Embed Size (px)
Citation preview
CARDIOVASCULAR CONFERENCE: Approach to a patient with
cyanotic heart disease
General Data:
• Name: Baby Boy G• Neonate• born of a 22 year old primigravida
History of the Present Illness
• Initial prenatal check-up– 6th month of pregnancy at local health center– CBC, urinalysis normal– UTZ (9/6/10): right ventricle appears collapsed
• Single live intrauterine pregnancy, cephalic, good cardiac and somatic activity, 24-25 weeks AOG, rule out hypoplastic right ventricle.
• Suggests congenital anomal scan scan with detailed cardiac evaulation preferably using fetal echocardiogram
– Referred to USTH
September 8, 2010
• UTZ: 2nd and 3rd trimester– Single live intrauterine pregnancy of about 24-25
weeks in breech presentation with good cardiac and somatic activity
– Suggest fetal 2D echo c/o Dr. Cuaso
September 8, 2010
• Assessment: Pregnancy 24-25 weeks AOG based on 2nd trimester ultrasound, t/c hypoplastic right ventricle
• Advised: – Multivitamins + FESO4 1 cap OD– Milk formula 1 glass OD– Request for CBC with blood typing, urinalysis, 50g
OGCT– Request for congenital scan– Attend mother’s class every Saturday 10-11 am
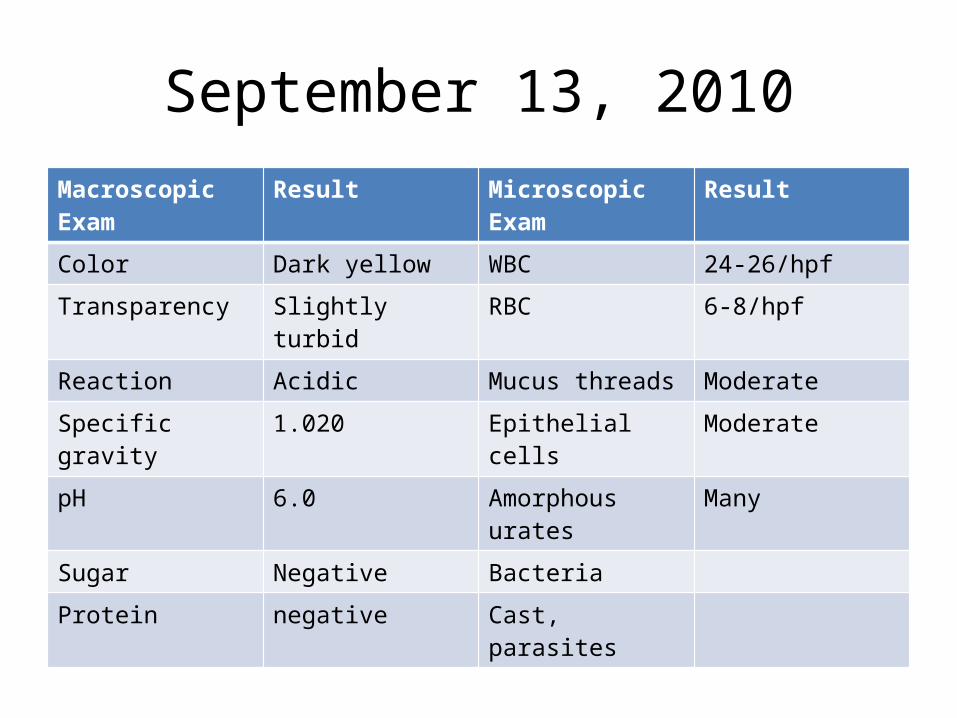
September 13, 2010Macroscopic Exam Result Microscopic Exam Result
Color Dark yellow WBC 24-26/hpf
Transparency Slightly turbid RBC 6-8/hpf
Reaction Acidic Mucus threads Moderate
Specific gravity 1.020 Epithelial cells Moderate
pH 6.0 Amorphous urates Many
Sugar Negative Bacteria
Protein negative Cast, parasites
