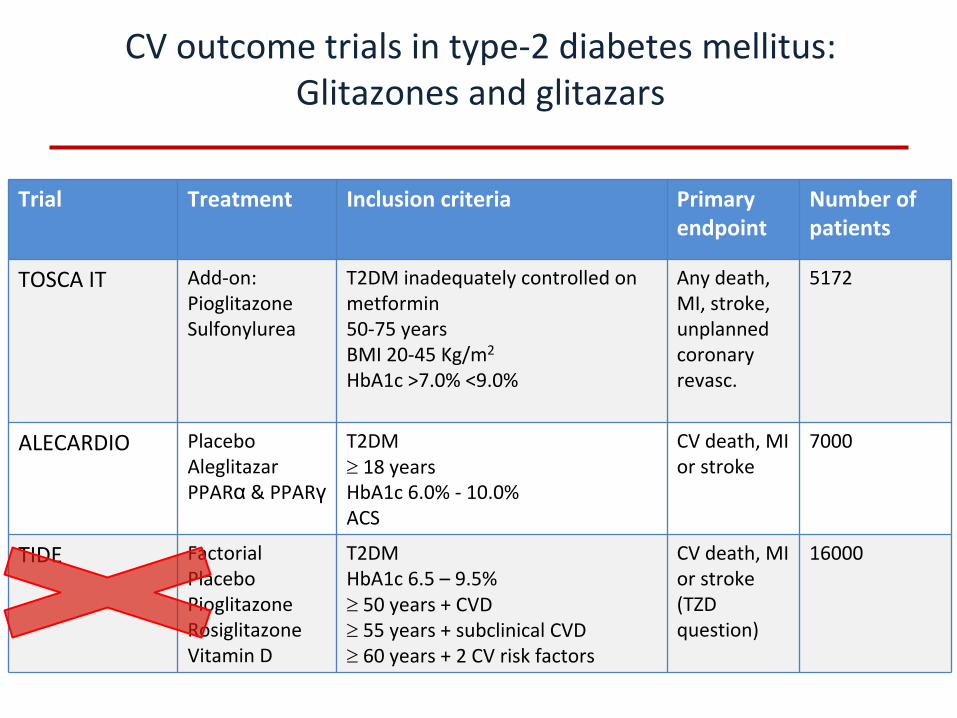
CV outcome trials in type‐2 diabetes mellitus: Glitazones and glitazars
Trial Treatment Inclusion criteria Primary
endpoint
Number of
patients
TOSCA IT Add‐on:PioglitazoneSulfonylurea
T2DM inadequately controlled on
metformin50‐75 years BMI 20‐45 Kg/m2
HbA1c >7.0% <9.0%
Any death,
MI, stroke,
unplanned
coronary
revasc.
5172
ALECARDIO PlaceboAleglitazarPPARα
& PPARγ
T2DM
18 years HbA1c 6.0% ‐
10.0%ACS
CV death, MI
or stroke
7000
TIDE FactorialPlaceboPioglitazoneRosiglitazoneVitamin D
T2DMHbA1c 6.5 – 9.5%
50 years + CVD
55 years + subclinical CVD
60 years + 2 CV risk factors
CV death, MI
or stroke
(TZD
question)
16000
•
Hypoglycemia–
? Adrenergic overdrive
–
? Causal pathway for mortality or macrovascular events
•
Off-target effects of therapeutic choices–
Cardiovascular morbidity?
–
Fractures?–
Cancer?
–
Pancreatitis? Pancreatic cancer?
Defining the risks of overtreatment
(unproven)
(unproven)
•
Generally unexpected, sometimes rare events
•
Gold standard for evaluation remains RCT, but not always feasible
•
Other methodologies –
Epidemiology
–
Post-marketing surveillance–
Registries/Electronic Medical Record
Understanding off-target effects
But there are inherent biases
Biases in existing data collection methods
•
Incomplete Data•
Total number exposed is unknown
•
Reporting bias–
Affected by emerging therapies
–
Affected by media attention
•
Little information to assess–
Exposure time
–
Relatedness
Future of outcomes trials in diabetes
•
More complex trials require efficiencies of design & conduct
•
Quantifying off‐target effects is the next challenge–
Common outcomes are easy to study (cardiovascular
disease)–
Rare outcomes will require innovative approaches
THANK YOU
BACKUP SLIDES
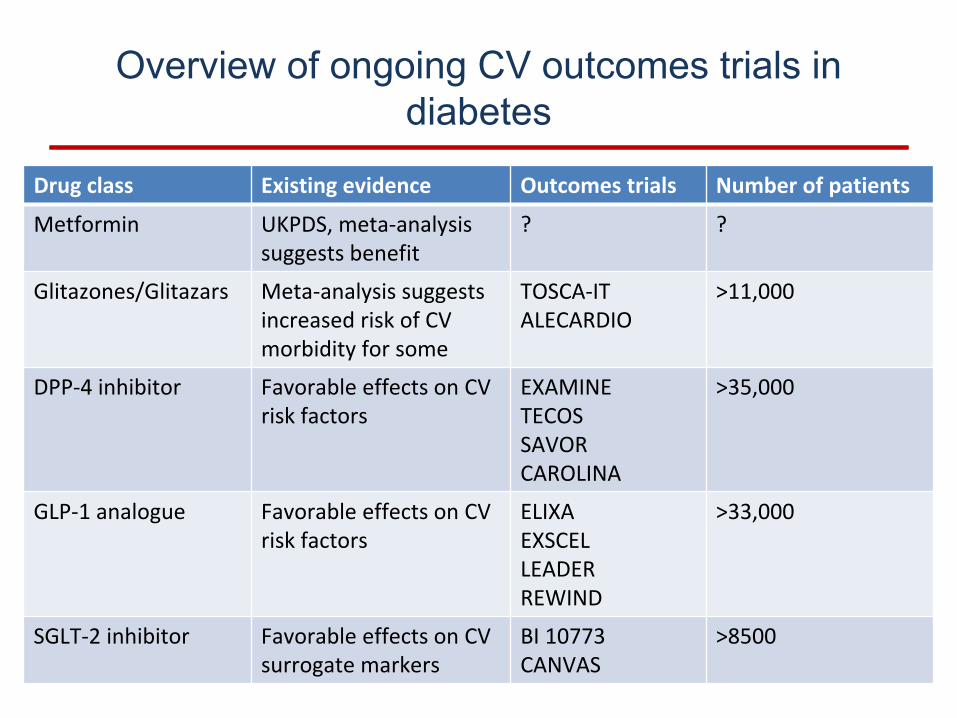
Drug class Existing evidence Outcomes trials Number of patients
Metformin UKPDS, meta‐analysis
suggests benefit
? ?
Glitazones/Glitazars Meta‐analysis suggests
increased risk of CV
morbidity for some
TOSCA‐ITALECARDIO
>11,000
DPP‐4 inhibitor Favorable
effects on CV
risk factors
EXAMINETECOSSAVORCAROLINA
>35,000
GLP‐1 analogue Favorable effects on CV
risk factors
ELIXAEXSCELLEADERREWIND
>33,000
SGLT‐2 inhibitor Favorable effects on CV
surrogate markers
BI 10773CANVAS
>8500
Overview of ongoing CV outcomes trials in diabetes