Embed Size (px)
Citation preview

Cardiovascular Injury Induced by Sympatbetie Catecholamines
Jacob I. Haft
The damaging effect of sympathetic catecholamines on phenomenon are presented, and the recent data that sug-
the cardiovascular system is reviewed. The catecholamines gests that intravascular platelet aggregation is of etiologic
in high dose cause diffuse necrotic lesions in the myo- importance is reviewed. The possible relation of ,these
cardium with accompanying inflammation and subsequent effects of catecholaminas to myocardial infarction that
fibrous scarring. This can be readily demonstrated in the occurs during stress is discussed. High doses of catechol-
experimental animal. The clinical counterpart is seen in amines causa medial necrosis, destruction of the elastic
patients dying after prolonged treatment with norepi- lamellae, and atrophic scarring of the wallsof large vessels.
nephrine and among patients dying with pheochromocy- The relationship of this lesion and other effects of
toma. The various theories suggested to explain this catecholamines to atherosclerosis is reviewed.
T HE SYMPATHETIC catecholamines have pro- found physiologic effects on the heart and
the blood vessels. In the heart, inotropy is en- hanced with an increase in the amount and rate of tension developed with each beat, with a resulting decrease in the end-diastolic pressure and the end- systolic volume. Cardiac automaticity is increased as manifested by an acceleration of the sinus rate and by the development of ectopic atria1 and ventricular arrhythmias. Oxygen and substrate con- sumption by the heart is increased as is the amount of lipid available in the blood for use as fuel. In the blood vessels, the various catecholamines lead to constriction and/or dilatation, depending on the specific vascular bed and on the specific sympa- thetic catecholamine. In addition to altering the function of the cardiovascular system, effects that can be either beneficial or deleterious to the organism, catecholamines have been demonstrated to cause anatomic damage to the heart and to the blood vessels. It is the purpose of this report to re- view the latter effects.
intramyocardial hemorrhage, edema, patchy areas of myofibrillar damage, round cell infiltration,, and proliferation of fibrous tissue in the hearts of rabbits subjected to repeated injections of adrena- lin. He found these lesions as early as 6 days after the onset of injections and noted areas of increased connective tissue and “anemic infarcts” after 10 days of adrenalin administration. Pearce’ in 1906 found similar lesions with myofibrillar edema, loss of striations, and increase in fibrous tissue in the heart after seven to 15 injections of adrenalin.
MYOCARDIAL DAMAGE DUE TO CATECHOLAMINES
The injurious effect of catecholamines on cardiac muscle has been known since the beginning of this century. With the availability of relatively purified extracts of the adrenal medulla, numerous investi- gators studied the pathologic effects of parenter- ally administered catecholamines on the heart.
In 1905, Ziegler’ reported the occurrence of
From the Cardiac Section, Bronx V.A. Hospital, and the Mount Sinai School of Medicine, New York, N. Y.
Reprint requests should be addressed to Dr. Jacob I. Haft, Chief Cardiac Section, V.A. Hospital, I30 West Kingsbridge Road, Bronx, N, Y. 10468.
0 1974 by Grune & Stratton, Inc.
During studies of induced cardiac hypertrophy, Josue in 1907 noted myocardial degeneration and foci of sclerosis (ilots de tissu sclereux) in rabbits who received adrenalin intravenously in conjunc- tion with subcutaneous injections of sterilized typhoid bacteria. Fleisher and Loeb4 in 1909 pro- duced similar lesions with either spartein or caffein in combination with adrenalin. They found that production of the lesions was dependent on the adrenalin, but in the absence of the additional substances higher doses of adrenalin were neces- m-y. In 19Y1, Christian et al.5”‘.fbund cardiac necrosis and fibrosis of the same type while in- vestigating the effects of adrenalin injections on the production of renal and cardiac injury.
These cardiotoxic effects of adrenalin have been confirmed repeatedly. 9-16 With demonstration that norepinephrine is also secreted by the sympathetic nervous system, and the development of isopro- terenol, it was shown that these catecholamines are also markedly effective in producing experi- mental myocardial injury.rr-r5 ,17-31 Characteristic myocardial lesions induced by catecholamines have been produced in many species of laboratory animals, including rabbits, rats, dogs, cats, pigs, hamsters, and turtles.
Catecholamine-induced necrosis and fibrosis of
Progress in Cardiovascuiar Diseases, Vol. XVII. No. 1 (July/August). 1974 73
74
the myocardium had also been documented to occur in man. In 1937, Franz,32 and in 1939, Gormsen33 each reported deaths related to an overdose of epinephrine that had been used for treatment of asthma. On postmortem examina- tion, these patients were found to have lesions in the myocardium similar to those described in ex- perimental animals. Szakacs and Cannon’7 in 1958 de&bed two patients who died after prolonged infusion of norepinephrine for the treatment of shock in whom focal myocarditis with degenera- tion of myofibrils and infiltration of leukocytes were found on histologic study of their hearts. In a further report in 1960, Szakacs and Mehlman” noted the occurrence of similar lesions in three additional patients treated with norepinephrine.
The spontaneous counterpart of administration of excess amounts of exogenous sympathetic cate- cholamines is seen in patients with pheochromocy- tomas. In a review of the literature in 1957, Wat- kins34 drew attention to the frequently reported finding of multiple sites of focal fibrosis in the myocardium in patients dying with pheochromo-
JACOB I. HAFT
cytomas. Szakacs and Cannon” found evidence of acute myocarditis in three of 17 patients with pheochromocytoma and myocardial disease in the others. The lesions were identical with those seen in patients dying after prolonged norepinephrine infusion and in animals experimentally infused with norepinephrine. Kline35 reported similar findings in four of seven patients with pheochro- mocytoma. Van Vliet et al.,22 on review of 26 cases seen at the Mayo Clinic from 1928 to 1964, found active myocarditis in 15 patients and myo- cardial fibrosis in eight of the others, including two that had distribution of the fibrotic lesions similar to that of the active myocarditic lesions. On com- parison of the myocardial lesion found in their patients with the experimental cardiac lesion pro- duced by norepinephrine injection in rats, these investigators found a marked similarity. Those rats killed shortly after injection showed lesions similar to the patients with active myocarditis, and those rats killed weeks after injection showed the diffuse pattern of myocardial scarring seen in the pheo- chromocytoma patients with myocardial fibrosis.
