Embed Size (px)
Citation preview
Cardiology Newsletter Volume 5 No 2August 2014
Sponsored in the interests of continuing medical education by:
CPD Accredited
• Place of Alpha Blockers in cardiology• Impact of reperfusion therapy for acute
ischaemic stroke• Case-report: Young man with dyspnoea• Ethics: Death certification: Key points
for medical practitioners
C
M
Y
CM
MY
CY
CMY
K
CarzinXL HeartMattersA4.pdf 1 2014/06/26 3:21 PM

Page 3 Volume 5 No 2 August 2014
Editorial board Dr M. Bennett (Editor)CardiologistWilgers Hospital, [email protected]
Dr D. BlomConsultant PhysicianLipid Clinic, Groote Schuur HospitalHealth Sciences FacultyUniversity of Cape TownCape Town
Dr A.J. DalbyCardiologistMyocardial Ischaemia and InfarctionMilpark Hospital, Johannesburg
Dr J. HarrisbergPaediatric CardiologistSunninghill HospitalJohannesburg
Prof B. JacobsonHaematologistThrombosis and Haemostasis University of WitwatersrandJohannesburg
Dr R. JardineCardiologistArrhythmiasGlynwood HospitalBenoni
Prof J.A. KerCardiologistDepartment of Internal Medicine,University of PretoriaPretoria
Prof. K. Sliwa-HanhleCardiovascular ResearchHatter Cardiovascular Research Institute and Institute of Infectious Disease and Molecular Medicine, University of Cape TownHeart Failure/Translational Research
Dr A. ThorntonCardiologistElectrophysiologySunninghill Hospital, Johannesburg
Editorial
The views expressed by the authors in this newsletter do not necessarily reflect those
of the sponsor and editorial board.
This newsletter is proudly sponsored by
If you have any suggestions or topics you would like to see published or have articles and/or
case studies for publishing, please email us at: [email protected].
Dr Mike BennettCardiologist
Wilgers Hospital, Pretoria
Production Editors: Ann Lake, Helen Gonçalves Design: Jane Gouveia
Enquiries: Ann Lake Publications 011 802 8847 Email: [email protected]
Website: www.annlakepublications.co.za
ach new issue of Heart Matters poses a new challenge – not because of a lack of news, but actually because of the explosion in medical
literature. A newsletter like Heart Matters does not publish Nobel Prize winning material, but informs readers who did win the prize and why they did.
Heart Matters aims to cover topics which are of practical nature that are frequently encountered by clinicians. By putting these issues into clinical perspective we hope that clinicians will be able to manage their patients in an informed and rational way. The topics chosen for this issue cover a broad variety of clinical cardiovascular disorders commonly encountered in practical practice.
Alpha blockers are primarily anti-hypertensive agents but are rarely used as first line drugs for this purpose. Their added benefit of symptomatic relief for patients with benign prostatic hypertrophy, often makes them an attractive choice in selected male patients with hypertension. Their role and place in clinical practice is outlined by Dr. David Gilmer.
Dr Roos and colleagues remind us of the devastating consequences of stroke in both the short- and long-term. Early diagnosis and early referral to a centre equipped to manage these patients remain the best option for limiting the extent of brain damage and physical disability.
The diagnosis of myocarditis is often abused. Unfortunately many patients with myocarditis are not diagnosed, leading to an unnecessary risk of long term myocardial dysfunction. Hopefully the guidelines provided by the ESC will be useful in making a more accurate diagnosis.
Prof Gert Zaayman touches on an important topic for every clinician regardless of his speciality or qualifications. We do not often enough think about the possible ramifications and consequences of filling in a “death certificate”.
FeedbackI wish to thank those colleagues who communicated with me and offered constructive feedback. Our aim is to disseminate information on the management of common clinical conditions frequently seen in cardiology practice. Please feel free to contact me if you have any specific topic that you think needs to be covered.
CPD pointsSeveral of you participate in the CPD section and we encourage readers to use this facility.
We hope that you will enjoy this issue and find it useful. I once again wish to thank the sponsor, Pharma Dynamics, for the generous sponsorship.

Volume 5 No 2 August 2014 Page 4
Dr David Gillmer MBChB FCP (SA) FRCP (Lon & Edin)Cardiologist
Ethekwini Hospital and Heart Centre, Durban, KwaZulu-Natal
Place of Alpha Blockers in cardiology
he first line drugs in the treatment of systemic hy-pertension are well estab-lished as beta blockers, cal-cium channel blockers
(CCB), ace inhibitors (ACE-Is)/angio-tensin receptor blockers (ARB) and thiazide diuretics. Drug of first choice is often chosen on the basis of clinical merit, for example beta blockers for patients with obstructive coronary ar-tery disease, ACE-Is for younger active people, CCB’s often together with thi-azide diuretic for older patients and black patients are more resistant to beta blockers and ACE-Is. Moderate to severe hypertension usually requires ACE-Is/CCB combination.
Beta blockers and ACE-Is are our first line treatment for systolic heart failure (after normovolaemia with diuretics). ACE-Is not infrequently need to be discontinued for non productive cough or rashes and in these situations ARB’s are preferred. Occasionally additional vasodilator therapy is required in the form of hydralazine with nitro-glycerine or occasionally alpha blockers.
Alpha blockers therefore have a limited place but are not infrequently used as add on therapy in resistant hypertension and sometimes as first choice when mild hypertension and symptomatic BPH is the presenting symptom. Alpha blockers also have a place in the treatment of rare but sometimes catastrophic pheochromocytoma.
Mechanism of actionIn simple terms the sympathetic nervous system balances the parasympathetic system to maintain the homeostasis of the body and of course its general action is to mobilise the “flight or fight” response. This releases adrenaline and nor - adrenaline from the adrenal cortex and sympathetic post ganglionic neurons. The effect is to increase heart rate, increase cardiac contractility,
widen bronchial passages, decrease mobility of the large intestine, dilate blood vessels to the exercising skeletal muscle and constrict others to deviate blood from non essential areas, increase peristalsis in the oesophagus, dilate pupils, cause piloerection and perspiration.
Stimulation of beta receptors causes vasodilation of vascular skeletal muscle whereas stimulation of alpha adrenergic receptors causes vasoconstriction, particularly in the skin, sphincters of the gastrointestinal system and brain. The effects on the urinary bladder are to cause contraction and increase tone of the detrusor muscle and prostate although the overall effect of sympathetic stimulation of the bladder is usually overwhelmed by the beta 3 adrenergic receptors which have a relaxing effect on the bladder and delay micturition during stress.
Adrenergic receptor blockers therefore dilate arteries and veins, particularly resistance vessels, and relax the bladder and bladder neck.
Potential Clinical roles of the alpha blockers1. Treatment of symptoms of prostatisim
and bladder neck obstruction related to benign prostatic hypertrophy.
2. Treatment of hypertension.3. Treatment of cardiac failure as an
additional vasodilator4. Treatment of pheochromocytoma
Current Clinical use of alpha blockers
1. Benign prostatic hypertrophyThis is the primary indication for alpha blockers and had revolutionized the management of BPH. Prazosin is effective but has a short half life requiring twice daily dosing and dose titration due to the development of tachyphylaxis.
Side effects include orthostatic hypertension, muscle fatigue, retrograde ejaculation, nasal stuffiness and headache. Long acting alpha blockers allow for once daily dosing e.g. Terazosin and Doxazosin. Tamsulosin is an alpha 1 receptor blocker which specifically blocks the receptors in the prostate and bladder neck resulting in fewer systemic side effects e.g. hypotension etc.
Many patients with hypertension and/or cardiac failure are already on ACE-Is and a diuretic and the introduction of an alpha blocker for incidental BPH may well provoke unexpected symptoms of postural hypotension often necessitating down tritation of the other anti hypertensive drugs. Good communication between cardiologists, GP and urologist is advisable.
2. Hypertension Prazosin and doxazosin are alpha receptor blockers which relax smooth muscle and reduce blood pressure by lowering peripheral vascular resistance. They are effective as single drug therapy in some individuals and obviously those presenting with BPH would be ideal candidates. Side effects are fairly common and include marked first dose hypotension and risk of syncope, palpitations, headache and nasal stuffiness. They have no adverse effects on serum lipids but this has not translated to benefit. The ALLHAT study showed that persons receiving doxazosin as single treatment had a
Alpha blockers have a lim-ited place but are not in-frequently used as add on therapy in resistant hy-pertension and sometimes as first choice when mild hypertension and sympto-matic BPH is the present-ing symptom.
Page 5 Volume 5 No 2 August 2014
significant increase in heart failure hospitalisations and higher risk of stroke relative to patients using chlorthalidone. They are therefore not generally used as initial agents except in patients with BPH (see ALLHAT study below).
Alpha blockers are more often used as 4th or 5th line treatment in resistant hypertension in patients already on beta blocker, CCB, ACE-Is/ARB and diuretic. The long acting examples e.g. doxazosin are valuable for controlling nocturnal and early morning hypertension.
3. Alpha blockers for cardiac failureAlpha blockers may be employed for their vasodilator effect in the treatment of cardiac failure when Ace Inhibitors and ARB’s are not tolerated but have largely fallen from favour after the findings of ALLHAT (see below).
