Embed Size (px)
Citation preview

Cardiac Valves
Sylvia Dennis
Fellow Pathology/Anatomy
NYCOM
Friday, October 07, 2005
1

Objectives
Concepts
To understand Cardiac Valve Gross & Micro Anatomy
Review of normal valve function
To learn the Pathophysiology of Stenosis and Regurgitation
Heart Murmurs/Physical exam findings
Cases
2

Concepts
StenosisStenosis: Failure of the valve to open & forward flow is impeded
InsufficiencyInsufficiency (incompetence, regurgitation): Failure of the valve to close & reverse flow of blood
Damaged valves:Damaged valves: Nidus for infection & thrombosis
Dilated cardiac chambersDilated cardiac chambers: stasis of blood, conduction defects
Normal blood flow is laminar --- turbulence causes murmurs
Rate of dysfunctional development determines symptoms and severityChronic vs Acute
3

Murmur Rules
Intra-thoracic Pressure & PreloadIntra-thoracic Pressure & Preload
Right sided Murmurs with InhalationLeft sided Murmurs with ExhalationStanding/Valsalva: all Murmurs except HCM and MVPSquatting: all Murmurs except HCM and MVP
4

Cardiac Valves
Four valvesTricuspid & Mitral (between atria and ventricles) Aortic & Pulmonic (semilunar)
• Derived from truncus arteriosus
Maintain unidirectional flowFibrous skeleton supports valves
Four fibrous rings (annuli fibrosi) – each encircling a valve , two trigonesElectrical insulator (R trigone provides passage of AV bundle)Provides attachments for the leaflets and cusps
5

Cardiac Valves
Semilunar ValvesSemilunar ValvesPulmonic valve on the right
Aortic valve on the left
Closure produces S2 (A2/P2)
Open in systole
Function depends on integrity of fibrous annulusDilatation of aortic root distorts annulus
Competency depends on ability to stretch/moldCusp/leaflet surface area increases up to 50% during diastole
Overlap of cusps at the lunula
Nodules of Arantii facilitate closure
6

AV valve AnatomyFeatures:Features:Cordae TendineaePapillary musclesBicuspid Mitral valve (L)
with 2 cuspsTricuspid valve ® with 3
cuspsFibrous annuli anchoring
the cusps
7

Clinical Evaluation of Valvular Anatomy
DopplerDoppler
EchocardiographyEchocardiographyEvaluation of LV function
Detection of abnormal wall motion
Measurement of LV volume, EJF and CO
EchocardiogramEchocardiogramTrans-Thoracic
Noninvasive 2 DSuperior spacial resolution
Trans – EsophagealTransducer placed in the esophagus Excellent evaluation of posterior cardiac chambers and aorta2D
8

Valve - Histology
Lined with endothelium (simple squamous epithelium)
Three major layers Ventricularis: rich in elastin – contracts during systole
Spongiosa: loose CT – shock absorber
Fibrosa: dense collagenous CT – provides strength, continuous with supporting structures
9

Cardiac Cycle
Cardiac Cycle & Heart Cardiac Cycle & Heart SoundsSounds
S1 (closure of AV valves) at the same time as QRS
Systole between S1& S2
S2 (closure of Semilunar valves) just after T wave
Diastole between S2 & S1
S3 & S4 are diastolic sounds
10

Cardiac Physiology
Review on your own!
Jugular Venous PulseJugular Venous Pulse
11

Classification of Murmurs
Systolic Systolic Stenosis of Semilunar valves (systolic ejection Murmur)
Regurgitation of AV-valves
MVP (click/murmur)
VSD (children) • Left to Right• Right to Left with
Eisenmenger Syndrome
DiastolicDiastolicStenosis of AV-ValvesRegurgitation of Semilunar valves
• S3 early diastole• S4 late diastole
12

