Embed Size (px)
Citation preview
ACS Case Presentation
Done By:
Sara AlArfaj, Pharm D, KSU

Patient’s information:
AN, is a 77 yo male
Chief Compliant:
Central chest pain and SOB for 2 days
HPI
• Admitted to ward 2.8 as a case of ACS
“NSTEMI”,DHF, Pulmonary Edema and
Respiratory distress
• ECHO showed
LVSF was severly reduced
EF 30-35%
Severe AS
• Patient was started in IV diuretics
“Furosemide and Metolazone”
• S/P Chest Drain
• On 28/3 started on IV Abx “Tazocin
and Azithromycin”
• Patient desaturated and started on
BiPAP then shifted to CCU-A

PMH
• IHD S/P CABG in 2002
PCI in 2013 at KFSH&RC
• IDDM on insulin, 11 years ago
• CKD
• HTN, 4 years ago
• DLP

Family history:
Not available
Social History:
Not available
Allergies:
None

Vital Signs
Temp = 36.9
SpO2 = 98%
RR = 19
BP = 124/41
HR = 56
Wt = 56.3 kg

Physical Examination
• GEN: Patient was in pain with respiratory
distress
• CNS: GCS 15/15, patient’s alert and
responsive
• CVS: S1 + S2, no abnormalities