4. Pheochromocytoma Alpha blockers have for many years been drugs of first choice in the preoperative treatment of pheochromocytoma. Phenoxybenzamine is a long acting non competitive alpha blocker most used. The initial starting dose is 10 mg, 12 hourly increased to a maintenance dose of 40 and 120 mg daily until optimal blockade is achieved (supine blood pressure below 160, standing blood pressure above 80/45 mm Hg).
Calcium blockers such as sustained release nifedipine are also effective and probably better tolerated and can be administered with alpha blockers. Labetalol (Trandate) is an intravenous alpha and beta blocker used in hypertensive crises.
Labetalol is now avoided in pheochro-mocytoma as it has been associated with post operative hypotension and interferes with measurement of uri-nary catecholamines.
5. Combined alpha/beta blockers (carvedilol and labetalol)Beta blockers antagonise the adverse effect of raised catecholamines in chronic heart failure. Beta blockers reduce mortality by reducing heart rate, increasing heart rate variability and improving ejection fraction. They also have direct anti arrhythmic properties.
Carvedilol is a non selective beta 1 and beta 2 receptor blocker with additional weak alpha blocking activity. It has been shown to improve prognosis in cardiac failure with reduction in death and hospitalisations. The benefit largely coming from reduction in heart rate but theoretically also because of it mild vasodilatory activity. Subsequent trials with beta 1 selective agents (bisoprolol and metoprolol) have shown similar reduction in mortality. Because of its alpha blocking activity carvedilol may cause more hypotension, dizziness and oedema.
Labetalol (Trandate) is an intravenous alpha beta blocker used for rapid control of hypertension in hypertensive emergencies and to induce controlled
hypertension under anaesthetic during surgical procedures. Its use in pheochromocytoma has largely been abandoned.
ConclusionAlpha blockers are widely used for benign prostatic hypertrophy and may cause postural hypotension. They are occasionally used as first line anti-hypertensive’s particularly in males with mild hypertension and bph and less commonly as 4th and 5th line additional drugs in resistant hypertension.
AddendumALLHAT trial (1994 to 2002) Anti Hypertensive and Lipid Lowering Treatment to Prevent Heart Attack compared chlorthalidone against doxazosin, lisinopril and amlodipine. Patients taking doxazosin had slightly better blood pressure control and a more favourable influence on lipids but a slightly increased cardiovascular risk (mainly stroke) and alarmingly twice the incidence of heart failure. Based on ALLHAT experience and a VA study in heart failure survival, alpha blockers are not usually 1st line therapy for hypertension or heart failure.
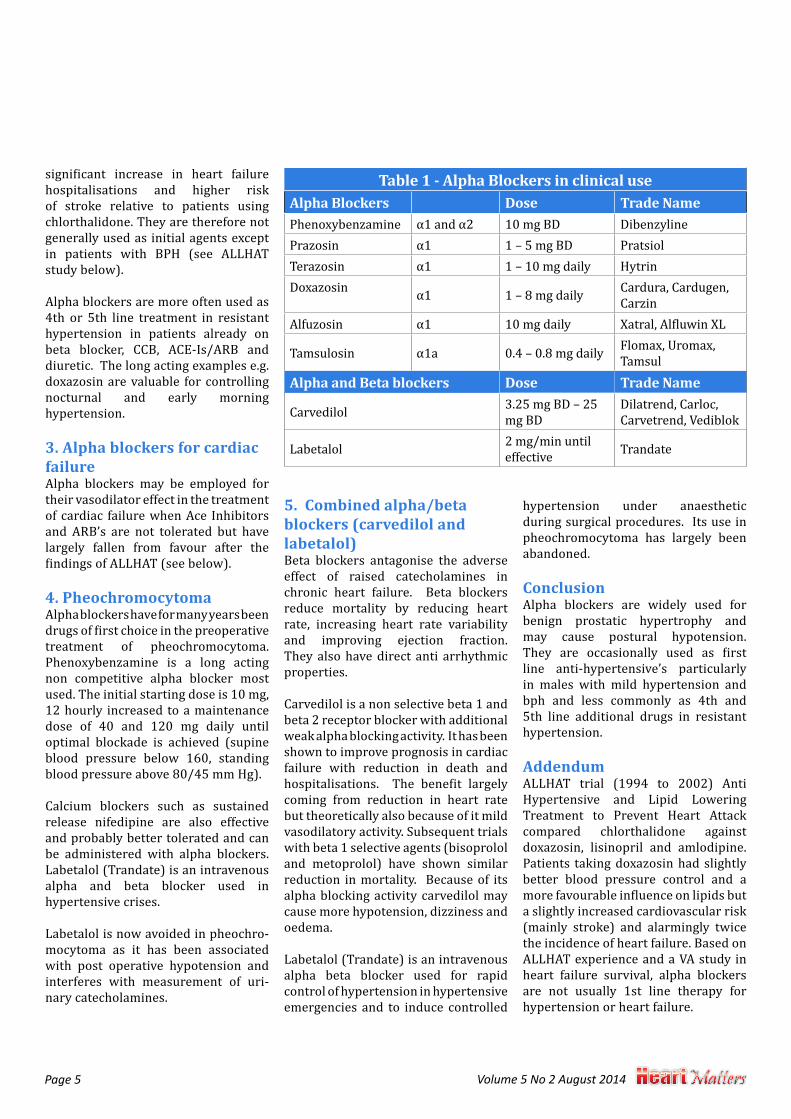
Table 1 - Alpha Blockers in clinical useAlpha Blockers Dose Trade NamePhenoxybenzamine α1 and α2 10 mg BD DibenzylinePrazosin α1 1 – 5 mg BD PratsiolTerazosin α1 1 – 10 mg daily HytrinDoxazosin α1 1 – 8 mg daily Cardura, Cardugen,
CarzinAlfuzosin α1 10 mg daily Xatral, Alfluwin XL
Tamsulosin α1a 0.4 – 0.8 mg daily Flomax, Uromax, Tamsul
Alpha and Beta blockers Dose Trade Name
Carvedilol 3.25 mg BD – 25 mg BD
Dilatrend, Carloc, Carvetrend, Vediblok
Labetalol 2 mg/min until effective Trandate
Volume 5 No 2 August 2014 Page 6
he World Health Organisation estimates that each year 15 million people suffer strokes worldwide.1 Stroke claims the lives of 5.8 million people
and another 5 million are left permanently disabled annually.2 Thrombolytic therapy for acute stroke was introduced in 1995 when the results of the NINDS Study with intravenous (iv) tissue plasminogen activator (tPA) were published.3 The ECASS 3 Trial suggested that extension up to 4½ hours may also be safe and effective.4 A pooled analysis of 8 major trials with tPA showed that the net benefit of tPA disappears beyond 4½ hours. It often fails to achieve reperfusion (particularly in large vessel occlusions), and is associated with a significant bleeding risk.5 Several attempts to develop thrombolytics with a better risk benefit profile than tPA failed.6 Third generation thrombolytics like Desmoteplase are more fibrin
specific with less neurotoxicity. Trials with this agent are still ongoing.7 The Diaz 4 Study (Desmoteplase) would also include subjects up to 9 hours addressing the issue of what to do with strokes out of the 4.5 hours time range. The IST 3 Trial for iv TPA up to 6 hours was negative for primary endpoints but subgroup analysis showed advantage for selective patients.8 It became evident from analysing the NINDS Study that iv tPA was not effective in large vessel stroke, which includes the internal carotid, proximal middle cerebral, basilar and vertebral arteries. Strokes due to occlusion of these arteries have a particularly high mortality and morbidity with very poor functional outcomes, especially if revascularisation could not be achieved. In a meta-analysis of the impact of reperfusion on stroke outcomes, successful recanalization of the affected artery was by far the most
important factor in improving stroke survival and functional outcomes (mortality 14.4% vs 41.6%, good outcome 58.1% vs 24.8% respectively).9 The Merci Retrieval System (Concentric Medical) was the first mechanical thromboembolectomy device developed for intracranial treatment of acute ischaemic stroke. It was FDA approved in August 2004 for patients who fail or who are ineligible for iv tPA. The Multi-Merci study showed successful recanalization occurred in 68%. In those patients successfully recanalized a good outcome (Modified Rankin Score (MRS) at 90 days post stroke ≤2) was seen in 49% vs 9.9% in those where recanalization failed. Mortality outcomes were 25% vs 52% respectively.10
New devices for mechanical embolectomy have become available over the last couple of years , include the Solitaire (EV-3) and Trevo (Concentric Medical) stent
Stroke remains a devastating disease. We believe the future of stroke therapy will parallel the evolution of treatment of ST elevation myocardial infarction, recognising that early reperfusion is critical to success.
In an era of older and newer reperfusion strategies applied in our stroke unit we did a retrospective analysis of our data base of all stroke patients admitted to the hospital from August 2011 – September 2012 (total of 196) and from Oct 2012 – Sept 2013 total of 204.
