Embed Size (px)
Citation preview

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 1/80
Cardiac MeasurementsGuidelines
Powered byMyLab Alpha eHD/Crystaline MyLab Seven eHD/Crystaline MyLab Class C
w: www.mideas.si
m: 00386 40 771 779

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 2/80
The following types of measurements are commonly included in a
comprehensive echocardiography report.
1) Left Ventricle:
a) Size: Dimensions or volumes, at end-systole and end-diastole
b) Wall thickness and/or mass: Ventricular septum and left ventricular posterior wall
thicknesses (at end-systole and end-diastole) and/or mass (at end-diastole)
c) Function: Assessment of systolic function and regional wall motion. Assessment
of diastolic function
2) Left Atrium:
• Size: Area or dimension
3) Aortic Root:
• Dimension
4) Right Ventricle:
a) Size: Dimensionsb) Function: Systolic and diastolic function
c) RV & pulmonary hemodynamics
5) Right Atrium:
a) Size: Dimensions, area
b) RA pressure

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 3/80
The following cardiac and vascular structures are generally be evaluated as
part of a
comprehensive adult transthoracic echocardiography report:
1) Left Ventricle (LV)
2) Left Atrium (LA)
3) Right Atrium (RA)
4) Right Ventricle (RV)5) Aortic Valve (AV)
6) Mitral Valve (MV)
7) Tricuspid Valve (TV)
8) Pulmonic Valve (PV)
9) Pericardium10) Aorta (Ao)
11) Pulmonary Artery (PA)
12) Inferior Vena Cava (IVC) and Pulmonary Veins

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 4/80
6) Valvular Stenosis:
a) Valvular Stenosis: Assessment of severity, including trans-valvular gradient and area.
b) Subvalvular Stenosis: Assessment of severity, Including subvalvular gradient.
7) Valvular Regurgitation: Assessment of severity with semi-quantitative descriptive
statements and/or quantitative measurements
8) Cardiac Shunts: Assessment of severity. Measurements of QP:QS (pulmonary-to
systemic flow ratio) and/or orifice area or diameter of the defect are often helpful.
9) Prosthetic Valves:
a) Transvalvular gradient and effective orifice area
b) Description of regurgitation, if present
The following types of measurements are commonly included in a
comprehensive echocardiography report.

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 5/80
① This icon identifies the level 1 measurements according to ASE’s
standard guidelines
② This icon identifies the level 2 measurements according to ASEstandard Guidelines
Clarification

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 6/80
Left Ventricle (LV)
LV Dimensions, wall thickness, LV mass: 2D Mode
Input:
- IVSd - Interventricular septal tickness at end-
diastole(green)
- LVEDD - LV End-Diastolic dimension (yellow)
- PWd - PW thickness at End-Diastolic (red)
- LVESD – LV End-Systolic dimension (right image)
Output:
- LVEF %
- LVFS (Fractional Shortening )
- LV Mass
- LVMI - LV Mass Index
- RWT - Relative wall thickness
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 7/80
LV Dimensions, wall thickness, LV mass: M-Mode (sax or plax)
Input:- IVSd (yellow)
- LVIDd – LV Internal diameter diastole (EDD)
- LVPWd – LV Posterior wall diastole (green)
- IVSs - Interventricular Septum systole (red)
- LVIDs - LV Internal diameter systole (ESD)
- LVPWs End-systolic diameter(blue)
Output:
- LV EF - (Teichholz formula)
- LV FS - (Fractional Shortening)- LVVd - Diastolic Volume
- LVVs - Systolic Volume
- SV - Stroke Volume
- SI - Stroke index
- Sept Thickening %
- PW Thickening %
- LV Mass- LVMI - LV Mass Index
Left Ventricle (LV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 8/80
The most commonly used 2D methods formeasuring LV mass are based on the area-
length formula and the truncated ellipsoid
model, as described in detail in the 1989 ASE
document on LV quantitation. Both methods
rely on measurements of myocardial area at
the midpapillary muscle level. The epicardiumis traced to obtain the total area (A1) and the
endocardium is traced to obtain the cavity
area (A2). Myocardial area (Am) is
computed as the difference: Am = A1 - A2.
Left Ventricle (LV)LV Mass: 2D Mode (A-L and Truncated ellipsoid method)
Input:
A1 – Area1 Pericardial border
A2 – Area 2 Endocardial border
A-L : LV length
Output:
LV Mass
LVMI – LV Mass index
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 9/80
LV Volumes & systolic function: Simpson method
The most commonly used 2D measurementfor volume measurements is the biplane
method of disks (modified Simpson’s rule) and
is the currently recommended method of
choice by consensus of the proper ASE
committee. The total LV volume is calculated
from the summation of a stack of ellipticaldisks. The height of each disk is calculated as a
fraction (usually 1/20) of the LV long axis
based on the longer of the two lengths from
the 2- and 4- chambers view. Papillary muscles
should be excluded from the cavity in the
tracing.
Input:
LV EDD – LV End-diastolic dimension (A4C)
LV ESD – LV End-systolic dimension (A4C)
LV EDD – LV End-diastolic dimension (A2C)
LV ESD – LV End-systolic dimension (A2C)
Output:
EDV – End-diastolic volume (mL)
ESV - End-systolic volume (mL)
LVDVI – LV Diastolic volume index (mL/m²)
LVSVI – LV Systolic volume index (mL/m²)
LVEF – LV Ejection fraction %
SV – Stroke Volume (mL)SI - Stroke Index
Left Ventricle (LV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 10/80
LV Volumes & systolic function (A-L)
As an alternative method to calculate the
LV Vol when apical endocardial definition
precludes accurate tracing is the area-
length where the LV is assumed to be
Bullet-shaped. The mid-LV cross-sectional
area is computed by planimetry in the
parasternal short-axis view and the
length of the ventricle taken from the
midpoint of the annulus to the apex in
A4C view. This measurements are
repeated in end-diastole and end-systole.
