Embed Size (px)
Citation preview
Respiratory Medicine (2012) 106, 249e256
ava i lab le at www.sc iencedi rec t .com
journa l homepage: www.e lsev ier .com/ locate / rmed
Cardiovascular disease in asthma and COPD:A population-based retrospective cross-sectionalstudy
Mario Cazzola a,b,*, Luigino Calzetta a,b, Germano Bettoncelli c,Claudio Cricelli c, Francesco Romeo a, Maria Gabriella Matera d,Paola Rogliani a
aDepartment of Internal Medicine, University of Rome Tor Vergata, Rome, ItalybDepartment of Pulmonary Rehabilitation, IRCCS, San Raffaele Pisana Hospital, Rome, ItalycHealth Search Institute, Italian College of General Practitioners, Florence, ItalydDepartment of Experimental Medicine, Second University, Naples, Italy
Received 7 March 2011; accepted 27 July 2011
KEYWORDSAsthma;COPD;Cardiovascular disease;Population-basedretrospective cross-sectional study
* Corresponding author. Cattedra dipellier 1, IT 00133 Roma, Italy. Tel.: þ
E-mail address: mario.cazzola@un
0954-6111/$ - see front matter ª 201doi:10.1016/j.rmed.2011.07.021
Summary
We conducted a large population-based retrospective cross-sectional study for determining theextent of clinically recognized chronic obstructive pulmonary disease (COPD) and asthma, andthe prevalence of associated cardiovascular diseases (CVDs), using information obtained fromthe Health Search Database (HSD) owned by the Italian College of General Practitioners (SIMG).Our study provides further evidence that patients with the diagnosis of COPD are at increasedassociation with the diagnosis of most CVDs. It also documents that age clusters between 35and 54 years are those at highest association of simultaneous presence of the diagnosis ofCVD and that of COPD, with a progressive significant reduction in older age clusters. Moreover,it shows that the diagnosis of asthma is modestly associated with the diagnosis of different CVmorbidities.ª 2011 Elsevier Ltd. All rights reserved.
Malattie Respiratorie, Dipartimento di Medicina Interna, Universita di Roma Tor Vergata, Via Mont-39 348 6412311; fax: þ39 06 72596621.
iroma2.it (M. Cazzola).
1 Elsevier Ltd. All rights reserved.

250 M. Cazzola et al.
Introduction
Chronic obstructive pulmonary disease (COPD) and asthmaare conditions associated with many comorbidities at thetime of diagnosis.1e5 In particular, there is solid evidencethat patients with COPD are at increased risk of cardio-vascular disease (CVD),3,6e8 whereas the link betweenasthma and CVD seems to be less strong,5,9e11 and someresearchers deny the existence of this link.12,13
In the current study, we determined the extent of clin-ically recognized COPD and asthma, and the prevalence ofassociated CVDs using information obtained from the HealthSearch Database (HSD) owned by the Societa Italiana MediciGenerici (SIMG), the Italian College of General Practi-tioners, which stores information on about 1.5% of the totalItalian population served by general practitioners (GPs).
Patients and methods
Collection of information
We conducted a population-based retrospective cross-sectional study using information obtained from the HSD.Primary-care data were obtained from the HSD of SIMG.Established in 1998 with the primary aim to carry outobservational studies on the incidence and prevalence ofchronic diseases and with the input of GPs who accept toparticipate on a voluntary basis, the HSD contains infor-mation provided by more than 650 GPs from all Italianregions. It included a total of 909,638 individuals (429,962men and 479,676 women) aged >14 years and registered inthe HSD at the end of December 2009.14
After intensive training, all participating GPs had to usespecially designed software to record data during theirnormal daily clinical practice (Millewin). The softwaresystem codes all the diagnostic records by using the Clas-sification of Diseases, Ninth Revision, Clinical Modification(ICD-9-CM).15 Prescription records are also coded accordingto the anatomical therapeutic chemical (ATC) classificationsystem. Data are recorded in the HSD with the consent ofthe patient, lawfully stored, managed according to privacyrules and can be used for scientific studies without anyfurther authorization from an ethics committee.
It is well known that before using any data resource,particularly one that is based on computer records, it isnecessary to determine the quality and completeness ofthe available information. Therefore, data are subject toa range of quality checks. Any variations within agreedranges are investigated and submitted to each participatingGP. Physicians who fail to meet standard quality criteria arenot considered for epidemiological studies.16
We must highlight that comparative analyses havedemonstrated the validity of the information gathered inthe HSD.17
Ascertainment of COPD, asthma and comorbidities
Cases of COPD were identified on the basis of the ICD-9codes 491, 492, and 496, and those of asthma on the basisof the ICD-9 code 493. The number of patients classified on
the basis of the ICD-9 code 493.2 was really small and forthis reason we have not considered it separately also foravoiding a statistical bias. Unfortunately we have notinformation related to temporality in HSD.
Always using the ICD-9 codes, we regarded as cardio-vascular comorbidities cases of hypertensive disease(401e405), ischemic heart disease (410e414), diseases ofpulmonary circulation (415e417), other forms of heartdisease (420e429), cardiac arrhythmia (427), heart failure(428), cerebrovascular diseases (430e438).
Analysis
The study was carried out by a cross-sectional and obser-vational field method. It permitted to describe the situationat the time of data collection, at the end of December2009, and it allowed determining the prevalence of inves-tigated outcomes. The studied population was divided byseveral clusters: age (35e44, 45e54, 55e64, 65e74, 75e84and older than 85 years old), gender (male and female),and comorbidities.
