Embed Size (px)
Citation preview

Cardiovascular Anatomy and Physiology
REVIEW
Reading:
Brubaker 2:37-56

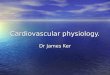
Normal HeartNormal Heart Myocardial Myocardial Infarct (LAD)Infarct (LAD)
Photos: Klatt, Edward C. MD, WebPath.edu

Primary Cardiac Function = Primary Cardiac Function = Tissue PerfusionTissue PerfusionMorbidity and Mortality of
Cardiovascular Disease:Inadequate Cardiac OutputReduced Perfusion (O2) to the
“BIG THREE” vital organs:Brain, Heart, Lungs
Other Organ Failure: Kidneys, Liver, GI, Skeletal Muscle

Cardiac AnatomyCardiac Anatomy: Pericardium: Visceral / Parietal
connective tissue “wrapping”Epicardium: next to the heartPericardial space: fluid filledFibrous/serous pericardium:
Prevents overdistension of the heart and produces fluid
Cardiac Tamponade: Life threateningAccumulation of fluid in p. space

Layers of Heart TissueLayers of Heart Tissue:Pericardium: Double Layered
Outer, Fibrous: Tough connective fibrous tissue - Parietal
Inner, Serous: Epithelial and thin connective tissue layer -Visceral, epicardium

Heart Layers: Heart Layers:
Myocardium: Cardiac muscle layer
Endocardium: Connective + Epithelial TissueStructural “ScaffoldingValvesChordae Tendinae

Endothelial “ScaffoldingEndothelial “Scaffolding””
Endocardium The fibrous network forms chambers of the Ventricles

Myocardium:Myocardium:
You end up with a very strong muscle in the shape of a multi-chambered pump

Coronary Arteries:Coronary Arteries:
Left Coronary Artery: Origin: Left side of AORTASupplies: Anterior/Left Heart
Right Coronary Artery:Origin: Rt. Side of AORTASupplies: Right Heart


Rt.MarginalBranch

Coronary Artery Bloodflow Coronary Artery Bloodflow Regulation:Regulation:Aortic Pressure is primary
regulatorSympathetic: Net Increase in
BloodflowParasympathetic: Maintain
BloodflowMetabolic: Bloodflow = VO2

Cardiac Cycle and Cardiac Cycle and Coronary Artery Flow:Coronary Artery Flow:Systole: The aortic valve opens,
and “covers” the Coronary arteries Blood flow is prevented
Diastole: The aortic valve closes, “opens” the coronariesBlood Flow is restored
What would be the effect of increased HR on Coronary blood flow (perfusion)?

Coronary Artery Disease: Coronary Artery Disease: CADCAD When critical bloodflow to the heart
muscle is compromised, The Heart Cannot “Rest” from its work! DEMAND > SUPPLY (Ouch!)
Arteriosclerosis: “Hardening of the arteries” (could be just aging) ATHEROsclerosis: The hardening and
progressive narrowing is caused by lipid deposits provoking fibrosis and calcification
Progressively PATHOLOGICAL!

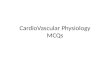
Fatty Arteries:
Normal CoronaryArtery
AtheroscleroticArtery
Photos: Klatt, Edward C., WebPath.com

Cardiovascular Cardiovascular Function:Function:
PUMP: Heart contractions propel Blood throughout the circulation!

Cardiac CycleCardiac Cycle:Ventricular Systole:
Ventricles Contract – eject bloodTri/Bicuspid valves closeFirst Heart Sound: “Lubb”
Ventricular Diastole: Ventricles relax, fillPulmonary/Aortic Valves closeSecond Heart Sound: “Dupp”

The Atria: The Atria: “Collection” of blood from either:
Right: The systemic circulation (low PO2)
Left: The pulmonary circulation (high PO2)
Atrial Contraction: Empties the final 30% of the End
Diastolic Volume (EDV)What is the impact of Atrial FibrillationOn Cardiac Output?