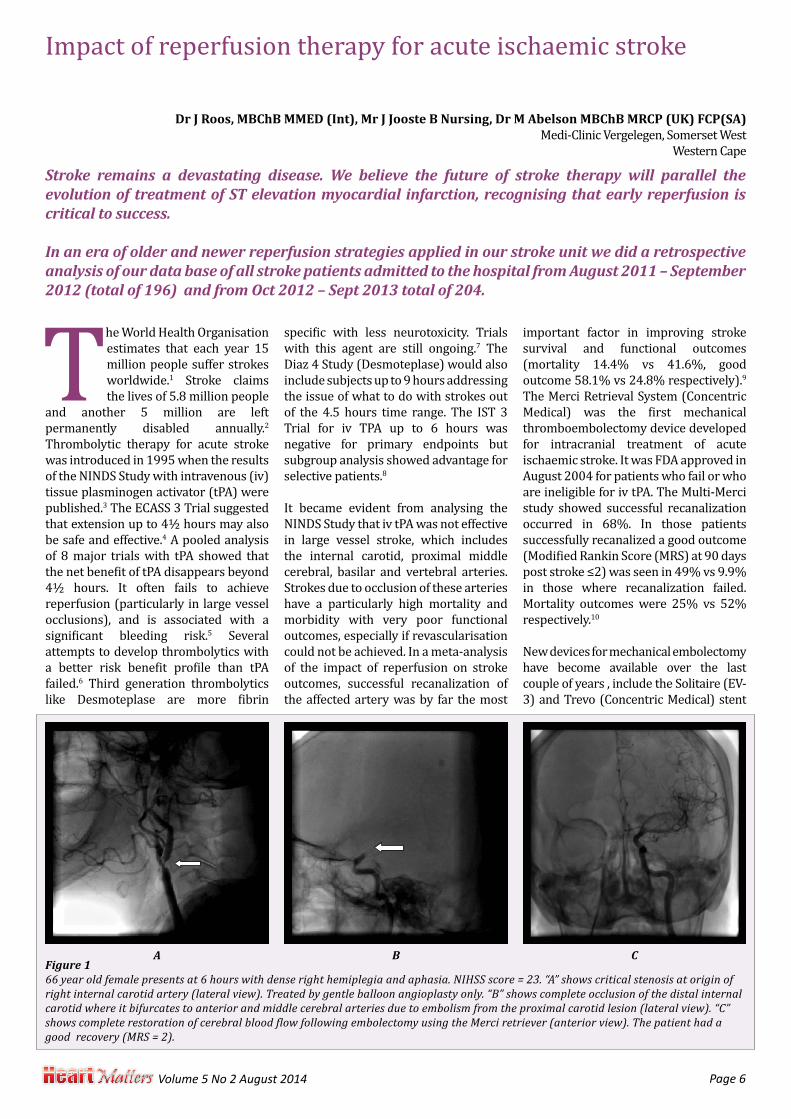
Figure 166 year old female presents at 6 hours with dense right hemiplegia and aphasia. NIHSS score = 23. “A” shows critical stenosis at origin of right internal carotid artery (lateral view). Treated by gentle balloon angioplasty only. “B” shows complete occlusion of the distal internal carotid where it bifurcates to anterior and middle cerebral arteries due to embolism from the proximal carotid lesion (lateral view). “C” shows complete restoration of cerebral blood flow following embolectomy using the Merci retriever (anterior view). The patient had a good recovery (MRS = 2).
Dr J Roos, MBChB MMED (Int), Mr J Jooste B Nursing, Dr M Abelson MBChB MRCP (UK) FCP(SA)Medi-Clinic Vergelegen, Somerset West
Western Cape
Impact of reperfusion therapy for acute ischaemic stroke
A B C
Page 7 Volume 5 No 2 August 2014
retrievers and the Penumbra system. The stent retrievers are quicker and technically easier to use with a significantly higher reperfusion rate (80+%) and less haemorrhage. The Swift Study comparing the Merci device to Solitaire in patients with large strokes who had failed iv tPA or ineligible and was stopped early as Solitaire was shown to be better.11 The Trevo 2 study also showed superiority versus Merci device with similar efficacy compared to the Solitaire.12 Both these devices are currently available in South Africa. Following the negative results from the IMS3 and MR rescue trials comparing mechanical embolectomy to standard therapy most interventional units became more selective doing intervention and reserving it mostly for patients with failed TPA or large artery occlusions (especially basilar) using the newer devices (Solitaire and Trevo).
In a study of 88 large ischaemic strokes due to acute middle cerebral artery occlusion patients received either iv tPA or, in those where iv tPA was contra-indicated, embolectomy using the Solitaire device. Despite the fact that those patients who underwent embolectomy had significantly larger strokes (NIHSS 14 vs 21) and strokes were of longer duration (134min vs 234min), a favourable clinical outcome (MRS ≤ 2) was seen significantly more frequently in the embolectomy patients (60% vs 37.5% p<0.001).13
Regarding diagnostic imaging in acute stroke, the Alberta Stroke Programme Early Computed Tomography Score
(Aspects) is an easy to use modality to assess a patient’s suitability to receive reperfusion therapy. Although the Aspects score has been criticized as being archaic and that we should use the more modern imaging modalities (multi-modal CT, perfusion CT and CT angiography or DWI-perfusion MRI mismatch) these imaging techniques are not always readily available, are more expensive and, of most importance, more time consuming - considering the principal of time is brain.14 New technology (CT angio perfusion) is now available and can be performed with minimal waste of time only using small contrast dosages and may be useful for selected patients without bleed or low Aspect score on the initial non contrasted screening CT.
Time to intervention post stroke onset is an area of ongoing study. Intravenous thrombolysis is of no benefit beyond 4.5 hours while intra-arterial tPA was shown to be of some benefit up to 6 hours post stroke onset. Mechanical embolectomy studies have included patients up to 8 hours and occasionally beyond with good outcomes in appropriately selected patients. In individuals with good collateral circulation, particularly via the pial arteries, the ischemic brain may remain viable, although non-functional, for up to 12 hours or more post stroke onset and these patients will respond well to late intervention.15 However, most patients will have had significant brain infarction by 6-8 hours post onset. The decision therefore, on whom to intervene on, has to be individualised and strict time guidelines are not appropriate.
Patients and methodsWe make use of an acute ischemic stroke management protocol based on the following:
1. Time interval from onset of stroke until admission to Emergency Unit
2. Severity of stroke graded as mild, moderate or severe using the NIHSS scoring system
3. Co-morbidities and contraindications for TPA
4. Radiological imaging carefully looking at early infarct changes (Most commonly CT scans using the Aspects score)
5. NIHSS scoring on admission and daily to monitor response to therapy
Mild strokes (NIHSS score of 7 or less) are not subjected to reperfusion strate-gies, but we prefer to admit them to ICU as they sometimes deteriorate and reas-sessment of management is then indi-cated. Moderate strokes (NIHSS score 8 – 16) get assessed for iv tPA according to the NINDS criteria and eligible patients are treated after admission to ICU. Severe strokes (NIHSS scores of 16 or more) are regarded as an extreme emergency and are assessed for reperfusion therapy (me-chanical embolectomy device) following angiography usually done in the cathe-terisation laboratory with occasional pa-tients having CT or MR angiography. Our unit started giving iv tPA in the late 90’s and mechanical embolectomy using the Merci Retriever began in 2007. For the past year or so only the Solitaire or Trevo stent retrievers are used.
We did a retrospective analysis of all stroke patients admitted to the hospital from the beginning of August 2011 till September 2012 and again from Oct 2012 to Sept 2013. There were a total of 196 patients and 204 in the two studies (all referrals or direct admissions from Somerset West and the surrounding areas). The average age was 71 and 70 years old, gender distribution equal - men and women (51 vs. 45%) and (43 versus 57). There were 90% ischemic and 10% haemorrhagic strokes. A significant improvement at time of discharge (good functional recovery) occurred in 142 (72%) and 145 (71%) patients. 19 (10%) and 19 (9%) died in hospital and no improvement was seen in 29 (15%) and 36 (18%) by the time of discharge. Ninety (46%) and 115 (56%) patients were admitted to the ICU. The average hospital stay was 5.8 and 6 days.