• Chest: Coarse crackles with tachypnea
• ABD: Non-tender with hypoactive BS
• CXR:Pleural effusion
• ECG:NSTEMI
• ECHO: Left ventricle is mildly dilated
LVSF is mod-severely reduced
EF = 30-35%
Low gradient AS “ needs Dobutamine Echo to determine AS severity”
Cath Report at KFSH
• Angiography:LM: distal diffuse 90% stenosis
LAD: totally occluded proximally
LCX: totally occluded at origin
RCA: proximal diffuse 90% stenosis then totally occluded
• Impression: 3VD, patent grafts
• Plan: For medical therapy as no value of
Revascularization
Past Medication History:
Medication Medication
Amlodipine 5 mg PO OD Furosemide 5 mg PO BID
Aspirin 81 mg PO OD Metoprolol 50 mg PO BID
Clopidogrel 75 mg PO OD Omeprazole 20 mg PO OD
Atorvastatin 20 mg PO OD Loperamide 10 mg PO BID
Isosorbide Dinitrate 40 mg BID Docusate Sodium 100 mg PO BID

Laboratory Data
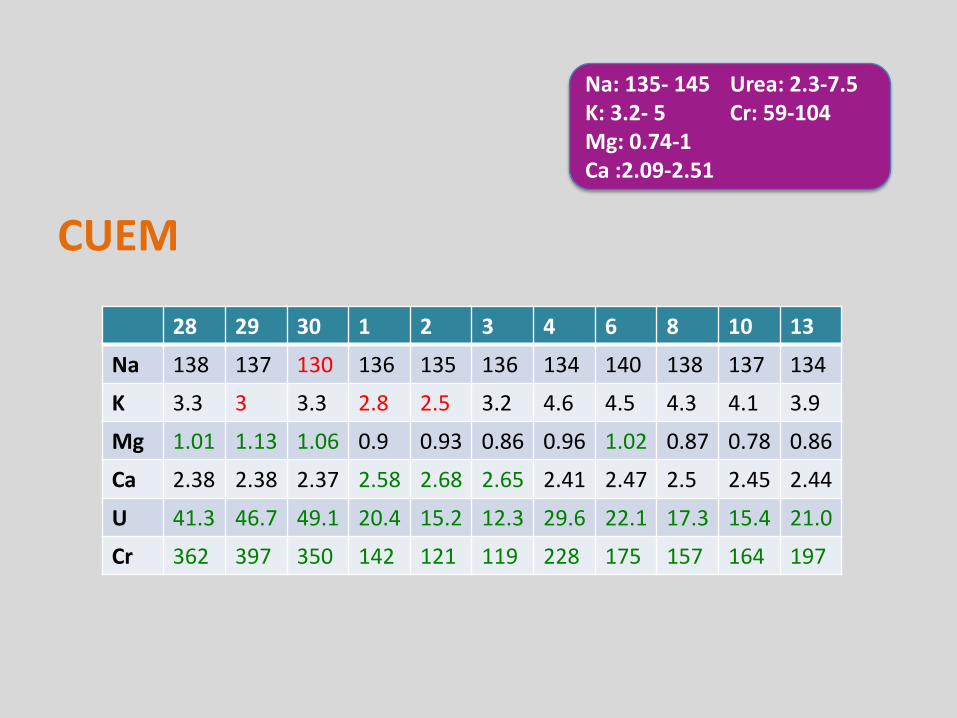
CUEM
28 29 30 1 2 3 4 6 8 10 13