The most widely used parameter for
indexing volumes is the Body Surface
Area (BSA) in square meters.
Input:
LV diastolic CSA – Cross sectional area
LV diastolic length – A4C
LV systolic CSA
LV systolic length – A4C
Left Ventricle (LV) ②
Output:
EDV – End-diastolic volume (mL)
ESV - End-systolic volume (mL)
LVDVI – LV Diastolic volume index (mL/m²)
LVSVI – LV Systolic volume index (mL/m²)
LVEF – LV Ejection fraction %
SV – Stroke Volume (mL)SI - Stroke Index
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 11/80
LV Systolic function: Stroke Volume (SV), Cardiac output (CO)
CO (LV) is the volume of blood being pumped by theleft ventricle in the time interval of one minute.
In order to obtain CO we need to measure the LVOT
diameter in PLAX view zoomed image (left) in systole
and the Velocity Time Integral in Pulsed wave mode
of the LVOT in apical 5 chamber view (left down).
Formula:
SV = π x (LVOT / 2)² x VTI₁
CO= (SV x HR) / 1000
Input:
LVOT – LV outflow tract diameter (mm)LVOT VTI - Subvalvular Velocity Time integral (cm)
R-R interval (HR) (Red doted line)
Output:
SV - Stroke Volume
CO - Cardiac output
SI – Stroke IndexCI - Cardiac Index
Left Ventricle (LV) ①
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 12/80
LV Systolic function: MPI LV (Myocardial Performance Index)
Also known as the Tei index. It is an index
that incorporates both systolic anddiastolic time intervals in expressing
global systolic and diastolic ventricular
function. Systolic dysfunction prolongs
prejection (isovolumic contraction time,
IVCT) and a shortening of the ejection
time (ET). Both systolic and diastolicdysfunction result in abnormality in
myocardial relaxation which prolongs the
relaxation period (isovolumic relaxation
time, IVRT).
Input:
MCOT - Mitral valve closure to opening time (orange)
LVET - LV Ejection time (blue lines)
Output:
LV MPI – LV Myocardial performance index
Formula:
LV MPI= (IVCT + IVRT) / LVET = (MCOT – LVET) / LVET
Left Ventricle (LV) ①
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 13/80
LV Systolic function: dP/dt (LV Contractility)
Peak dP/dt is one of the most commonly usedindexes for assessing left ventricular function.
Continuous wave Doppler determination of the
velocities of a mitral insufficiency jet should
allow calculation of instantaneous pressure
gradients between the left ventricle and left
atrium. The rising segment of the mitralinsufficiency velocity curve should reflect left
ventricular pressure elevation. The LV
contractility dP/dt can be estimated by using
time interval between 1 and 3 cm/sec on MR
velocity CW spectrum during isovolumetric
contraction, i.e. before aortic valve opens whenthere is no significant change in LA pressure.
Formula:
dP/dt= 32/T
Input:
T - Time between 1 and 3 cm/sec
Output:
dP/dt (mmHg/s)
Left Ventricle (LV) ①
②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 14/80
Systolic myocardial velocity (S’) at
the lateral mitral annulus is a measure
of longitudinal systolic function and iscorrelated with measurements of LV
ejection fraction and peak dP/dt . A
reduction in S’ (Systolic velocity annulus)
velocity can be detected within 15
seconds of the onset of ischemia, and
regional reductions in S’ are correlatedwith regional wallmotion abnormalities.
Incorporation of TDI measures of
systolic function in exercise testing to
assess for ischemia, viability, and
contractile reserve has been suggested
because peak S’ velocity normally
increases with dobutamine infusion and
exercise and decreases with ischemia. *
* A Clinician's Guide to Tissue Doppler Imaging Carolyn Y. Ho and Scott D. Solomon Circulation. 2006;113:e396-e398
LV Systolic function: TDI
Input:
S – Systolic velocity in lateral wall A4C (red)
Left Ventricle (LV) ②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 15/80
LV Wall motion score
Left Ventricle (LV)

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 16/80
LV Diastolic function
- PW mitral inflowIVRT (Isovolumic relaxation time)
- DTI (e′) (Tissue doppler)
- PV (Pulmonary vein) flow- Mitral inflow propagation
- LA volume
- PCWP by E/e’ (mean PulmonaryCapillary Wedge Pressure by E/e’) (Nagueh)
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 17/80
Left Ventricle (LV)
Input:
- E-wave - Peak early filling velocity (Yellow)
- A-wave - Late diastolic filling velocity (green)
- DT - Deceleration time (Blue)
- IVRT – Isovolumic relaxation time (red)
- A duration – (orange)
LV diastolic function: PW mitral inflow
The mitral inflow velocity profile is used to
initially characterize LV filling dynamics. The E
velocity (E) represents the early mitral inflow
velocity and is influenced by the relative
pressures between the LA and LV, which, in turn,
are dependent on multiple variables including LA
pressure, LV compliance, and the rate of LV
relaxation. The A velocity (A) represents theatrial contractile component of mitral filling and
is primarily influenced by LV compliance and LA
contractility. The deceleration time (DT) of the E
velocity is the interval from peak E to a point of
intersection of the deceleration of flow with the
baseline and it correlates with time of pressureequalization between the LA and LV.
