Embed Size (px)
Citation preview
CardiomyopathiesCardiomyopathies
Roger Kersten D.O., FACC Roger Kersten D.O., FACC
CardiomyopathiesCardiomyopathies
The cardiomyopathies are a diverse group of The cardiomyopathies are a diverse group of
disease that are not related to the usual causes of disease that are not related to the usual causes of
heart disease such as hypertension, valvular, heart disease such as hypertension, valvular,
congenital or pericardial disease.congenital or pericardial disease.
Cardiomyopathies are classified according to Cardiomyopathies are classified according to
anatomic or hemodynamic characteristics and anatomic or hemodynamic characteristics and
etiology.etiology.
CardiomyopathiesCardiomyopathiesFunctional ClassificationFunctional Classification
DilatatedDilatated (congestive, DCM, IDC) (congestive, DCM, IDC) ventricular enlargement and systolic ventricular enlargement and systolic
dysfunctiondysfunction HypertrophicHypertrophic (IHSS, HCM, HOCM) (IHSS, HCM, HOCM)
inappropriate myocardial hypertrophyinappropriate myocardial hypertrophyin the absence of HTN or aortic stenosisin the absence of HTN or aortic stenosis
RestrictiveRestrictive (infiltrative or myocardial (infiltrative or myocardial scarring)scarring) abnormal filling and diastolic functionabnormal filling and diastolic function
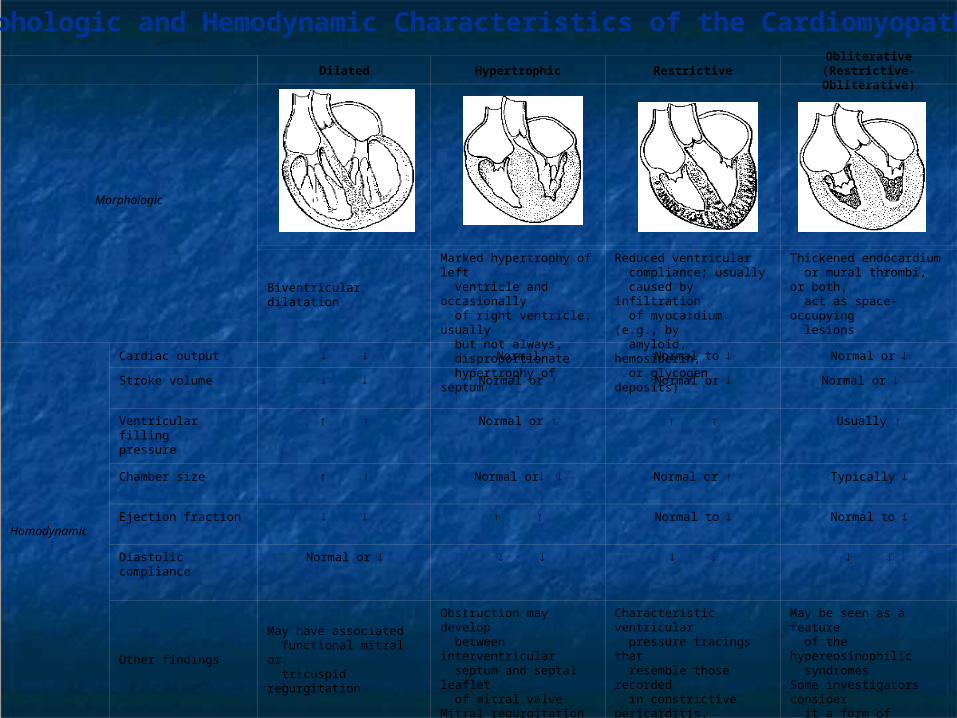
Hemodynamic
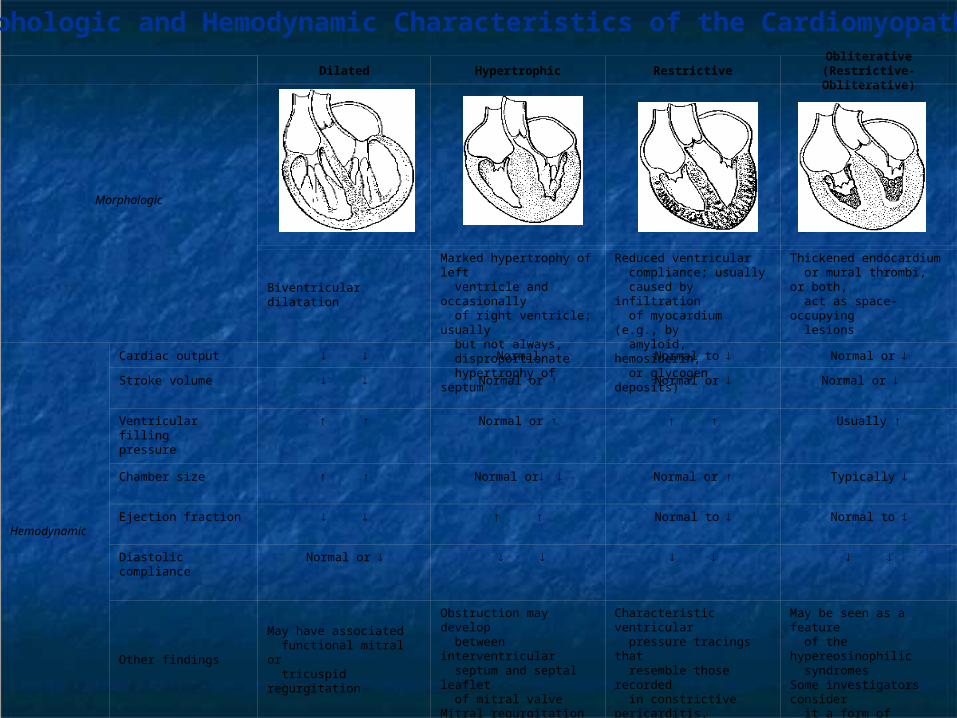
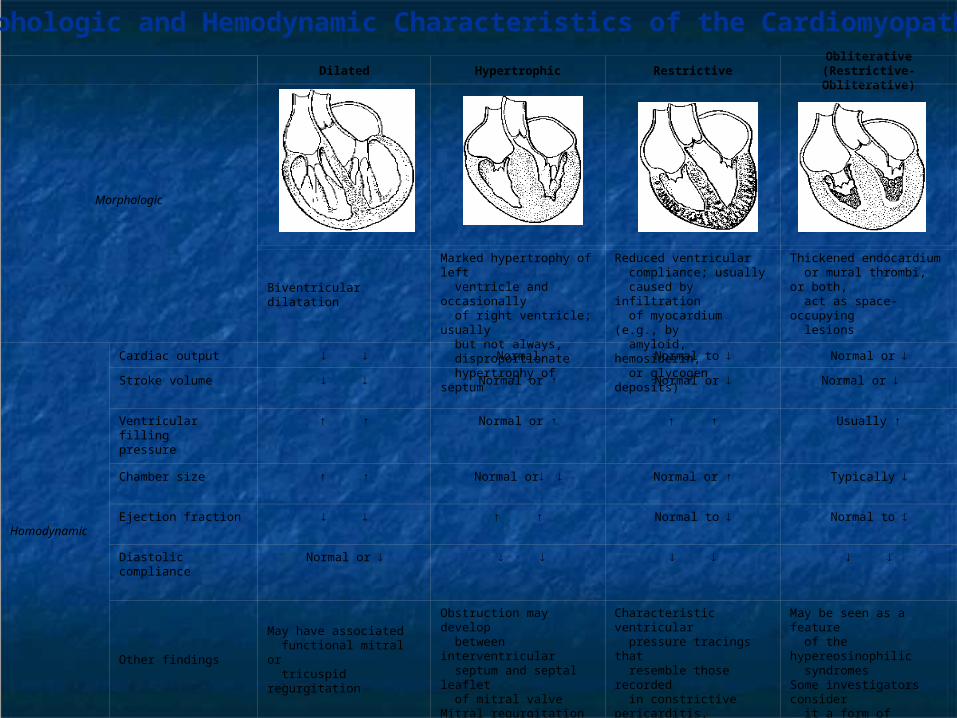
Cardiac output Normal Normal to Normal or
Stroke volume Normal or ↑ Normal or
Normal or
Ventricular fillingpressure
↑ ↑ Normal or ↑ ↑ ↑ Usually ↑
Chamber size ↑ ↑ Normal or Normal or ↑ Typically
Ejection fraction
↑ ↑ Normal to Normal to
Diastolic compliance Normal or
Other findingsMay have associated functional mitral or tricuspid regurgitation
Obstruction may develop between interventricular septum and septal leaflet of mitral valveMitral regurgitation may be present
Characteristic ventricular pressure tracings that resemble those recorded in constrictive pericarditis, with early diastolic dip- and-plateau configuration
May be seen as a feature of the hypereosinophilic syndromesSome investigators consider it a form of restrictive cardiomyopathy
Dilated Hypertrophic RestrictiveObliterative
(Restrictive-Obliterative)
Morphologic
Biventricular dilatation
Marked hypertrophy of left ventricle and occasionally of right ventricle; usually but not always, disproportionate hypertrophy of septum
Reduced ventricular compliance; usually caused by infiltration of myocardium (e.g., by amyloid, hemosiderin, or glycogen deposits)
Thickened endocardium or mural thrombi, or both, act as space-occupying lesions
Morphologic and Hemodynamic Characteristics of the Cardiomyopathies
Secondary Secondary CardiomyopathiesCardiomyopathies
When a cardiomyopathy has a definite etiology When a cardiomyopathy has a definite etiology
(e.g. sarcoidosis, infectious, scleroderma) – (e.g. sarcoidosis, infectious, scleroderma) –
signs of that process are usually evident.signs of that process are usually evident.
On rare occasions, cardiac involvement may On rare occasions, cardiac involvement may
precede other systemic manifestations.precede other systemic manifestations.
CardiomyopathiesCardiomyopathiesWHO ClassificationWHO Classification
Unknown causeUnknown cause(primary)(primary) Dilated Dilated HypertrophicHypertrophic RestrictiveRestrictive
Specific heart Specific heart muscle disease muscle disease (secondary)(secondary) InfectiveInfective MetabolicMetabolic Systemic diseaseSystemic disease HeredofamilialHeredofamilial HypersensitivityHypersensitivity ToxicToxic IschemicIschemic
Br Heart J 1980; 44:672-673
Etiologic Classification of Cardiomyopathies
Cardiomyopathies of Unknown Etiology Idiopathic dilated cardiomyopathy –DCM Peripartum cardiomyopathy -DCM* Hypertrophic cardiomyopathy -HCM Endomyocardial fibrosis -RCM Subendocardial fibroelastosis -RCM Eosinophilic endomyocardial disease -RCM (Löeffler endocarditis or fibroplastic endocarditis) Right ventricular dysplasia -DCM Idiopathic restrictive cardiomyopathy -RCM
*may be reversible
Idiopathic Dilated Idiopathic Dilated CardiomyopathyCardiomyopathy
Dilated (Congestive) Dilated (Congestive) CardiomyopathiesCardiomyopathies
IdiopathicIdiopathic SecondarySecondary PregnancyPregnancy Alcohol/DrugsAlcohol/Drugs MedicationsMedications Tachycardia inducedTachycardia induced Sleep apnea?Sleep apnea? InfectiousInfectious IschemicIschemic NutritionalNutritional ObesityObesity
Etiologic Classification of Cardiomyopathies
Dilated Cardiomyopathies of Known Etiology
InfectiousViral and rickettsial myocarditis (e.g., HIV, Coxsackie B,* CMV*)Septic (bacterial endocarditis*)SyphilisParasitic disease (e.g., Chagas disease, trichinosis, toxoplasmosis)*Bacterial toxins (e.g., diphtheria toxin- associated with heart block) or hypersensitivity (rheumatic fever)
*may be reversible
Etiologic Classification of Cardiomyopathies
Dilated Cardiomyopathies of Known Etiology Toxic (partial list)
Alcohol* (May take >10 years) Cobalt* (previously in beer) Carbon tetrachloride Carbon monoxide* Thoridazine drugs Anticancer agents (e.g. daunorubicin doxorubicin, cyclophosphamide) Antimonials, Lead, Mercury Cocaine* Antiretroviral agents (e.g., zidovudine,* dideoxyinosine*) Interferon alpha, IL2*may be reversible
Etiologic Classification of Cardiomyopathies Dilated Cardiomyopathies of Known Etiology
Systemic Diseases
Neuromuscular syndromes: Muscular dystrophies (i.e. Duchene’s progressive muscular dystrophy, end stage Friedreich’s ataxia, Limb-Girdle dystrophy of Erb, Fascioscapularhumeral disease.) Collagen vascular disease (scleroderma) Diabetic (small vessel) Hemochromatosis Hurlers, Neiman-Pic Endocrine diseases* (e.g., thyrotoxicosis, myxedema, pheochromocytoma, acromegaly, Cushings)
* may be reversible
Etiologic Classification of Cardiomyopathies
Dilated Cardiomyopathies of Known Etiology
Nutritional
Beriberi (thiamine deficiency)* Selenium deficiency* Kwashiorkor Hyophosphatemia*, Hypocalcemia* Carnitene deficiency* * Potentially reversible.
Etiologic Classification of Cardiomyopathies
Cardiomyopathies of Known Etiology
Ischemic * (hibernating myocardium)
* Potentially reversible
Congestive (Dilated) Congestive (Dilated) CardiomyopathyCardiomyopathy - Definition- Definition
A disease of unknown etiology that A disease of unknown etiology that principally affects the myocardium.principally affects the myocardium.
LV dilatation and systolic dysfunction.LV dilatation and systolic dysfunction. PathologyPathology
increased heart size and weight.increased heart size and weight. ventricular dilatation, normal wall ventricular dilatation, normal wall
thickness.thickness. heart dysfunction out of portion to fibrosis.heart dysfunction out of portion to fibrosis.
Secondary Secondary Congestive (Dilated) Congestive (Dilated)
CardiomyopathyCardiomyopathy Infectious and Autoimmune processes Infectious and Autoimmune processes
(Myocarditis)(Myocarditis) Coxsackie B etc.Coxsackie B etc.