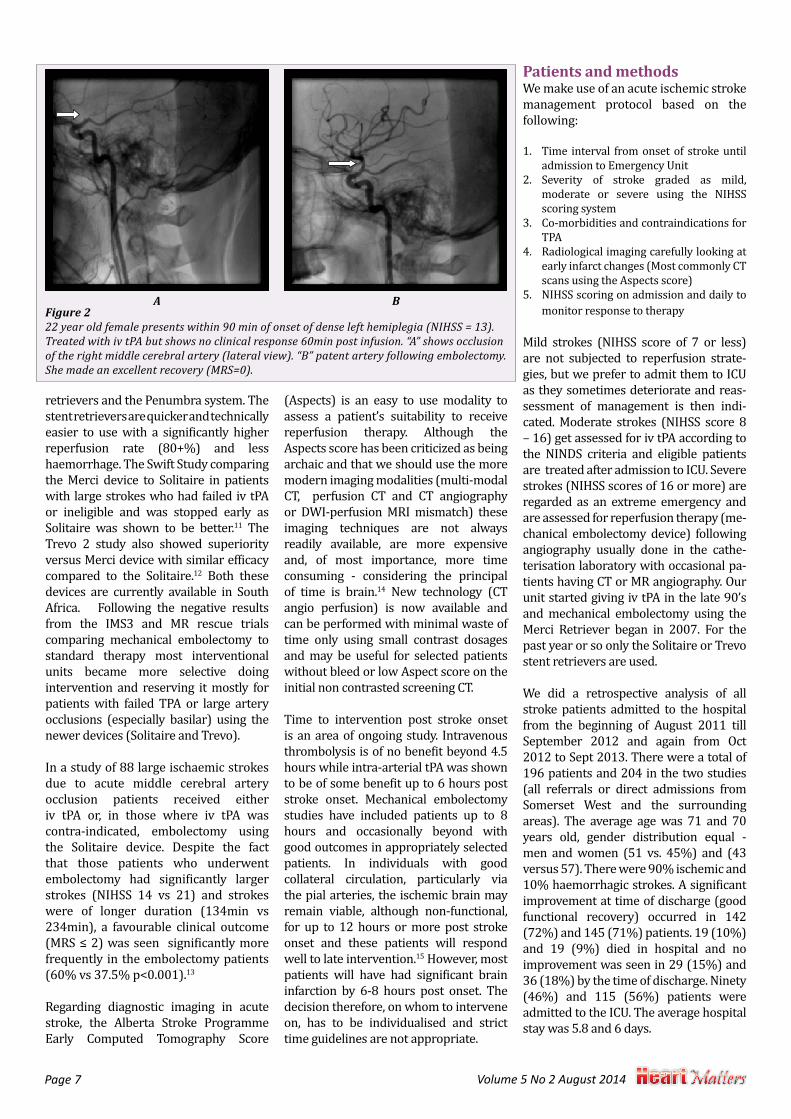
Figure 222 year old female presents within 90 min of onset of dense left hemiplegia (NIHSS = 13). Treated with iv tPA but shows no clinical response 60min post infusion. “A” shows occlusion of the right middle cerebral artery (lateral view). “B” patent artery following embolectomy. She made an excellent recovery (MRS=0).
A B
Volume 5 No 2 August 2014 Page 8
The average time period from start of symptoms to admission was 12 and 7 hours. Using the NIHSS score the severity was judged to be mild in 118 (60%) and 125 (61%), moderate 42 (21%) and 44 (22%) and severe 36 (18%) and 35 (17%). In the moderate to severe cohort
(n=78) and (n=79) 22 patients (28%) and 15 (18%) were treated with iv tPA and 21 (27%) and 18 (22%) went to the Catheterization Laboratory for head and neck angiography via the femoral artery. Mechanical embolectomy (occasionally including carotid angioplasty, carotid
stent, or intra-cerebral tPA) was performed if deemed suitable by the interventionalist.
Two patients with severe stroke and large artery occlusions who should have been referred for possible mechanical embolectomy according to our protocol, received iv tPA instead, due to unavailability of the interventionalist. Both did not respond to iv tPA and died.
One patient in the interventional group had a massive acute intra-cerebral haemorrhage a few hours after successful embolectomy of an occluded right internal carotid artery and died. He was a “wake up stroke” (duration unknown) who presented with a severe neurological defect but due to a favourable Aspects score on CT scan was given the benefit of doubt and referred for mechanical embolectomy.
DiscussionDespite our efforts to educate the public and ambulance service, many patients still get to hospital too late for reperfusion therapy. Furthermore, many are still judged to be ineligible for iv tPA and mechanical intervention due to other co-morbidities, financial considerations and imaging features indicating significant cerebral infarction.
We believe that this cohort of patients in general did quite well compared to other published stroke unit data and that optimal management in the first 24 hours makes a significant difference in outcome, with shorter hospital stay and better functional recovery. We would like to encourage other hospitals in South Africa to start Acute Stroke Units for thrombolytic treatment and possibly offer mechanical embolectomy for patients with failed or ineligible for TPA, who otherwise have no chance of cerebral reperfusion the strongest predictor of an improved clinical outcome.9,10,13
Reperfusion therapy for acute ischemic stroke lags far behind coronary intervention for acute myocardial infarction. The brain is a much more complicated and delicate organ. We need continued research and improvements in interventional therapies to optimize acute stroke intervention and help better select those patients who will benefit most from these procedures.
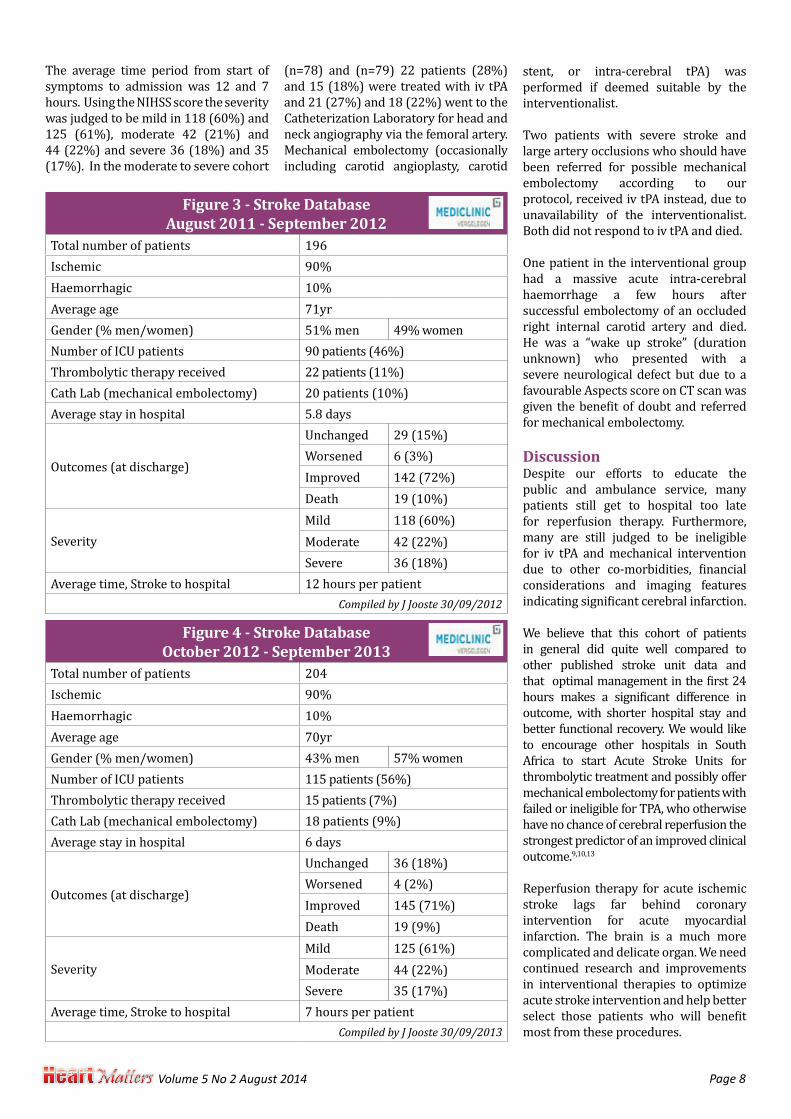
Figure 3 - Stroke Database August 2011 - September 2012
Total number of patients 196Ischemic 90%Haemorrhagic 10%Average age 71yrGender (% men/women) 51% men 49% womenNumber of ICU patients 90 patients (46%)Thrombolytic therapy received 22 patients (11%)Cath Lab (mechanical embolectomy) 20 patients (10%)Average stay in hospital 5.8 days
Outcomes (at discharge)
Unchanged 29 (15%) Worsened 6 (3%) Improved 142 (72%)Death 19 (10%)
SeverityMild 118 (60%)Moderate 42 (22%)Severe 36 (18%)
Average time, Stroke to hospital 12 hours per patientCompiled by J Jooste 30/09/2012
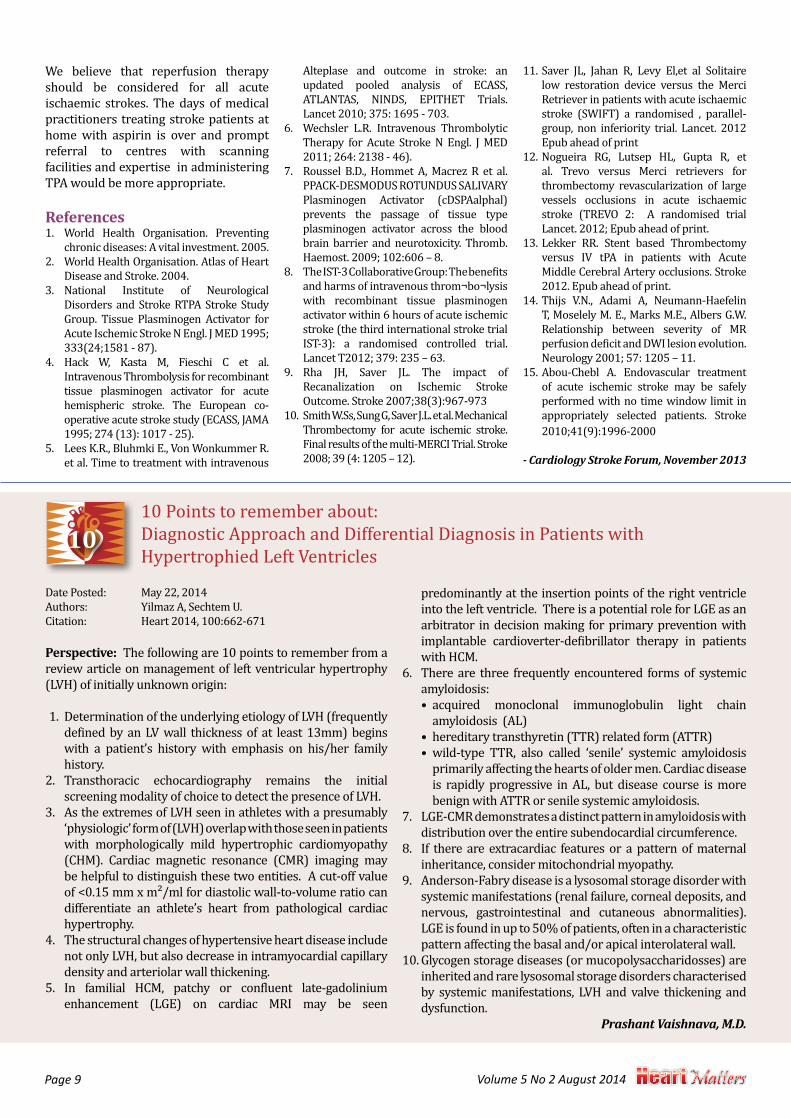
Figure 4 - Stroke Database October 2012 - September 2013
Total number of patients 204Ischemic 90%Haemorrhagic 10%Average age 70yrGender (% men/women) 43% men 57% womenNumber of ICU patients 115 patients (56%)Thrombolytic therapy received 15 patients (7%)Cath Lab (mechanical embolectomy) 18 patients (9%)Average stay in hospital 6 days
Outcomes (at discharge)
Unchanged 36 (18%) Worsened 4 (2%)Improved 145 (71%) Death 19 (9%)
SeverityMild 125 (61%)Moderate 44 (22%)Severe 35 (17%)
Average time, Stroke to hospital 7 hours per patientCompiled by J Jooste 30/09/2013
Page 9 Volume 5 No 2 August 2014
We believe that reperfusion therapy should be considered for all acute ischaemic strokes. The days of medical practitioners treating stroke patients at home with aspirin is over and prompt referral to centres with scanning facilities and expertise in administering TPA would be more appropriate.