We evaluated the odds ratio (OR) that was choseninstead of relative risk (RR) because asthma and COPD havea prevalence that is less than 10%.18,19 Positive and nega-tive OR values mean a co-relative positive and negativeassociation between evaluated variables. Data wereadjusted for sex and age by Mantel-Haenszel method, thatpermits a precision-based estimates of the OR. Further-more, if the prevalence of comorbidities were more than10%, and the OR was more than 2.5 or less than 0.5,correction of the OR was carried out.18,19 In order tocalculate statistical and epidemiological values, computersoftware GraphPad Prism (CA, USA), SPSS (Chicago, IL, USA)and OpenEpi (Dean AG, Sullivan KM, Soe MM. Open SourceEpidemiologic Statistics for Public Health) were used.
Results
We excluded the age cluster 15e34 years because in thispopulation the risk of COPD was not relevant.14 We iden-tified a population of 690,489 individuals aged >34 yearsand registered in the HSD at the end of December 2009.There were 39,741 (5.76% of the entire population) indi-viduals suffering from asthma and 25,281 (3.66% of theentire population) patients with a diagnosis of COPD. Theprevalence of asthma was greater in women than in menwith a men/women ratio of 0.71, whereas the prevalenceof COPD was greater in men than in women with a men/women ratio of 1.64, and increased with age in both menand women.
Association between asthma, COPD and CVmorbidities
Table 1 shows the demographic characteristics of the studypopulation by age distribution, asthma, COPD and CVmorbidities. All individuals that were not identified on thebasis of the ICD-9 code 493 were considered “non-asth-matics”, whereas all subjects that were not identified onthe basis of the ICD-9 codes 491, 492, and 496 wereconsidered “non-COPD patients”.
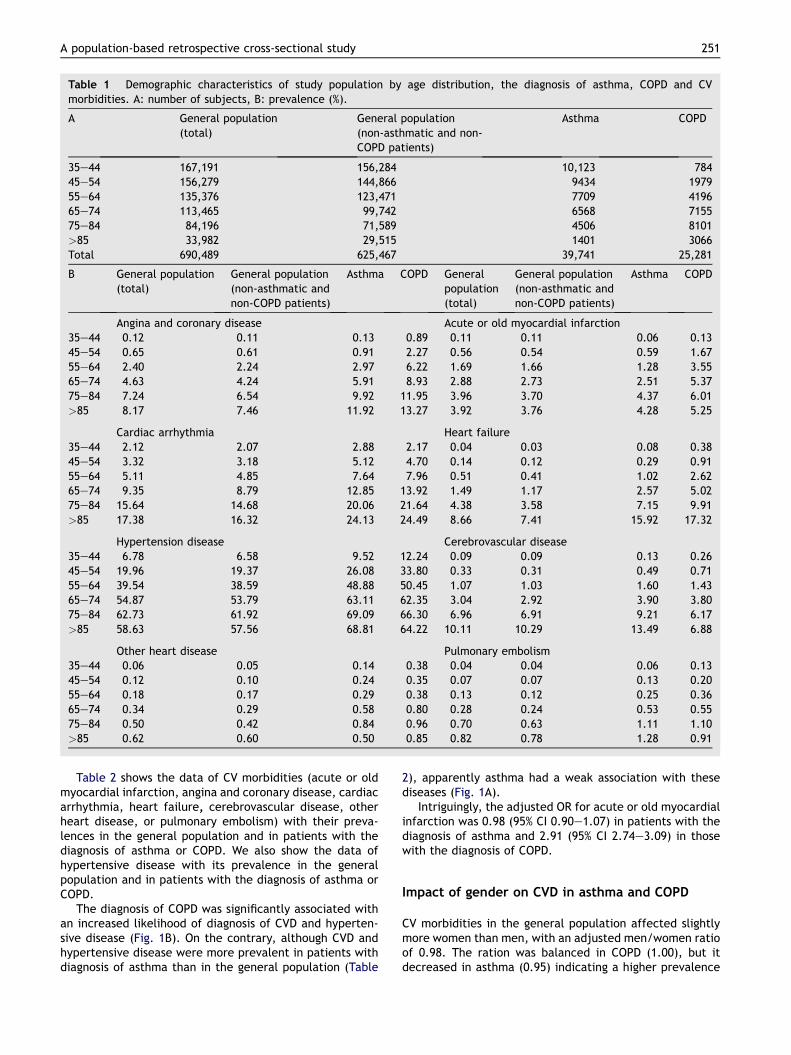
Table 1 Demographic characteristics of study population by age distribution, the diagnosis of asthma, COPD and CVmorbidities. A: number of subjects, B: prevalence (%).