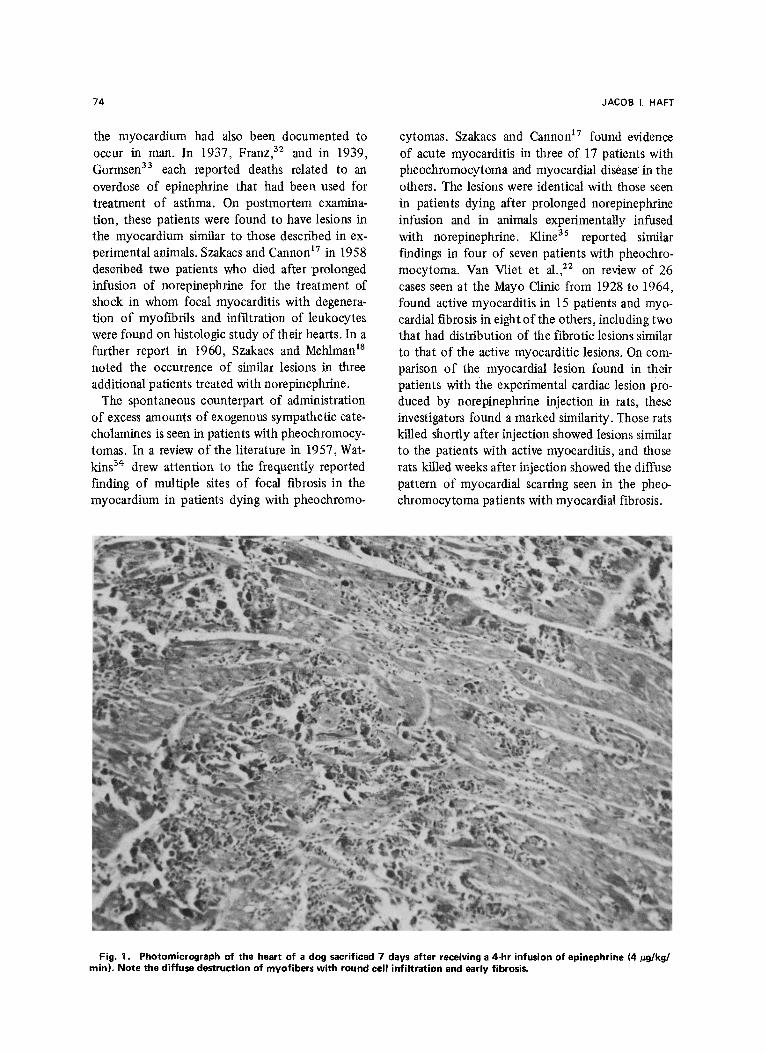
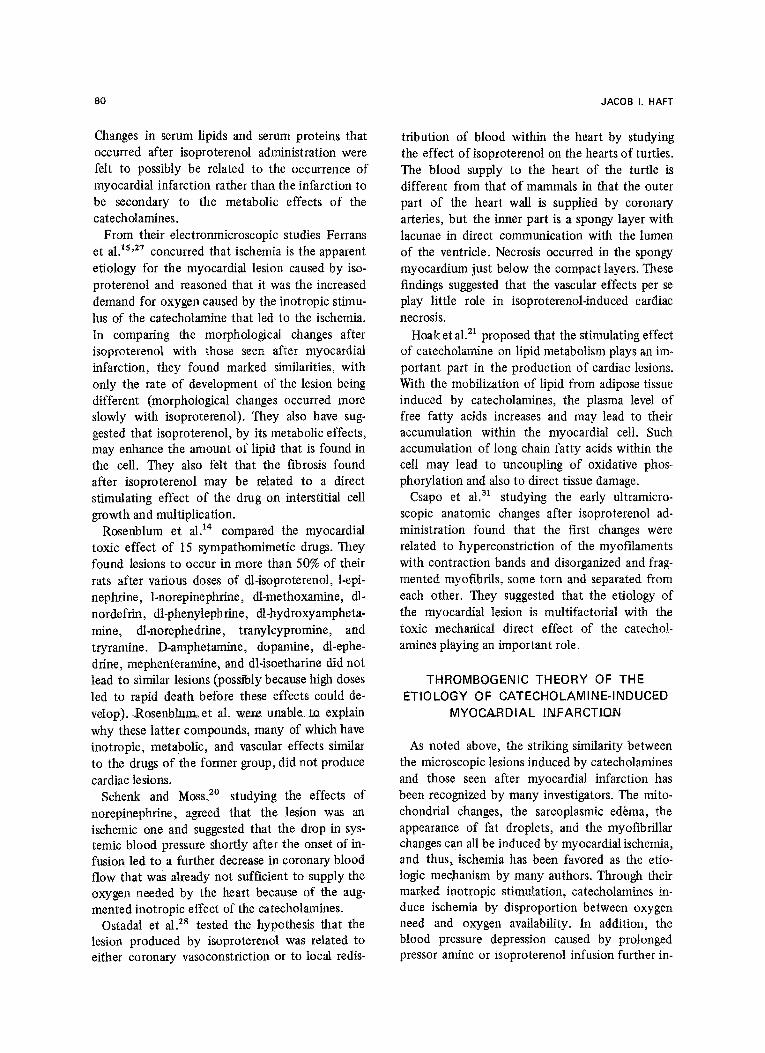
Fig. 1. Photomicrograph of the heart of a dog sacrificed 7 days after receiving a 4-hr infusion of epinephrine (4 @g/kg/ min). Note the diffuse destruction of myofibers with round cell infiltration and early fibrosis.
INJURY INDUCED BY SYMPATHETIC CATECHOLAMINES
THE MYOCARDIAL LESION
The myocardial lesion produ,ced by catechol- amine administration is similar in all species that have been studied (including man) and does not differ with the catecholamine used or the route of administration. The severity and extent varies directly with the dose and rate of administration; the pathologic appearance of the lesion is deter- mined by the time that has elapsed between ad- ministration of the drug and sacrifice of the animal.
On gross examination, in those animals studied shortly after infusion (or in those patients dying during norepinephrine infusion or with acute myo- carditis due to activity of a pheochromocytoma), subendocardial and intramyocardial hemorrhages are seen.‘1~‘2~18~20~21 These are found predomi- nantly in the left ventricle13y20P21 but occur in all chambers of the heart. Edema and hemorrhages into the valve leaflets and in the subendocardial
75
myocardium also are seen occasionally.‘1Y’2 Within hours to a few days, patches of anemic infarction with the appearance of pale, yellow-brown areas are found in the ventricular myocardium.4’13725 The myocardium in these areas is stiffened and loses its pliability? After weeks, areas of gray, scarred fibrosis may be seen.
Immediately after infusion, on microscopic ex- amination, congestion of the vasculature,5T’3 in- terstitial edema,2P47s313 focal myofiber degenera- tion with loss of striations of individual muscle fibers, vacuolization, and accumulation of lipid droplets within myofibers is seen.12~13~1s~1gy20~21~ 27T31 Subendocardial vascular congestion and hemorrhages” ,13 especially in the regions of thebesian vessels2’ are a common finding. Within hours 15Y2sy30 interstitial edema and infiltration with ’ polymorphonuclear leukocytes and then mononuclear cells appearsy13 frequently in peri- vascular areas or surrounding necrotic myocardial
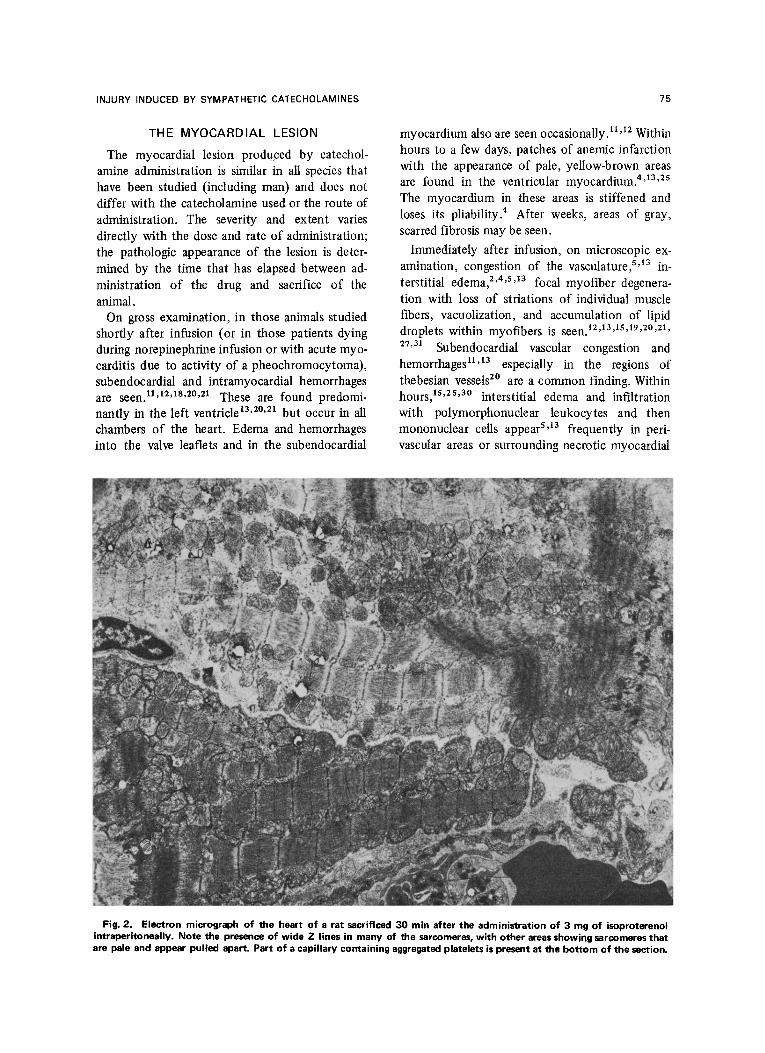
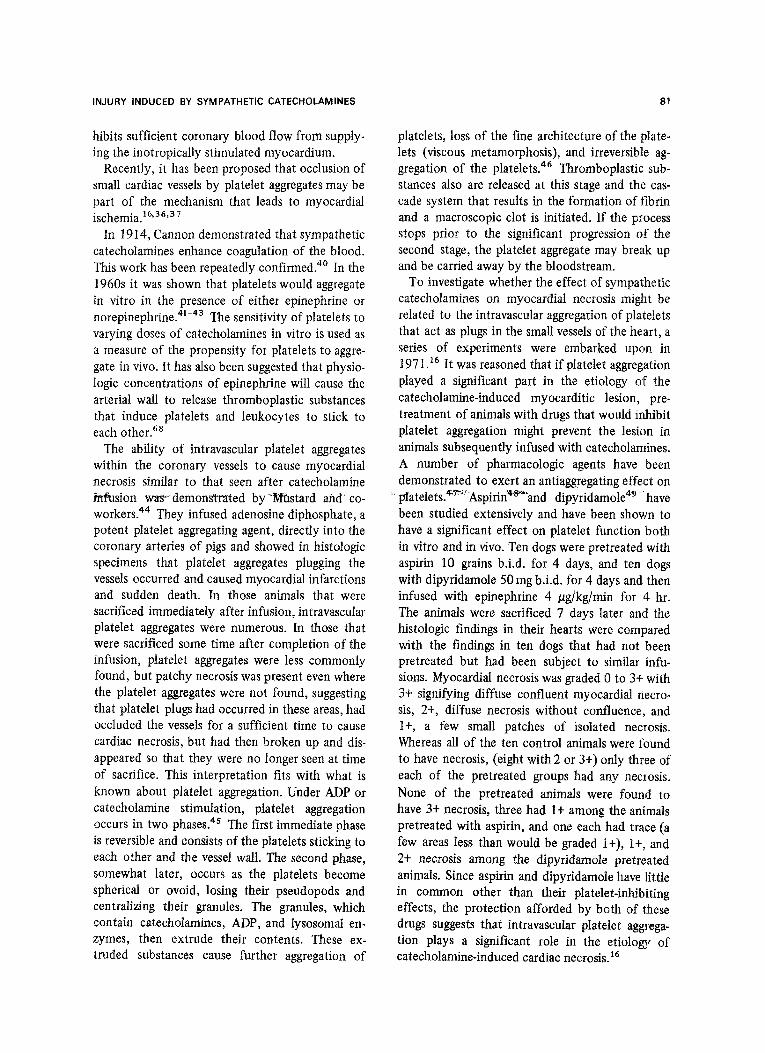
Fig. 2. Electron micrograph of the heart of a rat sacrificed 30 min after the administration of 3 mg of isoproterenol intraperitoneally. Note the presence of wide 2 lines in many of the sarcomeres, with other areas showing sarcomeres that are pale and appear pulled apart. Part of a capillary containing aggregated platelets is present at the bottom of the section.