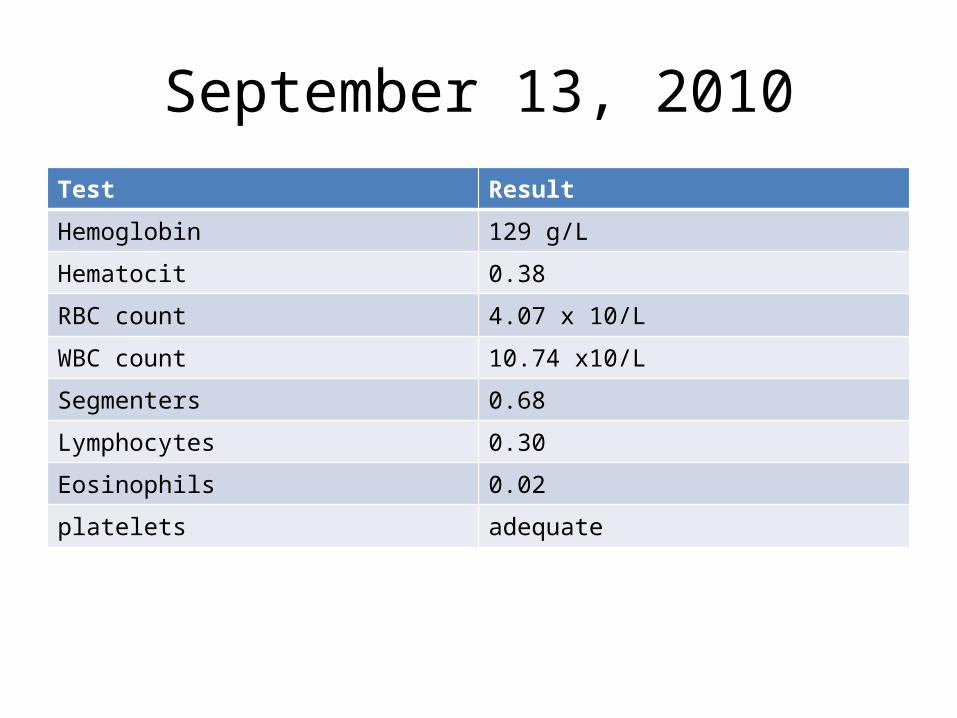
September 13, 2010Test Result
Hemoglobin 129 g/L
Hematocit 0.38
RBC count 4.07 x 10/L
WBC count 10.74 x10/L
Segmenters 0.68
Lymphocytes 0.30
Eosinophils 0.02
platelets adequate
September 16, 2010
• OB GYN OPD– Speculum exam: cervix violaceous, smooth with
moderate frothy yellowish creamy discharge– Assessment: Trichomoniasis– Advised: Metronidazole 500 mg/tab 1 tab BID
• Fetal 2D Echo once with funds• 50g OGCT, repeat urinalysis clean catch
September 24, 2010
• Follow-up• Unremarkable • Still for fetal 2D Echo, 50g OGCT
October 5, 2010
• (+) terminal dysuria• Urinalysis
– Acidic– (++) bacteria– 2-5/hpf pus cells
• Normal OGCT results• Advised:
– Amoxicillin 500 mg/tab 1 tab q8 for 7 days– Once with 2D Echo results, refer to pediatric surgery
• (+) hyperemic conjunctiva OD- referred to Ophtha
October 15, 2010
• USTH (October 11, 2010)– Fetal 2D- Echocardiogram: hypoplastic Left Ventricle,
hypoplastic Mitral Valve, and a patent foramen ovale– FHT 142
• Assessment: Pregnancy 29-30 weeks, hypoplastic left heart
• Advised: – Refer to pediatrics-cardiology and pediatric surgery
November 22, 2010
• (+) persistence of dysuria• Assessment: Pregnancy 35-36 weeks AOG,
cephalic, Hypoplastic left ventricle, t/c UTI• Advised
– Urinalysis, Hepatitis B Ag, Blood typing
November 25, 2010
• Assessment: UTI• Advised:
– Amoxicillin 500mg/cap 1 cap q8 for 7 days– Increase oral fluid intake
November 25, 2010
• Pediatric Surgery Consult• Assessment: Pregnancy 36 weeks AOG, (?)