A General population(total)
General population(non-asthmatic and non-COPD patients)
Asthma COPD
35e44 167,191 156,284 10,123 78445e54 156,279 144,866 9434 197955e64 135,376 123,471 7709 419665e74 113,465 99,742 6568 715575e84 84,196 71,589 4506 8101>85 33,982 29,515 1401 3066Total 690,489 625,467 39,741 25,281
B General population(total)
General population(non-asthmatic andnon-COPD patients)
Asthma COPD Generalpopulation(total)
General population(non-asthmatic andnon-COPD patients)
Asthma COPD
Angina and coronary disease Acute or old myocardial infarction35e44 0.12 0.11 0.13 0.89 0.11 0.11 0.06 0.1345e54 0.65 0.61 0.91 2.27 0.56 0.54 0.59 1.6755e64 2.40 2.24 2.97 6.22 1.69 1.66 1.28 3.5565e74 4.63 4.24 5.91 8.93 2.88 2.73 2.51 5.3775e84 7.24 6.54 9.92 11.95 3.96 3.70 4.37 6.01>85 8.17 7.46 11.92 13.27 3.92 3.76 4.28 5.25
Cardiac arrhythmia Heart failure35e44 2.12 2.07 2.88 2.17 0.04 0.03 0.08 0.3845e54 3.32 3.18 5.12 4.70 0.14 0.12 0.29 0.9155e64 5.11 4.85 7.64 7.96 0.51 0.41 1.02 2.6265e74 9.35 8.79 12.85 13.92 1.49 1.17 2.57 5.0275e84 15.64 14.68 20.06 21.64 4.38 3.58 7.15 9.91>85 17.38 16.32 24.13 24.49 8.66 7.41 15.92 17.32
Hypertension disease Cerebrovascular disease35e44 6.78 6.58 9.52 12.24 0.09 0.09 0.13 0.2645e54 19.96 19.37 26.08 33.80 0.33 0.31 0.49 0.7155e64 39.54 38.59 48.88 50.45 1.07 1.03 1.60 1.4365e74 54.87 53.79 63.11 62.35 3.04 2.92 3.90 3.8075e84 62.73 61.92 69.09 66.30 6.96 6.91 9.21 6.17>85 58.63 57.56 68.81 64.22 10.11 10.29 13.49 6.88
Other heart disease Pulmonary embolism35e44 0.06 0.05 0.14 0.38 0.04 0.04 0.06 0.1345e54 0.12 0.10 0.24 0.35 0.07 0.07 0.13 0.2055e64 0.18 0.17 0.29 0.38 0.13 0.12 0.25 0.3665e74 0.34 0.29 0.58 0.80 0.28 0.24 0.53 0.5575e84 0.50 0.42 0.84 0.96 0.70 0.63 1.11 1.10>85 0.62 0.60 0.50 0.85 0.82 0.78 1.28 0.91
A population-based retrospective cross-sectional study 251
Table 2 shows the data of CV morbidities (acute or oldmyocardial infarction, angina and coronary disease, cardiacarrhythmia, heart failure, cerebrovascular disease, otherheart disease, or pulmonary embolism) with their preva-lences in the general population and in patients with thediagnosis of asthma or COPD. We also show the data ofhypertensive disease with its prevalence in the generalpopulation and in patients with the diagnosis of asthma orCOPD.
The diagnosis of COPD was significantly associated withan increased likelihood of diagnosis of CVD and hyperten-sive disease (Fig. 1B). On the contrary, although CVD andhypertensive disease were more prevalent in patients withdiagnosis of asthma than in the general population (Table
2), apparently asthma had a weak association with thesediseases (Fig. 1A).
Intriguingly, the adjusted OR for acute or old myocardialinfarction was 0.98 (95% CI 0.90e1.07) in patients with thediagnosis of asthma and 2.91 (95% CI 2.74e3.09) in thosewith the diagnosis of COPD.
Impact of gender on CVD in asthma and COPD
CV morbidities in the general population affected slightlymore women than men, with an adjusted men/women ratioof 0.98. The ration was balanced in COPD (1.00), but itdecreased in asthma (0.95) indicating a higher prevalence
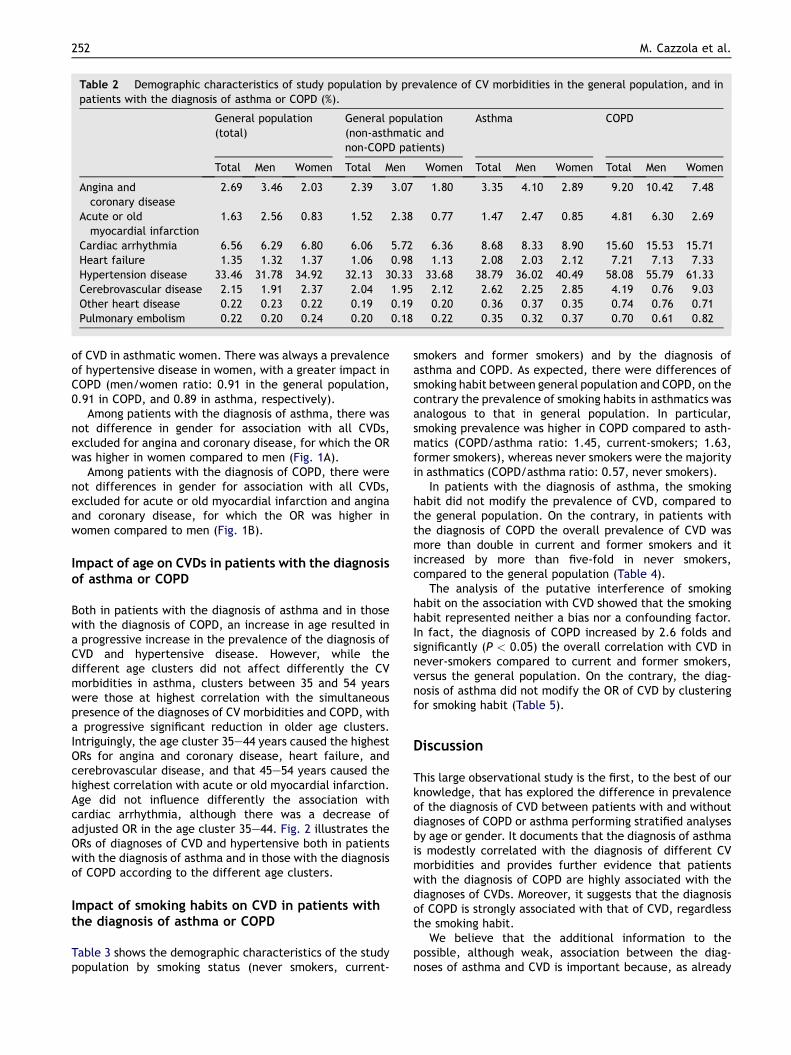
Table 2 Demographic characteristics of study population by prevalence of CV morbidities in the general population, and inpatients with the diagnosis of asthma or COPD (%).