Autoimmune processesAutoimmune processes
Acute Myocarditis vs. Congestive Acute Myocarditis vs. Congestive
CardiomyopathyCardiomyopathy Fever with CHFFever with CHF
PericarditisPericarditis
Elevated CPK – MB , TnT ( less than 30% of myocarditis)Elevated CPK – MB , TnT ( less than 30% of myocarditis)
Dilated (Congestive) Dilated (Congestive) CardiomyopathyCardiomyopathy
A familial form may be present in 10 – 30%A familial form may be present in 10 – 30%
Characterized by diminished myocardial Characterized by diminished myocardial
contractilitycontractility Reflected in reduction of systolic function. ( EF Reflected in reduction of systolic function. ( EF , ,
LV EDP LV EDP , SV , SV , C.O , C.O ) )
RV dysplasia characterized by RV failure and VTRV dysplasia characterized by RV failure and VT
Dilated Dilated (Congestive)Cardiomyopathy(Congestive)Cardiomyopathy
Clinical ManifestationsClinical Manifestations Highest incidence in middle ageHighest incidence in middle age
blacks 2x more frequent than whitesblacks 2x more frequent than whites men 3x more frequent than womenmen 3x more frequent than women
symptoms may be gradual in onsetsymptoms may be gradual in onset acute presentation acute presentation
misdiagnosed as viral URI in young adultsmisdiagnosed as viral URI in young adults uncommon to find specific myocardial uncommon to find specific myocardial
disease on endomyocardial biopsydisease on endomyocardial biopsy
Dilated (Congestive) Dilated (Congestive) CardiomyopathyCardiomyopathy
Clinical FeaturesClinical Features Dyspnea, fatigue, edema, orthopnea.Dyspnea, fatigue, edema, orthopnea. Palpitations, occasionally syncope.Palpitations, occasionally syncope. Systemic and pulmonary emboli (+4 Systemic and pulmonary emboli (+4
%/year.)%/year.) Atypical chest pain ( 1/3 of patients)Atypical chest pain ( 1/3 of patients)
Physical FindingPhysical Finding Reflects the variable severity of CHF.Reflects the variable severity of CHF.
Diagnostic StudiesDiagnostic Studies CXR, EKG, Echocardiogram (segmental vs CXR, EKG, Echocardiogram (segmental vs
global asynergy)global asynergy) MRI (Dysplastic RV Cardiomyopathy)MRI (Dysplastic RV Cardiomyopathy) Gallium 67 (sarcoidosis, myocarditis)Gallium 67 (sarcoidosis, myocarditis)
Cardiac Catheterization (r/o CAD, check Cardiac Catheterization (r/o CAD, check pressures, usually biopsy not indicated.) pressures, usually biopsy not indicated.)
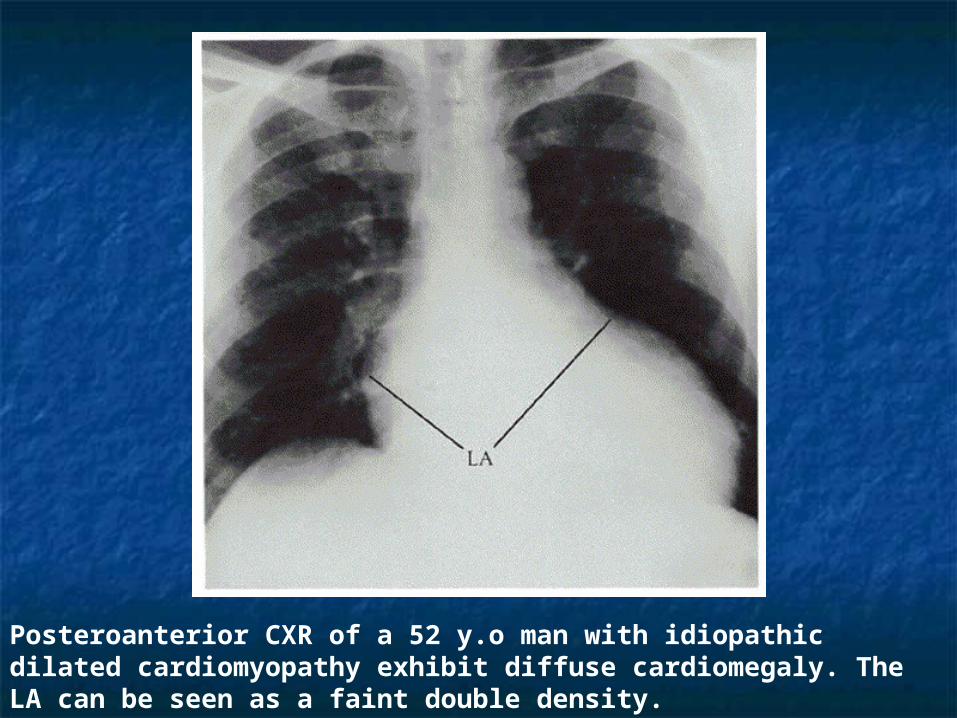
Posteroanterior CXR of a 52 y.o man with idiopathic dilated cardiomyopathy exhibit diffuse cardiomegaly. The LA can be seen as a faint double density.
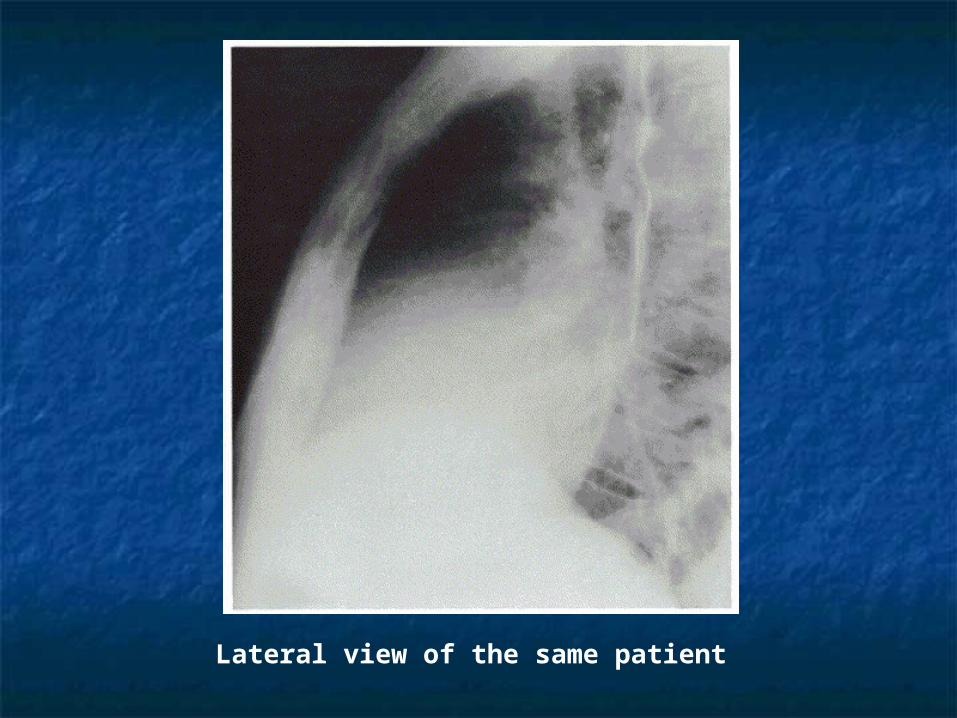
Lateral view of the same patient
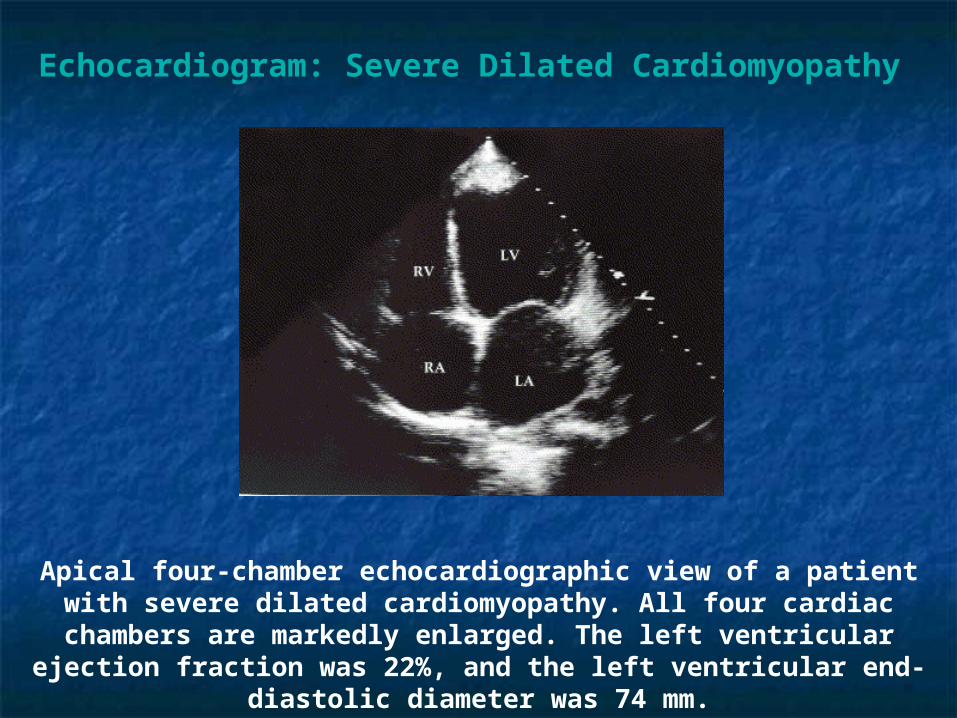
Echocardiogram: Severe Dilated Cardiomyopathy
Apical four-chamber echocardiographic view of a patient with severe dilated cardiomyopathy. All four cardiac chambers are markedly enlarged. The left ventricular ejection fraction was 22%, and the left ventricular end-diastolic
diameter was 74 mm.
Dilated (Congestive) Dilated (Congestive) CardiomyopathyCardiomyopathy
Endomyocardial Biopsy Endomyocardial Biopsy
Low diagnostic yieldLow diagnostic yield
Uncertainty regarding role of Uncertainty regarding role of
immunosuppressive therapyimmunosuppressive therapy
Led most investigators to abandon it routine useLed most investigators to abandon it routine use
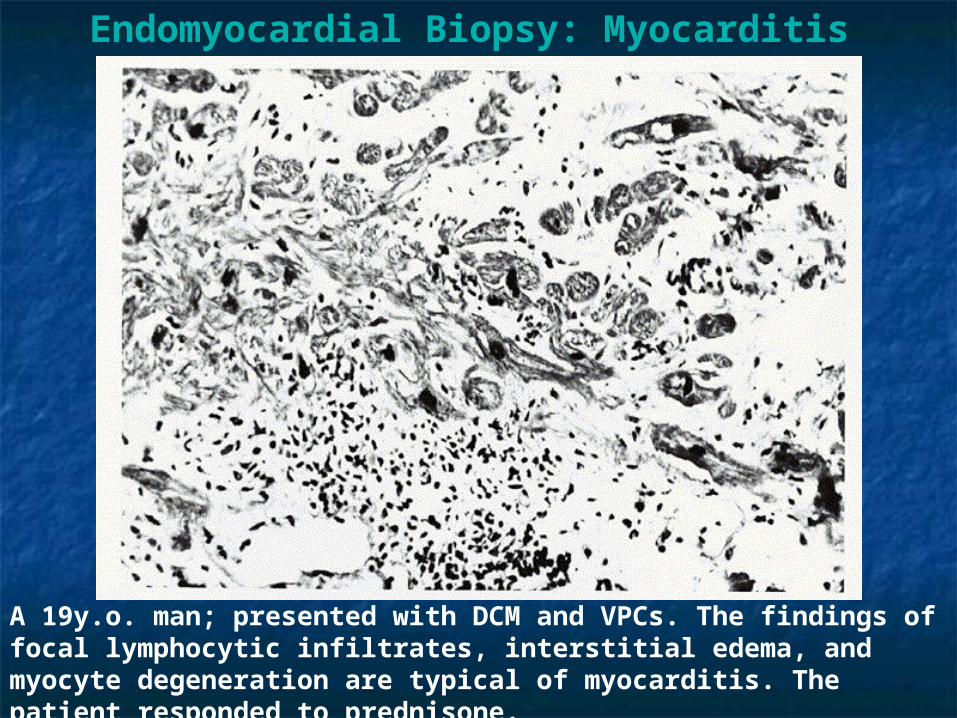
Endomyocardial Biopsy: Myocarditis
A 19y.o. man; presented with DCM and VPCs. The findings of focal lymphocytic infiltrates, interstitial edema, and myocyte degeneration are typical of myocarditis. The patient responded to prednisone.
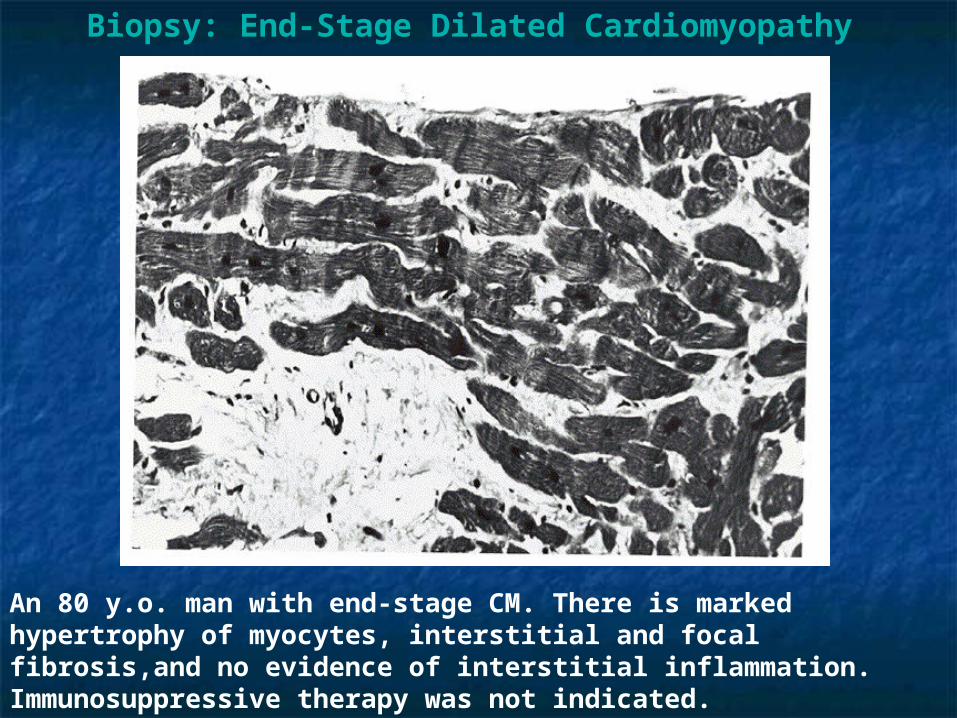
Biopsy: End-Stage Dilated Cardiomyopathy
An 80 y.o. man with end-stage CM. There is marked hypertrophy of myocytes, interstitial and focal fibrosis,and no evidence of interstitial inflammation. Immunosuppressive therapy was not indicated.
