-
8/12/2019 Cardiovascular Disease in Nonwestren Country
1/3
n engl j med 350;24
w ww.n ej m. org j un e 10, 2004
2438
P E R S P E C T I V E
Concern about increasing rates of death and dis-ability due to
cardiovascular disease in non-West-ern countries is often met with
skepticism: Do they really constitute a serious public health
problem?With justifiable alarm about the spread of
humanimmunodeficiency virus and AIDS and with old foessuch as
malaria and tuberculosis still posing for-midable challenges in
many developing countries,it is understandable that epidemics of
cardiovas-cular disease have insidiously established them-selves
without attracting global attention or localaction. The fact that
80 percent of deaths from car-diovascular disease worldwide and 87
percent of
related disability currently occur in low-income
andmiddle-income countries, however, indicates themagnitude of the
problem. Cardiovascular diseasehas become the leading cause of
death in many de- veloping countries and will soon attain that
statusin several others.
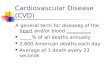
The high burden of mortality from cardiovas-cular causes in
developing countries (estimated at 9 million in 1990 and expected
to increase to 19 mil-lion by 2020
1
) is only partially explained by theirlarge populations (see
Figure 1). The projected in-crease in the proportion of all deaths
that are due tocardiovascular causes, from about 25 percent in1990
to more than 40 percent in 2020, signals theadvance of the
epidemics. China has witnessed adoubling of the number of deaths
attributed to cir-culatory diseases during the past two decades,
withthe most marked increase among persons 35 to54 years of age.
Over the past 40 years, the preva-lence of coronary heart disease
in urban India hasincreased by a factor of six to eight, to about
10 per-cent among persons 35 to 64 years of age. Stroke isnow the
dominant type of cardiovascular diseasein China, Southeast Asia,
and sub-Saharan Africa, whereas coronary heart disease predominates
inLatin America, the Middle East, and urban India. Asthe so-called
health transition in these countriesprogresses, hemorrhagic stroke
is being replacedby thrombotic stroke and coronary heart disease
asthe leading form of cardiovascular disease.
In non-Western countries, deaths due to cardio- vascular disease
tend to occur a decade or two ear-
lier than they do in Western countries; nearly half occur before
70 years of age, whereas only one fifthoccur so early in the West a
difference attribut-able to both the earlier occurrence of
cardiovas-cular events and the lower level of clinical
careavailable.
2
The rate of death due to stroke amongpersons 15 to 59 years of
age is three to eight timesas high in Tanzania as in England and
Wales. Deathand disability occurring in midlife have
disastrousconsequences for families who lose wage earners,and the
resulting loss in productivity adversely af-fects national
development. Of the 24 million peo-ple expected to die of
cardiovascular disease in
2020, about 9.3 million will be between 30 and 69 years of age;
most of them will be in non-Westerncountries.
These epidemics are driven by social and eco-nomic changes that
have profound effects on livinghabits. Although sharp shifts in
demographic pat-terns and lifestyle have resulted from
urbanizationand industrialization, the globalization that
consti-tuted the tailwind of the 20th century propelled de-
veloping countries into the worldwide epidemicof cardiovascular
disease. The change reflects botha demographic shift toward
increasing life expect-ancy and a shift in nutrition: people who
live long-er have greater exposure to cardiovascular risk factors,
and Westernized diets and patterns of phys-ical inactivity result
in elevations in blood pressure,body weight, blood sugar levels,
and lipid concen-trations. A huge increase in the prevalence of
dia-betes will further increase the burden of cardiovas-cular
disease; India, where nearly 20 million peoplehad diabetes in 1995,
will see at least a tripling of that number by 2025. Moreover, the
global expan-sion of the tobacco trade has led to large increasesin
the rate of smoking.
The levels of these risk factors have increasedsteeply in most
non-Western countries over the past two decades. Although there are
some differencesamong ethnic groups in the interactions
betweengenes and the environment, the available evidenceindicates
that the main risk factors for cardiovas-cular disease are relevant
to all populations and that most of the risk is environmentally
determined.
Cardiovascular Disease in Non-Western CountriesK. Srinath Reddy,
D.M.