Right Ventricle pumps blood to the lungs
Right Ventricle contracts
Increased pressure causes tricuspid valve closure
Blood leaves heart via Pulmonary Artery Only artery with O2

Left Ventricle Pumps Blood to the Body
The Left Ventricle contracts
Mitral Valve: Closes Aortic Valve: Opens Blood is pumped out
via the Aorta
Aorta

Terms: Terms: Preload: The pressure in the left
ventricle immediately before contraction: Mostly related to volume EDV
Afterload: The pressure in the left ventricle immediately after contraction:Mostly related to Vascular resistance
Ejection Fraction: The amount of blood ejected by the LV – expressed as a % of the EDV

Systemic Arterial Systemic Arterial Blood PressureBlood PressureSystolic: Systole causes increased
pressure in the arterial vessels: Systolic pressures indicate the
strength of cardiac contractionDiastolic: During diastole, arterial
pressure is at it’s lowestDiastolic Pressures indicate the
total resistance to blood flow

Cardiac Output: HR X SVCardiac Output: HR X SVCO = HR X SV“Emergencies”
SNS Autonomic NSIncrease HR/SV = Increase CO
“Relaxing” – Status Quo:PSNS Autonomic NSDecrease HR = Decrease CO

Electrophysiology of Electrophysiology of the Heart: ECGthe Heart: ECG
P: Atrial Depolarization/contractionQRS: Ventricular Depol/ContractionT: Ventricular Repolarization

Cardiac Muscle CellsCardiac Muscle Cells:Striated, Branched, Intercalated
DiscsSlower Action Potential than
nerve or skeletal muscle cellsVoltage Gated Ca++
Channels!

Electrical Activity: Electrical Activity: Excitation - ContractionExcitation - ContractionTo contract, cardiac muscle
cells must depolarize and propagate an Action Potential
The Conduction of Action Potentials and Contractions must be well coordinated to efficiently pump blood.

Action Potentials:Cardiac vs. Skeletal Depolarization
Na+ and Ca++ Channels open
Plateau: All but Ca++ channels close
Repolarization K+ open and Ca+
+channels close
Depolarization: Na+ channels open
Repolarization: Voltage Gated K+ channels open / Na+ channels close

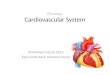
Myocardial Action PotentialMyocardial Action Potential
mV
-100
+40
0
4
0
1 2
3
4
ECG
AP

Why the Plateau Phase Why the Plateau Phase and Calcium?and Calcium? Plateau Phase: Longer Relative
Refractory period: Cannot be re-stimulated – permitting
coordinated contraction of entire heart muscle.
Calcium: Important in the automaticity of cardiac myocytes Links excitation to contraction Increases contraction force

Coordinating the Beats…Coordinating the Beats…
Contractions of the ventricles and atria must alternate
The excitation of the heart muscle follows a predictable path

Conduction System:Conduction System:SA Node: 90-100 bpmAV Node: Slows the message
downAV Bundles: (also His):L./R. Bundle Branches:Purkinje Fibers:

Heart Conduction SystemHeart Conduction SystemThe Sino-Atrial node (SA) serves as the pacemaker for the heart.When the SA node fires, it causes both atria to contractThe excitation-contraction signal is then “conducted” to the ventricles via the AV Node
SA

Heart Rate ControlHeart Rate Control Each heart cell can contract
independently and automatically The entire heart must not contract at
the same time. Excitation-Contraction of the heart is
coordinated from “top to bottom” The excitation-contraction pathway
is called “The Conduction System”

Extrinsic Control of Extrinsic Control of Heart RateHeart Rate
The SA node has an Intrinsic Rate of 90-100 bpm – “Default Rate”
External controls modify the heart rate: both at rest and during exercise
Controls: Parasympathic Nervous System, Sympathetic Nervous System, Endocrine System

Parasympathetic Nervous Parasympathetic Nervous SystemSystem “Maintenance” control Vagus nerve innervates heart at the SA
Node with some control of the AV Node Causes reduced HR Neurotransmitter: Acetylcholine
(“cholinergic”) Atropine blocks blocks PSNS and
increases HR

Sympathetic Nervous Sympathetic Nervous SystemSystem “Rescues” in homeostatic emergencies (like
exercise) Increases HR Increases Systolic contractility (Increased BP) Increases Mental acuity (you are prepared for
battle!) Neurotransmitter: Norepinepherine
(Adrenaline = “adrenergic”) Propranolol (SNS Beta-receptor blocker)
reduces HR

Endocrine SystemEndocrine System
The adrenal medulla (above kidney) secretes Catecholamines: Epinephrine Norepinephrine
Stimulated by and mimics the Sympathetic Nervous System Slower/Longer acting