Dilated Cardiomyopathy Dilated Cardiomyopathy (DCM)(DCM)
Course and PrognosisCourse and Prognosis The most common complication of DCM is progressive CHF – The most common complication of DCM is progressive CHF –
the cause of death in 50 – 75%the cause of death in 50 – 75% Sudden death (SD) by arrhythmia is common especially in Sudden death (SD) by arrhythmia is common especially in
patients with complex ventricular ectopy and severe LV patients with complex ventricular ectopy and severe LV dysfunction.dysfunction.
Systemic / pulmonary embolism is found at autopsy in 50% of Systemic / pulmonary embolism is found at autopsy in 50% of patients with DCM – emboli can cause catastrophic patients with DCM – emboli can cause catastrophic complications but rarely death.complications but rarely death.
Prognosis varies considerably from fulminent cases that result Prognosis varies considerably from fulminent cases that result in death within a few weeks, or conversely some patients do in death within a few weeks, or conversely some patients do remarkably well for years. Previously, most died within 5 years.remarkably well for years. Previously, most died within 5 years.
Spontaneous improvement in LV function occurs in 20 – 40%, Spontaneous improvement in LV function occurs in 20 – 40%, most frequently within 6 months.most frequently within 6 months.
A peak 0A peak 022 uptake less than 14 ml/kg /min predicts 1 year uptake less than 14 ml/kg /min predicts 1 year survival of 70%. Consider cardiac transplant if V0survival of 70%. Consider cardiac transplant if V02.2.
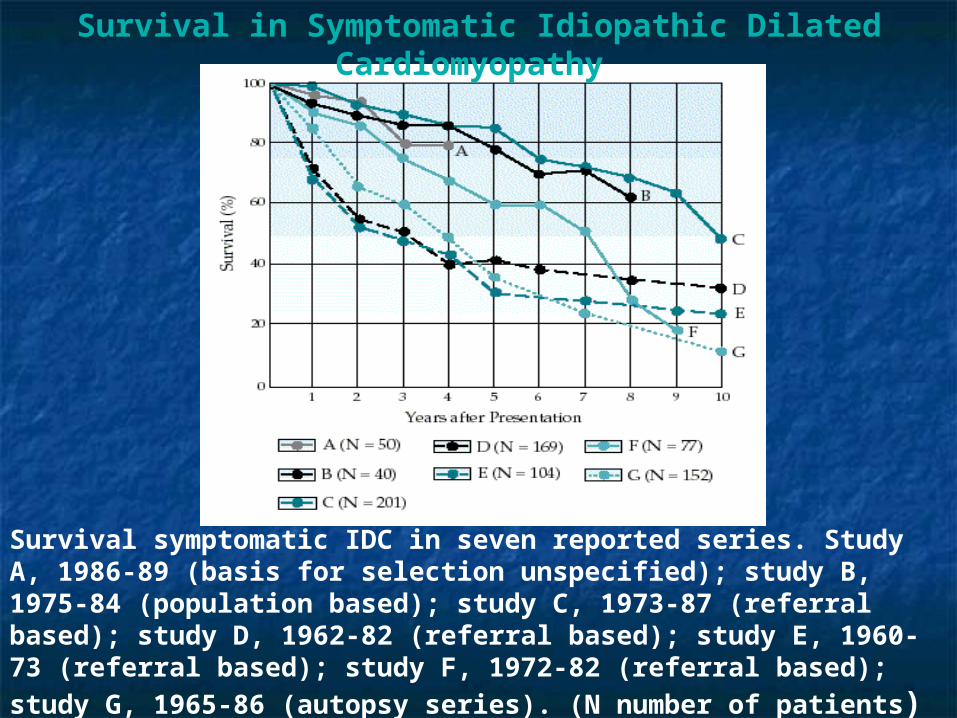
Survival in Symptomatic Idiopathic Dilated Cardiomyopathy
Survival symptomatic IDC in seven reported series. Study A, 1986-89 (basis for selection unspecified); study B, 1975-84 (population based); study C, 1973-87 (referral based); study D, 1962-82 (referral based); study E, 1960-73 (referral based); study F, 1972-82 (referral based); study G, 1965-86 (autopsy series). (N
number of patients)
Dilated Cardiomyopathy Dilated Cardiomyopathy Medical TreatmentMedical Treatment
Limit activity based on functional statusLimit activity based on functional status Salt restriction of a 2gm NaSalt restriction of a 2gm Na++ (5gm NaCl) diet (5gm NaCl) diet Fluid restriction for significant low Na+Fluid restriction for significant low Na+ Initiate combination medical therapyInitiate combination medical therapy
ACE inhibitors (lisinopril, enalopril, captopril, etc.) Beta ACE inhibitors (lisinopril, enalopril, captopril, etc.) Beta blockers (carvedilol, long acting metoprolol, bisoprolol) blockers (carvedilol, long acting metoprolol, bisoprolol)
Loop diuretics (toresemide, furosemide) for symptoms of Loop diuretics (toresemide, furosemide) for symptoms of fluid overload.fluid overload.
ARB (candesartan, valsartan)ARB (candesartan, valsartan) Aldosterone blockers (spironolactone, eplerenone)Aldosterone blockers (spironolactone, eplerenone) Digoxin (to treat symptoms)Digoxin (to treat symptoms) Hydralazine / nitrate combination (if unable to tolerate Hydralazine / nitrate combination (if unable to tolerate
ACE inhibition)ACE inhibition)
Dilated Cardiomyopathy Dilated Cardiomyopathy Medical TreatmentMedical Treatment
Anticoagulation therapy is controversial in idiopathic Anticoagulation therapy is controversial in idiopathic
cardiomyopathy. Consider with marked right sided cardiomyopathy. Consider with marked right sided
failure and/or EF < 30. Use if embolic event has failure and/or EF < 30. Use if embolic event has
already occurred.already occurred. Antiarrhythmics: arrhythmias are common however, Antiarrhythmics: arrhythmias are common however,
empiric antiarrhythmic drug therapy has been empiric antiarrhythmic drug therapy has been
disappointing. Only amiodarone seems relatively disappointing. Only amiodarone seems relatively
safe but without clear mortality benefit in DCM.safe but without clear mortality benefit in DCM.
Dilated Cardiomyopathy Dilated Cardiomyopathy Device TreatmentDevice Treatment
SAECG and EP are not reliable in assessing prognosis or SAECG and EP are not reliable in assessing prognosis or
guiding antiarrhythimic therapy in patients with DCM. guiding antiarrhythimic therapy in patients with DCM. Defibrillator (AICD) is indicated in patients with Defibrillator (AICD) is indicated in patients with
cardiomyopathy and EF<30%. SCUD-Heft demonstrated cardiomyopathy and EF<30%. SCUD-Heft demonstrated
mortality benefit in patients with EF<30% of either mortality benefit in patients with EF<30% of either
ischemic or nonischemic etiology.ischemic or nonischemic etiology. Biventricular pacing restores synchronous LV contraction Biventricular pacing restores synchronous LV contraction
and decreases heart failure symptoms when used in and decreases heart failure symptoms when used in
combination with medical therapy. Used in combination combination with medical therapy. Used in combination
with AICD.with AICD. If symptoms are still not controlled, may consider If symptoms are still not controlled, may consider
transplant.transplant.
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
Hypertrophic Hypertrophic Cardiomyopathy*Cardiomyopathy*
Obstructive Obstructive (HOCM. Labile and (HOCM. Labile and associated with associated with mitral valve mitral valve pathology.)pathology.)
Non ObstructiveNon Obstructive Concentric Concentric Mid ventricular Mid ventricular Apical Apical
* The vast majority of cases of hypertrophic cardiomyopathy result from specific defects in the genes regulating the formation of cardiac muscle This defect is either sporadic or hereditary in 50% of cases (autosomal dominant).
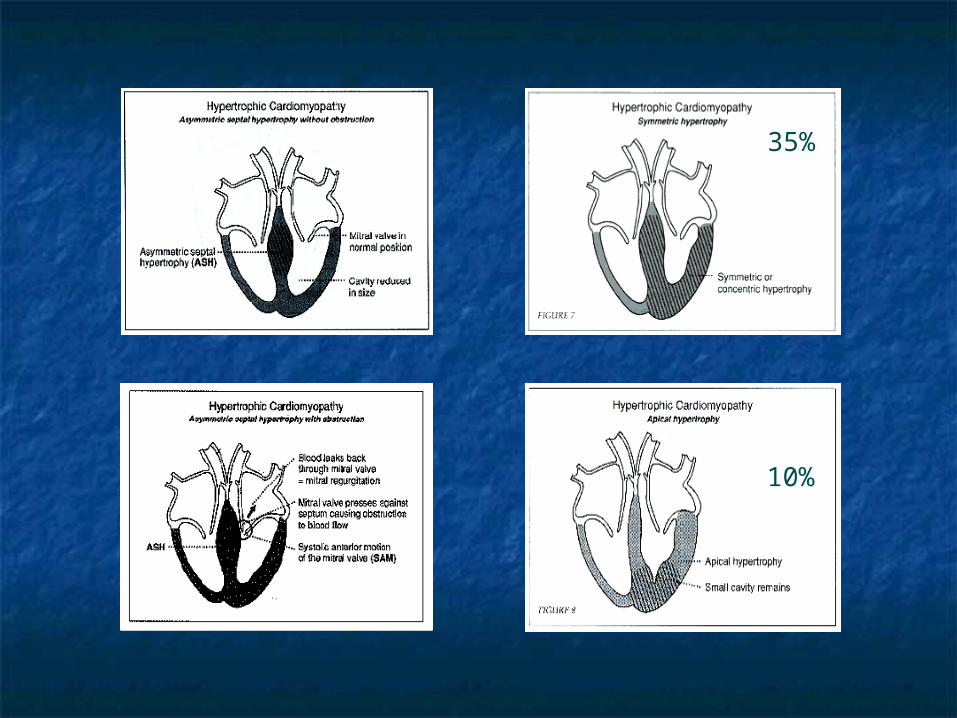
35%
10%
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
The hallmark of the disease is unexplained myocardial The hallmark of the disease is unexplained myocardial hypertrophy or hypertrophy out of proportion to the hypertrophy or hypertrophy out of proportion to the hemodynamic load.hemodynamic load.
Frequently inherited with autosomal dominant Frequently inherited with autosomal dominant transmission and highly variable penetrance.transmission and highly variable penetrance.
In the obstructive form: ASH, SAM, MR.In the obstructive form: ASH, SAM, MR. Obstruction may be fixed or labile.Obstruction may be fixed or labile. Hyper-contractile LV (EF 80 – 90%) with reduced ESV.Hyper-contractile LV (EF 80 – 90%) with reduced ESV. Reduced LV diastolic compliance. (cause of NEF-CHF)Reduced LV diastolic compliance. (cause of NEF-CHF) Factors that provoke or increase/decrease obstruction:Factors that provoke or increase/decrease obstruction:
Change in contractile state.Change in contractile state. Change in chamber size (preload and after load)Change in chamber size (preload and after load)
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
Usually assymetrical hypertrophy with the Usually assymetrical hypertrophy with the septum:posterior wall thickness >1.3:1.0 (although septum:posterior wall thickness >1.3:1.0 (although this may occasionally be seen in concentric this may occasionally be seen in concentric hypertrophy.)hypertrophy.)
Apical and mid ventricular variants are unusual. Apical and mid ventricular variants are unusual. The apical pattern may be characterized by giant T The apical pattern may be characterized by giant T wave inversions on ECG.wave inversions on ECG.
Hypertensive HCM may be seen in elderly Hypertensive HCM may be seen in elderly hypertensive pts and is characterized by severe hypertensive pts and is characterized by severe concentric LVH out of proportion to the degree of concentric LVH out of proportion to the degree of hypertension.hypertension.
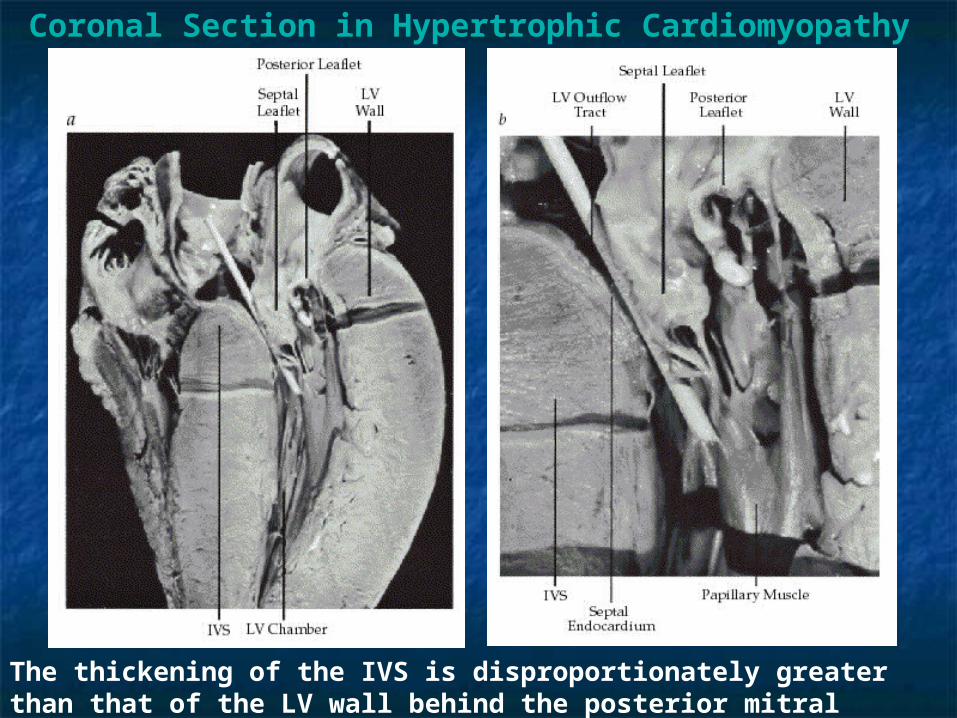
Coronal Section in Hypertrophic Cardiomyopathy
The thickening of the IVS is disproportionately greater than that of the LV wall behind the posterior mitral leaflet. The LV chamber is small and elongated.