①
Output:
- E/A ratio
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 18/80
The IVRT is the time interval between aortic
valve closure and mitral valve opening. The
transducer is placed in the apical position
with either a pulsed or continuous wave
Doppler sample placed between the aorticand mitral valves. A normal IVRT is
approximately 70 to 90 ms. The IVRT will
lengthen with impaired LV relaxation and
shorten when LV compliance is decreased
and LV filling pressures are increased.
IVRT - measurement from the Ao valve closure (yellow)
And Mitral valve opening (green)
LV diastolic function: IVRT (Isovolumic relaxation time)
Left Ventricle (LV) ①
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 19/80
Currently, the most sensitive and widely
used technique for LVDF is TDI.Diastolic dysfunction is directly related to the
reduction in early LV relaxation
compromising the effective transfer of the
blood from the atrial reservoir into the LV
cavity. The reduction in LV relaxation may be
characterized through the evaluation ofmitral annular motion, generally with
Doppler tissue imaging, which can resolve
subtle changes in LV relaxation by identifying
a low septal annular early diastolic mitral
annular motion (e’) velocity.
For the assessment of global LV diastolicfunction, it is recommended to acquire and
measure tissue Doppler signals at least
at the septal and lateral sides of the mitral
annulus and their average, given the
influence of regional function on these
velocities and time intervals.
Input:
s: Systolic annular velocity (blue)
e’: early diastolic annular velocity (yellow)
a’: late diastolic velocity (green)
Output:
E/e’ ratio
e’/a’ ratio
Left Ventricle (LV)
LV diastolic function: Tissue doppler image
①
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 20/80
LV diastolic function: Pulmonary veins
PW Doppler of pulmonary venous flow is
performed in the apical 4-chamber view
and aids in the assessment of LV diastolic
function. If the mitral inflow velocity
profile indicates a predominant
relaxation abnormality with a low E/e=
ratio (normal mean LA pressure), a
pulmonary vein flow duration greaterthan mitral inflow duration at atrial
contraction may indicate an earlier stage
of reduced LV compliance as well as
increased LV end-diastolic pressure.
PV flow is better
Input:
S - Peak systolic vel
D - Peak diastolic vel
Ar - Reverse vel in late diatole
Ar duration
Ar - A - Time difference between Ar duration and
mitral A-wave duration
Left Ventricle (LV) ①
Output:
S/D Ratio
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 21/80
LV diastolic function: Mitral Inflow Propagation
Acquisition is performed in the apical 4-chamberview, using color flow imaging with a narrow color
sector, and gain is adjusted to avoid noise. The M-
mode scan line is placed through the center of the
LV inflow blood column from the mitral valve to the
apex. Then the color flow baseline is shifted to
lower the Nyquist limit so that the central highestvelocity jet is blue. Flow propagation velocity (Vp)
is measured as the slope of the first aliasing
velocity during early filling, measured from the
mitral valve plane to 4 cm distally into the LV cavity.
Alternatively, the slope of the transition from no
color to color is measured. Vp 50 cm/s isconsidered normal. During heart failure and during
myocardial ischemia, there is slowing of mitral-to-
apical flow propagation, consistent with a
reduction of apical suction.
Input:
Vp - Flow propagation velocity (doted white
Line) (cm/s)
Left Ventricle (LV) ①
( ) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 22/80
LV diastolic function: Left Atrium (LA) Volume
Left atrial volume is regarded as a “barometer”
of the chronicity of diastolic dysfunction; with
the most accurate measurements obtained
using the apical 4-chamber and 2-chamber
views (Biplane areal-length or Simpson). This
assessment is clinically important, because
there is a significant relation between LA
remodeling and echocardiographic indices ofdiastolic function. However, Doppler velocities
and time intervals reflect filling pressures at the
time of measurement, whereas LA volume
often reflects the cumulative effects of filling
pressures over time.
Input:
A1 – Max planimetry LA area - A4C
A2 – Max planimetry LA area – A2C
L - Length
Left Ventricle (LV) ①
Output:
LA Volume – Left atrial volume
LAVI – LA volume index
f l ( ) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 23/80
Left Ventricle (LV)LV diastolic function: PCWP (Mean capilary wedge pressure) by E/e’
We can use the average e’ velocity obtained
from the septal and lateral sides of the mitralannulus for prediction of LV filling pressures.
E/e’ ratio < 8 is usually associated with normal
LV filling pressures (PCWP < 15 mmHg) while a
ratio > 15 is associated with increased filling
pressures (PCWP > 15 mmHg). Between 8 ans
15 there is a gray zone with overlapping ofvalues for filling pressures.
Input:
E: Mitral inflow E
velocity
e’ (lateral)
e’ (septal)
Output:
e’ (Average) - of the lateral and
septal e’ values (m/s)
E/e’: ratio
PCWP - Mean Pulmonary capillarywedge pressure (mmHg)
Formulas:
e’ = (e’ lateral + e’ septal) / 2
PCWP = 1.24 * (E/e’) + 1.9
①
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 24/80
Left Atrium (LA)
When LA size is measured in clinical practice,
volume determinations are preferred over
linear dimensions because they allow
accurate assessment of the asymmetric
remodeling of the LA chamber. In the
area-length formula the length is measuredin both the 4- and 2-chamber views and the
shortest of these
2 length measurements is used in the
formula.
①
Quantification of the Left Atrial size: LA Volume (Biplane)
Input:
A1 – Max planimetry LA area - A4C
A2 – Max planimetry LA area – A2C
L - Length
Output:
LA Diameter – (cm)
LA diameter index – cm/m²
LA Volume – Left atrial volume (mL)
LAVI – LA volume index (mL/m²)
②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 25/80
Quantification of the Left Atrial size: M-Mode
The LA size is measured at the end-ventricular
systole when the LA chamber is at its greatest
dimension, care should be taken to avoid
foreshortening of the LA. The base of the LA
should be at its largest size indicating that the
imaging plane passes through the maximalshortening area. The LA length should be also
maximized ensuring alignment along the true
long axis of the LA. The confluences of the
pulmonary veins, and LA appendage should be
excluded. AP linear dimensions of the LA as the
sole measure of LA size may be misleading and
should be accompanied by LA volume
determination in both clinical practice and
research.