hypoplastic left ventricle• Plans: will evaluate any time after delivery
November 26, 2010
• Blood type: AB+

December 10, 2010
• UTZ: 2nd and 3rd trimester– There seems to be a mass in the interventricular
septum– Single live intrauterine pregnancy of about 35-36
weeks in cephalic presentation– BPS 8/8; SEFW 2823 grams– Cardiomegaly
• Suggest referral to Dr. Cuaso
December 10, 2010
• High Risk OB GYN clinic• Assessment: Hypoplastic left ventricle,
hypoplastic mitral valve, UTI, r/o IUGR• Advised: Terraferon, Clusivol OB, Cefuroxime
500 mg/tab BID for 7 days– Repeat urinalysis after 7 days– BPS
December 17, 2010
• UTZ: 38 weeks 6 days AOG• (-) dysuria• (+) fetal movements, irregular hypogastric
pains, SEFW p10-50• IE: 1 cm dilated, 60% effaced, (+) BOW,
cephalic, Stn -3• Assessment: Pregnancy 38-39 weeks, cephalic,
not in labor, ? Mass at the interventricular septum, UTI s/p treatment
December 12, 2010
• UTZ: 2nd and 3rd trimester• Findings:
– There seems to be a mass at the interventricular septum
– Single live intrauterine pregnancy of about 35-36 weeks in cephalic presentation
– BPS 8/8; SEFW 2823 grams– Cardiomegaly– Suggest referral to Dr. Cuaso
December 20, 2010
• For follow up • Supposedly for repeat Fetal 2D Echo• 3 cm dilated, 70% effaced intact BOW, there
was progression of labor alongside with spontaneous rupture of BOW.
• Clear, non-foul smelling amniotic fluid
Maternal History
• (-) exposure to radiation• (-) symptoms of viral exanthems• (-) use of illicit drugs and abortifacients • Non-smoker• Non drinker of alcoholic beverages• (-) hypertension, allergy, thyroid disease, diabetes,