76
cells. Perivascular Anitschkow myocyte type cells are also seen.13~18920 Fibrinoid degeneration of arterioles has been noted.11718~z2
After 3 days, 2~4~14Y15~20,22 distinct foci of necro- sis with disolution of the myolibrils and sarcoplas- mic fragmentation are present (Fig. 1). Infiltration with histiocytes, lymphocytes, and occasionally plasma cells” are found. Polymorphonuclear cells are rare at this stage.30 Starting from about this time, fibrotic bands appear in the interstitium. Over the next few weeks, the necrotic debris of the destroyed myocardial cells are removed by phago- cytes, and the acute inflammatory changes abate. 2p4920 Fibrous replacement with collaginous bands, especially in areas surrounding the microvascula- ture, becomes prominent as healing progresses, 2p4~16 and late lesions show only these scars as evi- dence of the earlier acute necrotic 1esions.4920922t30
On electronmicroscopic examination, the myo- cardial cells show distinct changes in the myo-
JACOB I. HAFT
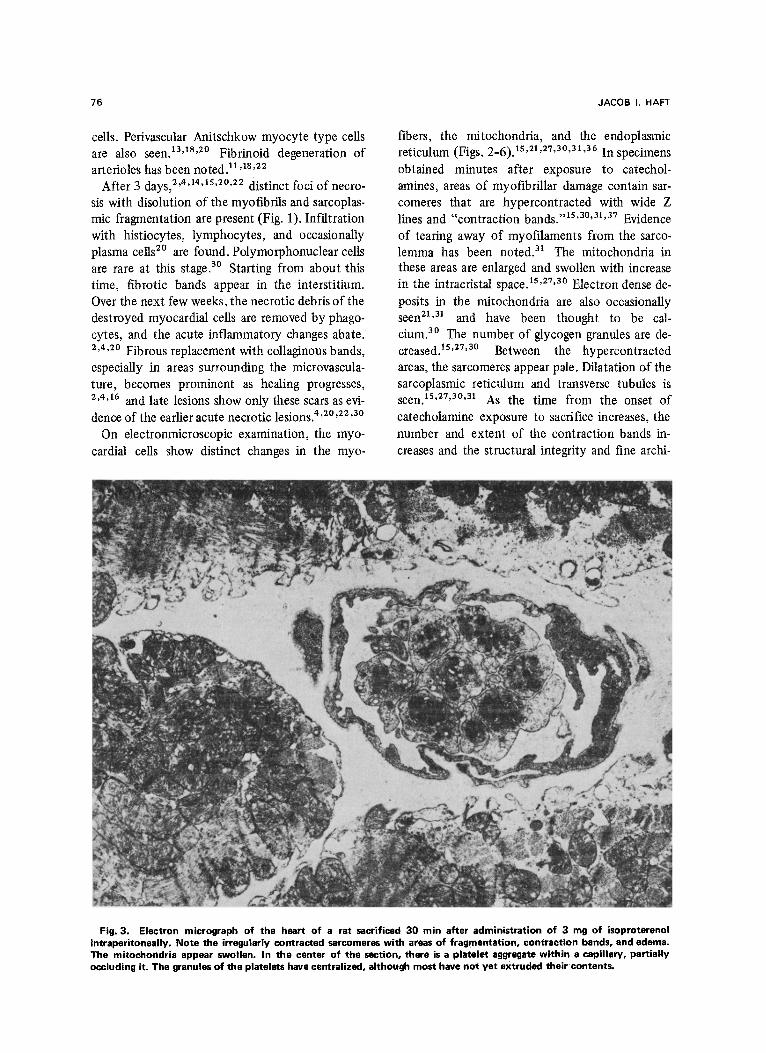
fibers, the mitochondria, and the endoplasmic reticulum (Figs. 2-6).‘5*21Y27~30~31~36 In specimens obtained minutes after exposure to catechol- amines, areas of myotibrillar damage contain sar- comeres that are hypercontracted with wide 2 lines and “contraction bands.“15~30931y37 Evidence of tearing away of myofilaments from the sarco- lemma has been noted.31 The mitochondria in these areas are enlarged and swollen with increase in the intracristal space. r5s27530 Electron dense de- posits in the mitochondria are also occasionally seen21s3’ and have been thought to be cal- cium.30 The number of glycogen granules are de- creased.15Y27Y30 Between the hypercontracted areas, the sarcomeres appear pale. Dilatation of the sarcoplasmic reticulum and transverse tubules is seen. 1sy27930931 As the time from the onset of catecholamine exposure to sacrifice increases, the number and extent of the contraction bands in- creases and the structural integrity and fine archi-
Fig. 3. Electron micrograph of the heart of a rat sacrificed 30 min after administration of 3 mg of isoproterenot intraperitoneaily. Note the irregularly contracted sarcomeres with areas of fragmentation, contraction bands, and edema. The mitochondria appear swollen. In the center of the section, there is a platelet aggregate within a capillary, partially occluding it. The granules of the platelets have centralized, although most have not yet extruded their contents.
INJURY INDUCED BY SYMPATHETIC CATECHOLAMINES
tecture of the sarcomeres begin to show evidence of destruction. Swelling and dilatation of the endo- plasmic reticulum15~30 and development of lipid droplets is seen. 15~27 In specimens obtained be- yond 8 hr after onset of catecholamine exposure, dissolution of myofibrils with loss of striations and Z lines is seen; mitochondria are markedly swollen with destruction of cristae,” and leukocytes make their appearance. Evidence of phagocytosis of myotibrillar debris appears.30 An increase in the number of lysosomes has been noted.r5 In our studies of the hearts of animals sacrificed shortly after administration of catecholamines,36p37 many small myocardial vessels were found to contain aggregated platelets.
THEORIES
There have been numerous theories suggested to explain the damaging effect of catecholamines on the heart. Pearce’ in 1906 considered the lesion to be related to constriction of the coronary arteries
77
caused directly by adrenalin. Such constriction was felt to be sufficient to interfere with augmentation of the blood supply that was needed by the more vigorously contracting myocardium. He noted that lesions were similar to those found after ligation of a coronary artery. Pearce considered but rejected a direct toxic effect of adrenalin on heart muscle and did not feel that lesions in the aorta at the ostia of the coronaries were sufficient to explain the findings.
Fleisher and Loeb4F38 felt that a mechanical factor played the significant role, with the violent contraction caused by adrenalin causing the re- sultant damage. They also suggested that direct toxic effects of adrenalin may be related. Because they considered adrenalin not to cause constriction of coronary vessels they did not feel that the myo- cardial lesions were related to a decrease in myo- cardial nutrition.