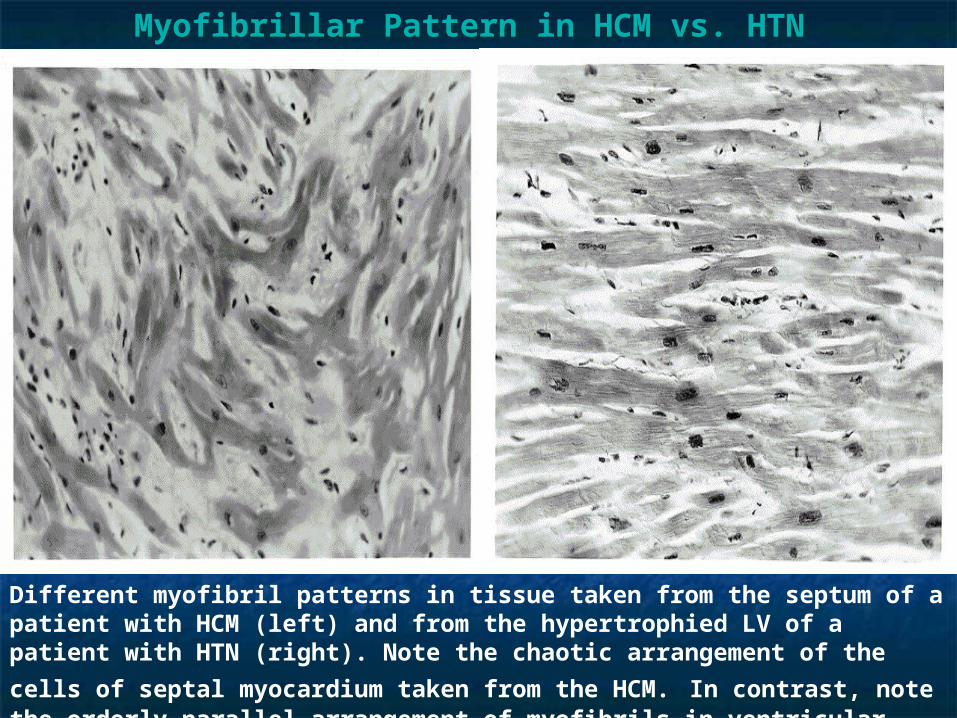
Myofibrillar Pattern in HCM vs. HTN
Different myofibril patterns in tissue taken from the septum of a patient with HCM (left) and from the hypertrophied LV of a patient with HTN (right). Note the chaotic
arrangement of the cells of septal myocardium taken from the HCM. In contrast, note the orderly parallel arrangement of myofibrils in ventricular myocardium in the HTN patient.
Homodynamic
Cardiac output Normal Normal to Normal or
Stroke volume Normal or ↑ Normal or
Normal or
Ventricular fillingpressure
↑ ↑ Normal or ↑ ↑ ↑ Usually ↑
Chamber size ↑ ↑ Normal or Normal or ↑ Typically
Ejection fraction
↑ ↑ Normal to Normal to
Diastolic compliance Normal or
Other findingsMay have associated functional mitral or tricuspid regurgitation
Obstruction may develop between interventricular septum and septal leaflet of mitral valveMitral regurgitation may be present
Characteristic ventricular pressure tracings that resemble those recorded in constrictive pericarditis, with early diastolic dip- and-plateau configuration
May be seen as a feature of the hypereosinophilic syndromesSome investigators consider it a form of restrictive cardiomyopathy
Dilated Hypertrophic RestrictiveObliterative
(Restrictive-Obliterative)
Morphologic
Biventricular dilatation
Marked hypertrophy of left ventricle and occasionally of right ventricle; usually but not always, disproportionate hypertrophy of septum
Reduced ventricular compliance; usually caused by infiltration of myocardium (e.g., by amyloid, hemosiderin, or glycogen deposits)
Thickened endocardium or mural thrombi, or both, act as space-occupying lesions
Morphologic and Hemodynamic Characteristics of the Cardiomyopathies
PathophysiologyPathophysiology
SystoleSystole Dynamic outflow tract gradient. May not be present Dynamic outflow tract gradient. May not be present
at rest but may provoke with standing, exercise or at rest but may provoke with standing, exercise or inotropic drugs.inotropic drugs.
DiastoleDiastole Impaired diastolic filling, Impaired diastolic filling, filling pressure of LV. filling pressure of LV.
Myocardial ischemiaMyocardial ischemia Muscle mass, filling pressure, OMuscle mass, filling pressure, O22 demand demand Coronary vasodilator reserve, capillary densityCoronary vasodilator reserve, capillary density Abnormal intramural coronary arteries with systolic Abnormal intramural coronary arteries with systolic
compression of arteries.compression of arteries.
Hypertrophic Cardiomyopathy
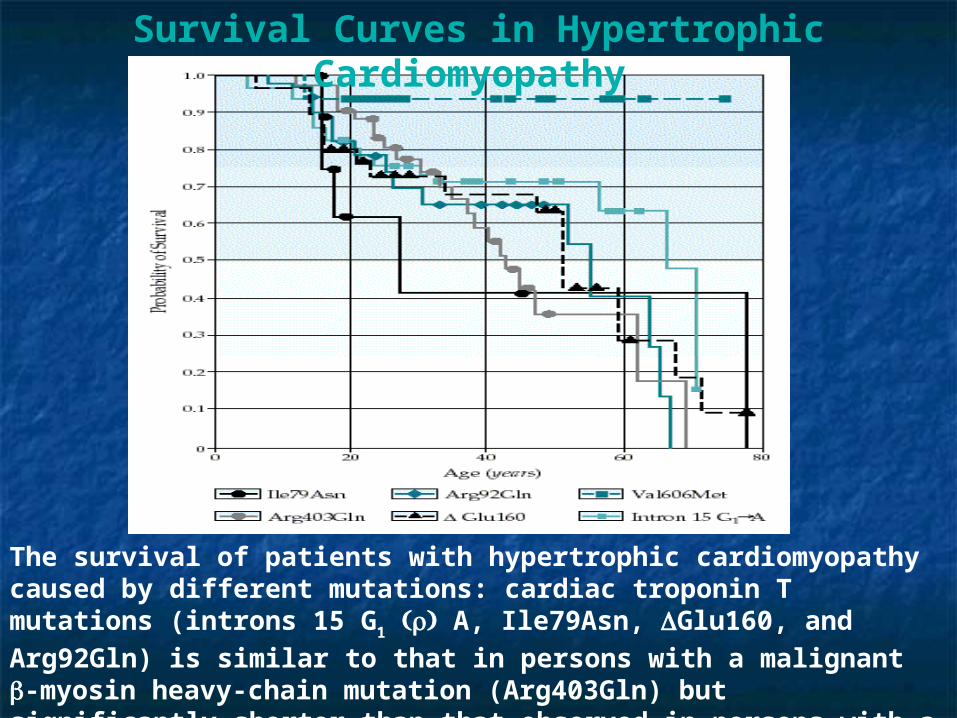
Survival Curves in Hypertrophic Cardiomyopathy
The survival of patients with hypertrophic cardiomyopathy caused by different mutations: cardiac troponin T mutations (introns 15 G1 A, Ile79Asn, Glu160,
and Arg92Gln) is similar to that in persons with a malignant -myosin heavy-chain mutation (Arg403Gln) but significantly shorter than that observed in persons with a benign myosin mutation (Val606Met).
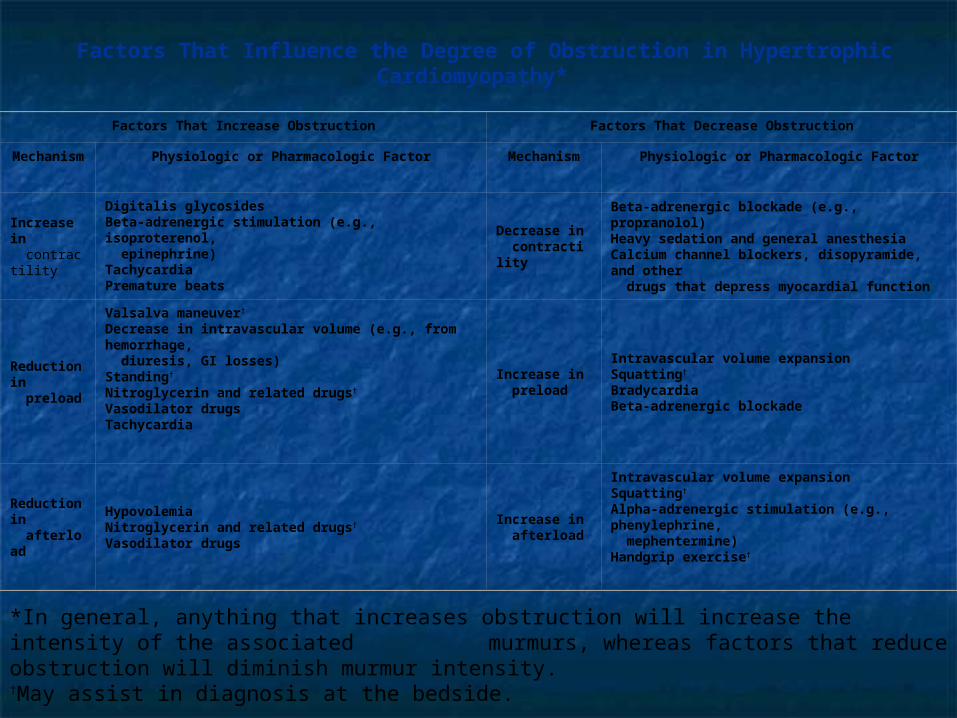
Factors That Influence the Degree of Obstruction in Hypertrophic Cardiomyopathy*
Factors That Increase Obstruction Factors That Decrease Obstruction
Mechanism Physiologic or Pharmacologic Factor Mechanism Physiologic or Pharmacologic Factor
Increase in contractility
Digitalis glycosidesBeta-adrenergic stimulation (e.g., isoproterenol, epinephrine)TachycardiaPremature beats
Decrease in contractility
Beta-adrenergic blockade (e.g., propranolol)Heavy sedation and general anesthesiaCalcium channel blockers, disopyramide, and other drugs that depress myocardial function
Reduction in preload
Valsalva maneuver†
Decrease in intravascular volume (e.g., from hemorrhage, diuresis, GI losses)Standing†
Nitroglycerin and related drugs†
Vasodilator drugsTachycardia
Increase in preload
Intravascular volume expansionSquatting†
BradycardiaBeta-adrenergic blockade
Reduction in afterload
HypovolemiaNitroglycerin and related drugs†
Vasodilator drugs
Increase in afterload
Intravascular volume expansionSquatting†
Alpha-adrenergic stimulation (e.g., phenylephrine, mephentermine)Handgrip exercise†
*In general, anything that increases obstruction will increase the intensity of the associated murmurs, whereas factors that reduce obstruction will diminish murmur intensity.
†May assist in diagnosis at the bedside.
Hypertrophic Cardiomyopathy Hypertrophic Cardiomyopathy DiagnosisDiagnosis
SymptomsSymptoms Angina (Recumbent position)Angina (Recumbent position) Syncope (After exercise, arrhythmia)Syncope (After exercise, arrhythmia) Palpitations (AF, VT)Palpitations (AF, VT) CHF (Loss of atrial contraction, AF with fast response)CHF (Loss of atrial contraction, AF with fast response) Systemic embolismSystemic embolism Sudden Death. (Even in asymptomatic patients.) Lethal arrhythmia Sudden Death. (Even in asymptomatic patients.) Lethal arrhythmia
more likely in young.more likely in young.
Physical examinationPhysical examination EKG (May have LVH pattern, preexcitation, abnormal Q waves, EKG (May have LVH pattern, preexcitation, abnormal Q waves,
giant T waves.) giant T waves.) Echocardiography (LVH concentric, apical, ASH, Echocardiography (LVH concentric, apical, ASH,
septum:posterior > 1.3:1, SAM, “lobster claw” outflow tracing.)septum:posterior > 1.3:1, SAM, “lobster claw” outflow tracing.) Cardiac Cath (Pressure tracings demonstrating outflow tract Cardiac Cath (Pressure tracings demonstrating outflow tract
obstruction.)obstruction.)
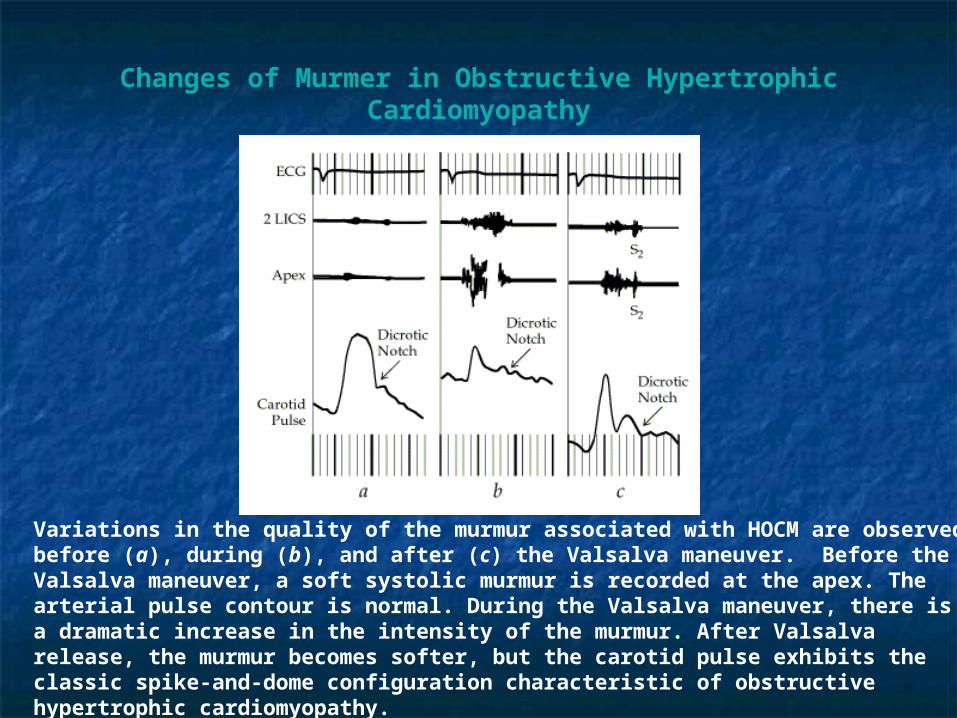
Changes of Murmer in Obstructive Hypertrophic Cardiomyopathy
Variations in the quality of the murmur associated with HOCM are observed before (a), during (b), and after (c) the Valsalva maneuver. Before the Valsalva maneuver, a soft systolic murmur is recorded at the apex. The arterial pulse contour is normal. During the Valsalva maneuver, there is a dramatic increase in the intensity of the murmur. After Valsalva release, the murmur becomes softer, but the carotid pulse exhibits the classic spike-and-dome configuration characteristic of obstructive hypertrophic cardiomyopathy.