Na 138 137 130 136 135 136 134 140 138 137 134
K 3.3 3 3.3 2.8 2.5 3.2 4.6 4.5 4.3 4.1 3.9
Mg 1.01 1.13 1.06 0.9 0.93 0.86 0.96 1.02 0.87 0.78 0.86
Ca 2.38 2.38 2.37 2.58 2.68 2.65 2.41 2.47 2.5 2.45 2.44
U 41.3 46.7 49.1 20.4 15.2 12.3 29.6 22.1 17.3 15.4 21.0
Cr 362 397 350 142 121 119 228 175 157 164 197
Na: 135- 145K: 3.2- 5Mg: 0.74-1Ca :2.09-2.51
Urea: 2.3-7.5Cr: 59-104
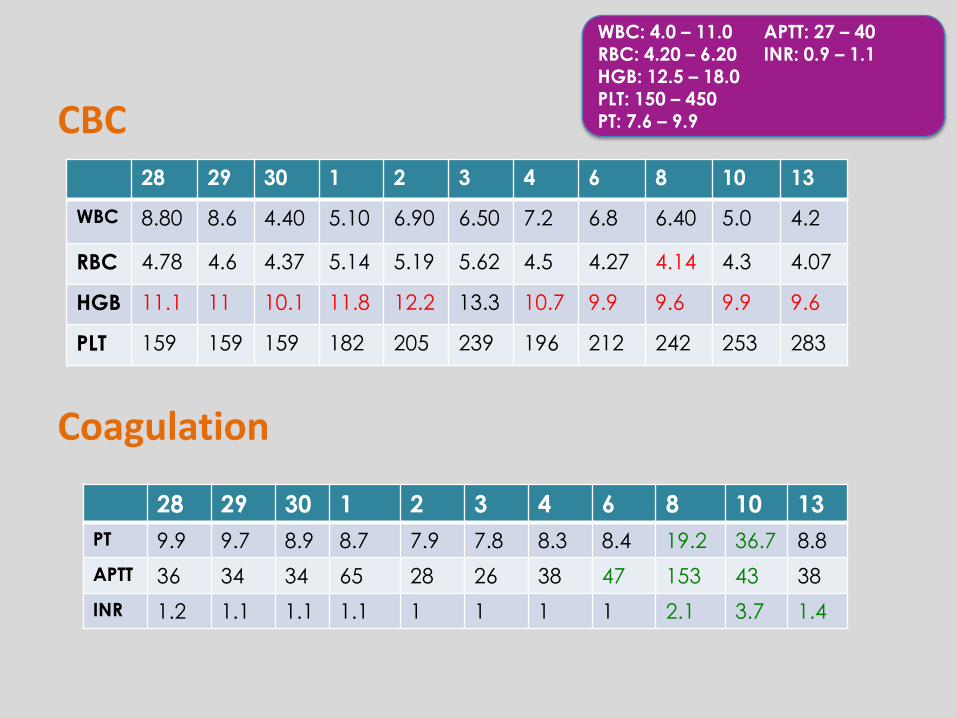
CBC
Coagulation
28 29 30 1 2 3 4 6 8 10 13
WBC 8.80 8.6 4.40 5.10 6.90 6.50 7.2 6.8 6.40 5.0 4.2
RBC 4.78 4.6 4.37 5.14 5.19 5.62 4.5 4.27 4.14 4.3 4.07
HGB 11.1 11 10.1 11.8 12.2 13.3 10.7 9.9 9.6 9.9 9.6
PLT 159 159 159 182 205 239 196 212 242 253 283
28 29 30 1 2 3 4 6 8 10 13
PT 9.9 9.7 8.9 8.7 7.9 7.8 8.3 8.4 19.2 36.7 8.8
APTT 36 34 34 65 28 26 38 47 153 43 38
INR 1.2 1.1 1.1 1.1 1 1 1 1 2.1 3.7 1.4
WBC: 4.0 – 11.0
RBC: 4.20 – 6.20HGB: 12.5 – 18.0PLT: 150 – 450PT: 7.6 – 9.9
APTT: 27 – 40
INR: 0.9 – 1.1
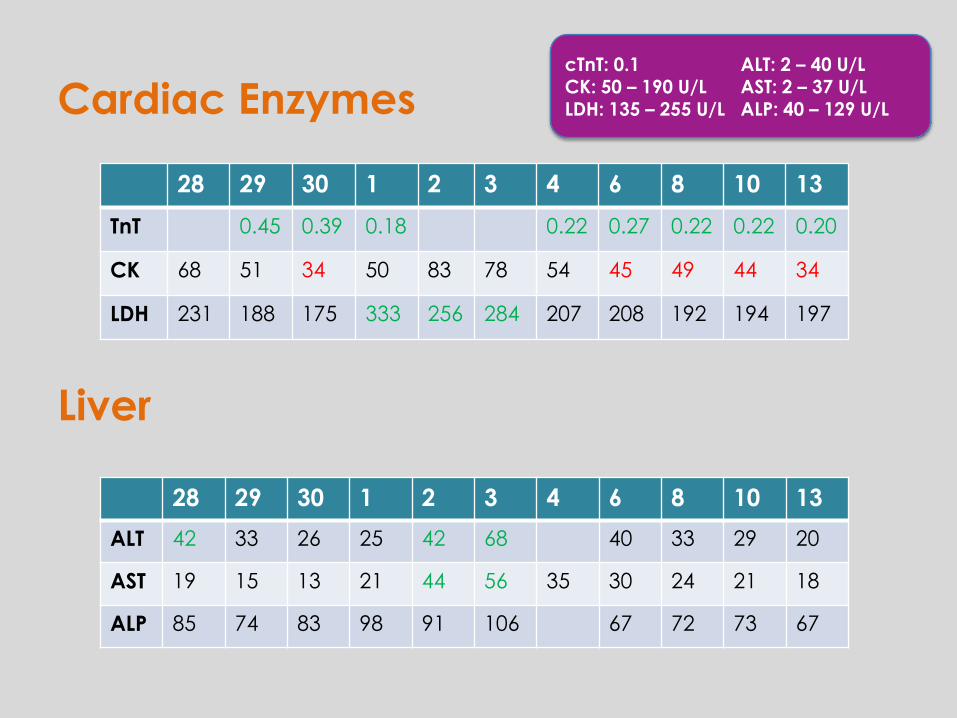
Cardiac Enzymes