Vishnevskayar’ studied the relationship of the nervous system to the myocarditis that occurs
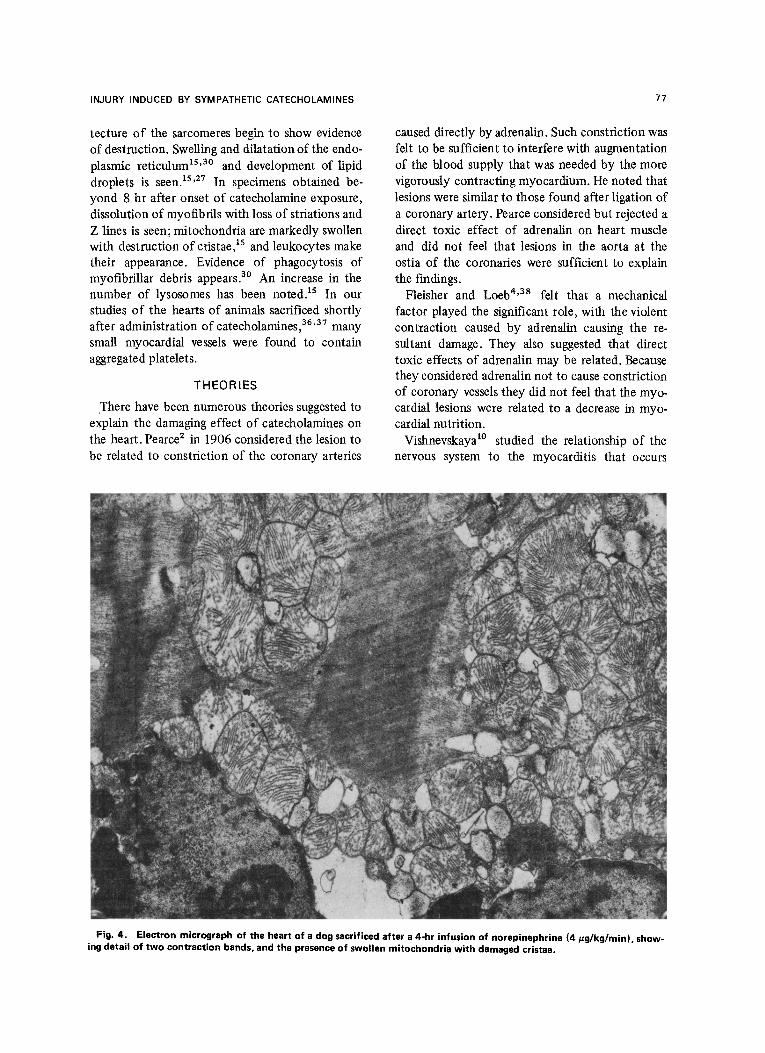
Fig. 4. Electron micrograph of the heart of a dog sacrificed after a 4-hr infusion of norepinephrine (4 pg/kg/min), show-
ing detail of two contraction bands, and the presence of swollen mitochondria with damaged cristae.
78
after adrenalin administration. He found that the incidence of the myocardial lesion was signifi- cantly decreased in rats that had their spinal cords severed at C7-Tl prior to adrenalin administration and that the severity of the lesion increased in rats that had been decorticated. He interpreted these results to indicate that reflex arcs play a part in the etiology of the lesion.
Szakacsr7 suggested three possible mechanisms to explain the myocarditic damage associated with norepinephrine. The vagal stimulation seen during administration of both epinephrine and norepi- nephrine was felt to possibly play a role, since it had been previously shown that vagal stimulation alone can lead to subendocardial hemorrhages. The role of catecholamines in high energy phosphate transfer that is necessary for dissociation of actin and myosin during the relaxation phase might be of etiologic importance. An overabundance of epi- nephrine or norepinephrine may be toxic, increas-
JACOB I. HAFT
ing the dissociation of actin and myosin molecules of the contractile apparatus to an irreversible ex- treme. He also, considered that anoxia might be related but did not feel that direct mechanical effects on contraction played a significant role.
Maling and Highman12 noted fat droplets in myocardial cells after catecholamine administra- tion and suggested that these were similar in etiology to the fat infiltration seen at the periphery of infarcts, suggesting that ischemia plays an im- portant role. This ischemia might be due either to increased oxygen utilization because of increased work of the heart, or to coronary vasoconstriction. They found that the myocardium was protected from these effects by dibenzyline, and interpreted this to suggest that hypertension and coronary vasoconstriction were of etiologic importance. Direct alterations in lipid metabolism might also play a role.
Nahas et al.rr isolated the heart from nervous
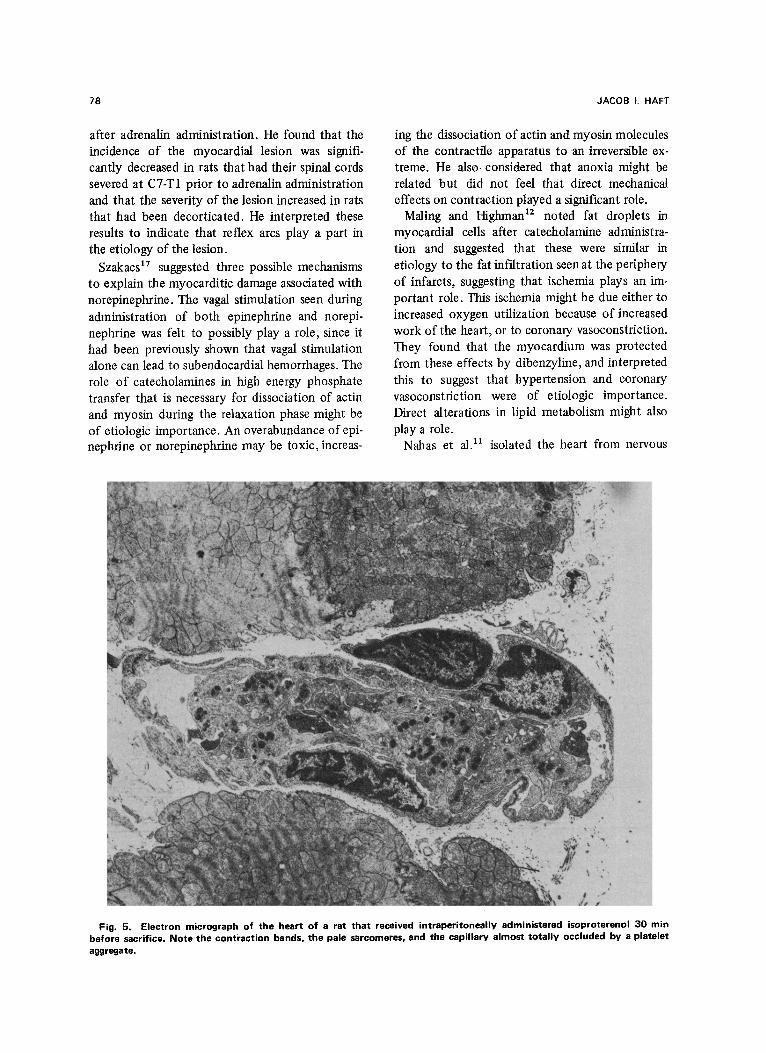
Fig. 5. Electron micrograph of the heart of a rat that received intraperitoneally administered isoproterenol 30 min before sacrifice. Note the contraction bands, the pale sarcomeres, and the capillary almost totally occluded by a platelet aggregate.
INJURY INDUCED BY SYMPATHETIC CATECHOLAMINES
and hormonal influences by studying the effects of catecholamines on the heart-lung preparation. They found the same cardiac lesions, suggesting that reflex arcs do not play a role. They suggested that the prolonged increased myocardial tension induced by the catecholamines may be responsible for cardiac lesions. Furthermore, they also pro- posed that catecholamine effects on lipid metabo- lism may be important, and that the,alteration in lymphatic flow, with dilation and enlargement of lymphatics that they observed, may be related to the interstitial edema that occurred as an early manifestation of damage.
Chappel et al. compared the cardiotoxic effects of isoproterenol with epinephrine, norepinephrine, and ephedrine. Finding that a much lower per- centage of the median lethal dose of isoproterenol (although a much larger amount in milligrams) re- sulted in larger amounts of necrosis, they reasoned that coronary constriction did not play a role. However, they feel that the ischemia due to a dis- proportion between the enhanced myocardial re- quirement for oxygen from the increased inotropy
79
of the heart and the oxygen available was the cause of the lesion. The depressor effect of isopro- terenol on the systemic vasculature widens the in- equality between oxygen supply and demand.
By injection of india ink into the coronary arte- ries of hamsters sacrificed shortly after injection of isoproterenol, Handforth demonstrated that blood flow to the inner areas of the left ventricular wall was markedly reduced, even prior to the de- velopment of myocardial edema or necrosis. He felt that the necrosis that developed was due to ischemic infarction and suggested that either local- ized vasoconstriction or shunting of blood to effectively bypass the subendocardial areas had occurred.