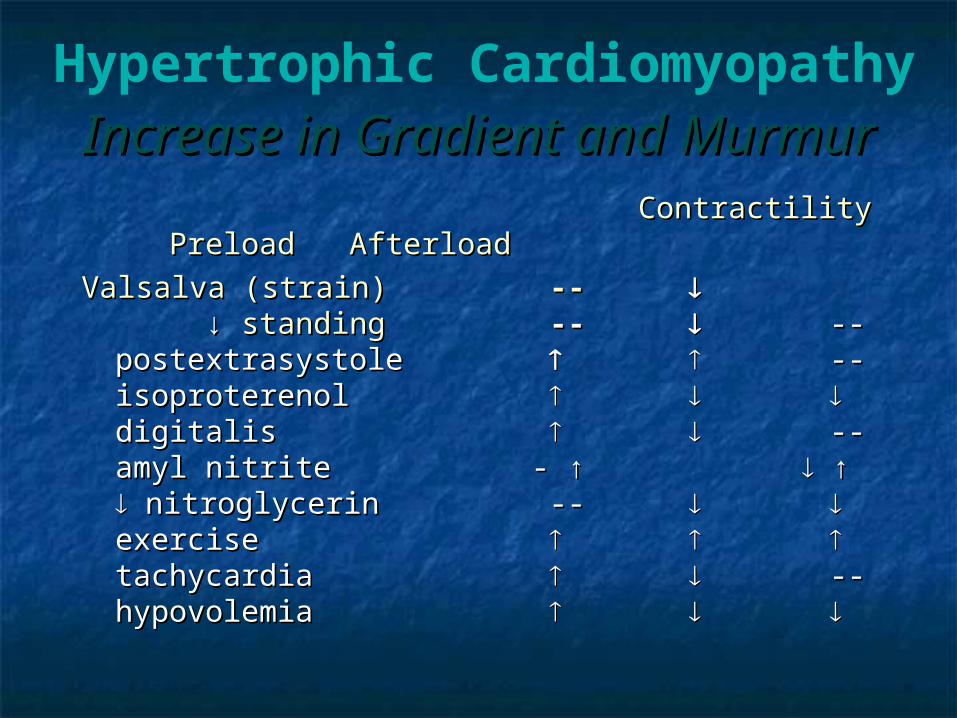
Increase in Gradient and Increase in Gradient and MurmurMurmur
Contractility Preload Contractility Preload Afterload Afterload
Valsalva (strain)Valsalva (strain) -- -- ↓↓ standingstanding -- -- ----postextrasystolepostextrasystole -- -- isoproterenolisoproterenol digitalisdigitalis ----amyl nitriteamyl nitrite - ↑ - ↑ ↑ ↑ nitroglycerinnitroglycerin -- -- exerciseexercise tachycardiatachycardia ----hypovolemiahypovolemia
Hypertrophic Cardiomyopathy
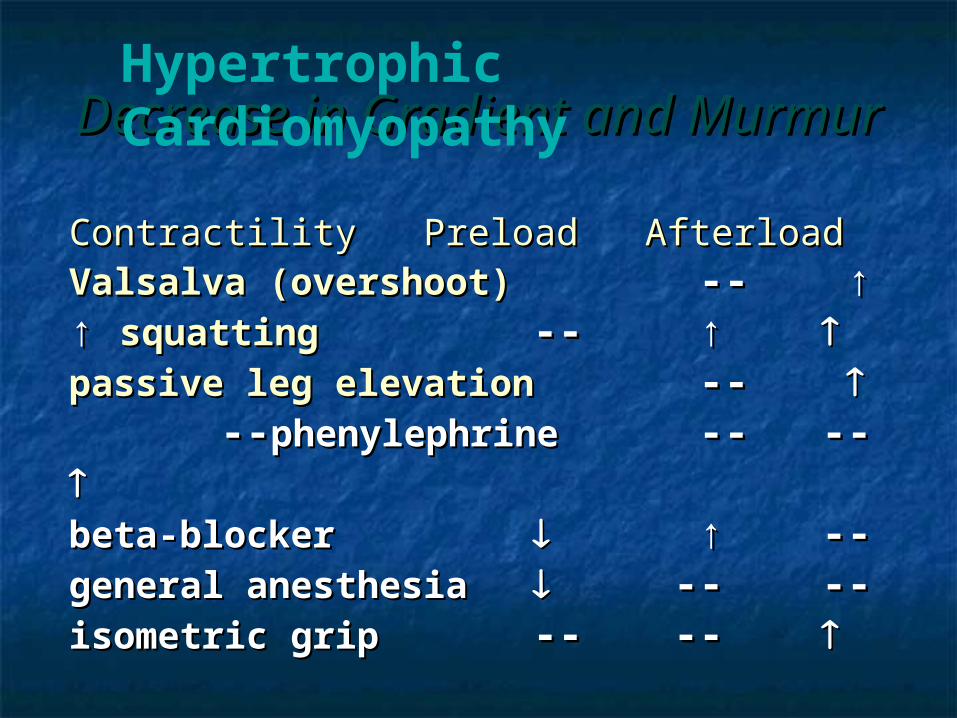
Decrease in Gradient and Decrease in Gradient and MurmurMurmur
Contractility Preload Contractility Preload AfterloadAfterload Valsalva (overshoot)Valsalva (overshoot) -- -- ↑ ↑ ↑ ↑ squattingsquatting -- -- ↑ ↑ passive leg elevationpassive leg elevation -- -- -- --phenylephrinephenylephrine -- -- ---- beta-blockerbeta-blocker ↑ ↑ -- -- general anesthesiageneral anesthesia -- -- ----isometric gripisometric grip -- -- -- --
Hypertrophic Cardiomyopathy
HypertrophicHypertrophic CardiomyopathyCardiomyopathy HCM vs HCM vs
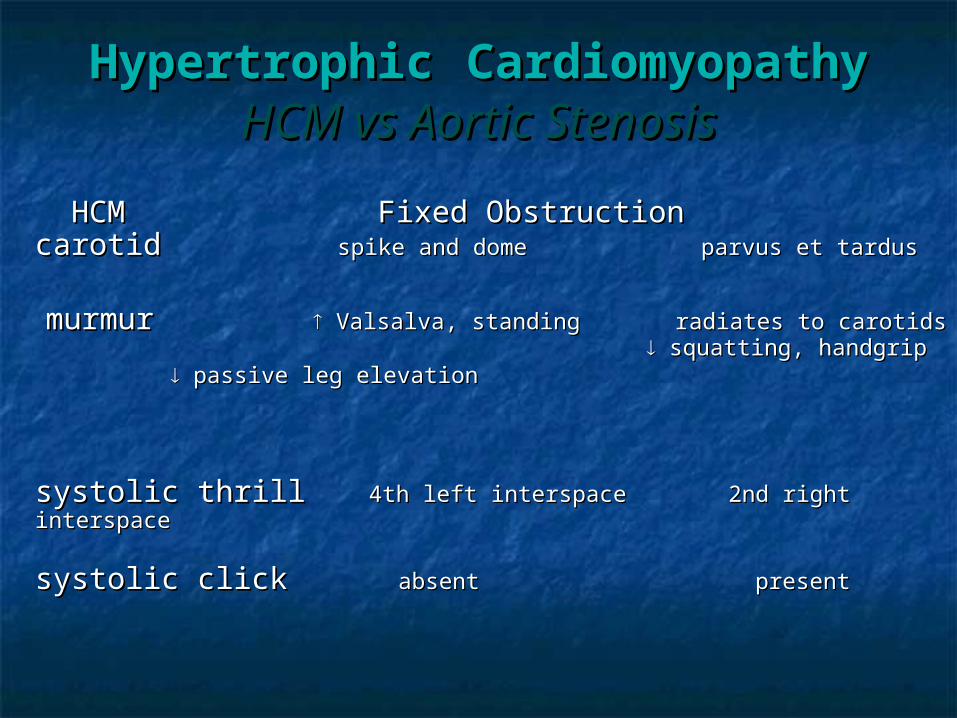
Aortic StenosisAortic Stenosis HCM Fixed Obstruction HCM Fixed Obstruction
carotid carotid spike and domespike and dome parvus et tardus parvus et tardus
murmurmurmur Valsalva, standing radiates to carotids Valsalva, standing radiates to carotids squatting, handgrip squatting, handgrip
passive leg elevation passive leg elevation
systolic thrillsystolic thrill 4th left interspace4th left interspace 2nd right interspace 2nd right interspace
systolic clicksystolic click absentabsent present present
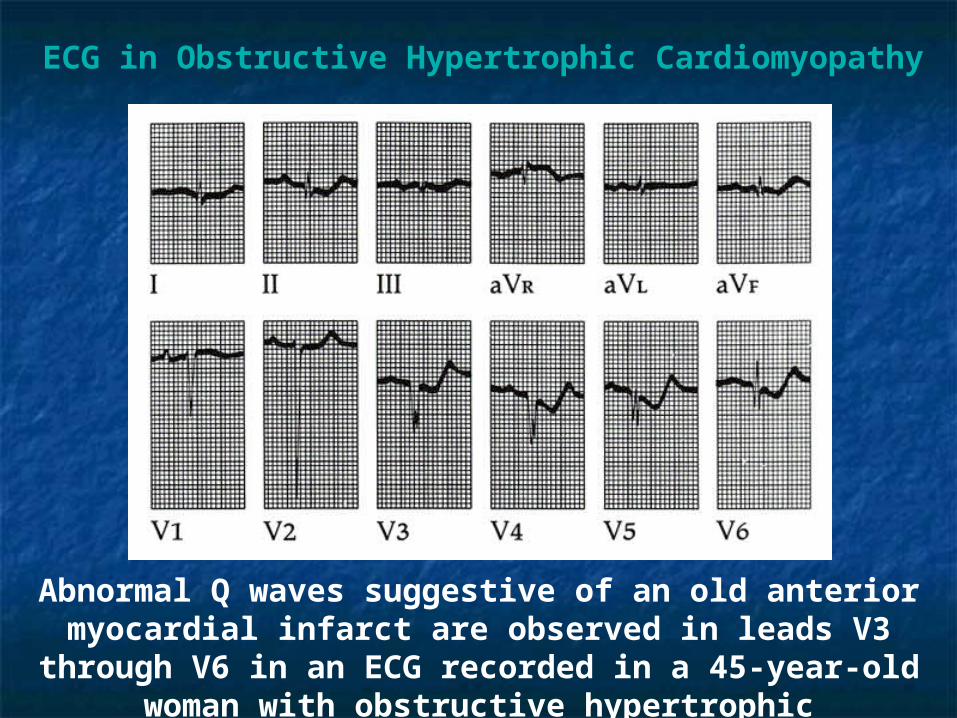
ECG in Obstructive Hypertrophic Cardiomyopathy
Abnormal Q waves suggestive of an old anterior myocardial infarct are observed in leads V3 through V6 in an ECG recorded in a 45-year-old woman with obstructive hypertrophic cardiomyopathy.