asthma, liver disease, or blood dyscrasia – Hep B screening non-reactive– OGCT normal
Family HistoryName Age Relation Educational
AttainmentOccupation Health
MPG 22 Mother 2nd year nursing student
Student Healthy
LG 23 Father High school graduate
Unemployed Healthy
Family History
• No diabetes, hypertension, cardiac diseases, cancer, tuberculosis, allergies
• Denies hereditary illnesses
Physical Examination
• General Data– live, term, singleton, male, delivered via normal
spontaneous delivery– BW 2.75 kg, BL 48 cm– AS 6 and 7 at 5 minutes, MT 38-39 weeks – AGA
Physical Examination on Admission
• HR 134 bpm, RR 58 cpm, T 37.2˚C • Blue, pale, (+) circumoral cyanosis• (-) Rash, (-) birth marks, (+) palmar and plantar
cyanosis• (+) Molding, (+) caput succedaneum (-)
cephalhematoma• (+) ROR OU, (-) eye discharge, normal set ears,
(-) preauricular pits, patent nares, (-) Epstein’s pearls
Physical Examination on Admission
• (-) Palpable neck masses, intact clavicle, no crepitations
• (-) Chest deformities, symmetrical chest expansion, (-) retractions, clear and equal breath sounds, good respiratory effort
• Adynamic precordium, regular heart rate and rhythm, grade 1 holosystolic murmur at left parasternal area
• Globular abdomen, (+) umbilical stump with 2 arteries and 1 vein, (-) organomegaly, (-) palpable masses
• Grossly male, bilaterally descended testes, good rugae, patent anus
• Femoral pulses full and equal, good flexion of extremities, (-) Barlow, (-) Ortolani
