Embed Size (px)
Citation preview

Update in Cardiology 2015 Royal College
Sara Thorne
Cardiology Update Native Valve Disease and Pregnancy
Sara Thorne October 2015

Case History 1
21 year old from Somalia, 16/40 1st pregnancy Seen in A&E by acute medicine SpR 3 week history increasing breathlessness Worse at night, dry cough Breathless, sitting up Coughs++ lying flat P120 sinus rhythm BP 105/60 HS I___II___I Chest widespread wheeze
Case History 1
What happened next…… Differential diagnosis? Pregnancy induced asthma Chest infection Investigations? No, because pregnant Initial management? Oxygen Salbutamol nebuliser Antibiotics Initial response? dyspnoea and distress Heart rate 130

Socioeconomic Factors and Maternal Pregnancy Outcome
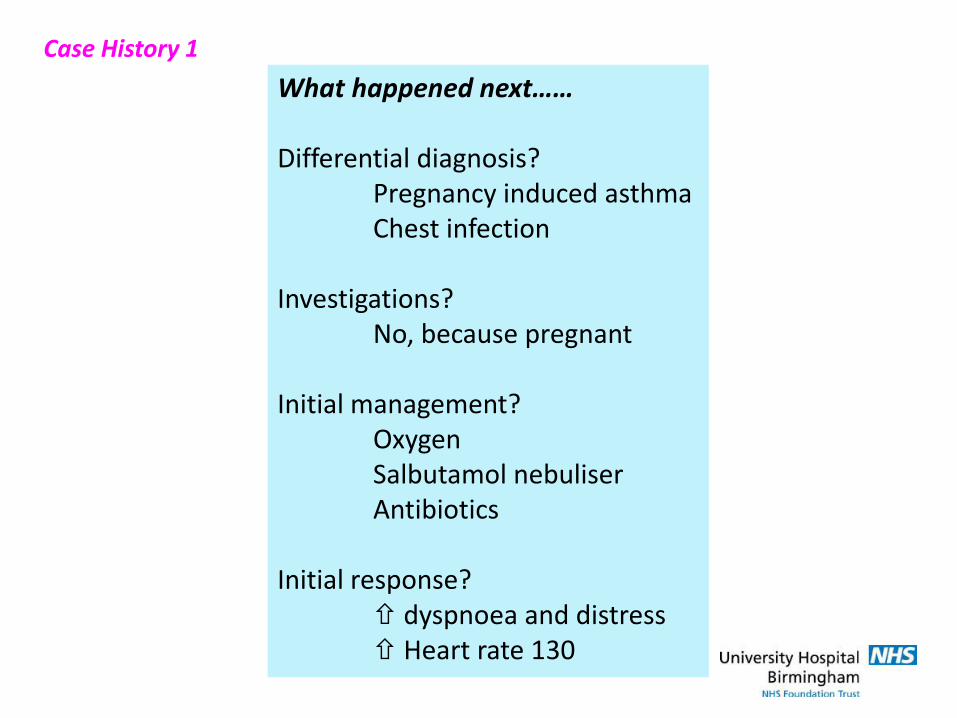
Maternal Mortality By Cause UK 2010-2012 Overall mortality 10 per 100 000 women giving birth

Cause of death Number (early n =53) Ischaemic heart disease 11 Cardiomyopathy 4 (+1 late death) PPCM 9 (+ 6 late deaths) Sudden death 10 Aortic dissection 7 Congenital heart disease 1 Endocarditis 2 Pulmonary hypertension 2 Thrombosed mechanical valve 2
Major Causes Of Maternal Death From Cardiac Disease; UK 2006-2008.
.....No deaths from native valve disease
.....Safe in pregnancy?