Murmurs
Sounds due to turbulent blood flowSystolic vs DiastolicFeatures
• Radiation • Maneuvers (Inhalation/Exhalation, valsalva & squatting, positioning)
Mechanisms• Structural valve disease• Anemia • Innocent (children)
Types• Continuous (venous hum, PDA)• Stenosis vs Regurgitation
13
Auscultation
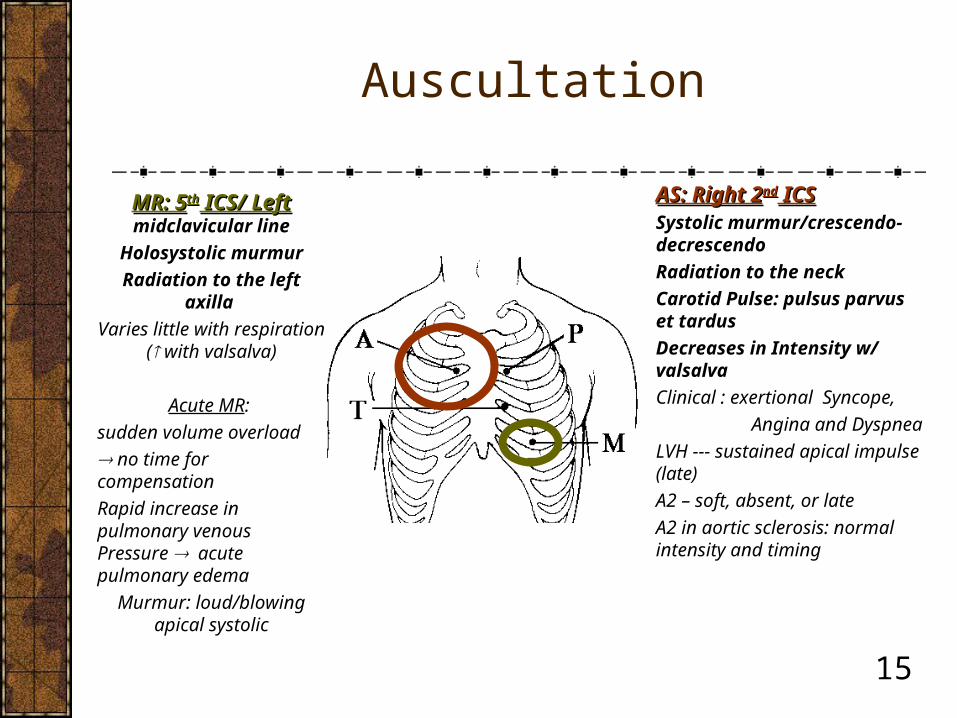
AS: Right 2AS: Right 2ndnd ICS ICSSystolic murmur/crescendo-decrescendo
Radiation to the neck
Carotid Pulse: pulsus parvus et tardus
Decreases in Intensity w/ valsalva
Clinical : exertional Syncope,
Angina and Dyspnea
LVH --- sustained apical impulse (late)
A2 – soft, absent, or late
A2 in aortic sclerosis: normal intensity and timing
MR: 5MR: 5thth ICS/ Left ICS/ Left midclavicular line
Holosystolic murmur
Radiation to the left axilla
Varies little with respiration ( with valsalva)
Acute MR:
sudden volume overload
no time for compensation
Rapid increase in pulmonary venous Pressure acute pulmonary edema
Murmur: loud/blowing apical systolic
15

Regurgitation vs. Stenosis
Acute vs. ChronicLeaky valve/ backflow of bloodCompensatory Mechanism: eccentric hypertrophy
Intrinsic valvular pathologyPost-inflammatory scarringEndocarditisMyxomatous changes (MVP)
Functional regurgitationVentricular Dilation Aortic/Pulmonic Root dilation
Chronic process
Stiff valve/increase in afterload
Compensatory mechanism: concentric hypertrophy
MCC - primary valve pathology
Calcific stenosis *Dystrophic calcification
Congenital
Post-inflammatory scarring
16

HypertrophyEccentric Concentric
Volume overload
Increase in myocardial cell length and cross sectional area
Dilation with increased ventricular diameter
Dilation of ventricle leads to stretching of papillary muscles
Pressure overload Sarcomere deposition parallel to long axis of cell Increased wall thickness (increase in wall stress)
Increase in metabolic requirements
Structural/molecular alterations (decreased capillary to myocyte ratio
Adaptive changes
17