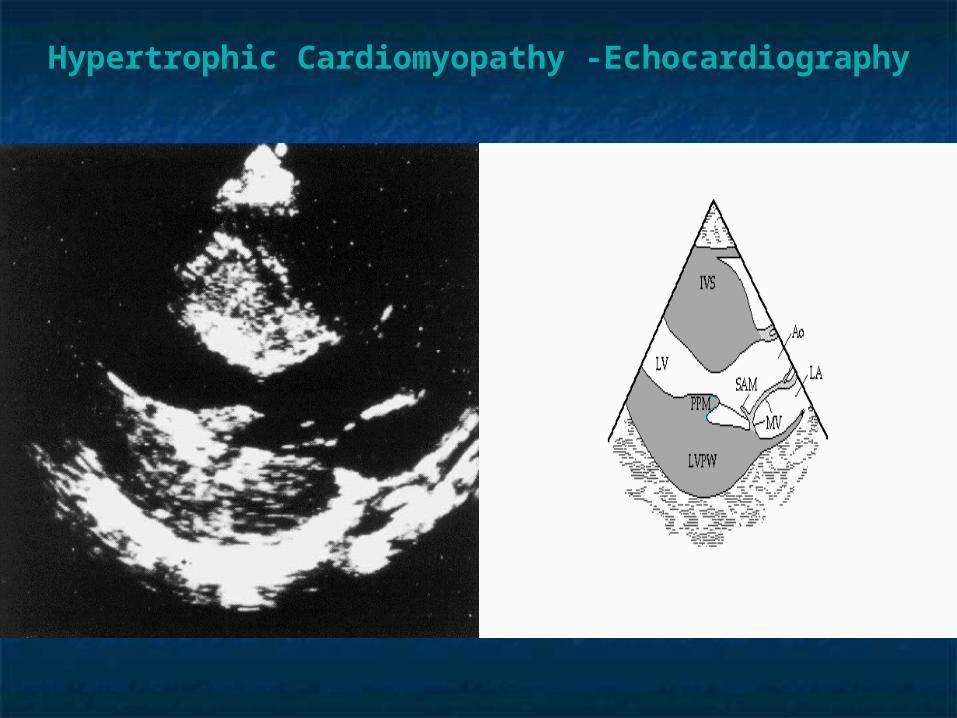
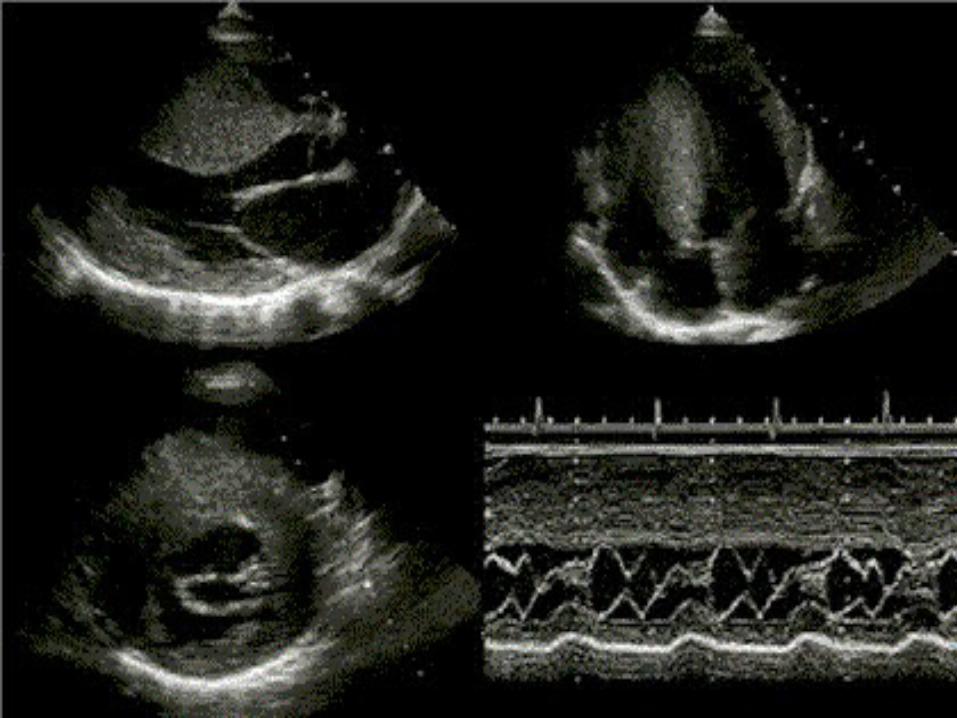
Hypertrophic Cardiomyopathy -Echocardiography
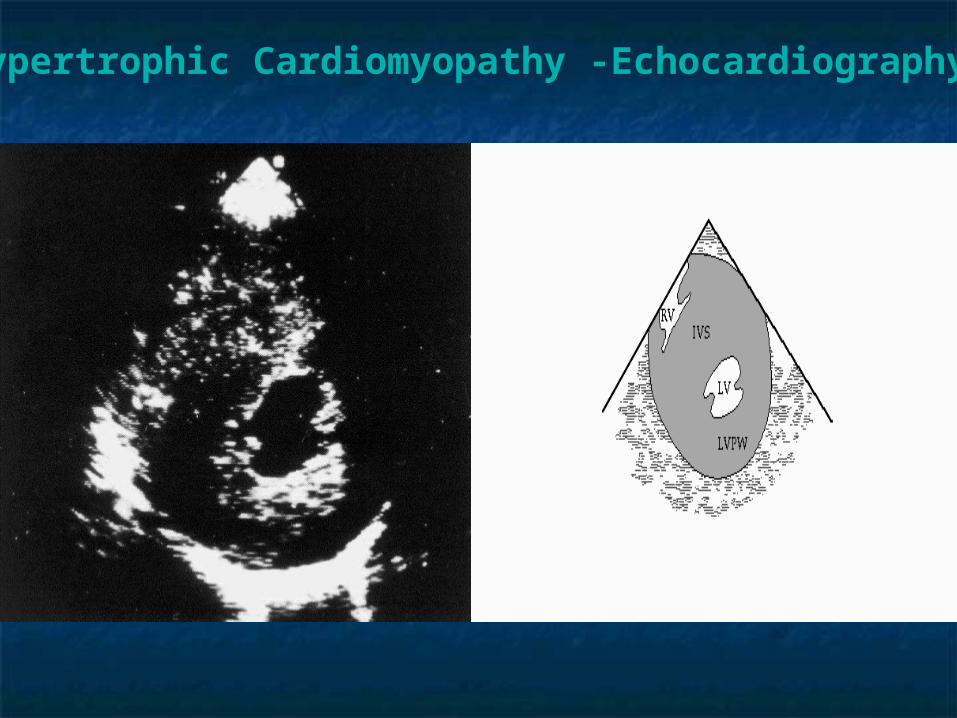
Hypertrophic Cardiomyopathy -Echocardiography
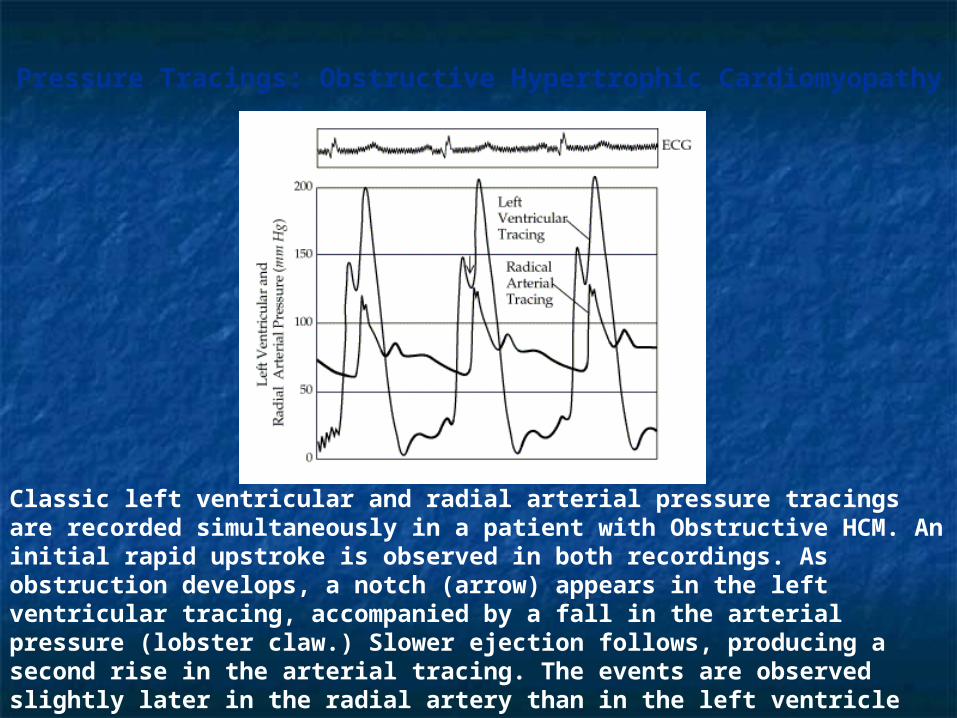
Pressure Tracings: Obstructive Hypertrophic Cardiomyopathy
Classic left ventricular and radial arterial pressure tracings are recorded simultaneously in a patient with Obstructive HCM. An initial rapid upstroke is observed in both recordings. As obstruction develops, a notch (arrow) appears in the left ventricular tracing, accompanied by a fall in the arterial pressure (lobster claw.) Slower ejection follows, producing a second rise in the arterial tracing. The events are observed slightly later in the radial artery than in the left ventricle because some delay occurs in the transmission of the impulse to the artery.
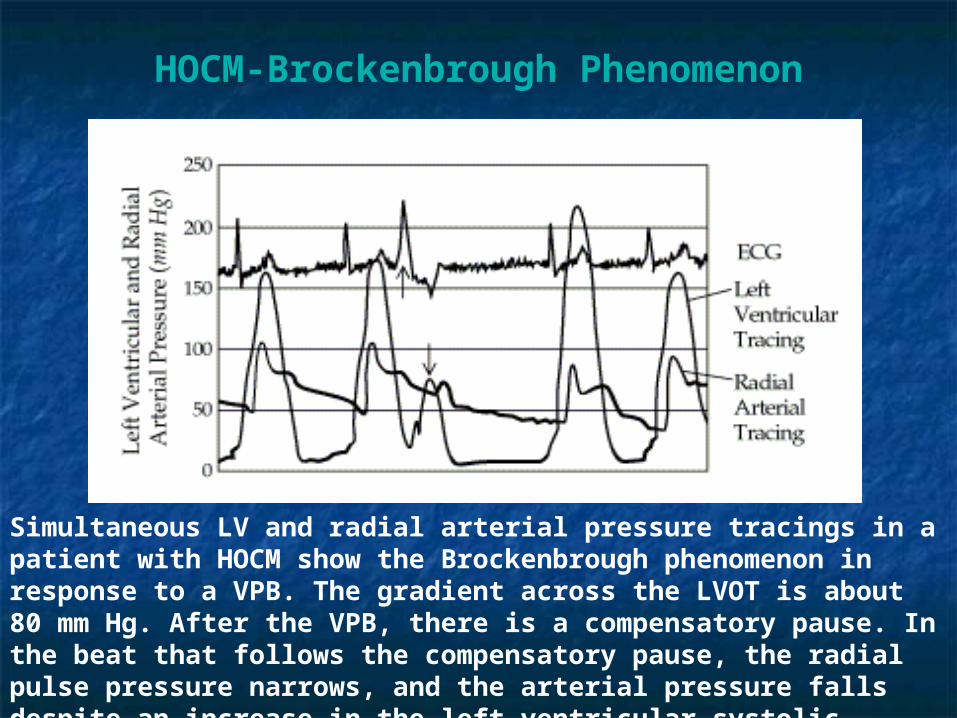
HOCM-Brockenbrough Phenomenon
Simultaneous LV and radial arterial pressure tracings in a patient with HOCM show the Brockenbrough phenomenon in response to a VPB. The gradient across the LVOT is about 80 mm Hg. After the VPB, there is a compensatory pause. In the beat that follows the compensatory pause, the radial pulse pressure narrows, and the arterial pressure falls despite an increase in the left ventricular systolic pressure.
Clinical ManifestationClinical Manifestation
Asymptomatic, echocardiographic Asymptomatic, echocardiographic findingfinding
SymptomaticSymptomatic Dyspnea in 90%Dyspnea in 90% Angina pectoris in 75%Angina pectoris in 75% Fatigue, pre-syncope, syncopeFatigue, pre-syncope, syncope risk of SCD in children and adolescentsrisk of SCD in children and adolescents Palpitations, PND, CHF, dizziness less Palpitations, PND, CHF, dizziness less
frequentfrequent
Hypertrophic Cardiomyopathy
HypertrophicHypertrophic CardiomyopathyCardiomyopathy Course and Course and
PrognosisPrognosis Course and prognosis exceedingly variable.Course and prognosis exceedingly variable.
Most patient do very well.Most patient do very well. Some experience progression of symptoms.Some experience progression of symptoms.
S.D.S.D. More common in children and young adults More common in children and young adults
(younger than 25 years) with the familial form of the (younger than 25 years) with the familial form of the disease.disease.
May result from arrhythmia even without significant May result from arrhythmia even without significant LVH or LVOT obstruction.LVH or LVOT obstruction.
May result from development of LVOT obstruction May result from development of LVOT obstruction with exercise.with exercise.
Hypertrophy progresses, some patient with no Hypertrophy progresses, some patient with no obstruction will develop it later in life. (Progression obstruction will develop it later in life. (Progression is faster in the younger.)is faster in the younger.)
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
Treatment of symptomatic patientsTreatment of symptomatic patients Beta blockers and/or calcium channel blockersBeta blockers and/or calcium channel blockers
Provide relief of angina, dyspnea syncope and improve Provide relief of angina, dyspnea syncope and improve exercise capacityexercise capacity
Disopyramide (antiarrhythmic but used for depression Disopyramide (antiarrhythmic but used for depression of LV performance.) of LV performance.)
Diuretics (with caution)Diuretics (with caution) Avoid Digitalis glycosides (AF?)Avoid Digitalis glycosides (AF?)
Prophylactic measures (secondary)Prophylactic measures (secondary) EndocarditisEndocarditis S.D. – Markers of increased risk: young age S.D. – Markers of increased risk: young age
massive hypertrophy, VT, NSVT, VFmassive hypertrophy, VT, NSVT, VF h/o syncope and family h/o of S.D. h/o syncope and family h/o of S.D. Troponin T gene mutationsTroponin T gene mutations
Treatment of asymptomatic patients – Treatment of asymptomatic patients – Primary prophylaxisPrimary prophylaxis
Beta BlockersBeta Blockers Prohibition from engagement in competitive sportsProhibition from engagement in competitive sports If strong family history of S.D – EPIf strong family history of S.D – EP
Hypertrophic – Hypertrophic – CardiomyopathyCardiomyopathy
Non-Medical TreatmentNon-Medical Treatment
Cardiac Pacing (palliation of Cardiac Pacing (palliation of symptoms)symptoms)
SeptostomySeptostomy Chemical septal ablation with Chemical septal ablation with
alcoholalcohol
Chemical Septal Ablation in Hypertrophic Cardiomyopathy
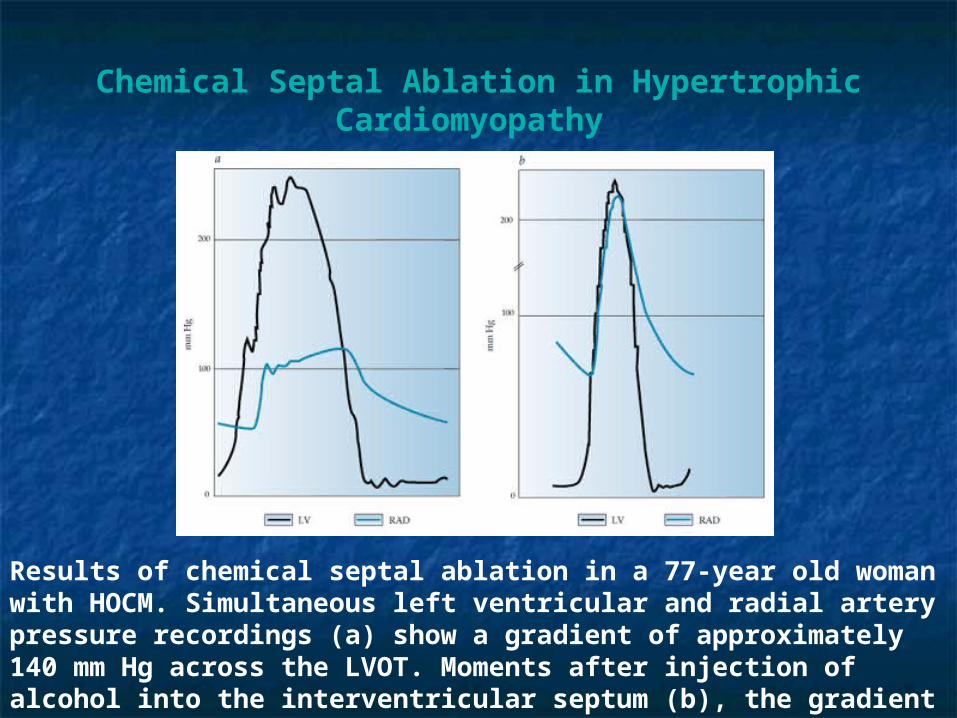
Results of chemical septal ablation in a 77-year old woman with HOCM. Simultaneous left ventricular and radial artery pressure recordings (a) show a gradient of approximately 140 mm Hg across the LVOT. Moments after injection of alcohol into the interventricular septum (b), the gradient is abolished. (LV-left ventricle; RAD-radial artery)
Risk Factors for SCDRisk Factors for SCD
Young age (<30 years)Young age (<30 years) ““Malignant” family history of sudden deathMalignant” family history of sudden death Gene mutations prone to SCD (ie. Arg403Gln)Gene mutations prone to SCD (ie. Arg403Gln) Aborted sudden cardiac deathAborted sudden cardiac death Sustained VT or SVTSustained VT or SVT Recurrent syncope in the youngRecurrent syncope in the young Nonsustained VT (Holter Monitoring)Nonsustained VT (Holter Monitoring) Bradyarrhythmias (occult conduction disease)Bradyarrhythmias (occult conduction disease)
Br Heart J 1994; 72:S13
Hypertrophic Cardiomyopathy
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
Recommendations for Athletic Recommendations for Athletic ActivityActivity
Avoid most competitive sports Avoid most competitive sports (whether or not symptoms and/or (whether or not symptoms and/or outflow gradient are present.)outflow gradient are present.)