Liver
28 29 30 1 2 3 4 6 8 10 13
TnT 0.45 0.39 0.18 0.22 0.27 0.22 0.22 0.20
CK 68 51 34 50 83 78 54 45 49 44 34
LDH 231 188 175 333 256 284 207 208 192 194 197
28 29 30 1 2 3 4 6 8 10 13
ALT 42 33 26 25 42 68 40 33 29 20
AST 19 15 13 21 44 56 35 30 24 21 18
ALP 85 74 83 98 91 106 67 72 73 67
cTnT: 0.1CK: 50 – 190 U/LLDH: 135 – 255 U/L
ALT: 2 – 40 U/LAST: 2 – 37 U/LALP: 40 – 129 U/L

Medication status Medication status
Aspirin 81 mg PO OD Ivabradine 7.5 mg PO Q12 hrs DC’ed1/4(low HR)
Clopidogrel 75 mg PO OD Pregabaline Capsule 75 mg PO
OD
Atorvastatin 40 mg PO OD Trimetazidine 35 mg PO Q 12 hrs
Bisoprolol 2.5 mg PO OD Azithromycin 500 mg PO OD DC’ed 4/4(7 days completed)Calci Heparin 5000 units SC Q12 hrs Tazocin 2.25 g PO Q 12 hrs
Furosemide 40 mg IV Q 12 hrs Renal function
Hydralazine 25 mg PO BD
Esmoprazole 40 mg PO OD Isosorbide Dintirate 20 mg BD
Calcium Carbonate 600 mg PO Q24 hrs
Mixt. Insulin •16 U SC predinner•20 U SC breakfast