References1. World Health Organisation. Preventing
chronic diseases: A vital investment. 2005.2. World Health Organisation. Atlas of Heart
Disease and Stroke. 2004.3. National Institute of Neurological
Disorders and Stroke RTPA Stroke Study Group. Tissue Plasminogen Activator for Acute Ischemic Stroke N Engl. J MED 1995; 333(24;1581 - 87).
4. Hack W, Kasta M, Fieschi C et al. Intravenous Thrombolysis for recombinant tissue plasminogen activator for acute hemispheric stroke. The European co-operative acute stroke study (ECASS, JAMA 1995; 274 (13): 1017 - 25).
5. Lees K.R., Bluhmki E., Von Wonkummer R. et al. Time to treatment with intravenous
Alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTAS, NINDS, EPITHET Trials. Lancet 2010; 375: 1695 - 703.
6. Wechsler L.R. Intravenous Thrombolytic Therapy for Acute Stroke N Engl. J MED 2011; 264: 2138 - 46).
7. Roussel B.D., Hommet A, Macrez R et al. PPACK-DESMODUS ROTUNDUS SALIVARY Plasminogen Activator (cDSPAalphal) prevents the passage of tissue type plasminogen activator across the blood brain barrier and neurotoxicity. Thromb. Haemost. 2009; 102:606 – 8.
8. The IST-3 Collaborative Group: The benefits and harms of intravenous throm¬bo¬lysis with recombinant tissue plasminogen activator within 6 hours of acute ischemic stroke (the third international stroke trial IST-3): a randomised controlled trial. Lancet T2012; 379: 235 – 63.
9. Rha JH, Saver JL. The impact of Recanalization on Ischemic Stroke Outcome. Stroke 2007;38(3):967-973
10. Smith W.Ss, Sung G, Saver J.L. et al. Mechanical Thrombectomy for acute ischemic stroke. Final results of the multi-MERCI Trial. Stroke 2008; 39 (4: 1205 – 12).
11. Saver JL, Jahan R, Levy El,et al Solitaire low restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT) a randomised , parallel-group, non inferiority trial. Lancet. 2012 Epub ahead of print
12. Nogueira RG, Lutsep HL, Gupta R, et al. Trevo versus Merci retrievers for thrombectomy revascularization of large vessels occlusions in acute ischaemic stroke (TREVO 2: A randomised trial Lancet. 2012; Epub ahead of print.
13. Lekker RR. Stent based Thrombectomy versus IV tPA in patients with Acute Middle Cerebral Artery occlusions. Stroke 2012. Epub ahead of print.
14. Thijs V.N., Adami A, Neumann-Haefelin T, Moselely M. E., Marks M.E., Albers G.W. Relationship between severity of MR perfusion deficit and DWI lesion evolution. Neurology 2001; 57: 1205 – 11.
15. Abou-Chebl A. Endovascular treatment of acute ischemic stroke may be safely performed with no time window limit in appropriately selected patients. Stroke 2010;41(9):1996-2000
- Cardiology Stroke Forum, November 2013
10 Points to remember about: Diagnostic Approach and Differential Diagnosis in Patients with Hypertrophied Left Ventricles
Date Posted: May 22, 2014Authors: Yilmaz A, Sechtem U.Citation: Heart 2014, 100:662-671
Perspective: The following are 10 points to remember from a review article on management of left ventricular hypertrophy (LVH) of initially unknown origin:
1. Determination of the underlying etiology of LVH (frequently defined by an LV wall thickness of at least 13mm) begins with a patient’s history with emphasis on his/her family history.
2. Transthoracic echocardiography remains the initial screening modality of choice to detect the presence of LVH.
3. As the extremes of LVH seen in athletes with a presumably ‘physiologic’ form of (LVH) overlap with those seen in patients with morphologically mild hypertrophic cardiomyopathy (CHM). Cardiac magnetic resonance (CMR) imaging may be helpful to distinguish these two entities. A cut-off value of <0.15 mm x m²/ml for diastolic wall-to-volume ratio can differentiate an athlete’s heart from pathological cardiac hypertrophy.
4. The structural changes of hypertensive heart disease include not only LVH, but also decrease in intramyocardial capillary density and arteriolar wall thickening.
5. In familial HCM, patchy or confluent late-gadolinium enhancement (LGE) on cardiac MRI may be seen
predominantly at the insertion points of the right ventricle into the left ventricle. There is a potential role for LGE as an arbitrator in decision making for primary prevention with implantable cardioverter-defibrillator therapy in patients with HCM.
6. There are three frequently encountered forms of systemic amyloidosis: • acquired monoclonal immunoglobulin light chain
amyloidosis (AL)• hereditary transthyretin (TTR) related form (ATTR)• wild-type TTR, also called ‘senile’ systemic amyloidosis
primarily affecting the hearts of older men. Cardiac disease is rapidly progressive in AL, but disease course is more benign with ATTR or senile systemic amyloidosis.
7. LGE-CMR demonstrates a distinct pattern in amyloidosis with distribution over the entire subendocardial circumference.
8. If there are extracardiac features or a pattern of maternal inheritance, consider mitochondrial myopathy.
9. Anderson-Fabry disease is a lysosomal storage disorder with systemic manifestations (renal failure, corneal deposits, and nervous, gastrointestinal and cutaneous abnormalities). LGE is found in up to 50% of patients, often in a characteristic pattern affecting the basal and/or apical interolateral wall.
10. Glycogen storage diseases (or mucopolysaccharidosses) are inherited and rare lysosomal storage disorders characterised by systemic manifestations, LVH and valve thickening and dysfunction.
Prashant Vaishnava, M.D.

Volume 5 No 2 August 2014 Page 10
Case-report:
Young man with dyspnoeaDr Mike Bennett
CardiologistWilgers Hospital, Pretoria
28-year male presented with new-onset shortness of breath. He exercised regu-larly for the past 8 years but noticed that he had difficulty
in doing the same intensity of exercise he had always done. Over the years he took his heart rate every morning and noticed that it was higher than usual. Six months earlier, he underwent an insurance exam-ination including, a treadmill exercise ECG, and no abnormalities were detected. He has always been healthy and apart from an appendectomy at the age of ten, he had never been admitted to a hospital.
Clinical examination was unremarkable. Resting heart rate was 86/minute with occasional ectopic beats. Blood pres-sure and cardiac examination were nor-mal and no murmurs or abnormal heart sounds were audible.
Resting ECG showed a sinus rhythm, P-Q interval 0.24 ms, normal axis and QTc interval. Nonspecific ST-segment changes were present in the infero-lateral leads. M-mode echocardiograhy revealed a moderately dilated left ventricle (LV) of 64 mm diastolic diameter and the LV ejection fraction (EF) was 44% with mild general hypocontractility. No pericardial fluid or significant valvular disease (only trivial mitral and tricuspid regurgitation) were present. Blood count was normal and C-reactive protein levels were 21(normal= <10); high sensitivity troponin T 24 ng/L (N= <14) and pro-BNP levels of 522 (N=<300). No other biochemical abnormalities were detected. Chest X-ray was normal.
