Embed Size (px)
Citation preview

Cardiac Pacemakers
Aishwarya Sreenath Naheed Baksh

2
Presentation Outline
History of pacemakerAnatomy of the heartNatural pacemaker Hemodynamics of heart Types of artificial pacingBasics structure, materials and power supply
Types of permanent pacemakerWhen are pacemaker prescribedHemodynamic effects of cardiac pacemakersExample: Stokes Adams SyndromeImplementation and implementation risksFuture

3
History of Artificial Pacemakers
Since the beginning of the eighteenth century, physicians and scientist knew that heart is just a muscle and it can be contracted by electrical simulation.
Re-animation chair, “FRANKENSTEIN”
1932 American physiologist Albert Hyman invented an electro-mechanical instrument, and he named it “artificial pacemaker”

4
First human pacemaker, Made In Canada
1950, Canadian Electrical Engineer John Hopps and surgeon Wilfred Gordon Bigelow designed the first pacemaker to be used on patients in Toronto General Hospital.
John Hopps was the founding president of the Canadian Medical and Biological Engineering Society
A Transcutaneous pacemaker
Painful for the patient
Used the AC wall sockets there was a potential risk of electrocution.

5
PM – 65
Early 1950, Paul ZollBoth electrocardiograph and electrical pulse generator.Pace the heart from external device.Also Transcutaneous Uncomfortable Limitations in movement Acceptable as long as the pacemaker was considered emergency apparatus for post-surgical care

6
First implantable pacemaker
Dr. C. Walton Lillehei encountered a power failure and thus realized that a pacemaker should be a compact device that runs on batteries.
Earl Bakken upon Dr. Lillehei’s request, designed a prototype that ran on batteries.
Engineer Rune Elmqvist and Dr. Ake Senning created the first implantable pacemaker and successfully implanted in a patient on October of 1958.
After that all the developments are based on the implantable pacemaker model.

7
Further Developments
1975 - Lithium-iodine batteries took battery life from months to yearsmid-1970s, pacemaker settings could be programmed using radio-frequency signals.1980’s rate responsive pacing In the late 1990's, pacemakers could mimic the heart's natural rhythm even more closely by adjusting the rhythm according to a person's activity level.

8
Basic heart Structure

9
Blood flow

10
Conduction System
Autorhythmic fibers are specialized cardiac muscle cells that cause an inherent and rhythmical electrical activity in the heartAutorhythmic fibers are self excitable- they simulate contraction without a requisite electrical impulse from the central nervoussystemA single cardiac muscle cell can contact rhythmically at a steady rate without any inputIf two cardiac muscle cells are in contact, the one that contracts first will simulate the other to contractThe contractile activity is regulated by the autonomic nervous systemCardiac muscle cells are connected to each other through intercalated discs which support synchronized contraction of thecardiac tissue

11
Intercalated discs
Intercalated discs conduct electrochemical potentials between the cytoplasms of adjacent cells through gap junctions

12
Cardiac Action Potential Propagation

13
Pathway of AP

14
Hemodynamics of heart
EDV (END DIASTOLIC VOLUME)ESV (END SYSTOLIC VOLUME)Stroke Volume, SV = EDV – ESVGenerally SV = 70 ml/beat HR = heart rate = 75 beats/minCO = HR x SV CO = 5250 ml/min (5.25 L/min)

15
Types of artificial pacing
Percussive PacingTranscutaneous PacingTransvenous PacingPermanent pacing

16
Percussive Pacing
Strike from a distance of 20-30 cm with closed fist on the left lower edge of sternum.
The pressure in the ventricle should rise 10-15 mm hg.

17
Transcutaneous pacing
External methodEmergency optionTwo pads are placed on the patient Starting with low current the pacemaker is set to the optimal currentNot a comfortable procedure

18
Transvenous Pacing
Bridge to permanent pacemaker placement A sterilized wire is placed in a vein and carried to an atrium or ventricle. The wire is attached to an external pacemaker

19
Permanent Pacing
Implanted device similar to transvenous pacemaker Powered by battery that runs for 6-12 years. 2 components
1) Pulse generator 2) Insulated lead(s) and electrodes.

20
What is an artificial pacemaker?
A pacemaker is an electronic device implanted in the body to regulate the heart beat.A Pacemaker is not designed to defibrillate the heart by delivery of shocks. The PM delivers electrical stimuli over leads with electrodes in contact with the heart.

21
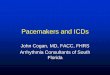
Basic structure of pacemaker
Pulse generator can be both rate responsive or fixed rate Pacing leads are passed through a vein (in this case SVC)Then the electrodes are placed on the myocardium of the desirable locationFigure: Atrioventricular pacemaker

22
Materials used in Pacemaker
Qualities for the materials used in the pacemaker:– Lowest stimulation voltage – Possible long term implementation – Biocompatibility and nontoxicity
Stainless steel electrodes are replaced by cobalt alloys, platinum-iridium alloys. Carbon is also being used to some extent. Stainless steel is still the most cost efficientPulse generator is housed in a titanium container

23
Power supply
Mercury-zinc battery – 48-60 months Lithium Iodide battery – 10+ years Biothermal Batteries (Under progress)

24
Types of permanent pacemakers
Single-Chamber PacemakersDual-Chamber Pacemakers

25
Single Chambered Pacemaker
One wire is placed on the heart chamberEither Atrium or the VentricleFigure: Single chamber ventricular pacemakerGenerally fixed rate$2,500.00 cheaper from dual chambered but similar efficiency in many cases.

26
Dual Chamber Pacemaker
Two leads are placed in two different chambers of heart Generally one lead goes to a ventricle and the other goes into the atrium This approach more closely matches the natural pacing of the heart 40% of the pacemakers used in Canada are dual chamber.