• Straight spine, (-) sacral dimpling, (-) tuft of hair
• (+) Moro, grasp, rooting, plantar, and sucking reflexes
APPROACH TO DIAGNOSIS OF A PATIENT PRESENTING WITH CYANOSIS AT BIRTH
Indicators that heart disease may exist
• Cyanosis• Cardiomegaly (Radiologic or Pericardial bulge)• Pathologic heart murmur• Tachypnea or overt respiratory distress (dyspnea)• Sweating especially during feeding• Increased or decreased pulses• Failure to thrive
Classification of Congenital Heart Diseases
A) Acyanotic
B) Cyanotic
Major Considerations
• Is there a shunt (LR or RL)• Is there obstruction to inflow or outflow• Abnormal heart valves• Abnormal connections of great vessels• Combination
Subgroups of Acyanotic Diseases
• Shunt anomalies• Valvular defects• Obstructive lesions• Inflow anomalies• Primary myocardial diseases
Shunt Anomalies
• L R shunt• Increased pulmonary blood flow• Increased pulmonary vascular arterial
markings on chest Xray
• ASD, VSD, PDA
Obstructive Lesion
• Discrepancy in amplitude of the peripheral pulses
• Coarctation of the Aorta
Inflow Anomalies
• Increased pulmonary venous markings on chest Xray
• No murmur
• Cor Triatriatum, Pulmonary vein stenosis
Valvular Defects
• Stenosis or regurgitant• Characteristic murmur
• AS, AR, PS, PR, MS, MR, TS, TR
Primary Myocardial Diseases
• No murmur• Disparity between cardiac size and pulmonary
vascular markings
• Glycogen storage disease• Cardiomyopathy
Hemodynamic Consequences
A) Volume (Diastolic) overload
B) Pressure (Systolic) overload