Left Atrium (LA)
Input:
LAD – Left atrium diameter (cm)
②
A ti t ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 26/80
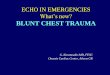
Aortic root
Aortic root dimension
Figure 19 Measurement of aortic root diameter at sinuses
of Valsava from 2-dimensional parasternal long-axis image.
Although leading edge to leading edge technique is shown,
some prefer inner edge to inner edge method.
TTE imaging.
Figure 18 Measurement of aortic root diameters at aortic
valve annulus ( AV ann) level, sinuses of Valsalva (Sinus
Val ), and sinotubular junction (ST Jxn) from midesophageal
long-axis view of aortic valve, usually at angle of
approximately 110 to 150 degrees. Annulus is measured by
convention at base of aortic leaflets. Although leading edge
to leading edge technique is demonstrated for the Sinus Val
and ST Jxn, some prefer inner edge to inner edge method.TEE imaging.
①
Input:
AV Ann – Aortic valve annulus (TEE)
Sinus Val – Sinuses of Valsalva (TEE)
ST Jxn – Sinotubular junction (TEE)
Ao – Aortic root diameter (TTE)
Ri h V i l (RV)

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 27/80
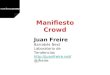
Right Ventricle (RV)RV segments & coronary supply
Segmental nomenclature of the right ventricular walls, along with their coronary supply.
Ao, Aorta; CS, coronary sinus; LA, left atrium; LAD, left anterior descending artery;
LV, left ventricle; PA, pulmonary artery; RA, right atrium; RCA, right coronary artery;
RV, right ventricle; RVOT, right ventricular outflow tract.
Ri ht V t i l (RV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 28/80
Right Ventricle (RV)
RV Size: RV linear dimension
Using 2D echocardiography, RV size canbe measured from a 4-chamber view
obtained from the apical window at
end-diastole. Although quantitative
validation is lacking, qualitatively, the
right ventricle should appear smaller
than the left ventricle and usually nomore than two thirds the size of the left
ventricle in the standard apical 4-
chamber view. If the right ventricle is
larger than the left ventricle in this view,
it is likely significantly enlarged.
RV dimension is best estimated at end-
diastole from a right ventricle –focused
apical 4-chamber view.Input:
RV Basal - RV Basal diameter (mm)
RV mid - RV Mid diameter (mm)
RV long - RV Longitudinal diameter (mm)
①
Ri ht V t i l (RV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 29/80
Right Ventricle (RV)
RV size: RVOT Dimensions
The RVOT is generally considered to include the subpulmonary infundibulum,
or conus, and the pulmonary valve. The RVOT is best viewed from the left parasternaland subcostal windows. The size of the RVOT should be measured at end-diastole on
the QRS deflection.
A) PLAX view, a portion of the proximal RVOT can be measured
B) PSAX view, proximal RVOT measurement
C) PSAX view, Distal RVOT measurement (preferred site for RVOT linear measurement)
Input:
RVOT proximal (mm)
RVOT Distal (mm)
①
Ri h V i l (RV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 30/80
Right Ventricle (RV)
RV size: RV Wall thickness
(A) Subcostal 2-dimensional image of right ventricular wall.
(B) Zoom of region outlined in (A) with right ventricular wall thickness indicated by arrows.
(C) M-mode image corresponding to arrows
in (B).
(D) Zoom of region outlined in (C) with arrows indicating wall thickness at end-diastole.
RV wall thickness is a useful measurement for RVH, usually the result of RVSP overload. RV free wall thicknesscan be measured at end-diastole by M-mode or 2D echocardiography from the subcostal window, preferably at
the level of the tip of the anterior tricuspid leaflet or left parasternal windows. Excluding RV trabeculations and
papillary muscle from RV endocardial border is critical for accurately measuring the RV wall thickness.When
image quality permits, fundamental imaging should be used to avoid the increased structure thickness seen with
harmonic imaging.
Input:
RV Wall thickness (mm)
①
Ri h V i l (RV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 31/80
Right Ventricle (RV)
RV systolic function: TAPSE (Tricuspid Annular Plane Systolic Excursion)
The systolic movement of the baseof the RV free wall provides one of
the most visibly obvious movements
on normal echocardiography. TAPSE
or TAM is a method to measure the
distance of systolic excursion of the
RV annular segment along its
longitudinal plane, from a standard
apical 4-chamber window. It is
inferred that the greater the descent
of the base in systole, the better the
RV systolic function. TAPSE is usually
acquired by placing an M-mode
cursor through the tricuspid annulusand measuring the amount of
longitudinal motion of the
annulus at peak systole
Input:
TAPSE – Tricuspid Annular Plane Excursion mm
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 32/80
Ri ht V t i l (RV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 33/80
Right Ventricle (RV)
Input:
S’ – Systolic excursion velocity
RV systolic function: RV S’ (Systolic excursion velocity)
Among the most reliably and reproducibly
imaged regions of the right ventricle are the
tricuspid annulus and the basal free wall
segment. These regions can be assessed by
pulsed tissue Doppler and color-coded tissue
Doppler to measure the longitudinal velocity
of excursion. This velocity has been termed
the RV S’ or systolic excursion velocity. To
perform this measure, an apical 4-chamber
window is used with a tissue Doppler mode
region of interest highlighting the RV free
wall. The pulsed Doppler sample volume is
placed in either the tricuspid annulus or the
middle of the basal segment of the RV freewall.