One Alpha 0.25 mcg PO OD
Scheduled Medications:

Medications
Dopamine 3
mcg/kg/hr
DC’ed 2/4
Heparin Infusion
(protocol)
Started 5/4
Medications
Acetaminophen 1000 mg PO
Lactulose 20 ml PO
Mg Gluconate 1000 mg PO
KCL 24 mEq PO
Regular Insulin sliding scale
Continuous Infusion:
PRN:
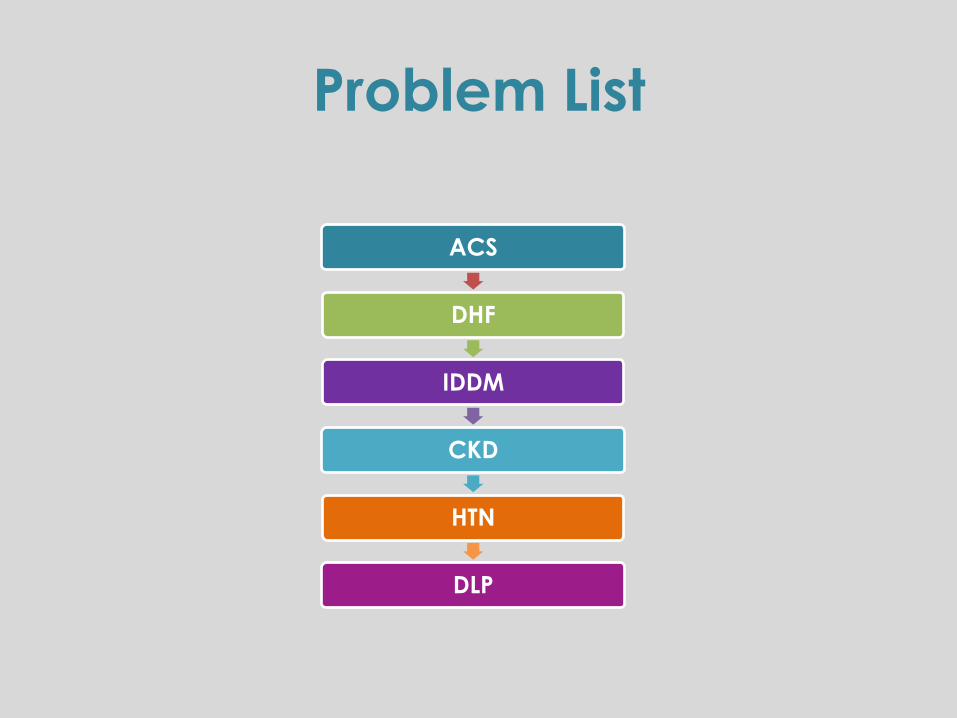
Problem List
ACS
DHF
IDDM
CKD
HTN
DLP
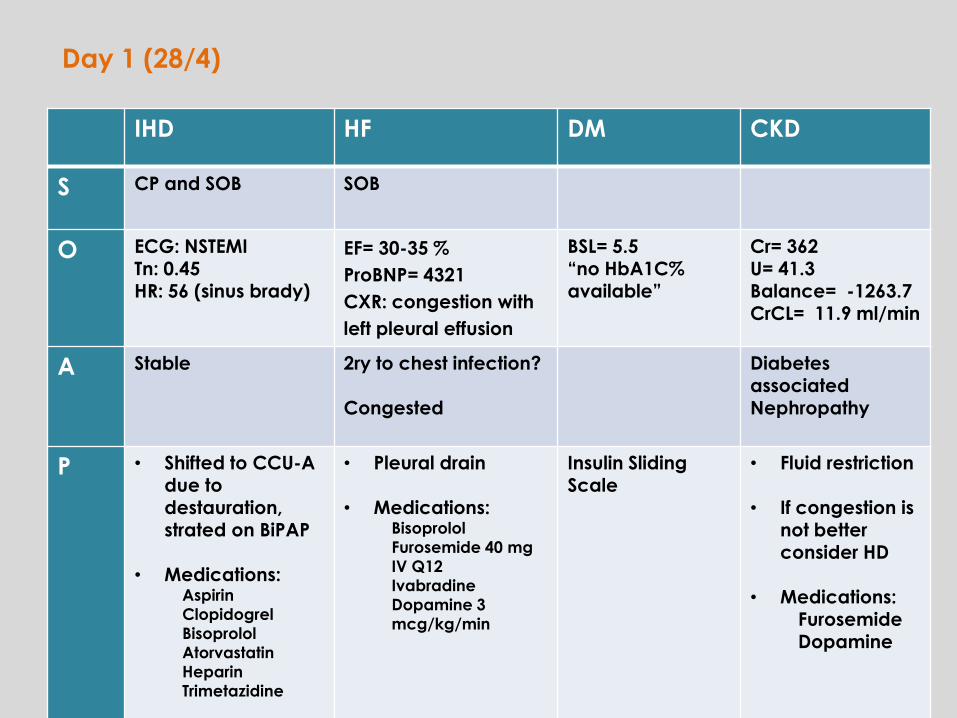
IHD HF DM CKD
S CP and SOB SOB
O ECG: NSTEMITn: 0.45HR: 56 (sinus brady)
EF= 30-35 %
ProBNP= 4321
CXR: congestion with
left pleural effusion
BSL= 5.5“no HbA1C%available”
Cr= 362U= 41.3Balance= -1263.7CrCL= 11.9 ml/min
A Stable 2ry to chest infection?
Congested
Diabetes associated
Nephropathy
P • Shifted to CCU-A
due to destauration, strated on BiPAP
• Medications:Aspirin
Clopidogrel
Bisoprolol
Atorvastatin
Heparin
Trimetazidine
• Pleural drain
• Medications:Bisoprolol
Furosemide 40 mg
IV Q12
Ivabradine
Dopamine 3
mcg/kg/min
Insulin Sliding
Scale
• Fluid restriction