27
Types of pacemaker
Fixed rate pacemakers – set to work at a certain heart rate – If the heart’s own intrinsic rate dropped below a
pre-set number the pacemaker would begin to pace at a preset rate.
Rate responsive pacemaker– Determines what the heart rate should be from
moment to moment

28
Rate Responsive Pacemaker
Technological advancements
The more the patient’s body is moving the faster the heart rate should be.
2 major mode to detect the optimal cardiac output– Activity sensor– Breathing sensor

29
When are pacemakers prescribed?
Bradycardia Fibrilation Heart failureSyncope

30
Quiz
What is Cardiac Output?

31
Hemodynamic effects and issues
Cardiac output decreases with many heart problems.
CO = HR x SV
The low CO is augmented when HR is increased by using the artificial pacemaker.
CO increases with the increment of rate until a maximum level of CO is reached.
Optimal rate = maximum cardiac output
This maximum level is very close to the CO in people with no heart trouble.

32
Frank-Starling Law Of The Heart
The greater the heart muscle is stretched during the filling, the greater the quantity of blood pumped.

33
Hemodynamic effects and issues
When CO is maximum, increase in heart rate decreases the stroke volume.
Thus, if artificial pacemaker is applied to a normal heart, no significant change in cardiac output will be observed.

34
Stokes Adams Syndrome example
Heart temporarily loses connection between atria and ventricles.Temporary heart block causing bradycardia. Brain does not get enough oxygen rich blood. Syncope (faint) and seizure

35
Causes
Heart diseases that affect the AV node. Surgical trauma– Repair of a heart defect – Replacement of valves
CardiomyopathiesMyocarditisMedication

36
Diagnosis
Electrocardiogram
Echocardiogram
Biopsy
Cardiac catheterization
Electrophysiological study

37
Treatment
Depending on the cause. Discontinuation of medication Pacemakers are used in severe cases.AV block One electrode is placed on the atrium and the other on the ventricle.

38
Implementation
Pacemaker surgery is done under local anesthesia. A small incision is made where the pacemaker will be located. The leads are guided through a large vein to the heart. The pulse generator is then placed under the skin and then the incision is closed. Approximately 1 hour longRegular monitoring of BP and HR might be needed.The incision spot should not be wet for 10 days. Minor pain and discomfort might occur for 5 – 10 days.

39
Risk of implementation
Implantation of the pacemaker is a safe procedure. Proceduralcomplications are rare. These include but are not limited to:
5% chance of bleeding or severe bruising at the insertion site. 1% chance of lung puncture while obtaining access into the veins.1% chance of puncture of heart muscle. This may require specific treatment1% chance of infectionOther risks may apply, depending upon the patients medical condition

40
Future of Cardiac Pacemakers
Biothermal Batteries – Converts body’s own heat into electricity
Transtelephonic monitoring– Already exists – Improving to a cellphone-like device
In body communication system – ZL70100 ultra low-power transceiver chip – transceiver in a pacemaker can wirelessly send
patient health and device performance data to a bedside base station.
– 500 kb/s data transmission over a typical two-meter range.
– This is already made and should be in the market anytime.

Any Question?
Thank you for your attention

42
References
Harold Siddong and Edgar Sowton, “Cardiac pacemakers”, Charles C Thomas PublisherL.A. Geddes, “Cardiovascular Devices and Their Applications”, Ed. 10, Wiley-IntersciencePublicationDr. Richard Sutton and Dr. Ivan Bourgeois “The foundation of Cardiac Pacing, Pt.1”, FuturaPublishing Company. Vol 1, 1991Heinemann, William, Fontaine. G, Grosgogeat.Y, and Welti. J.V.T. “The Essentials of cardiac pacing”. France: Cedig Publisher, 1976.H.J. Th. Thalen, Jw.van den Burg, J.N Homan can der Heide, and J, Nieveen. “The Artificial Cardiac Pacemaker”. The Netherlands: London Royal VanGorcum Publishers, 1969.Gerrard J. Tortora, Derrickson, Bryan. “Principles of Anatomy and Physiology”. United States of America: John Wiley & Sons, Inc, 2006.http://www.howstuffworks.com/heart.htmhttp://www.nlm.nih.gov/medlineplus/tutorials/pacemakers/htm/index.htmhttp://heartdisease.about.com/cs/arrhythmias/a/pacemakers.htmhttp://www.uvka.de/univerlag/volltexte/2005/77/pdf/Oertel_Modelling_the_human_cardiac_fluid.pdfhttp://www.emedicine.com/emerg/topic699.htmhttp://www.emedicine.com/med/topic189.htmhttp://www.medicinenet.com/pacemaker/article.htmhttp://www.thebakken.org/artifacts/pacemakers.htmhttp://www.sdrs.org/equipment-als.htmhttp://www.cardiocare.co.za/courses.php

43
References (Cont’d)
http://www.chw.org/display/displayFile.asp?filename=/Groups/PediatricHealthInformation/CardiovascularDisorders/pacemk10.jpghttp://fhs.mcmaster.ca/main/news/news_archives/pace.htmhttp://heart.health.ivillage.com/arrhythmia/stokes-adams.cfmhttp://www.londonafcentre.co.uk/images/pacemaker.gifhttp://www.chw.org/display/displayFile.asp?filename=/Groups/PediatricHealthInformation/CardiovascularDisorders/pacemk9.jpghttp://www.cardioassoc.com/patient_pgs/procedures/pacemaker.asphttp://en.wikipedia.org/wiki/Artificial_pacemakerhttp://www.medicineonline.com/reference/Computers/info/Pacemaker.htmhttp://en.wikipedia.org/wiki/Cardiac_pacemakerhttp://en.wikipedia.org/wiki/Cardiac_muscle