Low-risk older patients (>30 yrs) Low-risk older patients (>30 yrs) may participate in athletic activity may participate in athletic activity if all of the following are absent.if all of the following are absent.
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy
Recommendations for Athletic Recommendations for Athletic ActivityActivity
Low-risk older patients (>30 yrs) may participate Low-risk older patients (>30 yrs) may participate in athletic activity if all of the following are absentin athletic activity if all of the following are absent ventricular tachycardia on Holter monitoringventricular tachycardia on Holter monitoring family history of sudden death due to HCMfamily history of sudden death due to HCM history of syncope or episode of impaired consciousnesshistory of syncope or episode of impaired consciousness severe hemodynamic abnormalities, gradient severe hemodynamic abnormalities, gradient 50 50
mmHgmmHg exercise induced hypotensionexercise induced hypotension moderate or severe mitral regurgitationmoderate or severe mitral regurgitation enlarged left atrium (enlarged left atrium (50 mm)50 mm) paroxysmal atrial fibrillationparoxysmal atrial fibrillation abnormal myocardial perfusionabnormal myocardial perfusion
Hypertrophic Cardiomyopathy –Key Points
•Medical therapy with -blockers is first-line management of hypertrophic cardiomyopathy; verapamil is an alternative or adjuvant.
•Patients with syncope, a family history of sudden death, or documented ventricular tachycardia are at highest risk of sudden death and should be promptly referred for evaluation by an electrophysiologist.
•For patients with hypertrophic cardiomyopathy refractory to medical therapy, surgical septal myectomy or percutaneous ethanol septal ablation can be considered. Pacing therapy has limited efficacy.
•Participation in all but low-intensity competitive sports is contraindicated for patients with hypertrophic cardiomyopathy.
Other Causes of Septal Other Causes of Septal HypertrophyHypertrophy
Clinical mimicsClinical mimics glycogen storage (Pompe’s, Fabry’s), infants of glycogen storage (Pompe’s, Fabry’s), infants of
diabetic mothers, amyloid, Hyper or hypothyroid, diabetic mothers, amyloid, Hyper or hypothyroid, hyperparathyroid, acromegaly, tumor infiltration of hyperparathyroid, acromegaly, tumor infiltration of septum.septum.
GeneticGenetic Noonan’s, Friedreich’s ataxia, Turner’s, Familial Noonan’s, Friedreich’s ataxia, Turner’s, Familial
restrictive cardiomyopathy with disarrayrestrictive cardiomyopathy with disarray Exaggerated physiologic responseExaggerated physiologic response
Afro-Caribbean hypertension, old age hypertrophy, Afro-Caribbean hypertension, old age hypertrophy, athlete’s heartathlete’s heart
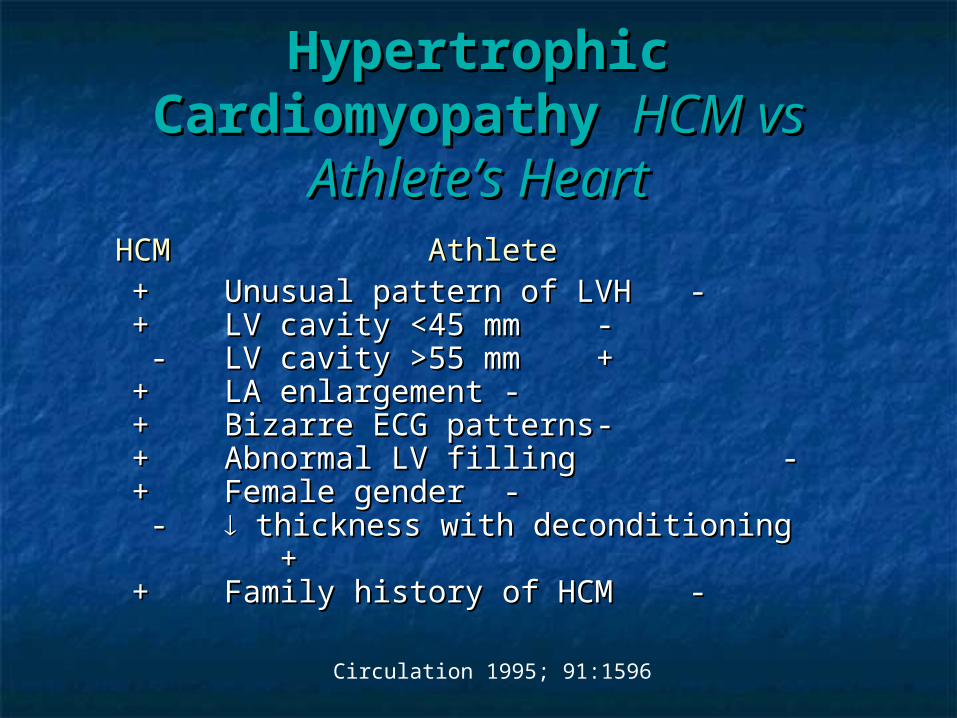
Hypertrophic Hypertrophic CardiomyopathyCardiomyopathy HCM vs HCM vs
Athlete’s HeartAthlete’s Heart HCMHCM Athlete Athlete
++ Unusual pattern of LVHUnusual pattern of LVH --++ LV cavity <45 mmLV cavity <45 mm -- - - LV cavity >55 mmLV cavity >55 mm ++++ LA enlargementLA enlargement --++ Bizarre ECG patternsBizarre ECG patterns --++ Abnormal LV fillingAbnormal LV filling - -++ Female genderFemale gender -- - - thickness with deconditioning thickness with deconditioning + +++ Family history of HCMFamily history of HCM --
Circulation 1995; 91:1596
Hypertensive HCM of the Hypertensive HCM of the Elderly Elderly
CharacteristicsCharacteristics
Modest concentric LV hypertrophy (<12 Modest concentric LV hypertrophy (<12 mm)mm)
Small LV cavity sizeSmall LV cavity size Associated hypertensionAssociated hypertension Ventricular morphology greatly distorted Ventricular morphology greatly distorted
with reduced outflow tractwith reduced outflow tract Sigmoid septum and “grandma SAM”Sigmoid septum and “grandma SAM”

Restrictive Restrictive CardiomyopathyCardiomyopathy
Restrictive Restrictive CardiomyopathyCardiomyopathy
EtiologyEtiology Usually a product of infiltrative disease such as: Usually a product of infiltrative disease such as:
amyloidosis, hemochromatosis, glycogen storage disease.amyloidosis, hemochromatosis, glycogen storage disease. Idiopathic – not uncommon.Idiopathic – not uncommon. Least common type of cardiomyopathy in the western Least common type of cardiomyopathy in the western
countries.countries. PathophysiologyPathophysiology
Rigid myocardium impeding ventricular filling. LVEDP is Rigid myocardium impeding ventricular filling. LVEDP is increased. Abnormal diastolic relaxation. Systolic increased. Abnormal diastolic relaxation. Systolic performance is often reduced.performance is often reduced.
DiagnosisDiagnosis CHF often predominant right sided failure (Kussmaul’s CHF often predominant right sided failure (Kussmaul’s
sign)sign) Differential diagnosis – constrictive Pericarditis.Differential diagnosis – constrictive Pericarditis.
Unequal diastolic pressures, more ventricular independence Unequal diastolic pressures, more ventricular independence in constriction, pulmonary HTN more in restriction .in constriction, pulmonary HTN more in restriction .
Homodynamic
Cardiac output Normal Normal to Normal or
Stroke volume Normal or ↑ Normal or
Normal or
Ventricular fillingpressure
↑ ↑ Normal or ↑ ↑ ↑ Usually ↑
Chamber size ↑ ↑ Normal or Normal or ↑ Typically
Ejection fraction
↑ ↑ Normal to Normal to
Diastolic compliance Normal or
Other findingsMay have associated functional mitral or tricuspid regurgitation
Obstruction may develop between interventricular septum and septal leaflet of mitral valveMitral regurgitation may be present
Characteristic ventricular pressure tracings that resemble those recorded in constrictive pericarditis, with early diastolic dip- and-plateau configuration
May be seen as a feature of the hypereosinophilic syndromesSome investigators consider it a form of restrictive cardiomyopathy
Dilated Hypertrophic RestrictiveObliterative
(Restrictive-Obliterative)
Morphologic
Biventricular dilatation
Marked hypertrophy of left ventricle and occasionally of right ventricle; usually but not always, disproportionate hypertrophy of septum
Reduced ventricular compliance; usually caused by infiltration of myocardium (e.g., by amyloid, hemosiderin, or glycogen deposits)
Thickened endocardium or mural thrombi, or both, act as space-occupying lesions
Morphologic and Hemodynamic Characteristics of the Cardiomyopathies
Restrictive Restrictive CardiomyopathyCardiomyopathy
Usually results from diseases that infiltrate the myocardium such as:Usually results from diseases that infiltrate the myocardium such as:
AmyloidosisAmyloidosis
CarcinoidCarcinoid
Loeffler’s endocarditis/ EMFLoeffler’s endocarditis/ EMF
SarcoidosisSarcoidosis
HemochromatosisHemochromatosis
Glycogen storage diseasesGlycogen storage diseases
Mucopolysaccharidoses (Hurler’s, Hurler-Scheie, Hunter, and Mucopolysaccharidoses (Hurler’s, Hurler-Scheie, Hunter, and
Morquio syndromes)Morquio syndromes)
Many cases of restrictive cardiomyopathies are idiopathic.Many cases of restrictive cardiomyopathies are idiopathic.
Restrictive Cardiomyopathies
Myocardial Infiltrative* or Storage Diseases with Known Etiology
Amyloidosis Scleroderma Hemochromatosis Glycogen storage disease Fabry disease Hurler syndrome Primary or metastatic tumors of the heart (e.g., lymphoma, melanoma)
* Usually causes a restrictive hemodynamic picture
Restrictive Cardiomyopathies Endomyocardial Causes of Restrictive Cardiomyopathies of Known Etiology
• Intense endocardial fibrotic thickening of apex and subvalvular region of one or both ventricles.
• Restriction to inflow of blood causing restrictive pattern.
• Etiologies: Lőffler’s endocarditis, endomyocardial fibrosis, endocardial fibroelastosis, carcinoid, Hurler’s, scleroderma.
Restrictive Restrictive CardiomyopathyCardiomyopathy
Endocardial fibroelastosisEndocardial fibroelastosis
May be primary or secondary. May be primary or secondary.
Found in infancy with primary form presenting Found in infancy with primary form presenting
between 2-12 months of life. between 2-12 months of life.
May be associated with left heart obstructive lesions May be associated with left heart obstructive lesions
ie. aortic stenosis, coarctation of aorta, hypoplastic ie. aortic stenosis, coarctation of aorta, hypoplastic
left heart syndrome. left heart syndrome.
Treat with digoxin. Treat with digoxin.
Restrictive Restrictive CardiomyopathyCardiomyopathy
Hurler’s Syndrome (resembles endocardial elastosis)Hurler’s Syndrome (resembles endocardial elastosis)
Mucopolysaccharide deposition (heparin and dermatan sulfate Mucopolysaccharide deposition (heparin and dermatan sulfate
compounds) in connective tissue.compounds) in connective tissue.
Hurler cells present (granular inclusions), and increased Hurler cells present (granular inclusions), and increased
collagen in the interstitium. Relative sparing of the actual collagen in the interstitium. Relative sparing of the actual
myocytes.myocytes.
Autosomal recessive and associated with dwarfism, corneal Autosomal recessive and associated with dwarfism, corneal
clouding, mental retardation, HSM, skeletal malformations.clouding, mental retardation, HSM, skeletal malformations.
Present with CHF caused by impaired ventricular filling and Present with CHF caused by impaired ventricular filling and
distorted and thickened mitral valves. May get narrowing of distorted and thickened mitral valves. May get narrowing of
coronary arteries as well. Prognosis is poor.coronary arteries as well. Prognosis is poor.
Restrictive Restrictive CardiomyopathyCardiomyopathy
CarcinoidCarcinoid
Symptoms arise from secretion of serotonin and include flushing, Symptoms arise from secretion of serotonin and include flushing,
diarrhea, bronchospasm.diarrhea, bronchospasm.
Cardiac involvement in >50% of pts and is usually right sided Cardiac involvement in >50% of pts and is usually right sided
involvement.involvement.
60-90% of tumors arise in the appendix but may metastasize to the 60-90% of tumors arise in the appendix but may metastasize to the
liver.liver.
May see fibrous plaques on right heart structures that may lead to May see fibrous plaques on right heart structures that may lead to
tricuspid regurgitation and pulmonic stenosis.tricuspid regurgitation and pulmonic stenosis.
Treat with digoxin, diuretics, alpha and serotonin blockers. May need Treat with digoxin, diuretics, alpha and serotonin blockers. May need
tricuspid valve replacement or pulmonic valvulotomy.tricuspid valve replacement or pulmonic valvulotomy.
Restrictive Restrictive CardiomyopathyCardiomyopathy
LLőffler’s endocarditis/ EMFőffler’s endocarditis/ EMF
Intense tissue and frequently peripheral blood eosinophilia.Intense tissue and frequently peripheral blood eosinophilia.
Primarily males and occurs in temperate climate zones.Primarily males and occurs in temperate climate zones.
May be aggressive.May be aggressive.
Associated with arthritis and thromboembolic phenomenon.Associated with arthritis and thromboembolic phenomenon.
May be same disease as endomyocardial fibrosis (EMF) that May be same disease as endomyocardial fibrosis (EMF) that
occurs in tropics.occurs in tropics.
May start as an intense necrotizing myocarditis followed by a May start as an intense necrotizing myocarditis followed by a
thrombotic stage after 1yr.thrombotic stage after 1yr.
The final stage is that of fibrosis and restriction.The final stage is that of fibrosis and restriction.