+
①
Ri ht V t i l (RV) ②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 34/80
Right Ventricle (RV)RV systolic function: MPI RV - Myocardial Performance Index RV
The MPI, also known as the RIMP or Tei index, is a
global estimate of both systolic and diastolic
function of the right ventricle. It is based on therelationship between ejection and nonejection work
of the heart. The MPI is defined as the ratio of
isovolumic time divided by ET, or [(IVRT +
IVCT)/ET]. The right-sided MPI can be obtained by
two methods: the pulsed Doppler method and the
tissue Doppler method: In the pulsed Doppler
method (A), the ET is measured with pulsedDoppler of Rv outflow (time from the onset to the
cessation of flow), and the tricuspid (valve) closure-
opening time is measured with either pulsed
Doppler of the tricuspid inflow (time from the end of
the transtricuspid A wave to the beginning of the
transtricuspid E wave) or continuous Doppler
of the TR jet (time from the onset to the cessation of
the jet). In the tissue Doppler method (B), all timeintervals are measured from a single beat by
pulsing the tricuspid annulus (left)
Output:
IVCT (Isovolumic Contraction Time)
IVRT (Isovolumic Relaxation Time)
MPI RV
Input:
ET - Ejection Time
TCO - Tric. Closure-Opening Time)
②
Ri ht V t i l (RV)
②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 35/80
Right Ventricle (RV)RV systolic function: RV dP/dt
RV dP/dt can be accurately estimated from the
ascending limb of the TR continuous-wave Doppler
signal. Is commonly calculated by measuring the
time required for the TR jet to increase in velocity
from 1 to 2 m/s. Using the simplified Bernoulli
equation, this represents a 12 mm Hg increase in
pressure. The dP/dt is therefore calculated as 12
mm Hg divided by this time (in seconds), yielding a
value in millimeters of mercury per second.
Because of the lack of data in normal
subjects, RV dP/dt cannot be recommended for
routine uses. It can be considered in subjects with
suspected RV dysfunction. RV dP/dt <
approximately 400 mm Hg/s is likely abnormal.Point 1 represents the point at which the tricuspid regurgitation
(TR) signal meets the 1 m/s velocity scale marker,while point 2 represents the point at which the TR signal meets
the 2 m/s velocity scale marker. Point 3 represents the time required
for the TR jet to increase from 1 to 2 m/s. In this example,
this time is 30 ms, or 0.03 seconds. The dP/dt is therefore 12mm
Hg/0.03 seconds, or 400 mm Hg/s.
②
Ri ht V t i l (RV)
②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 36/80
Right Ventricle (RV)RV systolic function: RV IVA (Myocardial Acceleration During
Isovolumic Contraction)Isovolumetric acceleration (IVA) is a novel
tissue Doppler parameter for the assessment
of systolic function. Myocardial acceleration
during isovolumic contraction is defined as the
peak isovolumic myocardial velocity divided by
time to peak velocity and is typically measured
for the right ventricle by Doppler tissue
imaging at the lateral tricuspid annulus. Forthe calculation
of IVA, the onset of myocardial acceleration is
at the zero crossing point of myocardial
velocity during isovolumic contraction. In
studies in patients with conditions affected by
RV function, RV IVA may be used, and whenused, it should be measured at the lateral
tricuspid annulus. RV IVA is not recommended
as a screening parameter for RV systolic
function in the general echocardiography
laboratory population.
Pulsed wave tissue Doppler imaging of the RV free
wall of a control subject. 1: peak myocardial systolic
velocity (Sm), 2: peak early diastolic velocity (Em), 3:
peak late diastolic velocity (Am) 4: isovolumetric
contraction time (IVCT), 5: ejection time (ET), 6: peak
myocardial isovolumetric contraction velocity (IVV),
acceleration time (AT), isovolumetric acceleration (IVA)(red).
②
Ri ht V t i l (RV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 37/80
Right Ventricle (RV)RV diastolic function: PW Tricuspid inflow
From the apical 4-chamber view, the Doppler beam
should be aligned parallel to the RV inflow. Proper
alignment may be facilitated by displacing the
transducer medially toward the lower parasternal
region.
The sample volume should be placed at the tips of
the tricuspid leaflets. With this technique,
measurement of transtricuspid flow velocities canbe achieved in most patients, with low
interobserver and intraobserver variability. Care
must be taken to measure at held end-expiration
and/or take the average of ≥ 5 consecutive beats.
The presence of moderate to severe TR or atrial
fibrillation could confound diastolic parameters,and most studies excluded such patients.Input:
Tricuspid Flow Profile (red)
Output:
E wave velocity
A wave velocity
E/A ratio
Tricuspid E/e’
DT - Deceleration time (ms)
E
①
Right Ventricle (RV) ②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 38/80
Right Ventricle (RV)RV diastolic function: Tissue doppler imaging
Input:
S’ Systolic velocity
E’ velovity
A’ velocity
Output:
E’/A’ ratio
E/E’ ratio
②
Among the most reliably and reproduciblyimaged regions of the right ventricle are the
tricuspid annulus and the basal free wall
segment. These regions can be assessed by
pulsed tissue Doppler and color-coded tissue
Doppler to measure the longitudinal velocity
of excursion. S’ is systolic velocity, E’ is early
diastolic velocity and A’ is late diastolic
velocity. To perform this measure, an apical
4-chamber window is used with a tissue
Doppler mode region of interest highlighting
the RV free wall. The pulsed Doppler sample
volume is placed in either the tricuspid
annulus or the middle of the basal segmentof the RV free wall.