Studying the effects of isoproterenol on serum enzymes and adrenal steroids, Wexler and Kittin- ger*’ noted the close resemblance between the myocardial lesion and that due to myocardial in- farction in breeder rats with spontaneous athero- sclerosis. The effects on serum enzymes and adrenal steroids showed a close similarity to the effects of myocardial infarction in humans.
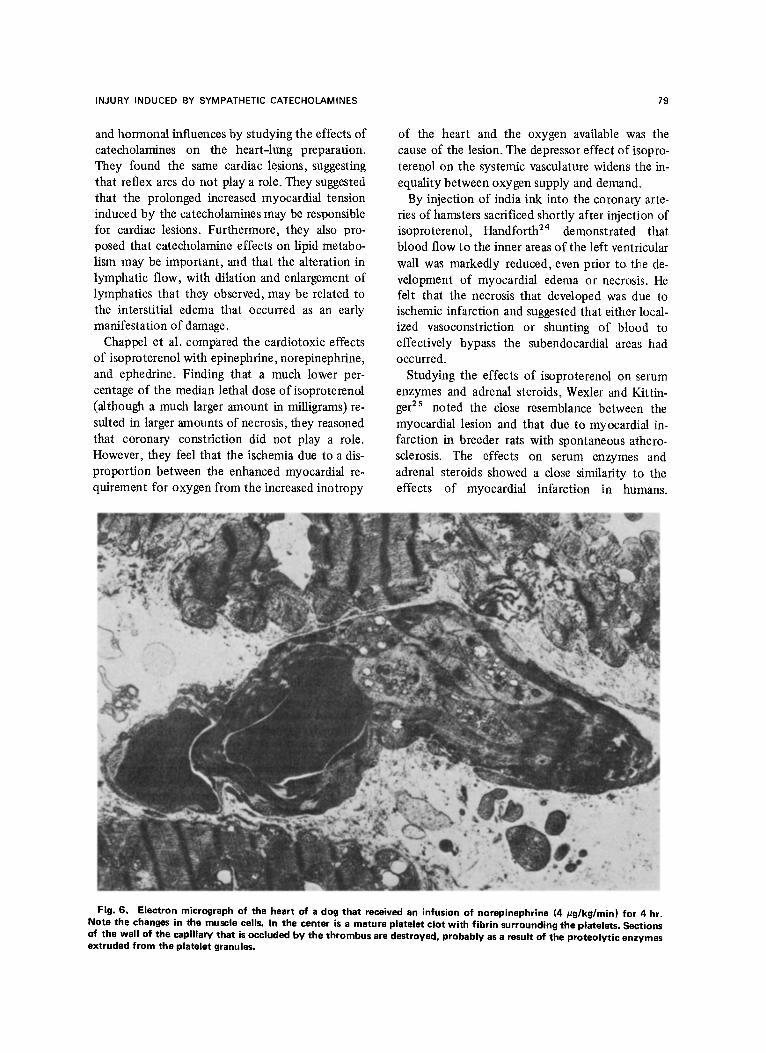
Fig. 6. Electron micrograph of the heart of a dog that received an infusion of norepinephrine (4 tigglkglmin) for 4 hr. Note the changes in the muscle cells. In the center is a mature platelet clot with fibrin surrounding the platelets. Sections of the wall of the capillary that is occluded by the thrombus are destroyed, probably as a result of the proteolytic enzymes extruded from the platelet granules.
80 JACOB I. HAFT
Changes in serum lipids and serum proteins that occurred after isoproterenol administration were felt to possibly be related to the occurrence of myocardial infarction rather than the infarction to be secondary to the metabolic effects of the catecholamines.
From their electronmicroscopic studies Ferrans et al.15~27 concurred that ischemia is the apparent etiology for the myocardial lesion caused by iso- proterenol and reasoned that it was the increased demand for oxygen caused by the inotropic stimu- lus of the catecholamine that led to the ischemia. In comparing the morphological changes after isoproterenol with those seen after myocardial infarction, they found marked similarities, with only the rate of development of the lesion being different (morphological changes occurred more slowly with isoproterenol). They also have sug- gested that isoproterenol, by its metabolic effects, may enhance the amount of lipid that is found in the cell. They also felt that the fibrosis found after isoproterenol may be related to a direct stimulating effect of the drug on interstitial cell growth and multiplication.
Rosenblum et al.r4 compared the myocardial toxic effect of 15 sympathomimetic drugs. They found lesions to occur in more than 50% of their rats after various doses of dl-isoproterenol, l-epi- nephrine, 1-norepinephrine, dl-methoxamine, dl- nordefrin, dl-phenylephrine, dl-hydroxyampheta- mine, dl-norephedrine, tranylcypromine, and tryramine. D-amphetamine, dopamine, dl-ephe- drine, mephenteramine, and dl-isoetharine did not lead to similar lesions (possibly because high doses led to rapid death before these effects could de- velop). ,Rosenblum. et al. were unab1e.t.o explain why these latter compounds, many of which have inotropic, metabolic, and vascular effects similar to the drugs of the former group, did not produce cardiac lesions.
Schenk and Moss,~’ studying the effects of norepinephrine, agreed that the lesion was an ischemic one and suggested that the drop in sys-
temic blood pressure shortly after the onset of in- fusion led to a further decrease in coronary blood flow that was already not sufticient to supply the oxygen needed by the heart because of the aug- mented inotropic effect of the catecholamines.
Ostadal et al.** tested the hypothesis that the lesion produced by isoproterenol was related to either coronary vasoconstriction or to local redis-
tribution of blood within the heart by studying the effect of isoproterenol on the hearts of turtles. The blood supply to the heart of the turtle is different from that of mammals in that the outer part of the heart wall is supplied by coronary arteries, but the inner part is a spongy layer with lacunae in direct communication with the lumen of the ventricle. Necrosis occurred in the spongy myocardium just below the compact layers. These findings suggested that the vascular effects per se play little role in isoproterenol-induced cardiac necrosis.
Hoak et al.*l proposed that the stimulating effect of catecholamine on lipid metabolism plays an im- portant part in the production of cardiac lesions. With the mobilization of lipid from adipose tissue induced by catecholamines, the plasma level of free fatty acids increases and may lead to their accumulation within the myocardial cell. Such accumulation of long chain fatty acids within the cell may lead to uncoupling of oxidative phos- phorylation and also to direct tissue damage.
Csapo et aL3r studying the early ultramicro- scopic anatomic changes after isoproterenol ad- ministration found that the first changes were related to hyperconstriction of the myofilaments with contraction bands and disorganized and frag- mented myofibrils, some torn and separated from each other. They suggested that the etiology of the myocardial lesion is multifactorial with the toxic mechanical direct effect of the catechol- amines playing an important role.
THROMBOGENIC THEORY OF THE
ETIOLOGY OF CATECHOLAMINE-INDUCED MYOCARDIAL lN.FARCT.LfJN
As noted above, the striking similarity between the microscopic lesions induced by catecholamines and those seen after myocardial infarction has been recognized by many investigators. The mito- chondrial changes, the sarcoplasmic edema, the appearance of fat droplets, and the myofibrillar changes can all be induced by myocardial ischemia, and thus, ischemia has been favored as the etio- logic mechanism by many authors. Through their marked inotropic stimulation, catecholamines in- duce ischemia by disproportion between oxygen need and oxygen availability. In addition, the blood pressure depression caused by prolonged pressor amine or isoproterenol infusion further in-
INJURY INDUCED BY SYMPATHETIC CATECHOLAMINES 81
hibits sufficient coronary blood flow from supply- ing the inotropically stimulated myocardium.