Cardiac Causes Maternal Mortality (per million maternities) 1952-2002
0
10
20
30
40
50
60
1954 1960 1966 1972 1978 1984 1990 1996 2002
Total cardiac
Congenital
PulmonaryhypertensionIschaemic
Rheumatic
CNP 2004 Courtesy of Cathy Nelson Piercy
Changing Pattern of Maternal Cardiac Deaths in the UK
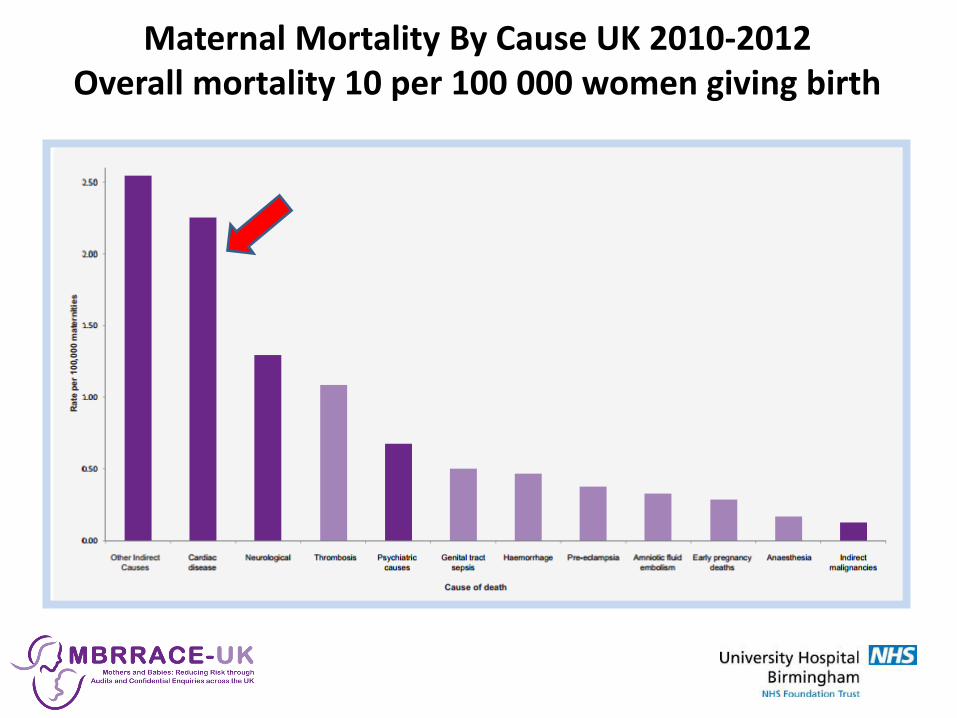
Direct deaths
71%
Cardiac
disease
17%
Other indirect
12%
Haemorrhage, sepsis, pre-eclampsia
Haththotuwa ‘10 IJGO
Maternal Death in Sri Lanka
MMR 38 per 100 000
Nearly all rheumatic mitral stenosis
2004

Hb
Karamermer et al ‘07
Cardiovascular Changes In Pregnancy
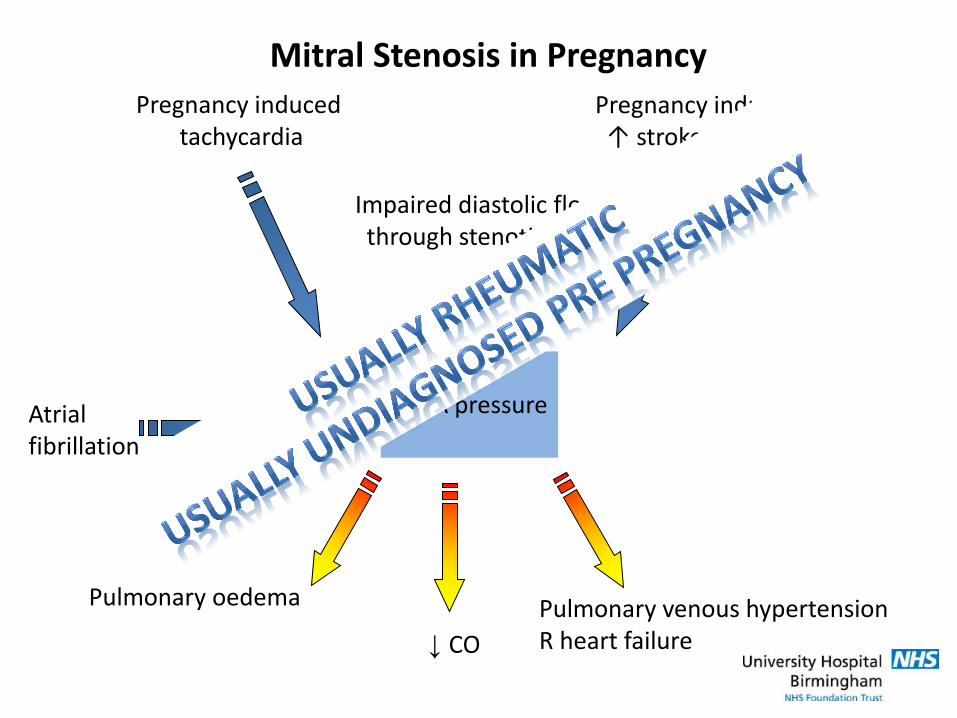
Impaired diastolic flow through stenotic MV
Pregnancy induced tachycardia
Pregnancy induced ↑ stroke volume
↑ LA pressure
Pulmonary oedema
Atrial fibrillation
Pulmonary venous hypertension R heart failure
Mitral Stenosis in Pregnancy
↓ CO