Cardiovascular Disease in Non-Western Countries
-
8/12/2019 Cardiovascular Disease in Nonwestren Country
2/3
n engl j med 350;24
w ww.n ej m. org j un e 10, 2004
2439
P E R S P E C T I V E
Thus, these trends portend an explosion of athero-thrombotic
cardiovascular diseases in developingcountries. Given the rate at
which the distributionsof body-mass index and blood cholesterol
levelshave changed in the Chinese population (see Fig-ure 2),
possibly in association with a sharp increase
in fat consumption, it is clear that countries likeChina will
see a rapid escalation of the rate of coro-nary heart disease.
The epidemics of cardiovascular disease struck the more affluent
sections of developing countriesfirst, but as the epidemics mature,
the social gradi-ent is reversing, with socioeconomically
disadvan-taged groups becoming increasingly vulnerable.The poor and
the less educated everywhere now use tobacco with greater frequency
than the richand the better educated do. In Brazil, women in
low-er-income groups have had increasing rates of over- weight and
obesity since 1989, in contrast to the sig-
nificant decrease observed in high-income groups.Studies
conducted in Indian cities in the past dec-ade have shown that the
poor have a higher risk of heart attack than the rich. The poor
also have lessaccess to health care; their risk factors are not
rec-ognized in a timely fashion; and they often do not receive
effective treatment, since public health careis generally
restricted to the treatment of infectiousdiseases. Neglect of the
epidemics of cardiovascu-lar disease will heap greater injustice on
the poor-est of countries and the poorest of people.
Although these developments mirror in many ways the path of the
epidemics of cardiovasculardisease in Western countries, there are
important differences. Whereas the epidemics in the West flowed and
ebbed over the course of a century, thehealth transition in
developing countries has beencompressed into a few decades.
Urbanization isoccurring in places with uncorrected poverty
andincreasing disparities in income, causing the poorto be
especially vulnerable, while resource-con-strained national health
systems are ill equippedto cope with the double burden of
infectious andchronic diseases. Globalization accelerates
thechange, as Western products and models of behav-ior are
increasingly exported to non-Western coun-tries. However,
globalization also offers opportu-nities to facilitate the
prevention of cardiovasculardisease, through the application of
knowledgegenerated in Western countries: the understand-ing of risk
factors, evidence regarding effective in-terventions, tools and
technology for reducing risk,
and new models of healthy behavior that can be
promoted through the mass media. Thus, there isan opportunity to
alter the pattern of health transi-tion in developing countries by
implementing ef-fective measures for prevention and control
beforethe epidemics peak ideally, permitting a rapidshift to a
state in which cardiovascular events oc-cur only or primarily after
70 years of age.
A concerted public health response must inte-grate
population-based prevention strategies andcost-effective clinical
care, since the health systemsof developing countries can ill
afford the demandsof technology-intensive treatments. The
popula-tion approach is more rewarding and sustainablein the medium
and long term, since even small re-ductions in each risk factor can
add up to huge re-ductions in the rate of cardiovascular events.
And if healthy behavior is established as a desirable normin a
society, it can have a multigenerational effect.
There are differences of opinion, however, re-garding whether
population-level interventionsshould rely principally on behavioral
change gov-erned by the personal choices of well-informedpeople or
should operate through policy interven-tions that modify behavior
through social andeconomic determinants. Western countries
gen-erally favor the personal-choice approach, but thisapproach
assumes that healthy choices are widely available and affordable
and that it is easy to edu-cate consumers about the merits and
demerits of each option. The North Karelia project in
Finlandprovides a successful model of behavioral changethrough
community health education combined
Cardiovascular Disease in Non-Western Countries
Figure 1. Deaths from Cardiovascular Causes,Worldwide, in 1990
and Estimated for 2020.
Data are from Murray and Lopez.
1
M i l l i o n s o
f D e a
t h s
f r o m
C a r
d i o v a s c u
l a r
C a u s e s
30
10
20
25
5
15
01990 2020
5
9
6
19
Non-Western (developing)countries
Western countries
-
8/12/2019 Cardiovascular Disease in Nonwestren Country
3/3
n engl j med 350;24
w ww.n ej m. org j un e 10, 2004
2440
P E R S P E C T I V E
with industry-level interventions for providinghealthful food
choices. Such programs, however,may be less effective in
non-Western societies, wherepersonal choice is limited by lack of
awarenessand highly restricted options.