General population(total)
General population(non-asthmatic andnon-COPD patients)
Asthma COPD
Total Men Women Total Men Women Total Men Women Total Men Women
Angina andcoronary disease
2.69 3.46 2.03 2.39 3.07 1.80 3.35 4.10 2.89 9.20 10.42 7.48
Acute or oldmyocardial infarction
1.63 2.56 0.83 1.52 2.38 0.77 1.47 2.47 0.85 4.81 6.30 2.69
Cardiac arrhythmia 6.56 6.29 6.80 6.06 5.72 6.36 8.68 8.33 8.90 15.60 15.53 15.71Heart failure 1.35 1.32 1.37 1.06 0.98 1.13 2.08 2.03 2.12 7.21 7.13 7.33Hypertension disease 33.46 31.78 34.92 32.13 30.33 33.68 38.79 36.02 40.49 58.08 55.79 61.33Cerebrovascular disease 2.15 1.91 2.37 2.04 1.95 2.12 2.62 2.25 2.85 4.19 0.76 9.03Other heart disease 0.22 0.23 0.22 0.19 0.19 0.20 0.36 0.37 0.35 0.74 0.76 0.71Pulmonary embolism 0.22 0.20 0.24 0.20 0.18 0.22 0.35 0.32 0.37 0.70 0.61 0.82
252 M. Cazzola et al.
of CVD in asthmatic women. There was always a prevalenceof hypertensive disease in women, with a greater impact inCOPD (men/women ratio: 0.91 in the general population,0.91 in COPD, and 0.89 in asthma, respectively).
Among patients with the diagnosis of asthma, there wasnot difference in gender for association with all CVDs,excluded for angina and coronary disease, for which the ORwas higher in women compared to men (Fig. 1A).
Among patients with the diagnosis of COPD, there werenot differences in gender for association with all CVDs,excluded for acute or old myocardial infarction and anginaand coronary disease, for which the OR was higher inwomen compared to men (Fig. 1B).
Impact of age on CVDs in patients with the diagnosisof asthma or COPD
Both in patients with the diagnosis of asthma and in thosewith the diagnosis of COPD, an increase in age resulted ina progressive increase in the prevalence of the diagnosis ofCVD and hypertensive disease. However, while thedifferent age clusters did not affect differently the CVmorbidities in asthma, clusters between 35 and 54 yearswere those at highest correlation with the simultaneouspresence of the diagnoses of CV morbidities and COPD, witha progressive significant reduction in older age clusters.Intriguingly, the age cluster 35e44 years caused the highestORs for angina and coronary disease, heart failure, andcerebrovascular disease, and that 45e54 years caused thehighest correlation with acute or old myocardial infarction.Age did not influence differently the association withcardiac arrhythmia, although there was a decrease ofadjusted OR in the age cluster 35e44. Fig. 2 illustrates theORs of diagnoses of CVD and hypertensive both in patientswith the diagnosis of asthma and in those with the diagnosisof COPD according to the different age clusters.
Impact of smoking habits on CVD in patients withthe diagnosis of asthma or COPD
Table 3 shows the demographic characteristics of the studypopulation by smoking status (never smokers, current-
smokers and former smokers) and by the diagnosis ofasthma and COPD. As expected, there were differences ofsmoking habit between general population and COPD, on thecontrary the prevalence of smoking habits in asthmatics wasanalogous to that in general population. In particular,smoking prevalence was higher in COPD compared to asth-matics (COPD/asthma ratio: 1.45, current-smokers; 1.63,former smokers), whereas never smokers were the majorityin asthmatics (COPD/asthma ratio: 0.57, never smokers).
In patients with the diagnosis of asthma, the smokinghabit did not modify the prevalence of CVD, compared tothe general population. On the contrary, in patients withthe diagnosis of COPD the overall prevalence of CVD wasmore than double in current and former smokers and itincreased by more than five-fold in never smokers,compared to the general population (Table 4).
The analysis of the putative interference of smokinghabit on the association with CVD showed that the smokinghabit represented neither a bias nor a confounding factor.In fact, the diagnosis of COPD increased by 2.6 folds andsignificantly (P < 0.05) the overall correlation with CVD innever-smokers compared to current and former smokers,versus the general population. On the contrary, the diag-nosis of asthma did not modify the OR of CVD by clusteringfor smoking habit (Table 5).
Discussion
This large observational study is the first, to the best of ourknowledge, that has explored the difference in prevalenceof the diagnosis of CVD between patients with and withoutdiagnoses of COPD or asthma performing stratified analysesby age or gender. It documents that the diagnosis of asthmais modestly correlated with the diagnosis of different CVmorbidities and provides further evidence that patientswith the diagnosis of COPD are highly associated with thediagnoses of CVDs. Moreover, it suggests that the diagnosisof COPD is strongly associated with that of CVD, regardlessthe smoking habit.
We believe that the additional information to thepossible, although weak, association between the diag-noses of asthma and CVD is important because, as already
Figure 1 Adjusted odds ratios and 95% confidence limits ofCV morbidities in patients with the diagnosis of asthma (A) andCOPD (B). "Total” adjusted for age and sex, “Men” and“Women” adjusted for age. p < 0.05 vs non-asthmatic (A) andvs non-COPD (B) population.