Recently, it has been proposed that occlusion of small cardiac vessels by platelet aggregates may be part of the mechanism that leads to myocardial ischemia.‘6Y36p37
In 1914, Cannon demonstrated that sympathetic catecholamines enhance coagulation of the blood. This work has been repeatedly confirmed.” In the 1960s it was shown that platelets would aggregate in vitro in the presence of either epinephrine or norepinephrine. 41-43 The sensitivity of platelets to varying doses of catecholamines in vitro is used as a measure of the propensity for platelets to aggre- gate in vivo. It has also been suggested that physio- logic concentrations of epinephrine will cause the arterial wall to release thromboplastic substances that induce platelets and leukocytes to stick to each other.68
The ability of intravascular platelet aggregates within the coronary vessels to cause myocardial necrosis similar to that seen after catecholamine i?#usion WXY demonstmted by “Wt%tard and’ co- workers.44 They infused adenosine diphosphate, a potent platelet aggregating agent, directly into the coronary arteries of pigs and showed in histologic specimens that platelet aggregates plugging the vessels occurred and caused myocardial infarctions and sudden death. In those animals that were sacrificed immediately after infusion, intravascular platelet aggregates were numerous. In those that were sacrificed some time after completion of the infusion, platelet aggregates were less commonly found, but patchy necrosis was present even where the platelet aggregates were not found, suggesting that platelet plugs had occurred in these areas, had occluded the vessels for a sufficient time to cause cardiac necrosis, but had then broken up and dis- appeared so that they were no longer seen at time of sacrifice. This interpretation fits with what is known about platelet aggregation. Under ADP or catecholamine stimulation, platelet aggregation occurs in two phases. 45 The first immediate phase is reversible and consists of the platelets sticking to each other and the vessel wall. The second phase, somewhat later, occurs as the platelets become spherical or ovoid, losing their pseudopods and centralizing their granules. The granules, which contain catecholamines, ADP, and lysosomal en- zymes, then extrude their contents. These ex- truded substances cause further aggregation of
platelets, loss of the fine architecture of the plate- lets (viscous metamorphosis), and irreversible ag- gregation of the platelets4’ Thromboplastic: sub- stances also are released at this stage and the cas- cade system that results in the formation of Ifibrin and a macroscopic clot is initiated. If the process stops prior to the significant progression of the second stage, the platelet aggregate may break up and be carried away by the bloodstream.
To investigate whether the effect of sympat.hetic catecholamines on myocardial necrosis might be related to the intravascular aggregation of platelets that act as plugs in the small vessels of the heart, a series of experiments were embarked upon in 197 1. l6 It was reasoned that if platelet aggregation played a significant part in the etiology o-f the catecholamine-induced myocarditic lesion, pre- treatment of animals with drugs that would inhibit platelet aggregation might prevent the lesion in animals subsequently infused with catecholamines. A number of pharmacologic agents have been demonstrated to exert an antiaggregating effect on
-’ platelets.@?4spirin4*“and dipyridamole49 .‘have been studied extensively and have been shown to have a significant effect on platelet function both in vitro and in viva. Ten dogs were pretreated with aspirin 10 grains b.i.d. for 4 days, and ten dogs with dipyridamole 50 mg b.i.d. for 4 days and then infused with epinephrine 4 pg/kg/min for 4 hr. The animals were sacrificed 7 days later and the histologic findings in their hearts were compared with the findings in ten dogs that had not been pretreated but had been subject to similar infu- sions. Myocardial necrosis was graded 0 to 3+ with 3t signifying diffuse confluent myocardial necro- sis, 2t, diffuse necrosis without confluence, and l+, a few small patches of isolated necrosis, Whereas all of the ten control animals were found to have necrosis, (eight with 2 or 3t) only three of each of the pretreated groups had any necrosis. None of the pretreated animals were found to have 3+ necrosis, three had It among the ani.mals pretreated with aspirin, and one each had trace (a few areas less than would be graded 1 t), It, and 2+ necrosis among the dipyridamole pretreated animals. Since aspirin and dipyridamole have little in common other than their platelet-inhibiting effects, the protection afforded by both of these drugs suggests that intravascular platelet aggrega- tion plays a significant role in the etiology of catecholamine-induced cardiac necrosis.r6

82
To further support the concept that platelet aggregates in the small vessels of the heart played a role in the myocardial damage induced by cate- cholamines, it was necessary to demonstrate the presence of such platelet plugs. Platelets are diffi- cult to identify using the light microscope because they frequently appear as amorphous debris, but can be readily recognized using the electron microscope. The hearts of six dogs sacrificed im- mediately after 4-hr infusions of norepinephrine 4 pg/kg/min were studied with the electronmicro- scope. All the animals were found to have platelet aggregates within the small vessels of their hearts.36 Intravascular platelets in all stages of aggregation were found. These ranged from a few platelets ad- herent to. each other, to platelet plugs completely occluding vessel lumina with platelets that had al- ready undergone viscous metamorphosis. In most of the vessels the endothelial surfaces appeared intact, suggesting that the platelet aggregation was primary, rather than secondary to vessel wall dam- age. In some of the vessels containing occlusive mature platelet plugs there were areas of vessel wall breakdown that suggested damage caused by the extruded lysosomal enzymes” from the plate- lets that had already undergone viscous meta- morphosis.
Electronmicroscopic studies of the hearts of 14 rats given 3 mg isoproterenol i.p. 1 hr prior to sacrifice revealed similar platelet aggregates within the small vessels of the myocardium.37 Platelets in all degrees of aggregation ranging from two and three platelets adherent to each other and to the vessel wall to platelet plugs completely occluding small vessels were found.
An intriguing aspect of the study of catechol- amine-induced cardiac necrosis has been the rela- tionship of endogenous catecholamine secretion during stress and cardiac damage. The cardiac lesions induced by various forms of stress in the adrenal corticoid-pretreated animal reported by Selyes 1 are similar to those caused by excess cate- cholamines. In studies by Raab et al.,52 adrenergic- blocking agents were found effective in preventing these stress lesions in corticoid-pretreated animals, suggesting that these stress lesions require an intact sympathetic adrenergic system for their produc- tion. If the thrombogenic effect of catecholamines secreted during stressful situations plays a role in the etiology of these lesions, this finding might be of etiologic importance in the relation of acute myocardial infarction to stress. To determine if
JACOB I. HAFT
Table 1. Stress Studies
Cold stress 16 rats 100% with intravascular
platelet aggregation
Hot water stress 8 rats 87.5% with intravascular
platelet aggregation
Shocking stress 15 rats 87.8% with intravascular
platelet aggregation
Controls 14 rats 7.3% with intravascular
platelet aggregation
endogenous catecholamines were able to induce intravascular platelet aggregates, studies on rats exposed to immersion in ice cold water,53 exposed to immersion in hot water,54 and who had received repeated painful shocks to their pawss4 were carried out. In all of these stress studies, platelet aggregates similar to those seen after exogenous catecholamine administration were found in most of the rats (Table 1).
There is a large literature correlating stress with acute myocardial infarction or sudden death.ssYs6 It has also been demonstrated that catecholamine secretion is enhanced during stressful situations.52 It is possible that the link between stress and these myocardial events may be via a platelet aggregate induced to form intravascularly by endogenously secreted catecholamines, and traveling to an area previously narrowed by atherosclerosis. Such an aggregate might totally occlude the vessel lumen and lead to either a myocardial infarction, or to the induction of a fatal ventricular arrhythmia. If this is the case, chronic treatment with drugs that inhibit platelet aggregation might be effective in preventing myocardial infarction and sudden death. There are currently a number of large scale studies underway to determine if aspirin, an active platelet aggregation-inhibiting drug, will have an effect on the prognosis in patients at risk for myocardial infarction.
DIRECT VASCULAR INJURY INDUCED BY CATECHOLAM INES
Very early in this century, attention was drawn to adrenalin as a possible etiologic agent for the development of arteriosclerosis. Josues in 1904 demonstrated that injections of adrenalin in rabbits would cause degenerative changes and scarring in the wall of the aorta. A large number of investiga- tors throughout the world confirmed these find- ings over the subsequent years9.59160 (this work was exhaustively reviewed by Heupe? in 1948). Although most investigators have agreed that

INJURY INDUCED BY SYMPATHETIC CATECHOLAMINES 83
adrenalin can affect the vessel wall and damage it, the relationship of these lesions to atherosclerosis remains in question.
Grossly,58-60 the early vascular lesion induced by adrenalin is a punctate or linear, depressed, grayish area in the ascending or thoracic aorta. With time, confluent, irregular, brittle pearly gray areas develop that at first are depressed but later begin to bulge slightly. Later the aortic wall in- volved in the lesion becomes thin and hard, similar to parchment, and aneurysmal dilatation of these lesions may develop. The aorta may eventually be completely involved with numerous areas of nod- ularity and sacular dilatation. The late plaques are hard, shiny, with brownish discoloration and are arranged in groups or in longitudinal lines. Dissect- ing aneurysms that originate in these plaques are seen not infrequently. Occasionally hemorrhagic necrosis in the vessel wall is also seen. Involvement of middle-sized vessels including the coronary arteries also occasionally occurs in animals with the late lesion in the aorta.’