Dystrophic Calcification
Normal serum Calcium & Metabolism
Micro: fine white granule/clumps with gritty consistency
Pathogenesis: injury or microtrauma leading to early inflammatory lesion resulting in final deposition of calcium phosphate crystals
18

Case 1
A 26-year old women with no significant past medical history, presents with a history of chest palpitations particularly when anxious. Physical exam reveals a mid-systolic ejection click followed by a mid-systolic ejection click followed by a murmurmurmur. The click murmur moves closer to S1 when the patient is standing and closer to S2 when lying down. The murmur is heard loudest at the apex.
Diagnosis: MVP
Mechanism of valvular disorder: myxomatous degeneration
Which compound in the extracellular matrix would be increased? Dermatan Sulfate
Explain why the murmur varies with position of the patient: standing decreases
Venous return --- decreased Left ventricular volume – systole occurs faster
19

Case 2
A 60-year-old man is evaluated for a heart murmur. He jogs 3 miles per day and is asymptomatic. Physical examination reveals a delayed carotid upstroke, a 3/6 late-peaking systolic ejection murmur that radiates to the neck, and a single S2.
An echocardiogram shows normal systolic
function and a heavily calcified aortic valve.
Diagnosis: AS
Features that identify the murmur?
Possible etiologies for this patients AS?
Which symptoms can be anticipated with progressive stenosis?
20

Case 3
59 year old man is brought to the ED for syncopal episodesyncopal episode while running in the park. He reports no similar preceding events. He denies shortness of breath and dyspnea. He has a childhood history of pharyngitis x3pharyngitis x3. BP is 110/90 mmHg. He has a late and weak carotid upstrokelate and weak carotid upstroke. On cardiac exam there is a midsystolic murmurmidsystolic murmur 3/6, the apical impulse is sustained and and displaced laterally and the murmur is found to radiate to the neck.radiate to the neck. An S4 heart sound is audible. Lungs are clear. There is no lower extremity edema.
Diagnosis: Aortic StenosisDiagnosis: Aortic StenosisFeatures of the Murmur of ASMost likely etiology of AS in this case ?
21

Aortic stenosis
EtiologyEtiologycongenital
senile calcific AS
rheumatic AS
PathologyPathologyPartially fused leaflets
fibrosis and calcification
Leaflets are less flexible, calcium deposits at valve base
leaflet tips relatively normal
Fibrosis and calcification of valve leaflets, associated with AR
Most common valvular pathology
22

Case 4
A 45 year old women who recently immigrated from Mexico complaints of exertional dyspnea, fatigue, palpitations and edema. She mentions coughing up pink, frothy looking sputum several times over the past weeks. Further questioning reveals some difficulty swallowing solids as well as hoarseness. Her past medical history is significant for a several severe throat infection in childhood. She is otherwise healthy. PE reveals a soft mid-diastolic murmur that increases with expiration. There is an accentuated P2. EKG shows
atrial fibrillation. Diagnosis: Mitral Stenosis with Ortner’s Syndrome
What would you see on TEE? Enlarged Left atrium
Explain the accentuated P2: Pulmonary HTN/RVH
23

Mitral Stenosis
LV inflow tract obstruction Diastolic Murmur loudest at the apex/Opening snap Accentuated P2 with Pulmonary Hypertension (PH)RVH secondary to PHDysphagia for solids --- left atrial enlargement
Hoarseness: compression of left recurrent laryngeal nerve Etiology:
MC- chronicchronic rheumatic valvulitis leading to fusion of commissure, and shortened Chordae tendineae
Intermittent or acute LV inflow tract obstruction --- atrial myxoma or
Atrial thrombus can mimic MS
24

Case 5
Your patient is a 55 year old man on his 4th day after an MI involving the RCA. The EKG shows NSR and PE was within normal limits at 7am. At 4 pm the nurse calls you because the patient complains of severe sudden SOB and diaphoresis. On evaluation he has dyspnea and rales are heard at the lung bases. His BP is 80/50 mmHg. Cardiac exam reveals a new holosystolic murmur loudest at the apex.
Diagnosis: Acute MR due to rupture of papillary muscle
Sudden left atrial volume overload
Rales and dyspnea indicate pulmonary edema25