• If congestion is not better consider HD
• Medications:Furosemide
Dopamine
Day 1 (28/4)

HTN DLP
O BP= 142/41 No lipids profile for this patient
A BP is controlled
P Continue same
management
Atorvastatin 40 mg OD
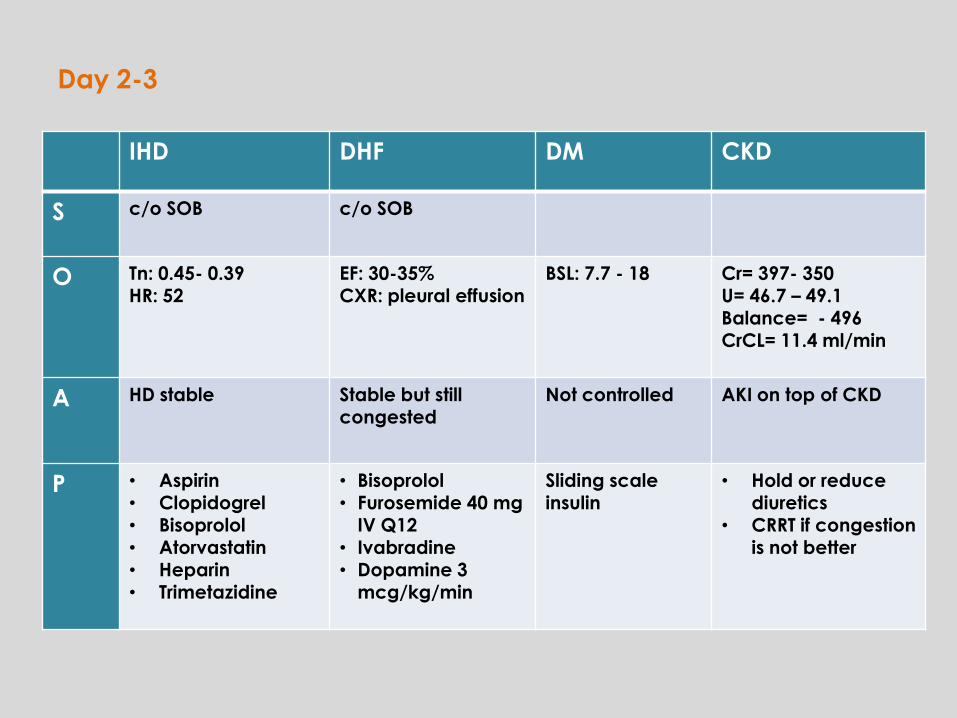
IHD DHF DM CKD
S c/o SOB c/o SOB
O Tn: 0.45- 0.39HR: 52
EF: 30-35%CXR: pleural effusion
BSL: 7.7 - 18 Cr= 397- 350 U= 46.7 – 49.1Balance= - 496CrCL= 11.4 ml/min
A HD stable Stable but still congested
Not controlled AKI on top of CKD
P • Aspirin• Clopidogrel• Bisoprolol• Atorvastatin• Heparin• Trimetazidine
• Bisoprolol• Furosemide 40 mg
IV Q12 • Ivabradine• Dopamine 3
mcg/kg/min
Sliding scale insulin
• Hold or reduce diuretics
• CRRT if congestion is not better
Day 2-3
IHD DHF DM CKD
O Tn= 0.45 – 0.18
HR= 68
EF= 30-35% BSL= 11.2 Cr= 142
U= 20.4
Balance= -524
CrCL= 30.3 ml/min
A No active compliant
P • Hold Ivabraidine
• Hold Bisoprolol if HR<50
Insulin sliding
scale
• DC Lasix
• Started HD for 3