Maternal Heart Disease & Risk of Pregnancy
Modified WHO risk criteria Thorne et al Heart 2006
Low risk (mortality ≤1%) Unoperated small/mild: Pulmonary stenosis Septal defects Patent arterial duct
Most successfully repaired: Septal defects CoA repaired Fallot repaired
Significant risk (mortality 1-10%) Mechanical valve Ischaemic HD Systemic R ventricle Cyanotic, no PHT Fontan
High risk/contraindicated (Mortality >10%) Pulmonary hypertension Ventricular function ↓↓
Aortic aneurysm

Case History 1
What should have happened next…. Differential diagnosis? Pulmonary oedema Pregnancy induced asthma Chest infection Investigation? CXR – LA dilatation, pulmonary oedema ECG – SR, p mitrale, p pulmonale, RV+ Echo – oxygen & diuretics given whilst waiting Urgent cardiology referral

Case History 1

Case History 1 Cardiology review Salbutamol nebuliser removed Furosemide 20mg IV given RV heave Tapping apex Apical loud S1, opening snap, mid diastolic murmur Echo Severe rheumatic mitral stenosis, valve area 0.9cm2

Case History 1
Further management Improved on Furosemide 20mg od Bisoprolol 1.25 – 3.75 mg od Prophylactic LMWH Pulse 90 SR BP 95/60 Able to lie flat What next? 1. Termination of pregnancy 2. Continue medical management to term or until decompensates 3. Mitral valve replacement 4. Balloon mitral valvuloplasty

Balloon Mitral Valvuloplasty For Rheumatic Mitral Stenosis
• Usually suitable in young women – pliable, not calcified, not regurgitant
• Diminishing UK experience – get an expert Procedural echo to minimise screening time Reduce fluoroscopy frame rate Pelvic wedge under L hip • Timing ≤ 20/40: routine cardiology and anaesthetic team present ≥20/40: need to empty uterus if arrests obstetrician present ≥24/40: fetus viable obstetrician, obstetric theatre team, neonatal team present

Case History 1
Further management 19/40 Successful balloon mitral valvotomy MVA 1.6cm2, no MR Asymptomatic 39/40 Spontaneous normal delivery
5 years later….. No further intervention Just completed 3rd pregnancy uneventfully

Aortic Stenosis in Pregnancy
In contrast to mitral stenosis: Usually bicuspid Easy to hear…. Usually known pre-pregnancy Opportunity for pre-pregnancy assessment

• Assess risk
• Optimise condition
• Plan alternatives – timed pregnancy, no pregnancy
• Plan antenatal care, delivery, post partum care
Bicuspid Aortic Stenosis: Pre Pregnancy Assessment
*Pre conception planning requires reliable contraception*
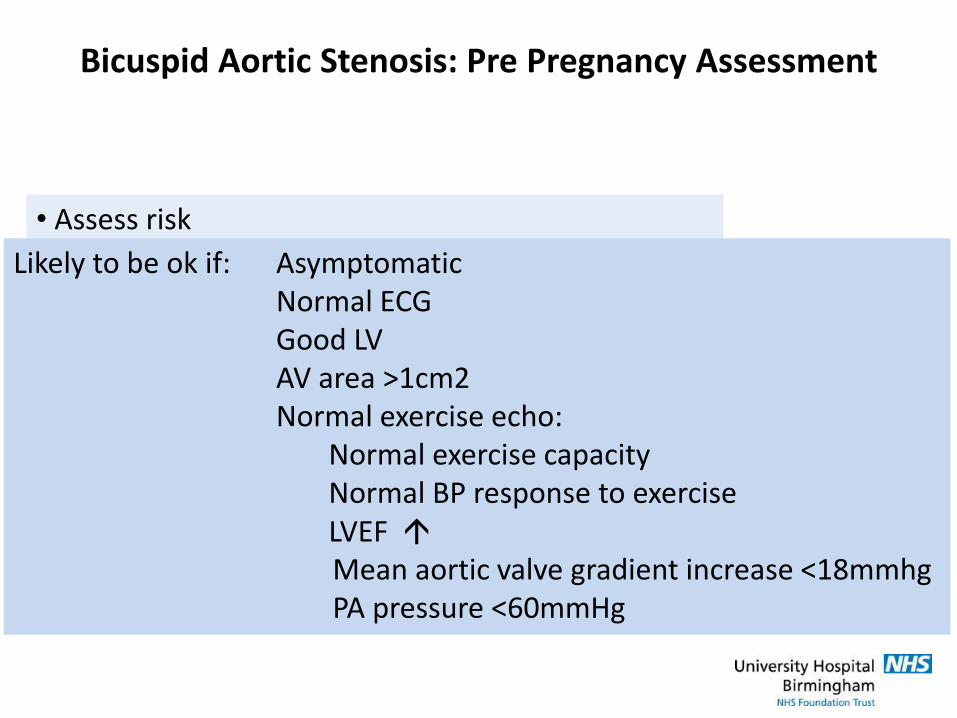
• Assess risk
• Optimise condition
• Plan alternatives – timed pregnancy, no pregnancy
• Plan antenatal care, delivery, post partum care
Likely to be ok if: Asymptomatic Normal ECG Good LV AV area >1cm2 Normal exercise echo: Normal exercise capacity Normal BP response to exercise LVEF Mean aortic valve gradient increase <18mmhg PA pressure <60mmHg
Bicuspid Aortic Stenosis: Pre Pregnancy Assessment