Right Ventricle (RV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 39/80
Right Ventricle (RV)RV hemodynamics: sPAP (Systolic pulmonary artery pressure)
SPAP can be estimated using TR velocity, and
PADP can be estimated from the end-diastolicpulmonary regurgitation velocity. Mean PA
pressure can be estimated by the PA
acceleration time (AT) or derived from the
systolic and diastolic pressures. RVSP can be
reliably determined from peak TR jet velocity,
using the simplified Bernoulli equation and
combining this value with an estimate of the
RA pressure: RVSP = 4 (V) ² + RA pressure,
where V is the peak velocity (in meters per
second) of the tricuspid valve regurgitant jet,
and RA pressure is estimated from IVC
diameter and respiratory changes. Because
velocity measurements are angle dependent,it is recommended to gather TR signals from
several windows and to use the signal with the
highest velocity.
Input:
TR Jet velocity
PAP mmHg
(depending on
IVC collapsability on sniff)
Output:
TR velocity
sPAP
RV Systolic pressure
①
Right Ventricle (RV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 40/80
RV hemodynamics: dPAP (Diastolic Pulmonary artery pressure)
mPAP (mean Pulmonary Artery Pressure)
Right Ventricle (RV)
dPAP can be estimated from the velocity
of the end-diastolic pulmonary
regurgitant jet using the modified
Bernoulli equation: [PADP = 4 (end-diastolic pulmonary regurgitant velocity)²
+ RA pressure]. Mean PA pressure
correlates with 4 x (early PI velocity) ² +
estimated RAP .
Input:
PR PHT (yellow)
PR Vmax – Pulmonary regurgitation
max velocity (red)
PR end Vmax - Pulmonary
regurgitation end max velocity
(green)
Output:
PA Reg PHT (ms)
PA peak diastolic gradient
dPAP (end diastolic gradient)
mPAP (mean Pulmonary
Artery pressure)
①
Right Ventricle (RV) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 41/80
Right Ventricle (RV)RV hemodynamics: mPAP (mean Pulmonary artery pressure)
AT method
Once systolic and diastolic pressures
are known, mean pressure may be
estimated by the standard formula
mean PA pressure = 1/3(SPAP) +
2/3(PADP). Mean PA pressure may
also be estimated by using pulmonary
AT measured by pulsed Doppler of thepulmonary artery in systole, whereby
mean PA pressure = 79 (0.45 AT).
Generally, the shorter the AT
(measured from the onset of the Q
wave on electrocardiography to theonset of peak pulmonary flow
velocity), the higher the PVR
(Pulmonary Vascular Resistance) and
hence the PA pressure.
Input:
PA TVI - (Time velocity
Integral) (yellow)
Output:
PA AT (acceleration time)
mPAP
mPAP (mean Pulmonary
Artery pressure)
①
Right Atrium (RA) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 42/80
Right Atrium (RA)
The primary transthoracic window for imaging the
right atrium is the apical 4-chamber view. From thiswindow, RA area is estimated by planimetry. The
maximal long-axis distance of the right atrium is
from the center of the tricuspid annulus to the
center of the superior RA wall, parallel to the
interatrial septum. A mid-RA minor distance is
defined from the mid level of the RA free wall to theinteratrial septum, perpendicular to the long axis.
RA area is traced at the end of ventricular systole
(largest volume) from the lateral aspect of the
tricuspid annulus to the septal aspect, excluding the
area between the leaflets and annulus, following
the RA endocardium, excluding the IVC and superior
vena cava and RA appendage
Right atrium size
Input:
RA End-Systolic Area (cm ²)
RA Major Dimension (mm)
RA Minor Dimension (mm)
①
Right Atrium (RA) ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 43/80
Right Atrium (RA)
Inferior Vena Cava: RA pressure
The subcostal view is most useful for imaging
the IVC, with the IVC viewed in its long axis.
The measurement of the IVC diameter should
be made at end-expiration and just proximal
to the junction of the hepatic veins that lie
approximately 0.5 to 3.0 cm proximal to the
ostium of the right atrium. To accurately
assess IVC collapse, the change in diameter ofthe IVC with a sniff and also with quiet
respiration should be measured, ensuring that
the change in diameter does not reflect a
translation of the IVC into another plane.
The measurements are done at end-diastole.
IVC diameter ≤ 2.1 cm that collapses >50% with a sniff suggests a normal RA pressure of 3 mm Hg (range, 0-5 mmHg)
IVC diameter > 2.1 cm that collapses <50% with a sniff suggests a high RA pressure of 15 mm Hg (range, 10-20 mmHg)
In indeterminate cases in which the IVC diameter and collapse do not fit this paradigm, an intermediate value
of 8 mm Hg (range, 5-10 mm Hg) may be used
①
Valvular stenosis ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 44/80
Valvular stenosis
Aortic stenosis: AS jet velocity
AS jet velocity (Antegrade Systolic Velocity) isdefined as the highest velocity signal obtained from
any window after a careful examination; lower values
from other views are not reported.The antegrade
systolic velocity across the narrowed aortic valve, or
aortic jet velocity, is measured using continuous-
wave (CW) Doppler (CWD) ultrasound. A dedicated
small dual-crystal CW transducer is recommended
both due to a higher signal-to-noise ratio and to allow
optimal transducer positioning and angulation,
particularly when suprasternal and right parasternal
windows are used. However, when stenosis is only
mild (velocity 3 m/s) and leaflet opening is well seen,
a combined imaging-Doppler transducer may be
adequate.