Histologically, 58-60 the initial lesion is a focus of necrosis of the muscularis with atrophic degenera- tive changes and eventual necrosis occurring in the muscle cells. Calcium salts enter these necrotic areas early in their development and the medial layer of the vessel wall becomes calcified. The elastic lamellae become stretched out and com- pacted and eventually they degenerate with swell- ing, fragmentation, and clumping of the elastic fibers. Reactive inflammation with Iymphocytes and polymorphonuclears accumulation is seen. Giant cells are an inconstant finding, and occasion- ally granulation tissue develops. The intimal layer of the wall is usually not primarily involved but occasionally shows endothelial thickening and proliferation9 over the area of the medial lesion. In areas of sacculation of the wall, hyperpiasia, hyalinization, and fibrosis of the intimal layer may occur. The adventitia remains normal. In the smaller arteries, thickening with degenerating mus- cle cells are seen and occasionally perivascular cuff- ing with inflammatory cells occurs. The vasa vasorum of the larger vessels occasionally are found to have obliterative endothelial proliferation. It has been suggested that the lesions in the medial layer of large- and medium-sized vessels may be due to ischemia secondary to compromise of blood flow through the vasa vasorum.
These lesions caused by large doses of sym- pathetic catecholamines are quite different, how-
ever, from atherosclerosis as seen in humans,58a59 especially with respect to location, the early de- velopment of calcification, and the absence Iof fat. Whereas the location of atherosclerosis is primarily at the sites of branching of vessels and involves the smaller vessels very soon after the aorta is involved, adrenalin-induced lesions are diffuse, occur almost exclusively in the larger vessels, and only much later are smaller vessels involved. The intima is the layer most prominently affected in atherosclerosis with the media not involved in the early lesions, whereas adrenalin first and most prominently af- fects the muscularis. Lipid infiltration and prolifer- ation of the intima is an early event in athero- sclerosis; necrosis of the media is not seen, and calcification, rather than occurring early im the course, is a late manifestation, while calcification is early and prominent in adrenalin-induced lesions, and lipid infiltration is rarely seen. The hallmark of human atherosclerosis is the presence of yellow, fatty, cholesterol-containing plaques, whereas this is not seen in adrenalin-induced vascular sclerosis. The lesions produced by large dose adrenalin are more similar to those seen with Monckeberg’s sclerosis.
Although the lesions produced after ,large Idoses of adrenalin are quite different, lesions simil.ar to human atherosclerosis have been produced by repeated administration of small amounts of adren- alin Braun61 produced marked fibrous intimal thickening in the aorta, renal, pulmonary, and tibial arteries of rabbits by this technique, lesions that were quite reminiscent of early arterio- sclerosis. Similar lesions,58 but also containing cholesterol, have been found in patients dying with pheochromocytoma.
An interesting aspect of the re1ationshi.p of catecholamines and atherosclerosis has been noted by Anitschkow . 59 He found that the combination of adrenalin injection and cholesterol feeding en- hanced the production of atherosclerotic plaques in the experimental animal, although the location of the lesion was more typical of adrenalin sclerosis. He considered these changes to be sec- ondary atherosclerotic lesions; similar to the cho- lesterol infiltration occasionally seen in syphil- litic aortas and not related to primary atherosclerosis as usually seen in humans. It is likely that degenerative changes in the vessel wall induced by catecholamines predispose to the in- filtration of the wall by lipids.
The etiology of the vascular lesion induced by

84 JACOB I. HAFT
catecholamines remains unclear. It has been pro- posed that constriction of the vasa vasorum with resultant medial ischemia,s9 a direct toxic effect of adrenalins or the mechanical trauma to the vessel wall by the induced rise in blood pres- sure9ps9 may each be of etiologic importance.
Catecholamines may play an indirect role in the development of atherosclerosis. Epidemiologically, hypertension is found to be one of the major risk factors in the development of atherosclerotic cardiovascular disease. 62 Although, the relationship between catecholamines and hypertension, other than when a pheochromocytoma is present, is still not clear, there has been recent evidence presented that norepinephrine blood levels are elevated among patients with essential hypertension.63 Such a finding would help to explain the effectiveness of antihypertensive drugs that work by interfering with catecholamine action (e.g., alpha methyldopa, reserpine, and guanethidine). The relationship of hypertension to atherosclerosis is felt to be via enhancement of the ultrafiltration of plasma into vessel walls and by the increase in turbulence around areas of vessel branching.
Another action of catecholamines on the vessel wall that might indirectly lead to vessel wall damage is the relation of catecholamines to intra- vascular clotting. In the middle 18OOs, Rokitan- Sky64 suggested that arteriosclerotic plaques were the final result of degeneration of mural thrombi. This theory lay dormant until the 1940s when Duguid6sS66 demonstrated that mural thrombi be- come covered with endothelium and then de- generate, liquify, and are replaced by fatty debris and cholesterol crystals. He found lesions that suggested various phases of this progression.
In the late 1950s Woolf and &stair@’ studied atherosclerotic plaques by staining them with fluorescein-tagged antibodies to platelets. Deep within mature atherosclerotic lesions, these in- vestigators found material that reacted antigeni-
tally like platelets. Their work suggests that plaques may grow by the repeated formation of mural thrombi, endothelialization of the clot, and de- generation of the thrombi, with the process repeat- ing itself over and over again, until a large athero- sclerotic plaque is formed.
As noted previously, the relationship of clotting to catecholamines has been recognized since the work of Cannon in the early I~OOS.~’ A direct effect of adrenalin and noradrenalin on platelet aggregation has been well documented in vitro,41-43 and catecholamine-induced intravas- cular platelet aggregation in vivo has been demon- strated.36337 If the thrombogenic thesis for the production of atherosclerosis is valid, catechol- amines may affect the induction of atherosclerotic plaques by causing the formation of mural thrombi.
In addition, catecholamine-induced platelet ag- gregates that adhere to vessel walls may damage the endothelium during the release action that occurs as platelets undergo viscous metamorphosis. During this second, irreversible stage of platelet aggregation, the substances present within the platelet granules are released.46 In addition to the secretion of ADP, serotonin and sympathetic catecholamines that tend to perpetuate and prolif- erate the platelet aggregate, lysosomal enzymes are released. So These enzymes may damage the endothelial surface to make it more permeable to the ultrafiltration of lipids, and in such a manner the development of an atherosclerotic plaque may be initiated.69 If catecholamines are related to atherosclerosis by way of these thrombogenic ef- fects, the recent finding that emotional and physical stress, probably by way of endogenous catecholamines, can lead to intravascular platelet aggregates in the experimental anima137S53*54 may help to explain the epidemologic correlation that individuals who are driving, aggressive, and fre- quently exposed to stress are those who are prone to develop atherosclerosis.”