• Assess risk
• Optimise condition
• Plan alternatives – timed pregnancy, no pregnancy
• Plan antenatal care, delivery, post partum care
If symptomatic or high risk Consider AVR (or valvotomy)
Tissue vs mechanical AVR
Bicuspid Aortic Stenosis: Pre Pregnancy Assessment

• Assess risk
• Optimise condition
• Plan alternatives – timed pregnancy, no pregnancy
• Plan antenatal care, delivery, post partum care
Bicuspid Aortic Stenosis: Pre Pregnancy Assessment

• Assess risk
• Optimise condition
• Plan alternatives – timed pregnancy, no pregnancy
• Plan antenatal care, delivery, post partum care
Where should care be Where should delivery be Mode of delivery Post partum follow up & investigation
Bicuspid Aortic Stenosis: Pre Pregnancy Assessment
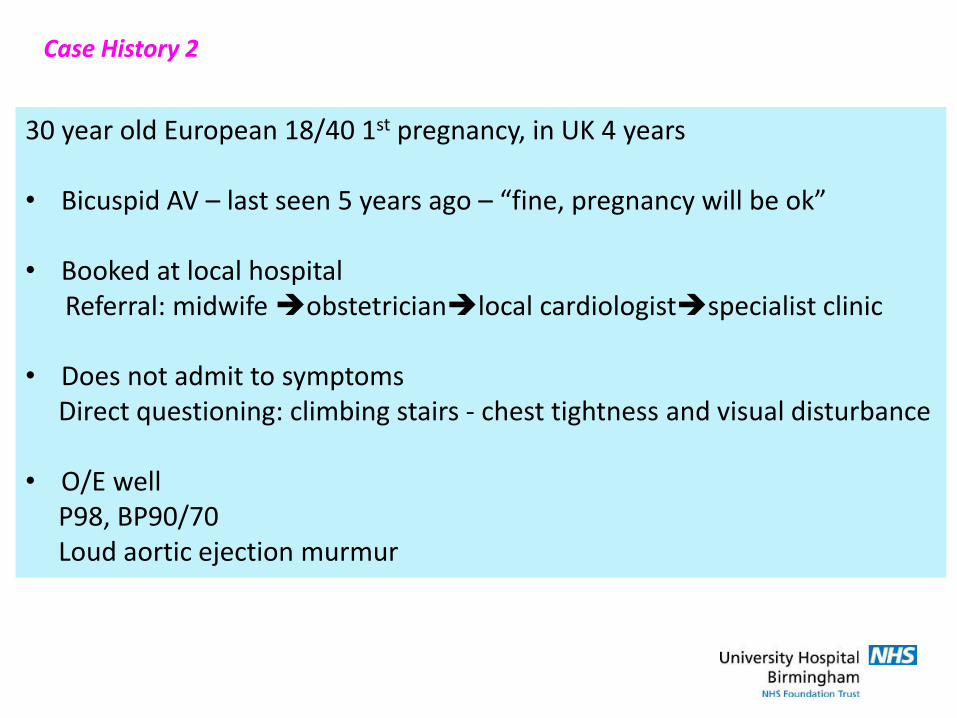
Case History 2
30 year old European 18/40 1st pregnancy, in UK 4 years • Bicuspid AV – last seen 5 years ago – “fine, pregnancy will be ok” • Booked at local hospital Referral: midwife obstetricianlocal cardiologistspecialist clinic • Does not admit to symptoms Direct questioning: climbing stairs - chest tightness and visual disturbance • O/E well P98, BP90/70 Loud aortic ejection murmur
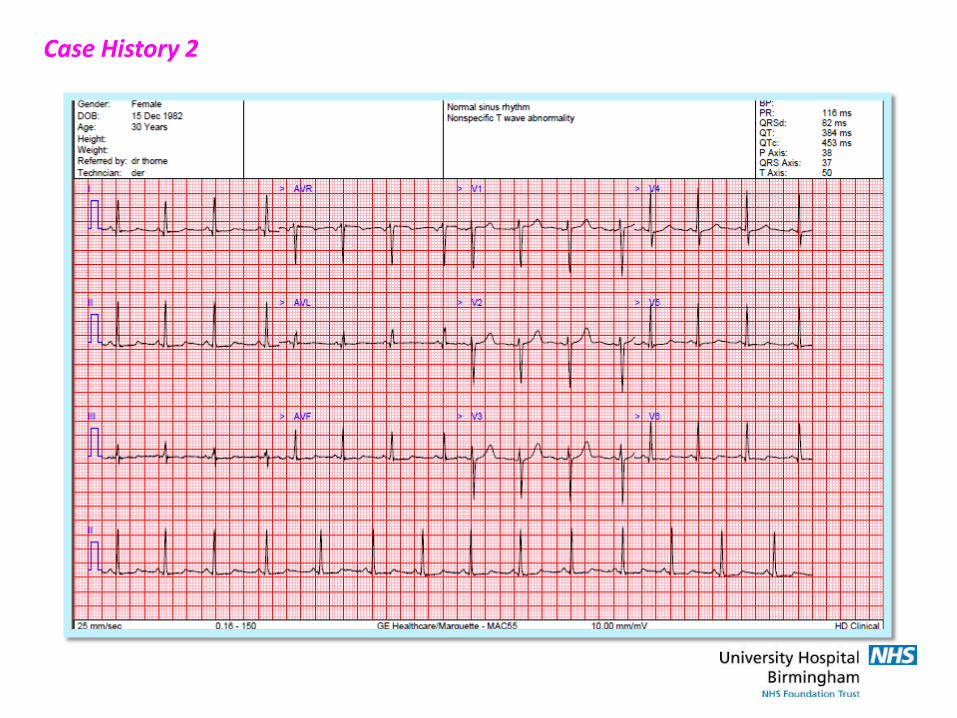
Case History 2

Case History 2
Echocardiogram • Critical bicuspid aortic stenosis, with some calcification Valve area 0.66cm2 Vmax 4.8m/s Mean gradient 56mmHg • Hyperdynamic LV, normal function, mild LVH