A population-based retrospective cross-sectional study 253
mentioned, literature on this topic is conflicting.5,8e13 Ourdata confirm a higher prevalence of the diagnosis of CVD inwomen with that of asthma, show that, at least in men, thediagnosis of asthma is associated with diagnosis of anginaand coronary disease but not with that of acute or oldmyocardial infarction, and do not confirm the reportedassociation between the diagnoses of asthma and cere-brovascular disease.13 We must admit that we are unable toexplain why there was an association of the diagnosis ofasthma with that of angina and coronary disease but notwith that of myocardial infarction in men, although theprevalence of the diagnosis of angina and coronary diseaseand that of myocardial infarction in asthmatic men weresimilar to those in men in the non-asthmatic population. Itis likely that the low number of events could have gener-ated information that larger numbers could deny, althoughagain we must emphasize the breadth of our sample. In any
case, we cannot exclude that the observed increased ORsfor the diagnoses of cardiac arrhythmia and heart failure,as well as other heart diseases, may suggest that theconsequences of those diseases on the lung could havebeen confounded with asthma. However, we must stressthat we have only considered comorbidities that werepresent in the same patient simultaneously with the diag-nosis of asthma.
Another finding that is difficult to explain is the impactof gender in the association between the diagnoses ofasthma or COPD and CVD. Several reports suggest a role forfemale sex hormones in promoting the asthmatic pheno-type.20 On the other hand, female smokers appear to bemore susceptible than male smokers to developing COPD.Women have a more vigorous inflammatory reaction andgenerate more oxidative stress in the airways than men21
likely because estrogens could cause an imbalance in theformation and removal of toxic intermediates of cigarettesmoke components.22 All this would suggest a strongerassociation between the diagnoses of asthma or COPD andCVD in women, but often our data did not confirm it.
Soriano and colleagues1 suggested that the occurrenceof CVD events in their study was generally lower in asthmapatients compared to COPD patients likely because of theyounger age distribution. Also in our population the diag-nosis of asthma was prevalent in younger people and thiscould indicate that the age is the main association factor ofCVD in asthma or COPD. However, although an increase inage resulted in a progressive increase in the prevalence ofthe diagnoses of CVD and hypertensive disease both in thediagnoses of asthma and COPD, the various age clusters didnot affect differently the association of the diagnosis of CVmorbidities with that of asthma, whereas cluster 35�44years was that at highest correlation with the simultaneouspresence of CV morbidities and COPD, with a progressivesignificant reduction in older age clusters. Also Feary andcolleagues found that the association between diagnoses ofCOPD and CVD was strongest in the younger age groups,persisted across all ages but reduced as age increased.23
It is also difficult to explain the higher association of thediagnosis of CVDs with the diagnosis of COPD among youngerthan older patients that we have found in our study. It hasbeen suggested that it may be mediated by the use ofinhaled bronchodilators24 because these agents were shownto impose a larger relative risk in people with unrecognizedCVD than in people with known disorders.25 We do notagree with this hypothesis because our data show thatthe adjusted ORs of cardiac arrhythmia, a common sideeffect of bronchodilators, were almost constant in all ageclusters.
We believe that our results are interesting because theycome from a large, validated, population-based databasethat illustrates what can be observed in real life and can beconsidered representative of the general population. This isthe major strength of the present study. Moreover, use ofroutine medical records should have eliminated differentialmisclassification due to recall or interviewer bias.
The main limitations of our study are common to retro-spective database analyses. These limitations might beassociated mainly with bias towards the selection of morehighly motivated, or better organized, practices. Conse-quently, our findings might likely be an overestimate of the
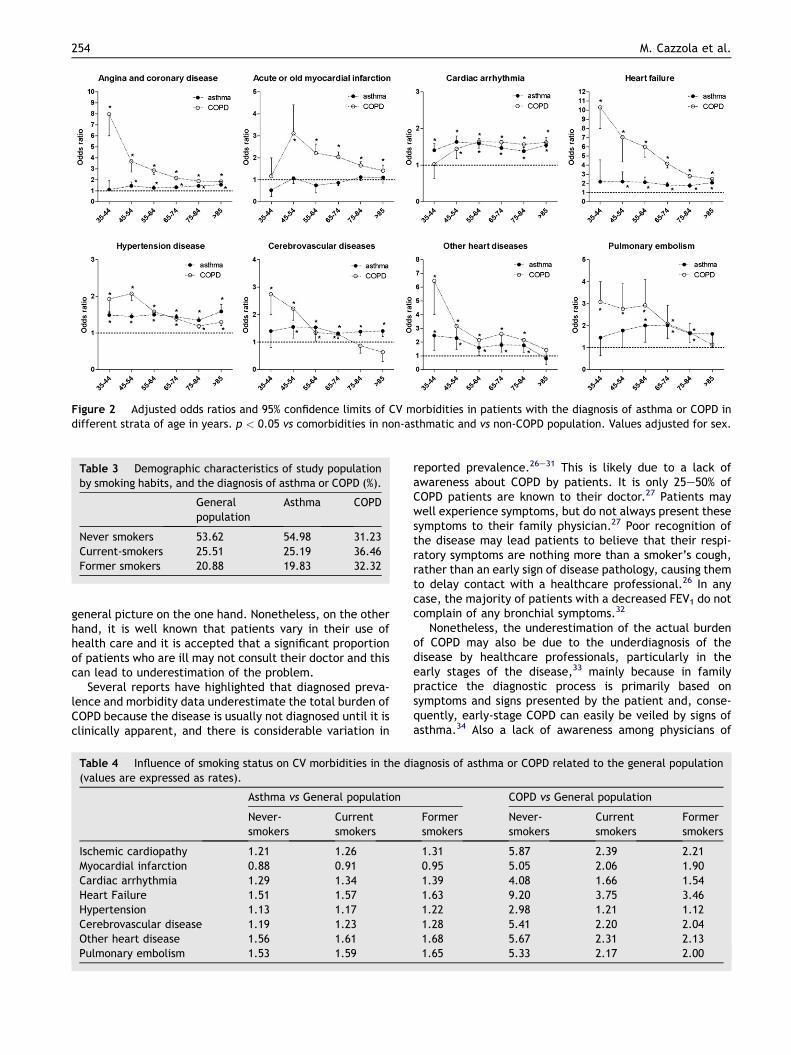
Figure 2 Adjusted odds ratios and 95% confidence limits of CV morbidities in patients with the diagnosis of asthma or COPD indifferent strata of age in years. p < 0.05 vs comorbidities in non-asthmatic and vs non-COPD population. Values adjusted for sex.