Input:
AS jet velocity (m/s)
VTI – Velocity Time
integral
Output:
Mean gradient (mmHg)
①
Valvular stenosis ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 45/80
Valvular stenosis
Aortic stenosis: AVA (Continuity equation VTI)
Aortic valve area can be calculated by usingthe principle of conservation of mass –
“What comes in must go out”.
AVA indexed to BSA should be considered
for the large and small extremes of body
surface area.
Left ventricular outflow tract diameter ismeasured in the parasternal long-axis view
in mid-systole from the white –
black interface of the septal endocardium to
the anterior mitral leaflet, parallel to the
aortic valve plane and within 0.5 –1.0 cm
of the valve orifice. Input:
LVOT diameter (mm)
VTI1 (Subvalvular VTI) (cm)
VTI2 (Max VTI across the valve
(cm)
Output:
AVA (cm²)
AVAI (Indexed to BSA)
(cm²/m²)
AVA = (CSALVOT x VTILVOT) / VTIAV
①
Valvular stenosis ②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 46/80
Valvular stenosis
Aortic stenosis: AVA (Continuity equation Vmax)
②
The simplified continuity equation is based
on the concept that in native aortic valve
stenosis the shape of the velocity curve in
the outflow tract and aorta is similar so that
the ratio of LVOT to aortic jet VTI is nearly
identical to the ratio of the LVOT to aortic jet
maximum velocity (V). This method is less
well accepted because some experts are
concerned that results are more variable
than using VTIs in the equation.
AVA = CSALVOT x VLVOT / V AV
Input:
LVOT diameter (mm)
V1 (Subvalvular Velocity) (m/s)
V2 (Max velocity across the valve)
(m/s)
Output:
AVA (cm²)
AVAI (Indexed to BSA)
(cm²/m²)
Valvular stenosis ②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 47/80
Valvular stenosis
Aortic stenosis: Velocity ratio
②
Another approach to reducing error related toLVOT diameter measurements is removing CSA from
the simplified continuity equation. This dimensionless
velocity ratio expresses the size of the valvular
effective area as a proportion of the CSA of the
LVOT. Substitution of the time-velocity integral can
also be used as there was a high correlation
between the ratio using time –velocity integral andthe ratio using peak velocities. In the absence of
valve stenosis, the velocity ratio approaches 1, with
smaller numbers indicating more severe stenosis.
Severe stenosis is present when the velocity ratio is
0.25 or less, corresponding to a valve area 25% of
normal.
Velocity ratio = VLVOT / V AV
Input:
V1 (Subvalvular Velocity) (m/s)
V2 (Max velocity across the valve)
(m/s)
Output:
VR - Velocity Ratio
Valvular stenosis ②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 48/80
Valvular stenosis
Aortic stenosis: Planimetry of anatomic valve area
②
Multiple studies have evaluated the method
of measuring anatomic (geometric) AVA by
direct visualization of the valvular orifice,
either by 2D or 3D TTE or TEE. Planimetry
may be an acceptable alternative when
Doppler estimation of flow velocities isunreliable. However, planimetry may be
inaccurate when valve calcification causes
shadows or reverberations limiting
identification of the orifice.
Input:
AV planimetry
Output:
AVA (cm²)

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 49/80
Valvular stenosis ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 50/80
Valvular stenosisMitral stenosis: PHT (Pressure Half-time)
Is the time interval in milliseconds between the
maximum mitral gradient in early diastole and the
time point where the gradient is half the maximum
initial value. The decline of the velocity of diastolic
transmitral blood flow is inversely proportional to
valve area (cm2), and MVA is derived using the
empirical formula: MVA = 220 ⁄ T1⁄2.
T1/2 is obtained by tracing the deceleration slope ofthe E-wave on Doppler spectral display of
transmitral flow and valve area is automatically
calculated by the integrated software of currently
used echo machines. The Doppler signal used is the
same as for the measurement of mitral gradient.
Input:MV PHT
Output:MV PHT (ms)
MVA (cm ²)
①
Valvular stenosis ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 51/80
Valvular stenosis
Mitral stenosis: Pressure gradient
Mitral stenosis is the most frequent valvularcomplication of rheumatic fever. Even in
industrialized countries, most cases remain of
rheumatic origin as other causes are rare. The
estimation of the diastolic pressure gradient is
derived from the transmitral velocity flow curve
using the simplified Bernoulli equation ΔP = 4v ².The use of CWD is preferred to ensure maximal
velocities are recorded. Doppler gradient is
assessed using the apical window in most cases as
it allows for parallel alignment of the ultra sound
beam and mitral inflow.
Input:MV Flow profile
Output:MV Peak Velocity
MV Peak GP (mmHg)
MV mean Velocity
MV Mean GP (mmHg)
①
Valvular stenosis ②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 52/80
Valvular stenosis
Mitral stenosis: Continuity equation
②
As in the estimation of AVA, the
continuity equation is based on the
conservation of mass, stating in this
case that the filling volume of diastolic
mitral flow is equal to aortic SV. The
accuracy and reproducibility of the
continuity equation for assessing MVAare hampered by the number of
measurements increasing the impact of
errors of measurements. The continuity
equation cannot be used in cases of
atrial fibrillation or associated significant
MR or AR.
MVA = (CSALVOT x VTIAortic) / VTIMitralInput:
LVOT (cm)
VTI Ao (cm)
VTI Mitral (cm)
Output:
MVA (cm²)
Valvular stenosis ②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 53/80
Valvular stenosis ②
The proximal isovelocity surface area method is
based on the hemispherical shape of theconvergence of diastolic mitral flow on the atrial
side of the mitral valve, as shown by colour Doppler.
It enables mitral volume flow to be assessed and,
thus, to determine MVA by dividing mitral volume
flow by the maximum velocity of diastolic mitral flow
as assessed by CWD. This method can be used in
the presence of significant MR.