Regulation of Cardiac Regulation of Cardiac Output:Output:Cardiac Output: Changes in
CO are responses to “Homeostatic Emergencies”:
Pressure EmergenciesChemical Emergencies

Baroreceptors: Sensing Baroreceptors: Sensing Pressure EmergenciesPressure Emergencies Increase CO = Increase Systolic BP Emergency 1: Decreased Pressure
Increase SNS: Increased HR X SV = Increased CO
Problem 2: Increased PressureDecrease SNS: Decrease HR =
Decreased CO

Chemoreceptors: Sensing Chemoreceptors: Sensing Metabolism EmergenciesMetabolism Emergencies Emergency 1: Increased Metabolic
Rate: Increased CO2, H+ (decreased pH) Increased SNS …CO
Problem 2: Decreased Metabolic Rate: What’s the Problem? Decreased CO2/ H+ (increased pH) Decreased SNS …CO Conserver the rescue efforts

Intrinsic Regulation of Cardiac Output: Starling’s LawIncreased Venous Return
Increased cardiac muscle stretchIncrease contraction forceIncreased SV = Increased CO
Occurs without SNS/PSNS involvement
Exercise….

Final Question: In a Heart
Transplant, the heart is “denervated”
How does someone with a heart transplant respond to exercise?

Hints: Remember – Starling’s Law of
the HeartRemember that though the
nerves are no longer signaling, there is another (though slower and longer acting) source of control…

Blood Vessels And Blood Vessels And CirculationCirculation

Peripheral Circulation:Systemic Circulation:
Blood vessels directing blood to the body tissuesLeft Heart to Right Heart
Pulmonary Circulation: Blood vessels directing blood to the
lungs for gas exchangeRight Heart to Left Heart
What do we call the circulation to The heart?

Perfusion HomeostasisPerfusion Homeostasis: Internal Environment: Depends
on appropriate perfusion (Blood flow)
Homeostasis: A constant balance of choices in maintaining central blood pressure (to maintain the “Big 3”) and distribution to demanding tissues

Three Vessel “Tunics”:Three Vessel “Tunics”:
Tunica Adventitia (Externa): Fibrous connective tissue
Tunica Media: Smooth Muscle and elastic connective tissue
Tunica Intima: Endothelium (forms the valves in veins)

Arteries: Vessels taking
blood Away From The Heart
Usually O2 and nutrient rich…”Supply” to tissues

Arteries: Structure/FunctionHigh Pressure Conduits:
Elastic Connective Tissue: Expands with systole, and recoils with diastole
Smooth Muscle: Assist in “pumping” and “directing” blood flow
Endothelium: Smooth inner surface

Veins: Vessels returning
blood Back To The Heart
Usually low in O2 – carrying wastes for removal

Veins: Structure/FunctionLow Pressure “Pools”:
Sometimes called “capacitance vessels” because they have a large reservoir (capacity) for blood
Less connective tissue and smooth muscle than arteries
Endothelium: Specialized valves assist blood flow toward heart

Arterial Blood PressureCardiac Output: Reflected by
Systolic blood pressureVascular Resistance:
Reflected by Diastolic PressureVessel DiameterBlood ViscosityVessel Length

Pressure and Resistance
Increased Resistance = Increased Pressure
Increased Resistance = Increased Work of the Heart
Measurement: 120/80 mm Hg

Vasoconstriction:Decreases Vessel DiameterIncreases ResistanceIncreases Diastolic BP
Increases Work of HeartIncreases SBP later
SNS, Cold, Hemorrhage etc cause vasoconstriction to “rescue” vital organs

Vasodilation:Increases Vessel DiameterDecreases ResistanceDecreases Diastolic PressurePSNS, Heat, Local Exercise
Demand cause vasodilation to perfuse skin, muscles for special situations

Arteriosclerosis
Limits VasodilationIncreases ResistanceIncreases PressureRisk Factors:
Obesity, Cholesterol, Inactivity, Smoking, Aging, Heredity

Systolic and Diastolic BP:Systolic: Ventricular Systole
Greatest Arterial PressureReflects CO and heart’s contribution to
BPDiastolic: Ventricular Diastole
Lowest Arterial PressureReflects the resistance of the vessels to
CO

Assignment:Assignment:We have focused on Short-Term
regulation of blood pressure…What causes chronic
hypertension?Answer: What is the role of the
kidneys and other hormones in the long term control of blood pressure?