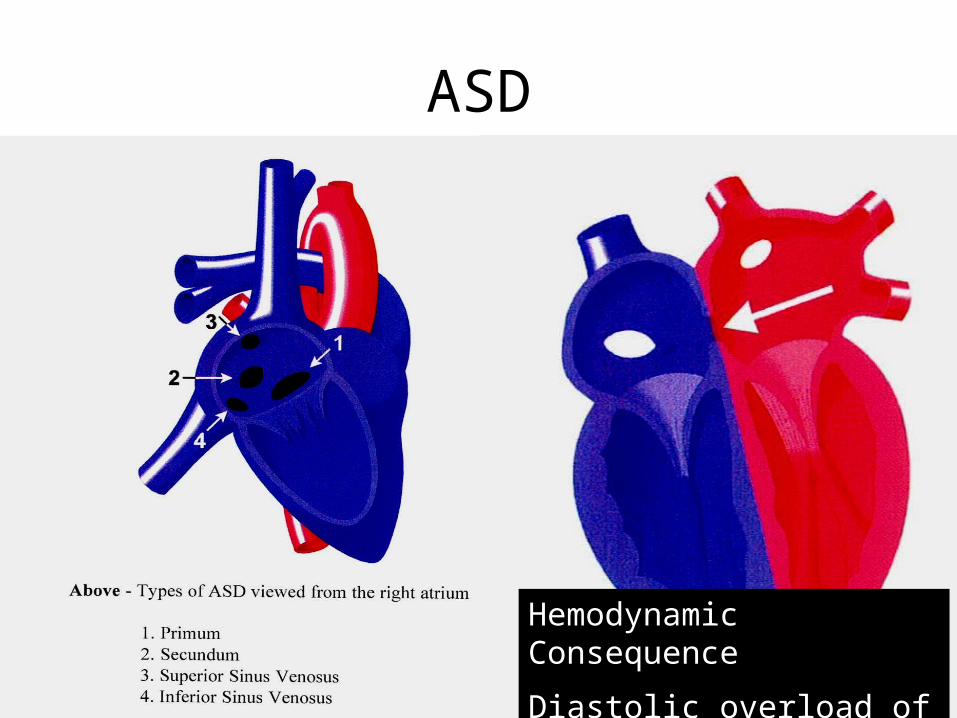
ASD
Hemodynamic Consequence
Diastolic overload of RV
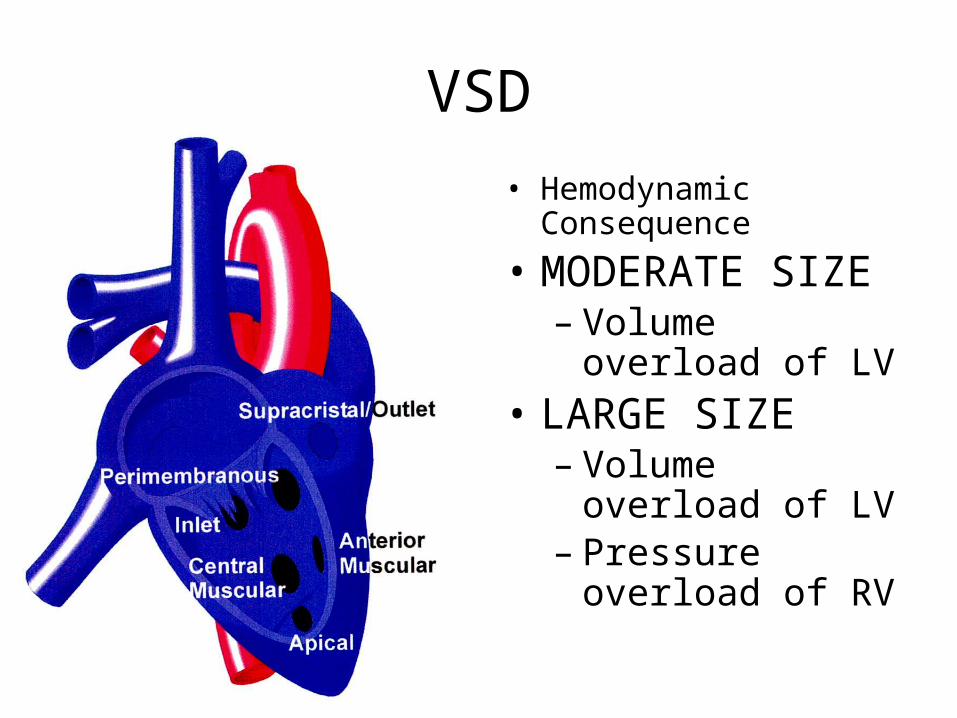
VSD• Hemodynamic
Consequence
• MODERATE SIZE– Volume overload of
LV• LARGE SIZE
– Volume overload of LV
– Pressure overload of RV
Cyanotic Heart Disease
• Cyanotic heart disease exist when one defect or association of defects allow the mixture of saturated and de-saturated blood to reach the systemic circulation
Do you suspect that patient is Cyanotic?
• When in doubtA) ClubbingB) CBCC) Hyperoxia test
Hyperoxia Test
• Hyperoxia test is considered positive for intracardiac shunting if PO2 < 150 mmHg (torr) after 10 minutes of 100% fiO2
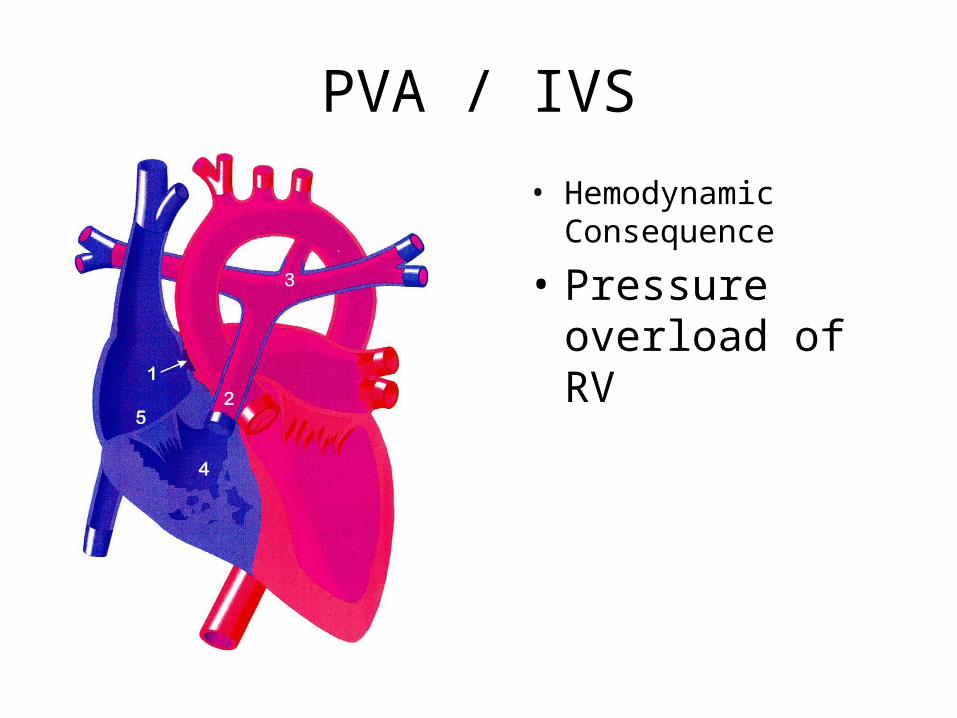
PVA / IVS
• Hemodynamic Consequence
• Pressure overload of RV
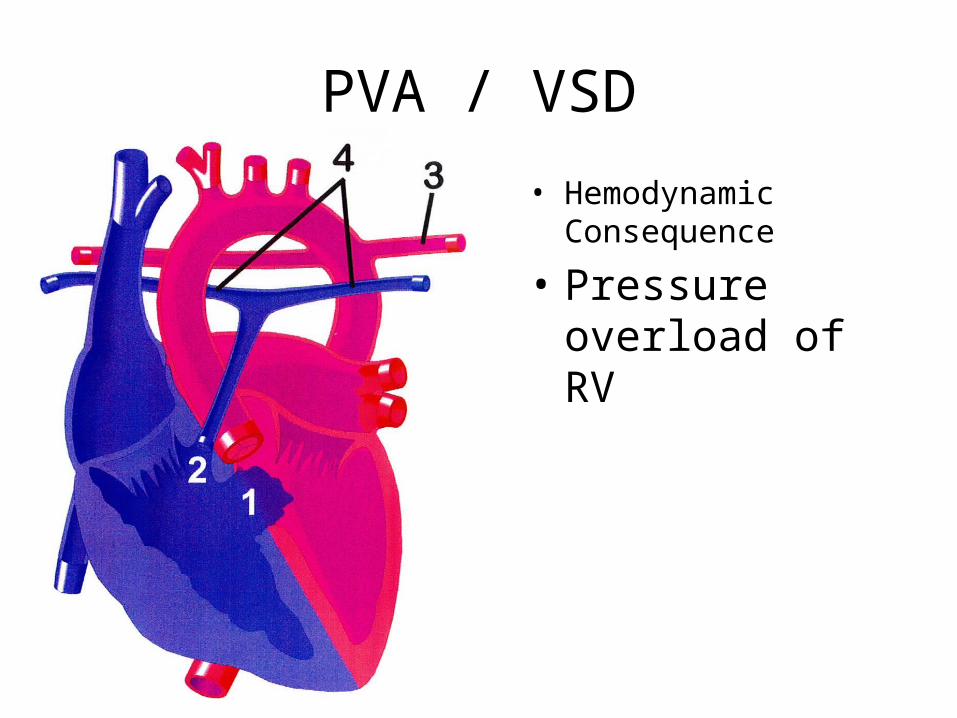
PVA / VSD
• Hemodynamic Consequence
• Pressure overload of RV
PDA Dependent Pulmonary Circulation
• Pulmonary valve atresia (PVA) with intact interventricular septum
• Other lesions with accompanying PVA
Approach to diagnosis
A) Chest Xray Increased or decreased pulmonary vascular arterial markings
B) EKG RVH, LVH, CVH
C) Character of second heart sound
S2 single, loudS2 single, normalSplit S2
Chest x-ray
Causes of Cyanosis
Noncardiac Cardiac
•Pulmonary disorders (structural abnormalities of the lung, ventilation-perfusion mismatching, congenital or acquired airway obstruction, pneumothorax, hypoventilation)•Abnormal forms of hemoglobin (methemoglobin)•Poor peripheral perfusion (sepsis, hypoglycemia, dehydration, hypoadrenalism)•primary or persistent pulmonary hypertension