Policy-level interventions have proved effec-
tive in bringing about population-wide behavioralchange and risk
reduction even in the short term. InMauritius, governmental action
to substitute soy-bean oil for palm oil as the subsidized, rationed
oilresulted in a remarkable reduction in cholesterollevels. Changes
in economic policy that increasedthe availability of fresh fruits
and vegetables andhelped to substitute vegetable fats for animal
fatsled to a sharp decline in mortality from cardiovas-cular causes
in Poland. Non-Western countries must implement policies that will
help to reduce the con-sumption of tobacco, salt, and unhealthful
fatsand increase the consumption of fruits and vege-
tables, through production and pricing mecha-nisms that increase
options and influence consum-er choice. But policy interventions
will have limitedsuccess if the community is unwilling to accept
them. Hence, the top-down approach of enablinglegislation and
regulation must be complementedby a bottom-up approach of community
mobiliza-tion through health education. Measures taken inWestern
countries to protect nonsmokers from ex-posure to environmental
tobacco smoke illustratesuch a combined approach.
At the same time, people with a high risk of car-diovascular
disease or clinical manifestations of disease need protection from
premature death andprolonged disability. Evidence-based,
context-spe-cific, and resource-sensitive interventions must
becost-effectively integrated into all levels of healthcare, to
strengthen both primary and secondary prevention of cardiovascular
disease. The exten-sive use of aspirin in primary care settings for
thetreatment of suspected myocardial infarction cansave millions of
lives at low cost (about $3 per lifesaved, in India).
Blood-pressurelowering thera-pies reduce overall cardiovascular
risk and have asubstantial effect on mortality from coronary heart
disease and stroke, and smoking cessation effec-tively reduces
cardiovascular risk. Operational re-search is required to ensure
the effective integration
of such therapies and community-based preven-tive strategies
into the health care systems of non-Western countries. The
Initiative for Cardiovascu-lar Health Research in the Developing
Countries isa multi-institutional, international program that works
to stimulate, support, and strengthen suchresearch.
Epidemics of cardiovascular disease in non-Western countries
present complex challenges but also great opportunities. Seldom in
the history of human health have we been endowed with suchforesight
about our destiny and forearmed withsuch power to change it. It is
a challenge to humanintellect and enterprise to apply our knowledge
cre-atively and cost-effectively to minimize the burdenof
cardiovascular disease throughout the world.
From the All India Institute of Medical Sciences, New Delhi.
1.
Murray CJL, Lopez AD. The global burden of disease: a
com-prehensive assessment of mortality and disability from
diseases,injuries, and risk factors in 1990 and projected to 2020.
Cam-bridge, Mass.: Harvard University Press, 1996.
2.
Reddy KS. Cardiovascular diseases in the developing coun-tries:
dimensions, determinants, dynamics and directions forpublic health
action. Public Health Nutr 2002;5:231-7.
3.
The world health report 2002: reducing risks, promotinghealthy
life. Geneva: World Health Organization, 2002.
Cardiovascular Disease in Non-Western Countries
Figure 2. Trends in Mean Total Cholesterol Levelsamong Persons
25 to 64 Years of Age in Beijing, China.
Data are from the Monitoring Cardiovascular Disease(MONICA)
study of the World Health Organization.
3
To convert values for cholesterol to milligrams per decili-ter,
divide by 0.02586.
M e a n
T o t a l
C h o l e s t e r o l
C o n c e n
t r a t
i o n
( m m o l
/ l i t e r
)
5.0
4.6
4.84.9
4.5
4.7
4.34.24.14.0
4.4
0
Women
Men
1984 1988 1993 1996 1999















![Cardiovascular disease [autosaved]](https://img.pdfslide.us/doc/110x75/554b2ab7b4c905d3088b4ab0/cardiovascular-disease-autosaved.jpg)