Case History 2
Options? • Continue pregnancy, monitor closely • Termination of pregnancy, then AVR • Planned surgical AVR & continue pregnancy • Planned balloon dilatation & continue pregnancy
Palliative balloon aortic valvotomy • Most experience operator – paediatric cardiologist • Risk: ineffective aortic regurgitation • Surgical & theatre standby
decompensation

Case History 2
Initial management • Counselled re options – cardiologist, obstetrician, surgeon • Oral diuretics • 20/40 cautious double balloon aortic valvotomy AVA 0.9cm2
no AR • Felt better – no visual disturbance, denied chest pain • Fortnightly joint review

Case History 2
28/40 • Admitted to local hospital Orthopnoea, paroxysmal nocturnal dyspnoea Central tight chest pain • On transfer Sitting up, breathless P100, BP 90 Chest clear Pitting oedema to thighs • Echo - LV less hyperdynamic
Case History 2
• Emergency Caesarean section in cardiac theatres Epidural Cardiac surgical team on standby Copious ascites • Fetus – good condition, intubated, to NNU • Mother – immediate improvement No cardiac symptoms

Case History 2
What next? • Remained asymptomatic Good contraception Careful observation • 6 months post partum - tissue AVR • 18 months later - daughter well, normal milestones - uneventful successful pregnancy at local hospital