Table 3 Demographic characteristics of study populationby smoking habits, and the diagnosis of asthma or COPD (%).
Generalpopulation
Asthma COPD
Never smokers 53.62 54.98 31.23Current-smokers 25.51 25.19 36.46Former smokers 20.88 19.83 32.32
254 M. Cazzola et al.
general picture on the one hand. Nonetheless, on the otherhand, it is well known that patients vary in their use ofhealth care and it is accepted that a significant proportionof patients who are ill may not consult their doctor and thiscan lead to underestimation of the problem.
Several reports have highlighted that diagnosed preva-lence and morbidity data underestimate the total burden ofCOPD because the disease is usually not diagnosed until it isclinically apparent, and there is considerable variation in
Table 4 Influence of smoking status on CV morbidities in the d(values are expressed as rates).
Asthma vs General population
Never-smokers
Currentsmokers
Ischemic cardiopathy 1.21 1.26Myocardial infarction 0.88 0.91Cardiac arrhythmia 1.29 1.34Heart Failure 1.51 1.57Hypertension 1.13 1.17Cerebrovascular disease 1.19 1.23Other heart disease 1.56 1.61Pulmonary embolism 1.53 1.59
reported prevalence.26e31 This is likely due to a lack ofawareness about COPD by patients. It is only 25e50% ofCOPD patients are known to their doctor.27 Patients maywell experience symptoms, but do not always present thesesymptoms to their family physician.27 Poor recognition ofthe disease may lead patients to believe that their respi-ratory symptoms are nothing more than a smoker’s cough,rather than an early sign of disease pathology, causing themto delay contact with a healthcare professional.26 In anycase, the majority of patients with a decreased FEV1 do notcomplain of any bronchial symptoms.32
Nonetheless, the underestimation of the actual burdenof COPD may also be due to the underdiagnosis of thedisease by healthcare professionals, particularly in theearly stages of the disease,33 mainly because in familypractice the diagnostic process is primarily based onsymptoms and signs presented by the patient and, conse-quently, early-stage COPD can easily be veiled by signs ofasthma.34 Also a lack of awareness among physicians of
iagnosis of asthma or COPD related to the general population
COPD vs General population
Formersmokers
Never-smokers
Currentsmokers
Formersmokers
1.31 5.87 2.39 2.210.95 5.05 2.06 1.901.39 4.08 1.66 1.541.63 9.20 3.75 3.461.22 2.98 1.21 1.121.28 5.41 2.20 2.041.68 5.67 2.31 2.131.65 5.33 2.17 2.00
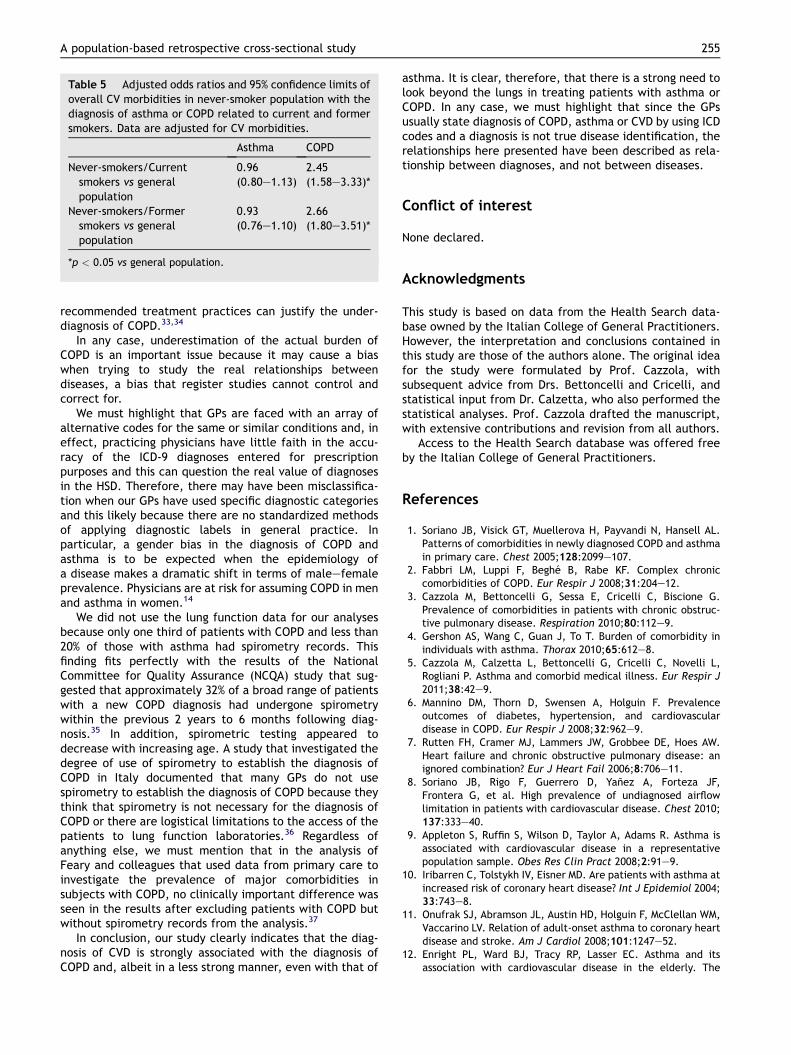
Table 5 Adjusted odds ratios and 95% confidence limits ofoverall CV morbidities in never-smoker population with thediagnosis of asthma or COPD related to current and formersmokers. Data are adjusted for CV morbidities.