Increased pulmonary vascularity•D-TGA•TAPVR without obstruction•PTA•Single ventricle•DORV w/o PS•PPHN
Decreased pulmonary vascularity•TOF•Ebstein’s anomaly•PS•PA•TA with PS•DORV with PS
Pulmonary Vascular MarkingsDecreased: Cyanotic
TOF Tricuspid Atresia
Complex heart with PS PVA / IVS
Second Heart Sound (S2)
Single Loud Single Normal Split S2
TGA TOF TAPVR without obstruction
Aortic / Mitral atresia
Tricuspid atresia
Truncus Arteriosus
PVA
Cardiac Work-Up
A) EKGB) Chest XrayC) 2D echocardiography
(TTE, TEE, ICE, IVUS)D) Cardiac catheterizationE) CT angiography, cardiac MRI
• PLACE THE:– ECG– 2-D ECHO
Modalities of Management
A) PharmacologicB) Catheter based therapyC) Surgical
Pharmacologic
A) digoxin, diuretics, inotropes (pressor), vasodilators
B) Prostaglandin
Catheter Based Therapy (DI KO PA ALAM ITO, EXAMPLES LANG TO)
A) Balloon atrio septostomy (Rashkind)B) Balloon valvuloplastyC) Balloon angioplastyD) Delivery of occlusion devicesE) Radio frequency ablation
Surgical (DI KO PA ALAM ITO, EXAMPLES LANG TO)
A) Shunts like Modified Blalock-TaussigB) PA bandC) Complete repairD) Glenn, FontanE) NorwoodF) Jatene, Mustard, Senning
Course in the Wards
• 1:31 AM (12/21/10)– May feed 10-15mL FBM q3 with strict aspiration precautions– Keep O2 sat >62%– Refer to pedia cardio– Prewarmed radiant warmer– Labs: CBC with PC, CXR, 2D echo, 15L ECG– Routine newborn care
• Erythromycin strip 1cm OU• Vit K 1mg/IM• Hepa B vaccine 0.5mg/IM at lateral thigh• Cord care with 70% ethanol