consecutive
sessions
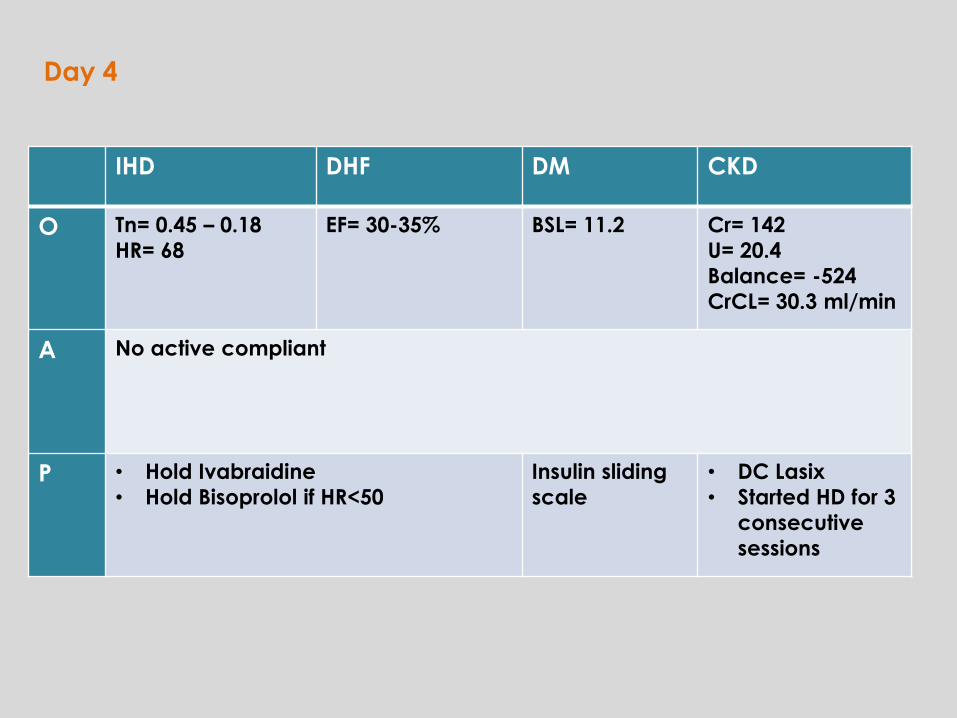
Day 4
IHD DHF DM CKD
O Tn= 0.45-0.22
HR= 77
EF= 30-35%
HR= 77
BP= 123/54
BSL= 14.4-9.4 Cr= 121-119
U=15.2- 12.3
Balance= -1973
CrCl=35 ml/min
A No active compliant Not controlled stable
P Same
management
• Hydralazine 25
mg PO BD
• Isosorbide
Dinitrate 20 mg
PO OD
Mixt. insulin
added with
sliding scale
• Finished 3
sessions of
dialysis
• Dopamine
DC’ed
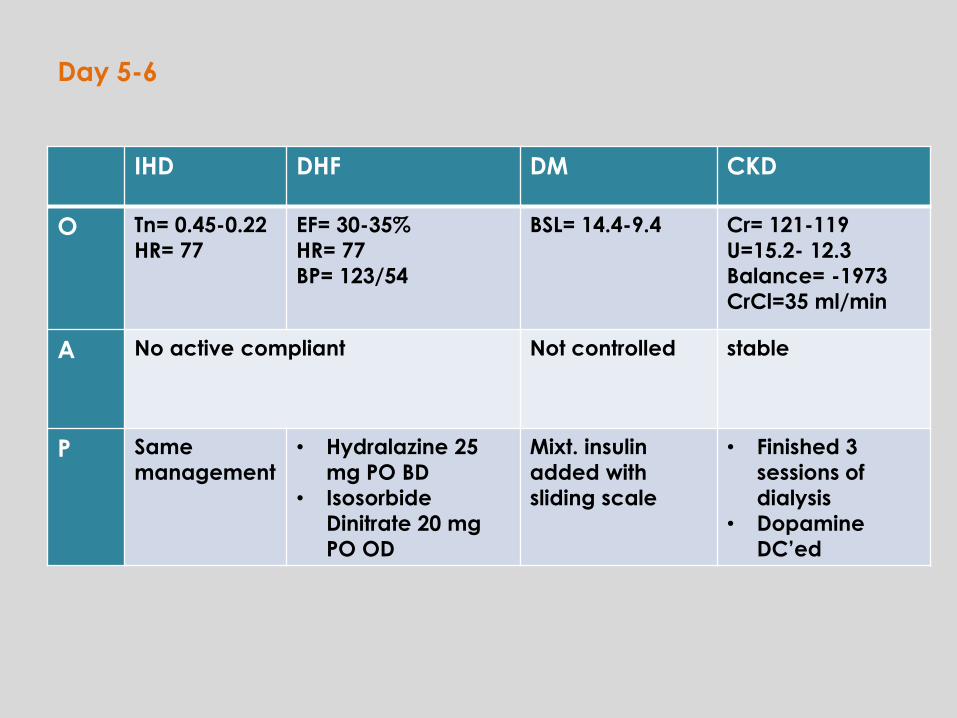
Day 5-6
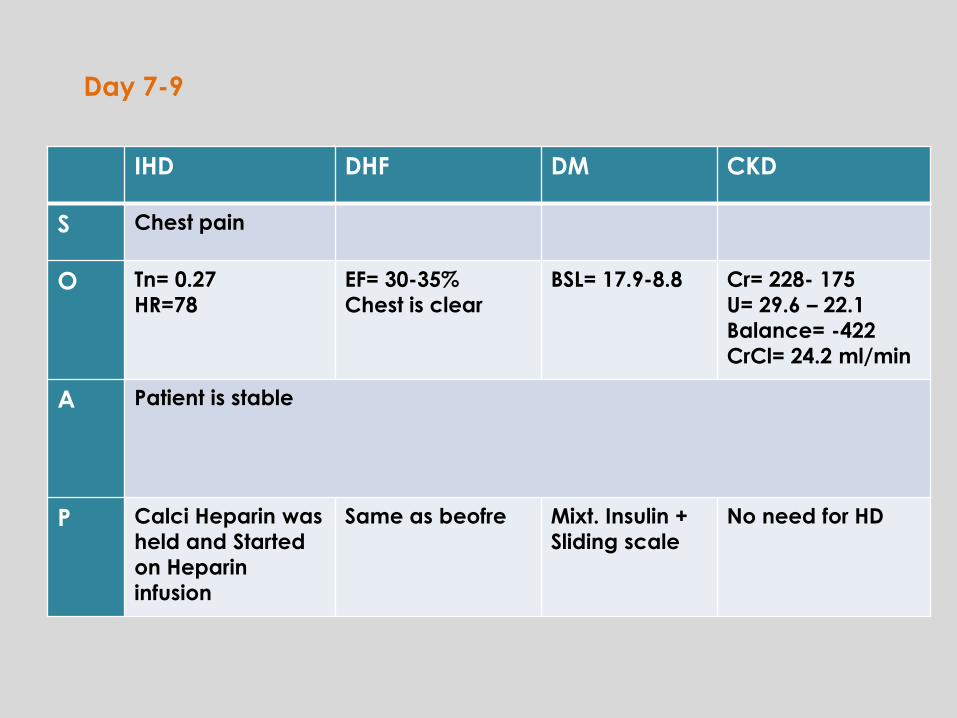
IHD DHF DM CKD
S Chest pain
O Tn= 0.27
HR=78
EF= 30-35%
Chest is clear
BSL= 17.9-8.8 Cr= 228- 175
U= 29.6 – 22.1
Balance= -422
CrCl= 24.2 ml/min
A Patient is stable
P Calci Heparin was
held and Started
on Heparin
infusion
Same as beofre Mixt. Insulin +
Sliding scale
No need for HD
Day 7-9
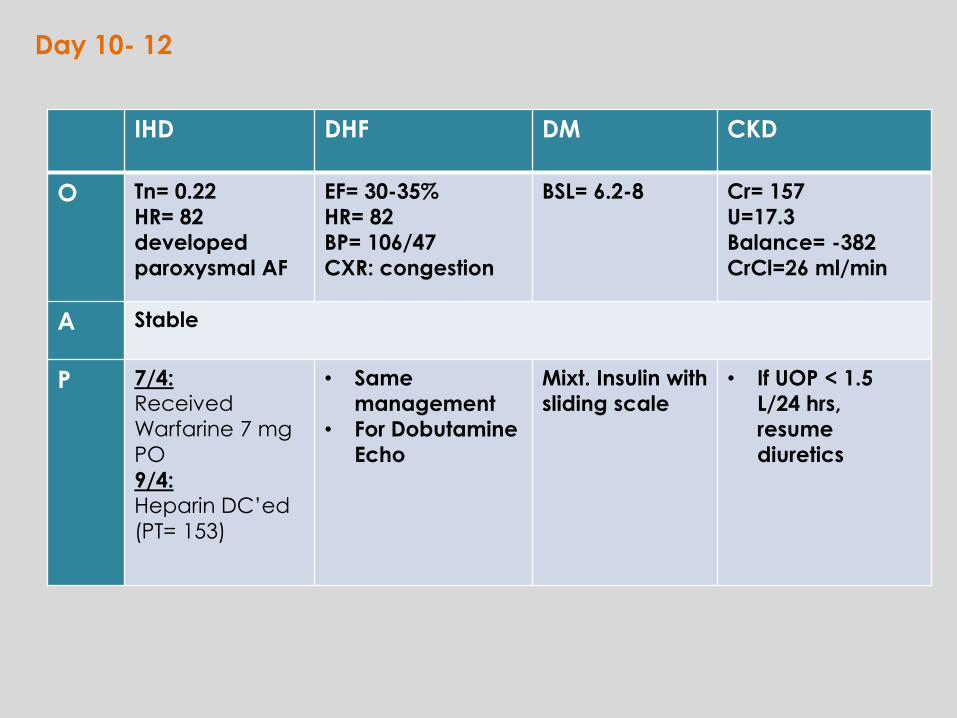
IHD DHF DM CKD
O Tn= 0.22
HR= 82
developed
paroxysmal AF
EF= 30-35%
HR= 82
BP= 106/47
CXR: congestion
BSL= 6.2-8 Cr= 157