Refer to specialist cardiac pregnancy service
• Isolated valvar regurgitation generally well tolerated
• If ventricular size & function are normal : Trivial MR or AR mWHO 1 = risk same as general population Mild MR or AR mWHO 2 = small risk M&M Moderate MR or AR mWHO 2-3 Severe MR or AR mWHO 3 = significant risk M&M, expert care needed • Risks higher if coexistent lesions Aortopathy, coarctation >1 valve disease Dilating ventricle Impaired LV
Valvar Regurgitation in Pregnancy

Individualise decision: Consider lifetime risk of 4 paths: • Pregnancy without intervention Will it be well tolerated? Will there be a permanent adverse effect on LV size & function? Subsequent operation • Valve repair, then pregnancy Risk of surgery Low risk pregnancy Possible need for reoperation • Tissue valve replacement, then pregnancy Risk of surgery Low risk pregnancy Risk of inevitable reoperation • Mechanical valve replacement, then pregnancy Risk of surgery High risk pregnancy (anticoagulation) Lifetime risk warfarin Low chance of reoperation
Severe Asymptomatic MR or AR
Can I have a
baby?

Summary: Native Valve Disease in Pregnancy
• Valvar regurgitation well tolerated if good ventricular function • Severe mitral & aortic stenosis poorly tolerated in pregnancy • MS: Cause is usually rheumatic, often not diagnosed Main cause maternal cardiac death in developing world Uncommon in UK pregnant women almost exclusively in 1st generation immigrants Balloon MVo usually successful • AS: Usually bicuspid Opportunity to assess pre pregnancy Even severe AS may be tolerated (exercise echo) Palliative balloon AVo often not possible
“1. What should you do if
you see an acutely unwell
pregnant woman? ”
Answer:
(a) Get help!
(b) Think what you would
do if she wasn’t pregnant…
…. And usually, do it.
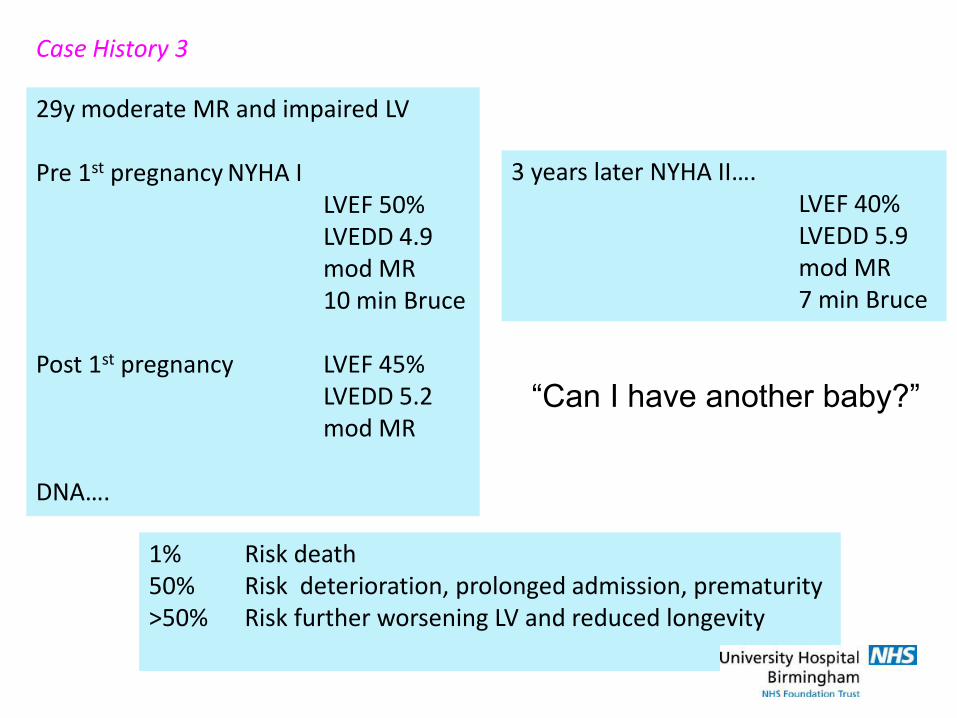
Case History 3
29y moderate MR and impaired LV Pre 1st pregnancy NYHA I LVEF 50% LVEDD 4.9 mod MR 10 min Bruce Post 1st pregnancy LVEF 45% LVEDD 5.2 mod MR DNA….
3 years later NYHA II…. LVEF 40% LVEDD 5.9 mod MR 7 min Bruce
“Can I have another baby?”
1% Risk death 50% Risk deterioration, prolonged admission, prematurity >50% Risk further worsening LV and reduced longevity

Confidential Enquiry into Maternal Deaths & Morbidity UK & Ireland, 2009-2012