REFERENCES
1. Ziegler K: Uber die Wirkung intravenoser Adren- alminjektion auf das Gefasssystem und ihre Beziehung zur Arteriosklerose. Ziegler’s Beitrage 38:229-254, 1905
2. Pearce RM: Experimental myocarditis: A study of the histological changes folIowing intravenous injections of adrenalin. J Exp Med 8:400-409,1906
3. Josue 0: Hypertrophie cardiaque causee par l’adren- aline et la toxine typhique. Compt Rend Sot Biol (Paris) 63:285-286,1907
4. Fleisher MS, Loeb L: Experimental myocarditis. Arch Intern Med 3~78-91, 1909
5. Christian HA, Smith RM, Walker IC: Experimental cardiorenal disease. Arch Intern Med 8:468-551,191l
6. Anitschkow N: Ueber die Histogene der Myokard- veranderungen Bei Einigen Intoxikationen. Virchows Arch (Path01 Anat) 211:193-232,1913
7. Veith G: Experimentelle Untersuchungen zur Wirk- ung von Adrenalin auf den Herzmuskel. Arch Kreislauf- forsch 6:335-360,194O
8. Raab W: The pathogenic significance of adrenalin and related substances in the heart muscle. Exp Med Surg 1:188-225,1943
INJURY INDUCED BY SYMPATHETIC CATECHOLAMINES 85
9. Waters IL, de Suto-Nagy GI: Lesions of the coronary arteries and great vessels of the dog following the injection of adrenalin. Science 111: 634-635,195O
10. Viihnevskaya OP: Reflex mechanisms in the patho- genesis of adrenalin myocarditis. Biull Eksp Biol Med 41:307-310,1956
11. Nahas GG, Brunson JG, King WM, et al: Functional and morphologic changes in heart-lung preparations fol- lowing administration of adrenal hormones. Am J Path01 34:717-729,1958
12. Maling HM, Highman B: Exaggerated ventricular arrhythmias and myocardial fatty changes after large doses of norepinephrine and epinephrine jn unanesthetized dogs. Am J Physiol194:590-596, 1958
13. Chappel Cl, Rona G, Balazs T, et al: Comparison of cardiotoxic actions of certain sympathomimetic amines. Can J Biochem Physiol37:35-42,1959
14. Rosenblum I, Wohl A, Stein AA: Studies in cardiac necrosis. I. Production of cardiac lesions with sym- pathomimetic amines. Toxic01 Appl Pharmacol 7:1-8, 1965
15. Ferrans VJ, Hibbs RG, Walsh JJ, et al: Histo- chemical and electron microscopical studies on the cardiac necrosis produced by sympathomimetic agents. Ann NY Acad Sci 156:309-332,1969
16. Haft JI, Gershengorn K, Kranz PD, et al: Protection against epinephrine-induced myocardial necrosis by drugs that inhibit platelet aggregation. Am J Cardiol 30:838- 84%,1972
17. Szakacs JE, Cannon A: L-norepinephrine myo- carditis. Am J Clin Path01 30:425-434,1958
18. Szakacs JE, Mehlman B: Pathologic changesinduced by I-norepinephrine. Am J Cardiol5:619-627,196O
19. Maling HM, Highman B, Thompson EC: Some similar effects after large doses of catecholamines and myocardial infarction in dogs. Am J Cardiol 5:628-633, 1960
20. Schenk EA, Moss AJ: Cardiovascular effects of sus- tained norepinephrine infusions. II. Morphology. Circ Res 18:605-615,1966
21. Hoak JC, Warner ED, Connor WE: New concept of levarterenol-induced acute myocardial necrosis. Arch Path01 87:332-338, 1969
22. Van Vliet PD, Burchell HB, Titus JL: Focal myocarditis associated with pheochromocytoma. N Engl J Med 272:1102-1108,1966
23. Rona G, Chappel CI, Balazs T, et al: An infarct-like myocardial lesion and other toxic manifestations pro- duced by isoproterenol in the rat. Arch Path01 67:443, 1958
24. Handforth CP: Isoproterenol-induced myocardial infarction in animals. Arch Path01 73:161-165, 1962
25. Wexler BC, Kittinger GW: Myocardial necrosis in rats: Serum enzymes adrenal steroid and histopathological alterations. Circ Res 13:159-171, 1963
26. Rona G, Chappel CI, Kahn DS: The significance of factors modifying the development of isoproterenol- induced myocardial necrosis. Am Heart J 66:389-395, 1963
27. Ferrans VJ, Hibbs RG, Black WC, et al: Isopro- terenolinduced myocardial necrosis. A histochemical and electron microscopic study. Am Heart J 68:71-90, 1964
28. Ostadal B, Rychterova V, Poupa 0: Isoproterenol- induced acute experimental cardiac necrosis in the turtle (Testudo Horsfleldi). Am Heart J 76:645-649,1968
29. Wexler BC, Judd JT, Kittinger GW: Myocardial necrosis induced by isoproterenol in rats. Angiology 19:665-682,1968
30. Bloom S, Cancilla PA: Myocytolysis and mito- chondrial calcification in rat myocardium after low doses of isoproterenol. Am J Path01 54:373-391,1969
31. Csapo Z, Dusek J, Rona G: Early alterations of the cardiac muscle cells in isoproterenol-induced nelcrosis. Arch Path01 93:356-365,1972
32. Franz G: Eine seltene Form von toxischer Myo- cardschadigung. Virchows Arch (Path01 Anat) 298:743- 752,1937
33. Gormsen H: Om Dodelig Adrenalin Forgiftning. Ugeskrift For Iaeger 101:242-245,1939
34. Watkins DB: Pheochromocytoma: A review of the literature. J Chronic Dis 6:510-527,1957
35. Kline IK: Myocardial alterations associated with pheochromocytomas. Am J Path01 38:539-557,196l
36. Haft JI, Kranz PD, Albert FJ, et al: Intravascular platelet aggregation in the heart induced by nor- epinephrine. Circulation 46:698-7081972
37. Haft JI, Fani K, Alcorta C, et al: Effect of propanolol on stress-induced intravascular platelet ag- gregation in the heart. Circulation 48 (Suppl IV):57, 1973
38. Fleischer MS, Loeb L: Further investigations in experimental myocarditis. Arch Intern Med 6:427438, 1910
39. Cannon WB, Gray H: Factors affecting the coagula- tion time of blood. The hastening or retarding of coagula- tion by adrenalin injections. Am J Physiol 341232-242, 1914
40. Rowsell HC, Hegardt B, Downie HG, et al: A,dren- aline and experimental tluombosis. Br J Haematol 12: 66-73,1966
41. O’Brien JR: Variability in the aggregation of human platelets by adrenaline. Nature (Lond) 200:763-764, 1963
42. Mitchell JRA, Sharp AA: Platelet clumping in vitro. Br J Haematol 10:78-93, 1964
43. O’Brien JR: Variability in the aggregation of human platelets by adrenaline. Nature (Lond) 202: 1188-X 190, 1964
44. Jorgensen L, Rowsell HC, Hovig T, et al: Adenosine diphosphate-induced platelet aggregation and myocardial infarction in swine. Lab Invest i7:616-644,1967
45. MacMillan DC: Secondary clumping effect in human titrated platelet rich plasma produced by adermsine diphosphate and adrenaline. Nature (Lond) 211:140-144, 1966
46. Rodman NF, Mason RG, Brinkhous KM: Some pathogenetic mechanisms of white thrombus formation: Agglutination and self-destruction of the platelet. Fed Proc 22:1356-1365,1963
47. Hampton J: Trends in the development of anti- thrombotic agents. Am J Cardiol27:659-669,197l
48. Weiss HJ, Aledort LM, Kochwa S: The effect of salicylates on the hemostatic properties of platelets in man. J Clin Invest 47:2169-2180,196s
86 JACOB 1. HAFT
49. Emmons PR, Harrison MJG, Honour AJ, et al: Effect of dipyridamole on human platelet behaviour. Lancet 2:603-606,1965
50. Mills DCB, Robb IA, Roberts GK: The release of nucleotides, 5-hydroxytryptamine and enzymes from human blood platelets during aggregation. J Physiol (Lond) 195:715-729,1968
51. Selye H: The Chemical Prevention of Cardiac Necrosis. New York, Ronald Press, 1958
52. Raab W, Stark E, MacMillan WH, et al: Sym- pathogenic origin and anti-adrenergic prevention of stress- induced myocardial lesions. Am J Cardiol 8:203-211, 1961
53. Haft JI, Fani K: Intravascular platelet aggregation in the heart induced by stress. Circulation 47:353-358, 1973 .
54. Haft JI, Fani K: Stress and the induction of intravascular platelet aggregation in the heart. Circulation 48:164-169, 1973
55. Wolf S: Psychosocial forces in myocardial infarc- tion and sudden death. Circulation 49 (Supp IV):74-83, 1969
56. Engel GL: Sudden and rapid death during psycho- logical stress. Ann Intern Med 74:771-782,1969
57. Josue MO: Les lesions du tissu elastique des arteres dans l’atherome. Compt Rend Sot Biol 57:539- 541,1904
58. Hueper WC: Arteriosclerosis. Arch Path01 38:245- 285,1944
59. Anitschkow N: Experimental arteriosclerosis in ani- mals, in Cowdry EV (ed): Arteriosclerosis. New -York, MacMillan, 1933, pp 271-322
60. Friedman B, Oester YT, Davis OF: The effect of arterenol and epinephrine on experimental arteriopathy. Arch Int Pharmacodyn 102:226-234,1955
61. Braun L: Zur Frage der Arteriosklerose nach intravenoses adrenalinzufuhr. Munch Med Wochensclu 52:533,1905
62. Atherosclerosis Study Group: Primary prevention of the atherosclerotic diseases. Circulation 42:A. 55-95, 1970
63. Louis WJ, Doyle AE, Anavekar S: Plasma nor- epinephrine levels in essential hypertension. N EngI J Med 288:599-601,1973
64. Von Rokitansky CF: A Manual of PathologicaI Anatomy, ~014 (Day GE, Translator). London, Sydenham Society, 1852, pp 261-272
65. Duguid JB: Thrombosis as a factor in the patho- genesis of coronary atherosclerosis. J Path01 Bacterial 58:207-212,1946
66. Duguid JB: Pathogenesis of atherosclerosis. Iancet 2:925-927,1949
67. Woolf N, Carstairs JKC: Infiltration and thrombosis in atherogenesis. Am J Path01 51:373-378, 1967
68. Shimamoto T, Ishioka T: Release of a thrombo- plastic substance from arterial walls by epinephrine. Circ Res 12:138-144,1963
69. Mustard JF, Packham MA, Rowsell HC, et al: The role of thrombogenic factors in atherosclerosis. Ann NY Acad Sci 149:848-859,1968
70. Friedman M, Rosenman RH: Association of specific overt behavior pattern with blood and cardiovascular findings. JAMA 169:1286-1296,1959