Asthma COPD
Never-smokers/Currentsmokers vs generalpopulation
0.96(0.80e1.13)
2.45(1.58e3.33)*
Never-smokers/Formersmokers vs generalpopulation
0.93(0.76e1.10)
2.66(1.80e3.51)*
*p < 0.05 vs general population.
A population-based retrospective cross-sectional study 255
recommended treatment practices can justify the under-diagnosis of COPD.33,34
In any case, underestimation of the actual burden ofCOPD is an important issue because it may cause a biaswhen trying to study the real relationships betweendiseases, a bias that register studies cannot control andcorrect for.
We must highlight that GPs are faced with an array ofalternative codes for the same or similar conditions and, ineffect, practicing physicians have little faith in the accu-racy of the ICD-9 diagnoses entered for prescriptionpurposes and this can question the real value of diagnosesin the HSD. Therefore, there may have been misclassifica-tion when our GPs have used specific diagnostic categoriesand this likely because there are no standardized methodsof applying diagnostic labels in general practice. Inparticular, a gender bias in the diagnosis of COPD andasthma is to be expected when the epidemiology ofa disease makes a dramatic shift in terms of maleefemaleprevalence. Physicians are at risk for assuming COPD in menand asthma in women.14
We did not use the lung function data for our analysesbecause only one third of patients with COPD and less than20% of those with asthma had spirometry records. Thisfinding fits perfectly with the results of the NationalCommittee for Quality Assurance (NCQA) study that sug-gested that approximately 32% of a broad range of patientswith a new COPD diagnosis had undergone spirometrywithin the previous 2 years to 6 months following diag-nosis.35 In addition, spirometric testing appeared todecrease with increasing age. A study that investigated thedegree of use of spirometry to establish the diagnosis ofCOPD in Italy documented that many GPs do not usespirometry to establish the diagnosis of COPD because theythink that spirometry is not necessary for the diagnosis ofCOPD or there are logistical limitations to the access of thepatients to lung function laboratories.36 Regardless ofanything else, we must mention that in the analysis ofFeary and colleagues that used data from primary care toinvestigate the prevalence of major comorbidities insubjects with COPD, no clinically important difference wasseen in the results after excluding patients with COPD butwithout spirometry records from the analysis.37
In conclusion, our study clearly indicates that the diag-nosis of CVD is strongly associated with the diagnosis ofCOPD and, albeit in a less strong manner, even with that of
asthma. It is clear, therefore, that there is a strong need tolook beyond the lungs in treating patients with asthma orCOPD. In any case, we must highlight that since the GPsusually state diagnosis of COPD, asthma or CVD by using ICDcodes and a diagnosis is not true disease identification, therelationships here presented have been described as rela-tionship between diagnoses, and not between diseases.
Conflict of interest
None declared.
Acknowledgments
This study is based on data from the Health Search data-base owned by the Italian College of General Practitioners.However, the interpretation and conclusions contained inthis study are those of the authors alone. The original ideafor the study were formulated by Prof. Cazzola, withsubsequent advice from Drs. Bettoncelli and Cricelli, andstatistical input from Dr. Calzetta, who also performed thestatistical analyses. Prof. Cazzola drafted the manuscript,with extensive contributions and revision from all authors.
Access to the Health Search database was offered freeby the Italian College of General Practitioners.
References
1. Soriano JB, Visick GT, Muellerova H, Payvandi N, Hansell AL.Patterns of comorbidities in newly diagnosed COPD and asthmain primary care. Chest 2005;128:2099e107.
2. Fabbri LM, Luppi F, Beghe B, Rabe KF. Complex chroniccomorbidities of COPD. Eur Respir J 2008;31:204e12.
3. Cazzola M, Bettoncelli G, Sessa E, Cricelli C, Biscione G.Prevalence of comorbidities in patients with chronic obstruc-tive pulmonary disease. Respiration 2010;80:112e9.
4. Gershon AS, Wang C, Guan J, To T. Burden of comorbidity inindividuals with asthma. Thorax 2010;65:612e8.
5. Cazzola M, Calzetta L, Bettoncelli G, Cricelli C, Novelli L,Rogliani P. Asthma and comorbid medical illness. Eur Respir J2011;38:42e9.
6. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalenceoutcomes of diabetes, hypertension, and cardiovasculardisease in COPD. Eur Respir J 2008;32:962e9.
7. Rutten FH, Cramer MJ, Lammers JW, Grobbee DE, Hoes AW.Heart failure and chronic obstructive pulmonary disease: anignored combination? Eur J Heart Fail 2006;8:706e11.
8. Soriano JB, Rigo F, Guerrero D, Yanez A, Forteza JF,Frontera G, et al. High prevalence of undiagnosed airflowlimitation in patients with cardiovascular disease. Chest 2010;137:333e40.
9. Appleton S, Ruffin S, Wilson D, Taylor A, Adams R. Asthma isassociated with cardiovascular disease in a representativepopulation sample. Obes Res Clin Pract 2008;2:91e9.
10. Iribarren C, Tolstykh IV, Eisner MD. Are patients with asthma atincreased risk of coronary heart disease? Int J Epidemiol 2004;33:743e8.
11. Onufrak SJ, Abramson JL, Austin HD, Holguin F, McClellan WM,Vaccarino LV. Relation of adult-onset asthma to coronary heartdisease and stroke. Am J Cardiol 2008;101:1247e52.
12. Enright PL, Ward BJ, Tracy RP, Lasser EC. Asthma and itsassociation with cardiovascular disease in the elderly. The
256 M. Cazzola et al.
Cardiovascular Health Study Research Group. J Asthma 1996;33:45e53.