Case 6
A 53-year old man presents complaining of diarrhea and “hot flashes” for 4 days. He also noticed his skin becoming unusually dark after having spend a few days at the beach. His son noted that dad was somewhat forgetful lately and sometimes confused. On physical exam there is hyperpigmentation of sun exposed areas. The patient is having some trouble when ask to inhale deeply. On cardiac exam there is a pansystolic murmur at the apex with radiation to the axilla. The murmur had not been noted on previous exams. The patients urine revealed high levels of serotonin metabolites. After careful examination and appropriate ancillary studies the patient was diagnosed with carcinoid tumor of the ileum/Carcinoid Syndrome.
Knowing that right sided valvular pathology is often associated with
Carcinoid syndrome, how do you explain the findings in the patients
Cardiac exam?26

Case 7
66-year-old man with a medical history notable only for locally treated prostate cancer presented with a two-month history of dyspnea on moderate exertion and repeated episodes of angina with mild effort or at rest. He came to the emergency room with exertional dyspnea that had worsened during the preceding week. There were no features of Marfan's syndrome. The blood pressure was 164/49 mm Hg (with a pulse pressure of 120 mm Hg), the radial pulses were bounding (Corrigan's pulse), and the carotid pulses were prominent. Cardiac examination revealed decreased S1 and increased S2 intensity, with a grade 2/6 systolic murmur and a grade 3/6 diastolic murmur along the left sternal border. Echocardiography showed a dilation of the aortic root, annuloaortic ectasia, severe aortic regurgitation, and mild tricuspid and mitral regurgitation. The left ventricle was enlarged, with an end-diastolic diameter of 90 mm, an end-systolic diameter of 61 mm, and an ejection fraction of 51 percent. NEJM
:Volume 353:e12
September 29, 2005
27

Aortic Regurgitation
Etiology• CHRONIC vs ACUTE
• Intrinsic valve disease vs Aortic pathology
Typical Murmur: early diastolic/decrescendo • Austin flint murmur (apical/diastolic)
• Systolic flow murmur
Volume overload
Wide Pulse Pressure (large SV)
28
Case 8
A 9-year-old child in a developing country is brought to a clinic by his parents because he has trouble keeping up with his classmates on the playground. Physical examination is remarkable for pulmonary rales. Cardiac Echo shows biventricular dilation of the heart. There is a soft holosystolic murmur appreciated at the apex with radiation to the axilla. Furthermore, the murmur increases on inhalation or squatting. EKG showed bilateral atrial enlargement.
Diagnosis: Wet Beriberi secondary to Thiamine (B1) deficiency Diagnosis: Wet Beriberi secondary to Thiamine (B1) deficiency
Name the two valvular dysfunctions and the supporting characteristics
Pathophysiology of valvular dysfunction
Other causes leading to TR 29

Referenceshttp://info.med.yale.edu/intmed/cardio/imaging/contents.htmlhttp://www-medlib.med.utah.edu/WebPath/webpath.htmlhttp://www.med.ucla.edu/wilkes/intro.htmlwww.blaufuss.orgRobbins and Cotran; Pathologic Basis of Disease, 7 th Ed.Ganong, Lingappa, Mc Phee; Pathophysiology of Disease, 4 th Ed.Kochar; Kochar’s Concise Textbook of Medicine, 4 th Ed.Harrison’s Principles of IM, 16th Ed.NEJM, Volume 351;15: 1539-1545, October 7, 2004
Aortic Regurgitation
Circulation 1994;90:844-853Otto CM, Kuusisto J, Reichenbach DD, Gown AM, O'Brien KD. Characterization of the early lesion of `degenerative' valvular aortic stenosis: histological and immunohistochemical studies
NEJM, Volume 352:2389-2397, June 9, 2005 Number 23“A Randomized Trial of Intensive Lipid-Lowering Therapy in Calcific Aortic Stenosis”