Course in the Wards
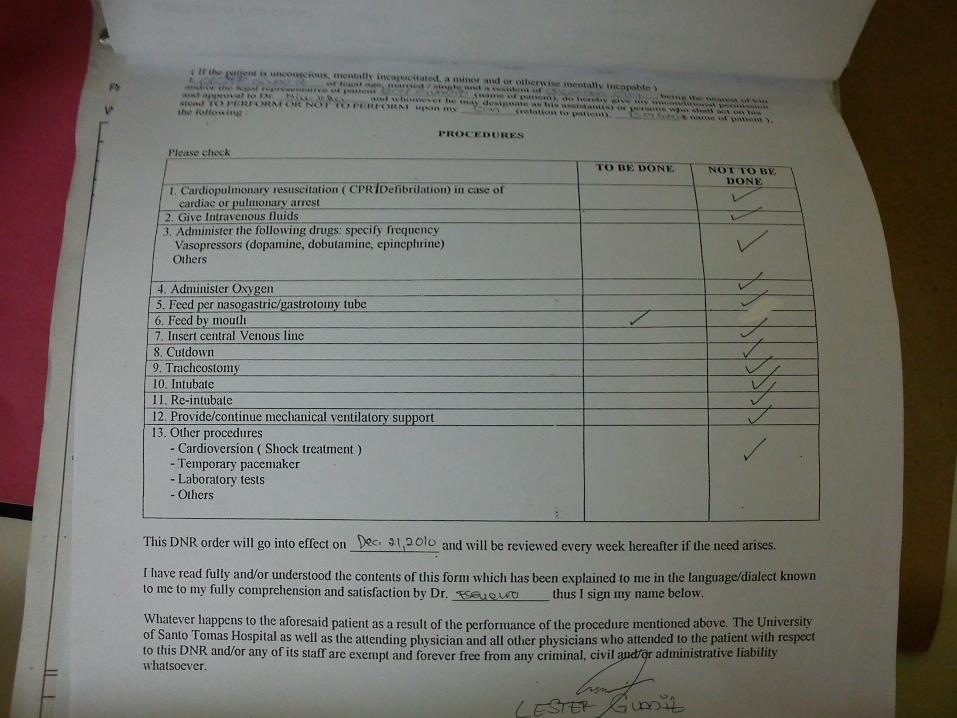
• 7:30 AM (12/21/10)– Opted to withhold any further aggressive
treatment• 1:00PM (12/21/10)
– Referral to pedia cardio answered• 7:00 AM (12/22/10)
– Feeding: 20-30mL FBM q3• 9:00 AM (12/23/10)
– Decision to take home baby
Course in the Wards
• 12:00 NN (12/23/10)• Discharge instructions
– Daily cord care with 70% ETOH q6– Daily bath with mild soap and lukewarm water– Daily sun exposure 7 to 9 AM for 15 min– Exclusive breastfeeding q2-q8 15 to 30min for each breast
• Discharge medications– Multivitamins 0.5mL/day
• Follow up at Pedia High Risk and cardio clinic• For hearing screening as out patient
15L ECG
• Normal axis• Sinus tachycardia• LVH
2D echo
• PDA• Pulmonary valve atresia• Intact ventricular septum• Hypertrophied right ventricle• Probably tripartite chamber• R->L shunt across formen ovale• Pulmonic annulus 5.6cm, MPA 5.22mm, RPA 5.0mm,
LPA 6.0mm• Normal aortic arch, coronary arteries, pulmonary veins
CXR
• Lung fields are clear• Prominent cardiac silhouette• Suspicious prominence of pulmonary
vascularity• Normal hemidiagphragms and sinuses• Unremarkable visualized osseous structures
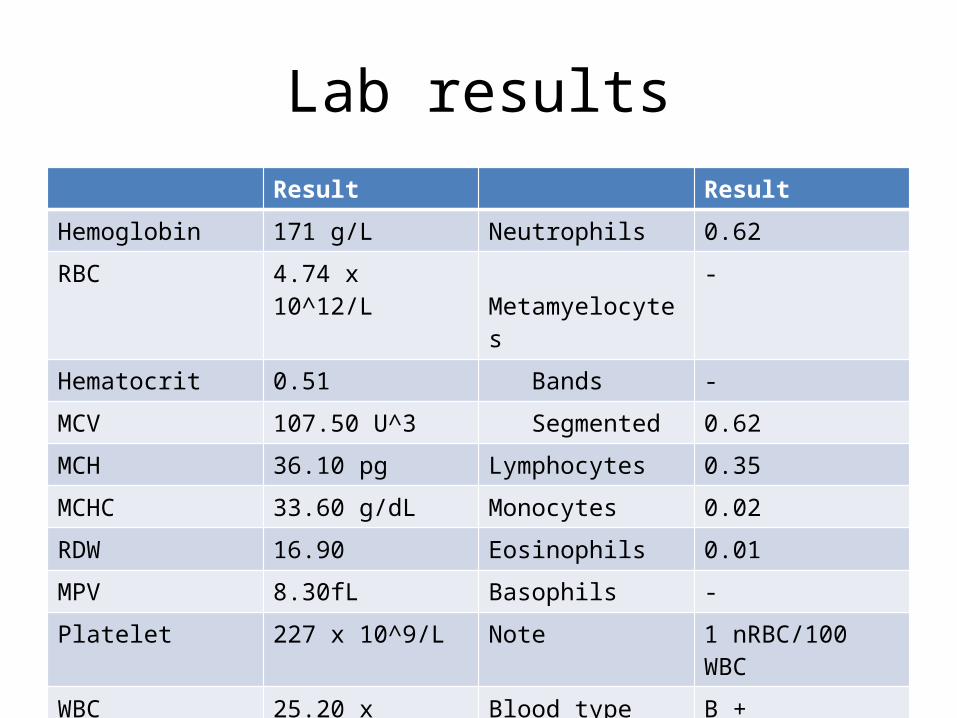
Lab resultsResult Result
Hemoglobin 171 g/L Neutrophils 0.62
RBC 4.74 x 10^12/L Metamyelocytes -
Hematocrit 0.51 Bands -
MCV 107.50 U^3 Segmented 0.62
MCH 36.10 pg Lymphocytes 0.35
MCHC 33.60 g/dL Monocytes 0.02
RDW 16.90 Eosinophils 0.01
MPV 8.30fL Basophils -
Platelet 227 x 10^9/L Note 1 nRBC/100 WBC
WBC 25.20 x 10^9/L Blood type B +