When asked specifically about a recent infection, he remembered a mild flu-like syndrome 3-4 weeks ago which at the time, was considered not severe enough to interrupt his exercise programme.
A clinical diagnosis of a viral myocarditis was made.
DiscussionThe diagnosis of viral myocarditis is complicated by the highly variable clinical presentation and the lack of a specific
biomarker or non-invasive test to confirm the clinical suspicion. Myocardial biopsy remains the gold standard but is not practical as a routine tool to confirm the diagnosis in the vast majority of patients with suspected myocarditis.
CausesAlthough there are many causes, the most common include idiopathic, viral (Group B Coxsackie virus, adenovirus, parvovirus B19, influenza virus, HIV) and rheumatic fever.
PathogenesisViral myocarditis is the result of viral proliferation and the immune response of the host. Using murine enteroviral models of myocarditis, the disease process can be divided into 3 phases:
1. Viral. After proliferation in the permissive tissue, the virus reaches the myocardium via haematogenous and/or lymphatic spread. Coxsackie group B and some adenoviruses use a special membrane receptor for internalization of the viral genome into the myocyte. Adenoviruses use special integrins as coreceptors. The receptors may partially explain why coxsackie- and adenoviruses are common causative viruses for myocarditis.
2. Subacute. ≈3-21 days. The immune response of the host is a major determinant of patient outcome. It needs to be sufficient to eliminate as many virus-infected cells as possible but modulated and turned off when appropriate; otherwise excessive tissue damage may lead to myocardial dysfunction.
3. Myopathic stage. Viral persistence may result in prolonged antigenic trigger, chronic immune activation and the potential for a cardiomyopa-thy. This chronic inflammatory pro-cess is accompanied by the release of several cytokines that can cause digestion of the interstitial collagen and elastin framework of the heart, participation in the inflammation, stimulation of profibrotic factors with pathological fibrosis and finally
results in cardiac dilatation, dysfunc-tion and progressive heart failure.
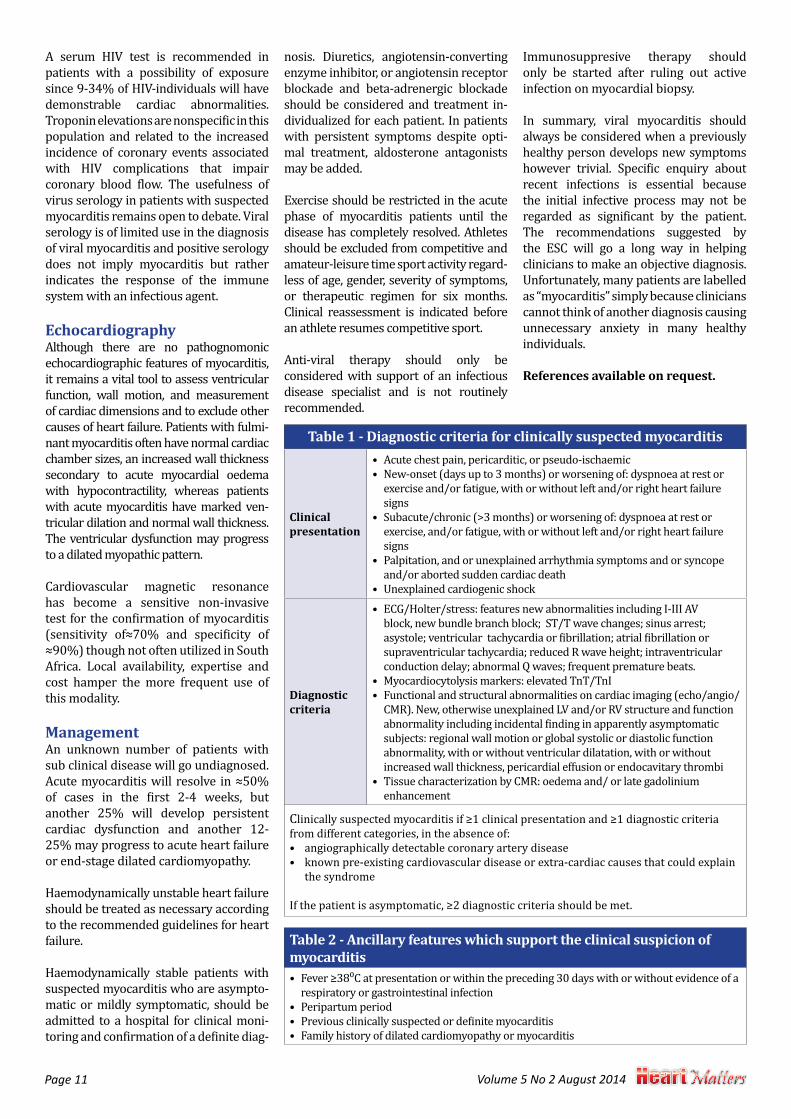
Clinical presentationThe acute phase of viral myocarditis is usually (and unfortunately) asymptomatic and symptoms will depend on the severity of the viral infection. Most patients will recover fully and never realize that they had myocarditis. The European Society of Cardiology working Group on Myocardial and Pericardial Diseases criteria for the diagnosis of clinically suspected myocarditis, are presented in Tables 1 and 2. Symptoms and signsThere is no single symptom or clinical sign diagnostic of myocarditis. Palpitations due to arrhythmias or new sinus tachycardia may be the presenting symptom. Chest pain is uncommon and usually associated with pericardial involvement. Dyspnoea on exertion should alert the clinician to look for other signs of heart failure.
Diagnosis Myocardial biopsy is the gold standard but its use is limited to specific clinical situations with a rapidly progressive course where giant cell or eosinophilic myocarditis is suspected.
ECGA normal ECG does not exclude myocarditis. ECG changes are nonspecific and range from sinus tachycardia, ST-segment and T-wave abnormalities, atrioventricular and bundle branch block, ventricular ectopic beats and other arrhythmias. A QTc prolongation>440 ms, QRS duration of >120 ms, an abnormal QRS axis and ventricular ectopic beats are associated with poor clinical outcomes.
BiochemistryElevated infection markers (leucocyto-sis, erythrocyte sedimentation rate, CRP) may reflect an infectious cause. Cardiac troponin levels are elevated in 30-50% of patients with myocarditis and seem to be more common among patients with ≤1 month of heart failure symptoms.
Page 11 Volume 5 No 2 August 2014
A serum HIV test is recommended in patients with a possibility of exposure since 9-34% of HIV-individuals will have demonstrable cardiac abnormalities. Troponin elevations are nonspecific in this population and related to the increased incidence of coronary events associated with HIV complications that impair coronary blood flow. The usefulness of virus serology in patients with suspected myocarditis remains open to debate. Viral serology is of limited use in the diagnosis of viral myocarditis and positive serology does not imply myocarditis but rather indicates the response of the immune system with an infectious agent.
EchocardiographyAlthough there are no pathognomonic echocardiographic features of myocarditis, it remains a vital tool to assess ventricular function, wall motion, and measurement of cardiac dimensions and to exclude other causes of heart failure. Patients with fulmi-nant myocarditis often have normal cardiac chamber sizes, an increased wall thickness secondary to acute myocardial oedema with hypocontractility, whereas patients with acute myocarditis have marked ven-tricular dilation and normal wall thickness. The ventricular dysfunction may progress to a dilated myopathic pattern.
Cardiovascular magnetic resonance has become a sensitive non-invasive test for the confirmation of myocarditis (sensitivity of≈70% and specificity of ≈90%) though not often utilized in South Africa. Local availability, expertise and cost hamper the more frequent use of this modality.
ManagementAn unknown number of patients with sub clinical disease will go undiagnosed. Acute myocarditis will resolve in ≈50% of cases in the first 2-4 weeks, but another 25% will develop persistent cardiac dysfunction and another 12-25% may progress to acute heart failure or end-stage dilated cardiomyopathy.
Haemodynamically unstable heart failure should be treated as necessary according to the recommended guidelines for heart failure.
Haemodynamically stable patients with suspected myocarditis who are asympto-matic or mildly symptomatic, should be admitted to a hospital for clinical moni-toring and confirmation of a definite diag-
nosis. Diuretics, angiotensin-converting enzyme inhibitor, or angiotensin receptor blockade and beta-adrenergic blockade should be considered and treatment in-dividualized for each patient. In patients with persistent symptoms despite opti-mal treatment, aldosterone antagonists may be added.
Exercise should be restricted in the acute phase of myocarditis patients until the disease has completely resolved. Athletes should be excluded from competitive and amateur-leisure time sport activity regard-less of age, gender, severity of symptoms, or therapeutic regimen for six months. Clinical reassessment is indicated before an athlete resumes competitive sport.
Anti-viral therapy should only be considered with support of an infectious disease specialist and is not routinely recommended.
Immunosuppresive therapy should only be started after ruling out active infection on myocardial biopsy.
In summary, viral myocarditis should always be considered when a previously healthy person develops new symptoms however trivial. Specific enquiry about recent infections is essential because the initial infective process may not be regarded as significant by the patient. The recommendations suggested by the ESC will go a long way in helping clinicians to make an objective diagnosis. Unfortunately, many patients are labelled as “myocarditis” simply because clinicians cannot think of another diagnosis causing unnecessary anxiety in many healthy individuals.