Clinical ManifestationsClinical Manifestations
Symptoms of right and left heart failureSymptoms of right and left heart failure Jugular Venous Pulse Jugular Venous Pulse
Prominent Prominent x x and and yy descents descents Echo-DopplerEcho-Doppler
Abnormal mitral inflow patternAbnormal mitral inflow pattern Prominent E wave (rapid diastolic filling)Prominent E wave (rapid diastolic filling) Reduced deceleration time (Reduced deceleration time ( LA pressure) LA pressure)
Restrictive Cardiomyopathies
HemodynamicsHemodynamics The jugulovenous pulse is an indication of The jugulovenous pulse is an indication of
right atrial pressure. The a wave right atrial pressure. The a wave corresponds to atrial contraction and the x corresponds to atrial contraction and the x descent to the drop in atrial pressure descent to the drop in atrial pressure during active filling of the right ventricle.during active filling of the right ventricle.
The v wave relates to the effect of right The v wave relates to the effect of right ventricular contraction. The y descent ventricular contraction. The y descent reflects the rapid passive filling phase of reflects the rapid passive filling phase of the right ventricle that begins once the the right ventricle that begins once the tricuspid valve opens.tricuspid valve opens.
Restrictive Cardiomyopathies
HemodynamicsHemodynamics In the case of restriction, when right ventricular In the case of restriction, when right ventricular
filling is impaired, the x and y descent are sharp filling is impaired, the x and y descent are sharp and swift.and swift.
After the y descent (passive filling phase of the After the y descent (passive filling phase of the right ventricle), the pressure cannot increase right ventricle), the pressure cannot increase resulting in a leveling off of the pressure tracing.resulting in a leveling off of the pressure tracing.
The combination of the sharp y descent and The combination of the sharp y descent and leveling of pressure tracing account for the “dip leveling of pressure tracing account for the “dip and plateau” or so called “square root sign.”and plateau” or so called “square root sign.”
A similar and analogous phenomenon is observed A similar and analogous phenomenon is observed when interrogating the mitral and tricuspid valves when interrogating the mitral and tricuspid valves on doppler echo. on doppler echo.
Restrictive Cardiomyopathies
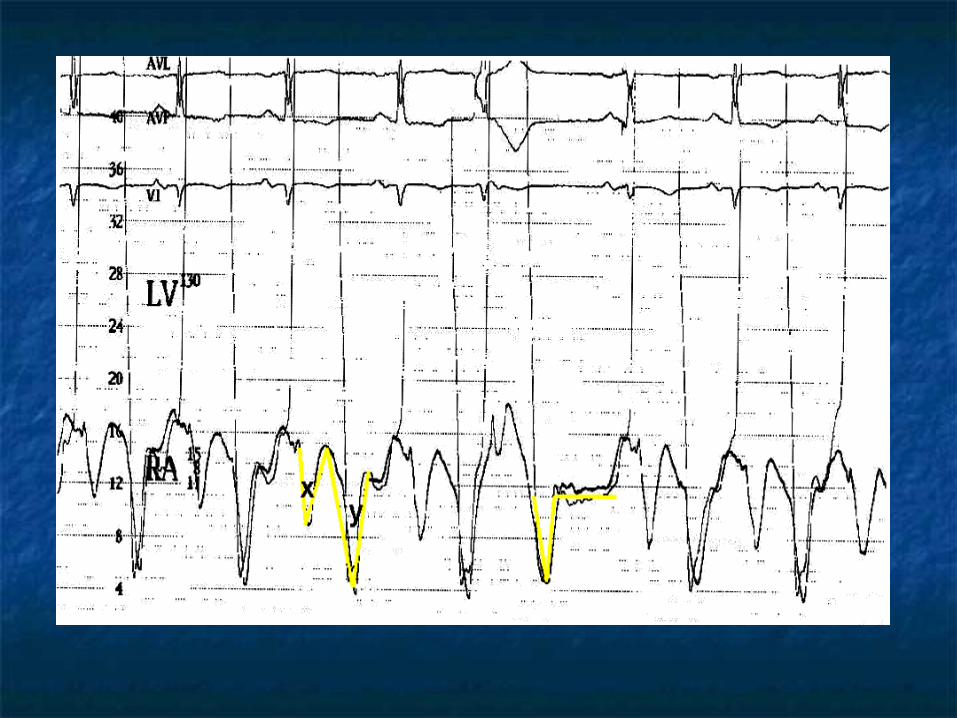
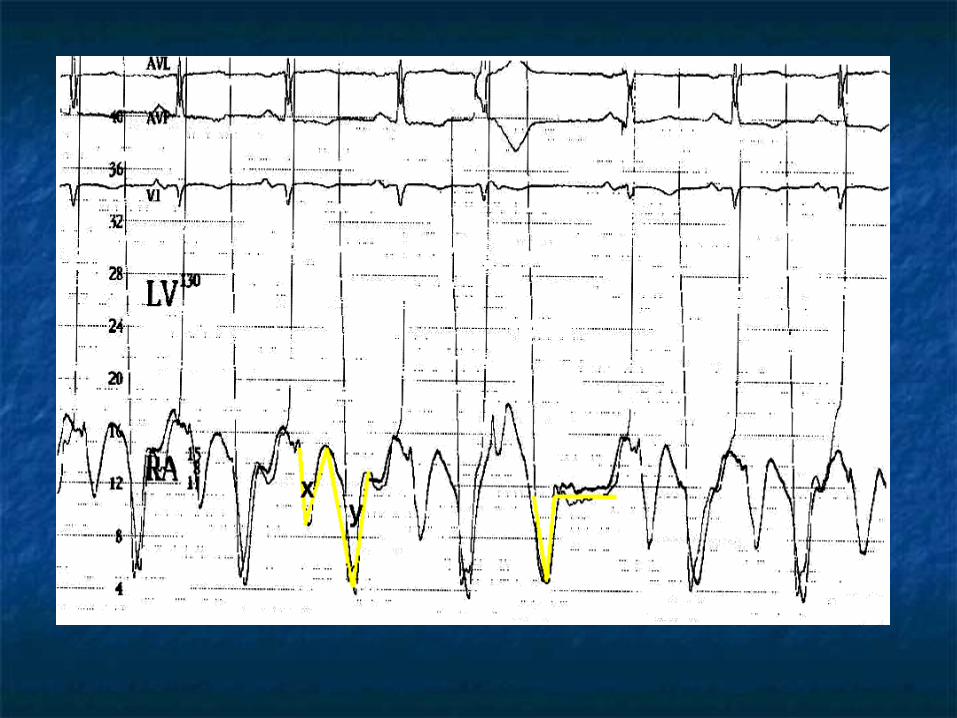
Restrictive Cardiomyopathy- Pressure Tracing
Shown is a right atrial pressure tracing in a patient with restrictive cardiomyopathy secondary to amyloidosis; some functional tricuspid regurgitation is present. The cardiac rhythm is atrial fibrillation. Large systolic (V) waves appear, followed by a typical early diastolic dip-and-plateau configuration.
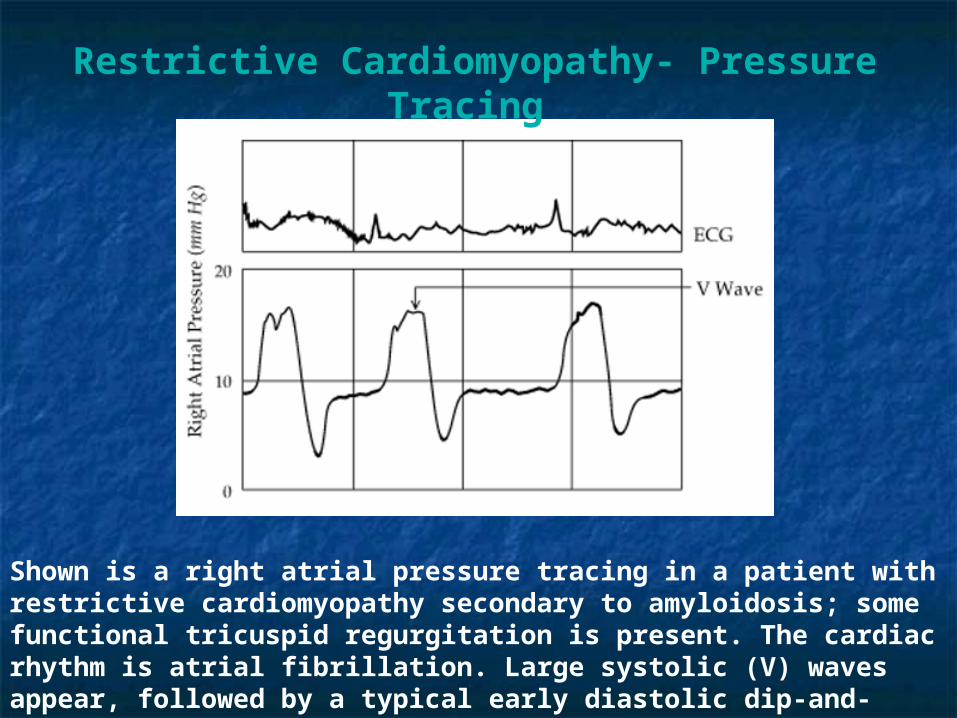
Constrictive - Restrictive PatternConstrictive - Restrictive Pattern““Square-Root Sign” or “Dip-and-Plateau”Square-Root Sign” or “Dip-and-Plateau”
Constrictive PericarditisConstrictive Pericarditis Fibrous scarring, adhesion and calcification of the Fibrous scarring, adhesion and calcification of the
pericardium (shell around the heart)pericardium (shell around the heart)
Similar to tamponade in restricting diastolic filling of Similar to tamponade in restricting diastolic filling of
the heart. Kussmaul’s sign v.s. paradoxical pulse.the heart. Kussmaul’s sign v.s. paradoxical pulse.
Difficult diagnosis: Venous congestion, fatigue, Difficult diagnosis: Venous congestion, fatigue,
effusions with normal LV function, normal pulmonary effusions with normal LV function, normal pulmonary
pressure and a small cardiac silhouette no pulmonary pressure and a small cardiac silhouette no pulmonary
congestion.congestion.
CT / MRI: pericardial thickeningCT / MRI: pericardial thickening
Echo / Doppler: Flow respiratory variationEcho / Doppler: Flow respiratory variation
Treatment: Conservative / SurgicalTreatment: Conservative / Surgical
Restriction vs ConstrictionRestriction vs Constriction
History provide can important cluesHistory provide can important clues Constrictive pericarditisConstrictive pericarditis
History of TB, trauma, pericarditis, collagen History of TB, trauma, pericarditis, collagen vascular disorders.vascular disorders.
Restrictive cardiomyopathyRestrictive cardiomyopathy Amyloidosis, hemochromatosisAmyloidosis, hemochromatosis
MixedMixed Mediastinal radiation, cardiac surgeryMediastinal radiation, cardiac surgery
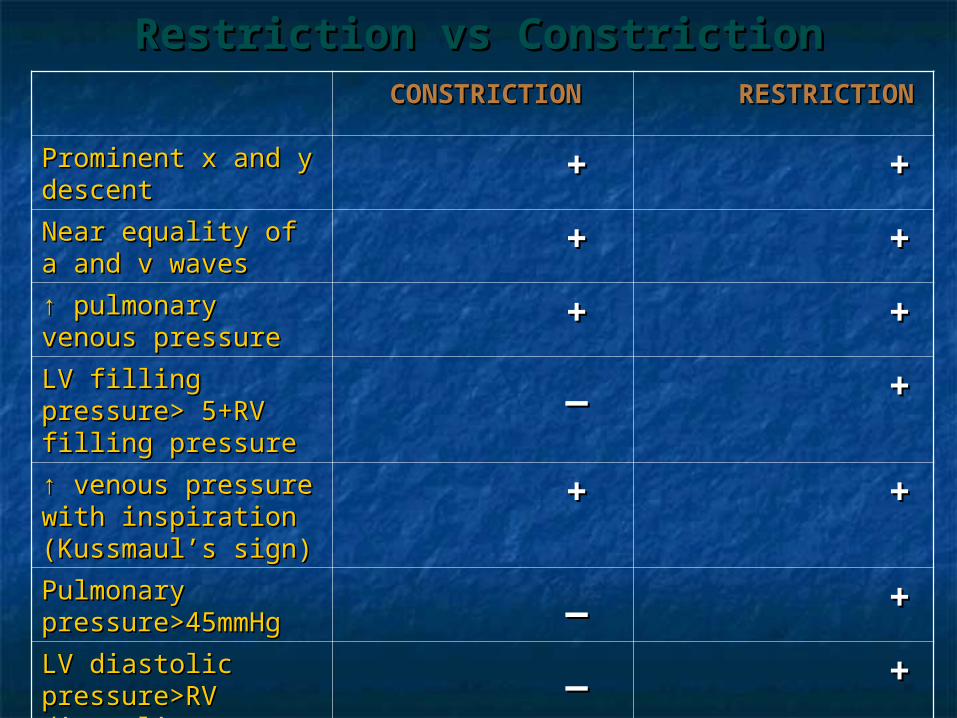
Restriction vs ConstrictionRestriction vs Constriction CONSTRICTIONCONSTRICTION RESTRICTIONRESTRICTION
Prominent x and y Prominent x and y descentdescent
++ ++
Near equality of a Near equality of a and v wavesand v waves
++ ++
↑↑ pulmonary venous pulmonary venous pressurepressure
++ ++
LV filling pressure> LV filling pressure> 5+RV filling 5+RV filling pressurepressure
__ ++
↑↑ venous pressure venous pressure with inspiration with inspiration (Kussmaul’s sign)(Kussmaul’s sign)
++ ++
Pulmonary Pulmonary pressure>45mmHgpressure>45mmHg
__ ++
LV diastolic LV diastolic pressure>RV pressure>RV diastolic pressure diastolic pressure with exercisewith exercise
__ ++
Restrictive Restrictive CardiomyopathiesCardiomyopathies TreatmentTreatment
No satisfactory medical therapyNo satisfactory medical therapy Drug therapy must be used with cautionDrug therapy must be used with caution
diuretics for extremely high filling pressuresdiuretics for extremely high filling pressures vasodilators may decrease filling pressurevasodilators may decrease filling pressure ? Calcium channel blockers to improve ? Calcium channel blockers to improve
diastolic compliancediastolic compliance digitalis and other inotropic agents are not digitalis and other inotropic agents are not
indicatedindicated
Restrictive Cardiomyopathy Key Points
. Restrictive cardiomyopathy often manifests as an insidious onset of exercise intolerance and right-sided heart failure similar to constrictive pericarditis.
















![Computational Vision Daniel Kersten Lecture 7: Image ...vision.psych.umn.edu/users/kersten/kersten-lab/... · testimage= ImageDataB F; Remember if you execute ImageData[< >]](https://img.pdfslide.us/doc/110x75/5fb588e8dd352c67bd5165e3/computational-vision-daniel-kersten-lecture-7-image-testimage-imagedatab-f.jpg)