U=17.3
Balance= -382
CrCl=26 ml/min
A Stable
P 7/4: Received
Warfarine 7 mg
PO
9/4: Heparin DC’ed
(PT= 153)
• Same
management
• For Dobutamine
Echo
Mixt. Insulin with
sliding scale
• If UOP < 1.5
L/24 hrs,
resume
diuretics
Day 10- 12
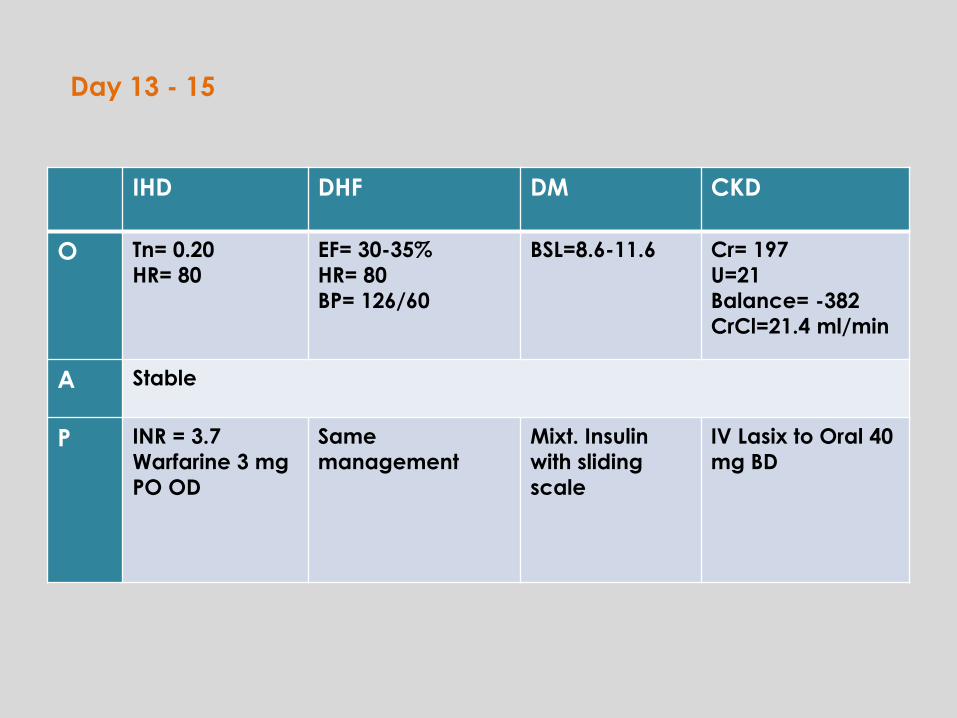
IHD DHF DM CKD
O Tn= 0.20
HR= 80
EF= 30-35%
HR= 80
BP= 126/60
BSL=8.6-11.6 Cr= 197
U=21
Balance= -382
CrCl=21.4 ml/min
A Stable
P INR = 3.7
Warfarine 3 mg
PO OD
Same
management
Mixt. Insulin
with sliding
scale
IV Lasix to Oral 40
mg BD
Day 13 - 15
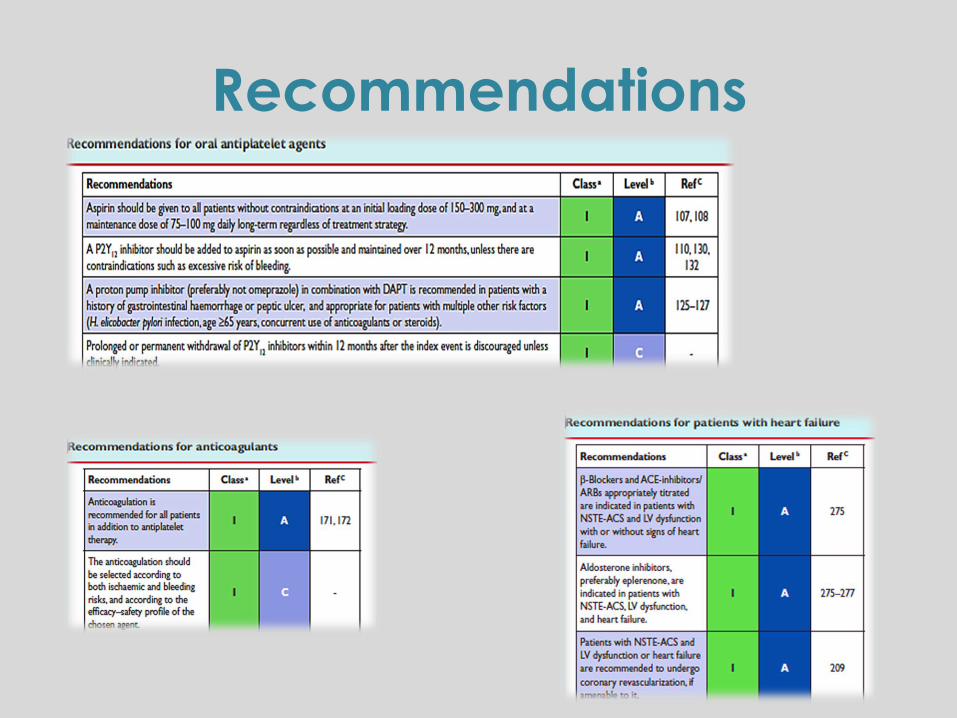
Recommendations
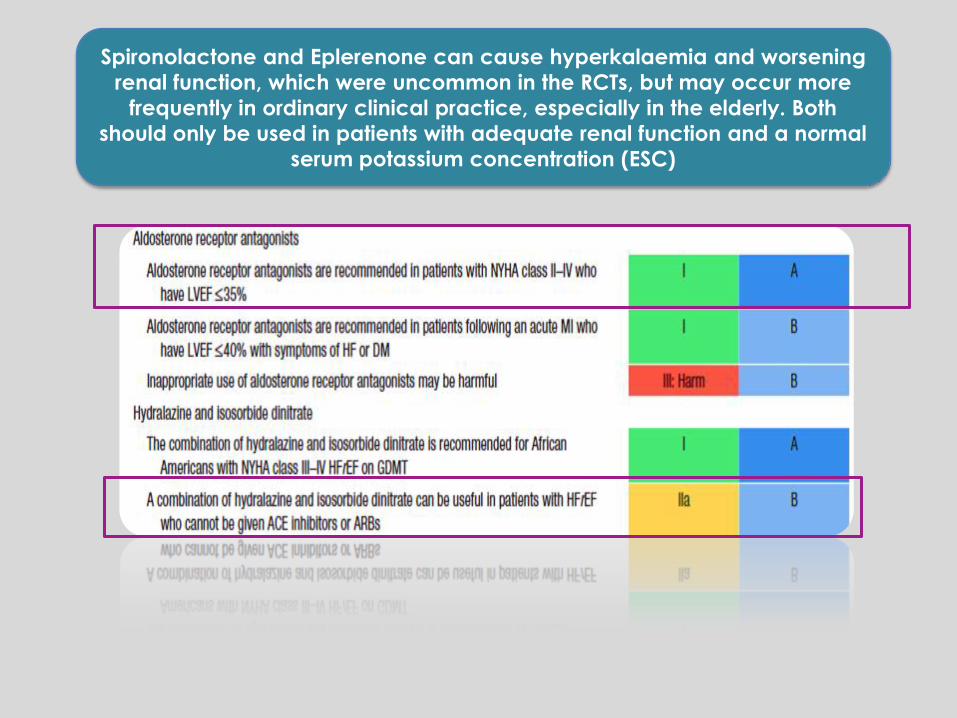
Spironolactone and Eplerenone can cause hyperkalaemia and worsening
renal function, which were uncommon in the RCTs, but may occur more
frequently in ordinary clinical practice, especially in the elderly. Both
should only be used in patients with adequate renal function and a normal
serum potassium concentration (ESC)
Thank You..
Questions?