References available on request.
Table 1 - Diagnostic criteria for clinically suspected myocarditis
Clinical presentation
• Acute chest pain, pericarditic, or pseudo-ischaemic• New-onset (days up to 3 months) or worsening of: dyspnoea at rest or
exercise and/or fatigue, with or without left and/or right heart failure signs
• Subacute/chronic (>3 months) or worsening of: dyspnoea at rest or exercise, and/or fatigue, with or without left and/or right heart failure signs
• Palpitation, and or unexplained arrhythmia symptoms and or syncope and/or aborted sudden cardiac death
• Unexplained cardiogenic shock
Diagnostic criteria
• ECG/Holter/stress: features new abnormalities including I-III AV block, new bundle branch block; ST/T wave changes; sinus arrest; asystole; ventricular tachycardia or fibrillation; atrial fibrillation or supraventricular tachycardia; reduced R wave height; intraventricular conduction delay; abnormal Q waves; frequent premature beats.
• Myocardiocytolysis markers: elevated TnT/TnI• Functional and structural abnormalities on cardiac imaging (echo/angio/
CMR). New, otherwise unexplained LV and/or RV structure and function abnormality including incidental finding in apparently asymptomatic subjects: regional wall motion or global systolic or diastolic function abnormality, with or without ventricular dilatation, with or without increased wall thickness, pericardial effusion or endocavitary thrombi
• Tissue characterization by CMR: oedema and/ or late gadolinium enhancement
Clinically suspected myocarditis if ≥1 clinical presentation and ≥1 diagnostic criteria from different categories, in the absence of: • angiographically detectable coronary artery disease• known pre-existing cardiovascular disease or extra-cardiac causes that could explain
the syndrome
If the patient is asymptomatic, ≥2 diagnostic criteria should be met.
Table 2 - Ancillary features which support the clinical suspicion of myocarditis• Fever ≥38⁰C at presentation or within the preceding 30 days with or without evidence of a
respiratory or gastrointestinal infection• Peripartum period• Previous clinically suspected or definite myocarditis• Family history of dilated cardiomyopathy or myocarditis

Volume 5 No 2 August 2014 Page 12
Prof Gert Saayman MBChB MMed(MedForens) FCForPath(SA)Department of Forensic Medicine, Faculty of Health Sciences, University of Pretoria, Pretoria
EthicsDeath certification and notification: Key points for medical practitioners
nnually, nearly three-quarters of a million people die in South Africa. Many of these deaths are due to unnatural causes and very
many are due to illnesses and conditions which are preventable and result in death at a relatively young age. Doctors play a vital role in regulating the process which follows on the death of a person. Section 15 of the Registration of Births and Deaths Act (Act 51 of 1992), states as follows:
“Where a medical practitioner is satisfied that the death of any person who was attended before his death by the medical practitioner was due to natural causes, he shall issue a prescribed certificate stating the cause of death”.
Although provision has been made for persons other than medical doctors to issue death notification forms (in exceptional circumstances), the vast majority of such forms are issued by medical practitioners who had attended to patients before their demise. Remember that such a “prescribed certificate” comprises the death notification form (form DHA1663), which is a precursor document to the true “death certificate”, the latter being issued by the Department of Home Affairs, once the population register details, etc., have been properly completed. Doctors should appreciate the vital and valuable role which they fulfil as custodians of the process of death registration, both in terms of the quality of data submitted (specific medical cause of death) and the legal implications (for instance, in distinguishing between natural and/or non-natural causes of death and in confirming the identity of the deceased).
There are thus essentially three elements pertaining to the issuing of death notification forms (DNF’s), to which doctors should pay close attention: these are the identity of the deceased, the distinction between natural and other than natural death and the formulation of the cause of death.
Where a doctor is called upon to issue a certificate for a patient whom the doctor had been treating, there is no specific legal requirement that the doctor must physically see the body of the deceased before issuing such a death certificate. In cases where the deceased is a known patient of the practitioner and/or where the family members are known to the doctor and where the circumstances of death are appropriately documented and corroborated, it will thus not be necessary for the attending practitioner to personally view and/or identify the deceased.
A doctor may be called upon to issue a death notification form for a person whom the doctor has not personally previously attended to. This may apply, for example, where the medical practitioner is acting as a locum tenens or when the doctor is attached to a state hospital where the patient may have been receiving out-patient treatment but where the doctor may not have personally known the patient. However, legal prescriptions then apply: Section 15 of the Births and Deaths Registration Act further provides that “A medical practitioner who did not attend any person before his death but after the death of the person examined the corpse and is satisfied that the death was due to natural causes, may issue a prescribed certificate to that effect”.
It is thus essential that the doctor insist upon seeing the body of deceased person, before issuing a certificate - even if this means that the body of the deceased be brought to the hospital/surgery by the funeral undertakers.
It is strongly recommended, in cases where the doctor on duty had not personally known or previously treated the patient, that additional steps are taken to ensure accuracy of the diagnosis provided on the DNF and to reliably certify the identity of the deceased. Such steps may require that formal statements or depositions be made by competent witnesses and/or next of kin, or by a police officer, confirming the identity of the deceased and for certified copies of identity documents to be made available to the doctor. It is also strongly advised that the doctor will ensure in such cases, that copies of supporting documentation or information (affidavits, identity documents) will be retained on the file of the patient. It will also be advisable, where the doctor may be unsure as to the accuracy and reliability of information supplied to him regarding the circumstances of death and the events immediately preceding the death of the patient (eg. where the patient did not die in hospital but at home), for the doctor to request that formal statements/depositions be made in this regard, by family members, witnesses and/or police officers - and once again, for copies of such documents to be retained on the patient file.
A primary function of medical practitioners in the event of the demise of a patient, is to distinguish between deaths which were due to natural causes and those which may have been due to unnatural causes. Section 2 of the Inquests Act (Act 58 of 1959) prescribes that “any person who has reason to believe that any other person has died and that death was due to other than natural causes, shall as soon as possible report accordingly to a policeman, unless he has reason to
Although provision has been made for
persons other than medical doctors to
issue death notification forms (in exceptional
circumstances), the vast majority of such forms
are issued by medical practitioners who had
attended to patients before their demise.

Page 13 Volume 5 No 2 August 2014
believe that a report has been or will be made by any other person”.
The death notification form which doctors have to complete upon the demise of a patient, thus requires that doctors clearly state whether the death may have been due other than natural causes. It is therefore essential that practitioners are fully aware of the criteria and parameters which should be applied in this distinction. In fact, specific legislative provisions will inform this decision.
The Regulations Regarding the Rendering of Forensic Pathology Services (gazetted in 2007 in terms of the National Health Act, 2004) state that an unnatural death, for the purposes of the medico-legal investigation of death, shall be any one of the following:
a. any death due to physical or chemical influence, direct or indirect, or related complications;
b. any death, including those deaths which would normally be considered to be a death due to natural causes, which in the opinion of a medical practitioner, has been the result of an act of commission or omission which may be criminal in nature; or
c. where the death is sudden and unexpected, or unexplained, or where the cause of death is not apparent.
It is clear that any death which follows causally from an event or circumstance which inflicted injury or insult to the body, or from a complication which subsequently arises in consequence thereto, will be deemed an unnatural death.
Subsection (b) above clearly provides for the reporting and medico-legal investigation of deaths where there are reasons to believe that death was due to negligence (or a failure to act), on behalf of someone who had a legal duty to act. Thus, if (medical) negligence is implicated in the death of a patient,
such as failure to act appropriately or failing to make a diagnosis which could reasonably have been expected under the circumstances, it may constitute a scenario where death due to an otherwise natural cause (eg. malaria), may in fact constitute an unnatural death! In such cases, the basis for such allegation or consideration of unnatural death should be provided to the police and state pathologist, preferably in written format, as inquest dockets will not readily be opened on vague verbal allegations of negligence.
Although sudden and unexpected deaths may indeed be due to entirely natural causes, the default position in such cases will be that death was due to unnatural causes, until such time as a medical practitioner can reliably certify that the death was due to natural causes.
In addition, the provisions of the Health Professions Amendment Act (Act 29 of 2007) state that “The death of a person undergoing, or as a result of, a procedure of a therapeutic, diagnostic or palliative nature, or of which any aspect of such a procedure has been a contributory cause, shall not be deemed to be a death from natural causes”. It is thus clear that the legislation has been amended to provide not only for the mandatory reporting and medico-legal investigation of so-called “anaesthetic” or “theatre deaths”, but also for all deaths where medical treatment or intervention (of a diagnostic or therapeutic nature), or complications related thereto, may have played a role.
This is indeed an extremely inclusive definition of unnatural death and one which not only places an exceptional burden on state investigative resources, but also greatly adds to delays in the finalisation of legal and administrative processes following death (eg. insurance and pension payouts, settling of estates, etc.). Doctors should note that there is no rule prescribing that deaths which take place within 24 hours of the administration of an anaesthetic require reporting as being unnatural deaths.