13. Schanen JG, Iribarren C, Shahar E, Punjabi NM, Rich SS,Sorlie PD, et al. Asthma and incident cardiovascular disease:the Atherosclerosis risk in communities study. Thorax 2005;60:633e8.
14. Cazzola M, Puxeddu E, Bettoncelli G, Novelli L, Segreti A,Cricelli C, et al. The prevalence of asthma and COPD inItaly: a practice-based study. Respir Med 2011;105:386e91.
15. World Health Organization. International classification ofdiseases. Manual of the international statistical classificationof diseases: injuries and causes of deaths (9th revision).Geneva: World Health Organization; 1977.
16. Lawrenson R, Williams T, Farmer R. Clinical information forresearch: the use of general practice databases. J PublicHealth Med 1999;21:299e304.
17. Filippi A, Bignamini AA, Sessa E, Samani F, Mazzaglia G.Secondary prevention of stroke in Italy: a cross-sectionalsurvey in family practice. Stroke 2003;34:1010e4.
18. Zhang J, Yu KF. What’s the relative risk? A method of correctingthe odds ratio in cohort studies of common outcomes. JAMA1998;280:1690e1.
19. Schmidt OC, Kohlmann T. When to use the odds ratio or therelative risk? Int J Public Health 2008;53:165e7.
20. Card JW, Zeldin DC. Hormonal influences on lung functionand response to environmental agents: lessons from animalmodels of respiratory disease. Proc Am Thorac Soc 2009;6:588e95.
21. Ben-Zaken Cohen S, Pare PD, Man SFP, Sin DD. The growingburden of chronic obstructive pulmonary disease and lungcancer in women. Examining sex differences in cigarettesmoke metabolism. Am J Respir Crit Care Med 2007;176:113e20.
22. Sin DD, Cohen SB, Day A, Coxson H, Pare PD. Understanding thebiological differences in susceptibility to chronic obstructivepulmonary disease between men and women. Proc Am ThoracSoc 2007;4:671e4.
23. Johnston AK, Mannino DM, Hagan GW, Davis KJ, Kiri VA. Rela-tionship between lung function impairment and incidence orrecurrence of cardiovascular events in a middle-aged cohort.Thorax 2008;63:599e605.
24. Macie C, Wooldrage K, Manfreda J, Anthonisen N. Cardiovas-cular morbidity and the use of inhaled bronchodilators. Int JChron Obstruct Pulmon Dis 2008;3:163e9.
25. Camp PG, Goring SM. Gender and the diagnosis, management,and surveillance of chronic obstructive pulmonary disease.Proc Am Thorac Soc 2007;4:686e91.
26. Britton M. The burden of COPD in the U.K.: results from theConfronting COPD survey. Respir Med 2003;97(Suppl C):S71e9.
27. van Schayck CP, Chavannes NH. Detection of asthma andchronic obstructive pulmonary disease in primary care. EurRespir J 2003;39(Suppl:1):6se22s.
28. Mohangoo AD, van der Linden MW, Schellevis FG, Raat H.Prevalence estimates of asthma or COPD from a health inter-view survey and from general practitioner registration: what’sthe difference? Eur J Public Health 2006;16:101e5.
29. Lindberg A, Bjerg A, Ronmark E, Larsson LG, Lundback B.Prevalence and underdiagnosis of COPD by disease severity andthe attributable fraction of smoking report from the obstruc-tive lung disease in Northern Sweden studies. Respir Med 2006;100:264e72.
30. Vandevoorde J, Verbanck S, Gijssels L, Schuermans D,Devroey D, De Backer J, Kartounian J, Vincken W. Earlydetection of COPD: a case finding study in general practice.Respir Med 2007;101:525e30.
31. Tinkelman DG, Price D, Nordyke RJ, Halbert RJ. COPDscreening efforts in primary care: what is the yield? Prim CareRespir J 2007;16:41e8.
32. White P. Prevalence of COPD in primary care: no room forcomplacency. Fam Pract 2009;26:1e2.
33. Nacul L, Soljak M, Samarasundera E, Hopkinson NS, Lacerda E,Indulkar T, et al. COPD in England: a comparison of expected,model-based prevalence and observed prevalence fromgeneral practice data. J Public Health 2011;33:108e16.
34. Albers M, Schermer T, Molema J, Kloek C, Akkermans R,Heijdra Y, et al. Do family physicians’ records fit guidelinediagnosed COPD? Fam Pract 2009;26:81e7.
35. Han MK, Kim MG, Mardon R, Renner P, Sullivan S, Diette GB,et al. Spirometry utilization for COPD: how do we measure up?Chest 2007;132:403e9.
36. Caramori G, Bettoncelli G, Tosatto R, Arpinelli F, Visona G,Invernizzi G, et al. Underuse of spirometry by general practi-tioners for the diagnosis of COPD in Italy. Monaldi Arch ChestDis 2005;63:6e12.
37. Feary JR, Rodrigues LC, Smith CJ, Hubbard RB, Gibson JE.Prevalence of major comorbidities in subjects with COPD andincidence of myocardial infarction and stroke: a comprehen-sive analysis using data from primary care. Thorax 2010;65:956e62.
















![static.cambridge.orgcambridge... · Web viewMultiple myeloma Retrospective cohort Cancer center VRI multiplex PCR Teh et al. 2015 [70] Canada 2007-2008 COPD Prospective cohort Hospital](https://img.pdfslide.us/doc/110x75/60c2ed71fbe2cf7121328195/cambridge-web-view-multiple-myeloma-retrospective-cohort-cancer-center-vri.jpg)