Perhaps the most vexing problem facing epidemiologists and mortality statisticians (and accordingly, health policy makers and planners), is the inaccuracy of the “cause of death” formulation by doctors. Doctors should carefully distinguish between the “primary medical cause of death”, which is the underlying medical condition, and the consequences thereof, being the secondary disease developments and complications which may ultimately result in the death of the patient. A typical illustrative example would be the patient who dies of terminal cerebral haemorrhage (stroke), but where the underlying medical condition (primary medical cause of death) is that of essential hypertension.
Although sudden and unexpected deaths may
indeed be due to entirely natural causes, the
default position in such cases will be that death
was due to unnatural causes, until such time as
a medical practitioner can reliably certify that the
death was due to natural causes.

Volume 5 No 2 August 2014 Page 14
CPD AccreditationDoctors can acquire CPD points with this newsletter by visiting www.saheart.org.za (cardiologists), www.mycpd.co.za, www.mycpd.co.za or www.annlakecpd.co.za (GPs and physicians) and completing an online form of ±15 questions. Accreditation is available only for a limited time on the site. Should you have any queries regarding the accreditation, please contact E2 Solutions at: 011 340 9100 or [email protected].
An important further consideration here is that the law requires that the primary medical cause of death be divulged, even if the diagnosis or information may be deemed “sensitive” or confidential (such as HIV/AIDS, etc). Practitioners should take reasonable steps to ensure that the certificate is sealed and marked as confidential, but should not refrain from providing the correct and accurate diagnosis, based on (for example) a request by family members or the consideration that patient privacy will be compromised.
In some countries, there is a legal specification that a practitioner may not issue a death certificate in the event where the doctor had not seen or attended to the patient for a specified period before the demise of the patient (for example, two weeks or one month). There is no such legal provision in South African law, although it is clear that a doctor should be particularly careful if he had last seen a patient long before his demise and/or where the circumstances preceding the death of the patient were unclear and/or not clearly related to the condition for which the doctor had last attended to the patient.
In the event of a subsequent query pertaining to the content of a death notification form, as provided by a medical practitioner, the latter should always be in a position to demonstrate that he had (contemporaneously)
properly reviewed the facts and circumstances pertaining to the event, and that he had arrived at a rational and considered decision as to the identity of the deceased and the actual (primary) medical cause of death. In other words, the doctor may be called upon to show that he had “applied his mind” to these circumstances and factors. It is thus clear that the doctor should keep appropriate notes pertaining to the event (with reference to information which had been provided, names of persons involved, including family members, SAPS officers, nurses, etc.).
Junior doctors who work in a team context (e.g. interns and community service doctors) will be well advised to take great care in ensuring that they have established all the relevant facts
(identity, diagnosis, possible role of medical treatment or other non-natural causes in contributing to death), before completing death notification forms. Consulting with senior colleagues regarding the nature and content of certificates and making concise entries in the patient file on the outcome of such consultations, is strongly recommended.
It is also important for doctors to realise that they may not charge a fee for the issuing of death notification forms and that such forms should be issued without delay, as such delays may have very negative effects on the emotional status of next of kin (inter alia by retarding funeral arrangements, etc.), whilst also compromising the administration of justice, especially if medico-legal investigative processes are to be initiated.
Death notification forms are documents upon which weighty further legal decisions are based and administrative processes are implemented. The issuing of such documents should not be taken lightly and all doctors should be well informed as to the statutory provisions which apply. The incorrect or inappropriate issuing of death notification forms unfortunately constitute a relatively common reason for disciplinary proceedings being instituted against medical practitioners at the Health Professions Council of SA.
Doctors should carefully distinguish between
the “primary medical cause of death”, which is the underlying medical
condition, and the consequences thereof,
being the secondary disease developments
and complications which may ultimately result in the death of the patient.
Page 15 Volume 5 No 2 August 2014
The impact of the Coronary Collateral Circulation on Outcomes in Patients with Acute Coronary Syndromes: Results from the Acuity Trial
Meier P, Lansky AJ, Fahy M, et alHeart 2014, 100: 647-651
Study QuestionWhat is the prognostic implication of collateral circulation in patients presenting with acute coronary syndrome (ACS)?
MethodsThe coronary collateral circulation was assessed by an independent angiographic core laboratory using the Rentrop Score in patients enrolled in the randomised ACUITY (Acute Catheterisation and Urgent intervention Triage Strategy) trial. The baseline characteristics and outcomes were compared between patients with visible collaterals (Rentrop score 1 – 3) and those without visible collaterals (Rentrop 0) in the vessel with the most severe stenosis.
ResultsThe study cohort comprised 5,412 patients with moderate to high-risk ACS. A total of 858 patients (16%) had visible collaterals, whereas 4,554 patients (84.0%) had no collaterals. The presence of collateral was not associated with any difference in clinical outcome at 1 year after multivariable adjustment major adverse cardiac events (MACE) (hazard ratio (HR), 0.94; 95% confidence interval (CI), 0.76-1.16; p = 0.55), mortality (HR, 1.03; 95% CI, 0.65-1.62; p=0.91), myocardial infarction (MI) (HR, 1.07; 95% CI, 0.83-1.38; p=0.60), and unplanned target vessel revascularisation (TVR) (HR) 0.95; 95% CI, 0.71-1.28; p=0.75). Similar results were observed in an analysis restricted to the subgroup of patients undergoing percutaneous
coronary intervention (adjusted HR for MACE, 1.1; 95% CI 0.76-1.61; p=0.595), mortality (HR, 0.81, 95% CI, 0.10-6.44; p=0.999) and MI (RR, 0.86; 95% CI, 0.54-1.35; p=0.564. The presence of collaterals was associated with an increased risk of unplanned TVR (HR, 2.74; 95% CI, 1.48-5, 10; p=0.004,
ConclusionThe authors concluded that the presence of collateral circulation was not associated with any improvement in outcome of patients with ACS.
PerspectiveThe results of this study are in contrast to prior work demonstrating improved outcomes in the presence of coronary collateral circulation. It is conceivable that the benefit of collateral circulation may be most pronounced in patients with stable coronary artery disease (CAD). It is also possible that presence of collaterals simply reflects the presence of more severe CAD, and thus, the presence of collateral may not overcome the implications of a greater burden of CAD when an ACS develops. Although counterintuitive, this is the largest study on the subject to date, and it would well be that presence of collaterals in patients with ACS may indeed not make a difference in the outcome (other than perhaps permitting retrograde approach to a chronic total occlusion)
Hitinder S. Gurm, MBBS, F.A.C.C Republished here with courtesy from the American College of Cardiology,
www.cardiosource.org/Science-And-Quality/Journal-Scan.aspx
High-Sensitivity Troponin I Concentrations are a Marker of an Advanced Hypertrophic Response and Adverse Outcomes in Patients with Aortic Stenosis
from a cardiovascular cause and 60 patients had an AVR. Plasma cTnl concentrations were associated with AVR or cardiovascular death (hazard ratio, 1.77; 95% confidence interval, 1.22-2.55) independent of age, sex, systolic ejection traction, and aortic stenosis severity.
ConclusionsThe authors concluded that in patients with aortic stenosis, plasma cTnl concentration is associated with advanced hypertrophy and replacement myocardial fibrosis as well as AVR or cardiovascular death.
PerspectiveThe study reports that plasma cTnl concentrations demonstrated a close association with magnitude of LV hypertrophy and the presence of mid-wall myocardial fibrosis in patients with aortic stenosis. Furthermore, high-sensitivity plasma cTnl concentration showed an independent association with long-term risk of AVR or cardiovascular deaths. High-sensitivity troponin assays appear to hold promise as a future clinical tool for patients with aortic stenosis, and large-scale prospective studies are required to investigate the use of CTnl in the management and risk stratification of patients with aortic stenosis to help identify asymptomatic patients who may potentially benefit from early surgery.
Debabrate Mukherjee, M.D., F.A.C.C. Republished here with courtesy from the American College of Cardiology,
www.cardiosource.org/Science-And-Quality/Journal-Scan.aspx
Chin CW, Shah AS, McAlister DA, et alEur Heart J 2014; May 14 (Epub ahead of print)
Study question What are the prognostic implications of plasma cardiac troponin I (cTnl) concentrations in patients with aortic stenosis?
MethodsPlasma cTnl concentrations were measured in two patient cohorts using a high-sensitivity assay. First in the Mechanism Cohort, 122 patients with aortic stenosis (median age 71.67% male, aortic valve area 1.0 ± 0.4cm²) underwent cardiovascular magnetic resonance and echocardiography to assess left ventricular (LV) myocardial mass, function and fibrosis. Kaplan-Meier analysis was performed across tertiles of cTnl concentrations.
ResultsThe indexed LV mass and measures of replacement fibrosis (the gadolinium enhancement) were associated with cTnl concentrations independent of age, sex, coronary artery disease, aortic stenosis severity, and diastolic function. In the separate Outcome Cohort, 131 patients originally recruited into the SALTIRE (Scottish Aortic Stenosis and Lipid Lowering Trial, Impact of Regression) study, had long term follow up for the occurrence of aortic valve replacement (AVR) and cardiovascular deaths. Over a median follow up of 10.6 years (1,178 patient-years), 24 patients died
C
M
Y
CM
MY
CY
CMY
K
CVS iphone A4 June 2014.pdf 1 2014/06/26 2:33 PM





