However, it is technically demanding and requires
multiple measurements. Its accuracy is impacted
upon by uncertainties in the measurement of the
radius of the convergence hemisphere, and the
opening angle.
MVA = 2 x π x r² x (Vr / Vmax) x (α⁰ / 180°)
Output:
VFR (Volume flow rate) (cc)
MVA (cm²)
Input:
2 × π × r 2 : Proximal isovelocity hemispheric surface area at a radial
distance r from the orifice.
Vr : Aliasing velocity at the radial distance r (cm/s)
Vmax : Peak mitral stenosis velocity by CW (m/s)α : Angle between two mitral leaflets on the atrial side (degree0)
Mitral stenosis: PISA method
Valvular stenosis ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 54/80
Valvular stenosis
Tricuspid stenosis: CWD hemodynamic evaluation
①
Tricuspid stenosis (TS) is currently the least common of
the valvular stenosis lesions given the low incidence ofrheumatic heart disease. As with all valve lesions, the
initial evaluation starts with an anatomical assessment
of the valve by 2D echocardiography using multiple
windows such as parasternal right ventricular inflow,
parasternal short axis, apical four-chamber and
subcostal four-chamber. The evaluation of stenosis
severity is primarily done using the hemodynamic
information provided by CWD. Because tricuspid inflow
velocities are affected by respiration, all measurements
taken must be averaged throughout the respiratory
cycle or recorded at end-expiratory apnea. In theory,
the continuity equation should provide a robust method
for determining the effective valve area as SV divided
by the tricuspid inflow VTI as recorded with CWD. In
the absence of significant TR, one can use the SV
obtained from either the left or right ventricular
outflow; a valve area of 1 cm2 is considered indicativeof severe TS.
However, as severity of TR increases, valve area is
progressively underestimated by this method.Input:
TV Flow profileOutput:
Peak diastolic velocity
Mean gradient (mmHg)
PHT (pressure half-time)
mmHg
Valvular stenosis ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 55/80
Valvular stenosis
Pulmonic stenosis: Pressure gradient
Pulmonary stenosis is almost always congenital in
origin. The normal pulmonary valve is trileaflet. The
congenitally stenotic valve may be trileaflet,
bicuspid, unicuspid, or dysplastic. Acquired stenosis
of the pulmonary valve is very uncommon.
Quantitative assessment of pulmonary stenosis
severity is based mainly on the transpulmonary
pressure gradient. The estimation of the systolic
pressure gradient is derived from thetranspulmonary velocity flow curve usingthe simplified Bernoulli equation ΔP = 4 (V) ². This
estimation is reliable, as shown by the good
correlation with invasive measurement using
cardiac catheterization. Continuous-wave Doppler
is used to assess the severity when even mild
stenosis is present. It is important to line up the
Doppler sample volume parallel to the flow with the
aid of colour flow mapping where appropriate. In
adults, this is usually most readily performed from aparasternal short-axis view.
①
Input:
Peak velocity (m/s)Output:
Peak Gradient (mmHg)
Valvular regurgitation ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 56/80
Valvular regurgitation
Aortic regurgitation: Jet diameter/LVOT diameter ratio %
①
Imaging of the regurgitant jet is used in all
patients with AR because of its simplicityand real time availability.The parasternal
views are preferred over apical views
because of better axial resolution. The
recommended measurements are those of
maximal proximal jet width obtained from
the long-axis views and its ratio to the LVoutflow tract diameter. Similarly, the cross-
sectional area of the jet from the
parasternal short-axis view and its ratio to
the LV outflow tract area can also be used.
The criteria to define severe AR are ratios
of ≥ 65% for jet width and ≥ 60% for jetarea.
Is possible to use the CSA instead width
for both Jet and LVOT.Input:
Jet Width (red)
LVOT Width (yellow)
Output:
Jet width/LVOT Width ratio (%)
Valvular regurgitation ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 57/80
Valvular regurgitation
Aortic regurgitation: VC (Vena contracta)
The Vena contracta is the narrowest portion of theregurgitant jet downstream from the regurgitant
orifice. It is sligtly smaller than the anatomic
regurgitant orifice due to boundary effect. For AR,
imaging of the VC is obtained from the PLAX view.
To properly identify the VC the three components of
the regurgitant jet should be visualized (flow
convergence zone, vena contracta, jet turbulence).
A narrow colour sector scan coupled with the zoommode is recommended to improve measurement
accuracy. It provides thus an estimation of the size
of the EROA (Estimated regurgitant orifice area)
and is smaller that the regurgitant jet width in the
LVOT. Using a Nyquist limit of 50-60 cm/s, a vena
contracta width of < 3mm correlates with mild AR,
whereas a width > 6mm indicates severe AR.When feasible the measurement of VC width is
recommended to quantify AR severity. Intermediate
VC values (3-6 mm) needs confirmation by a more
quantitative method.
Input:
AR VC width – Aortic regurgitation Vena Contracta width (cm)
①
Valvular regurgitation ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 58/80
a u a egu g a o
Aortic regurgitation: PISA (Proximal Isovolumetric Surface Area)
The assessment of the flow convergence zone has
been less extensively performed in AR than in MR.
The colour flow velocity scale is shifted towards the
direction of the jet (downwards or upwards in the
left parasternal view depending on the jet
orientation and upwards in the apical view).
1- Color Doppler settings must be correctly
adjusted for the PISA method. The Nyquist-limit
should be placed around 50-60 cm/s.2- Afterwards, base line should be shifted in the
direction of the regurgitation jet, until a well-defined
hemisphere appears.
3- To calculate VTI of regurgitation jet, CW-Doppler
profile area should be delineated.
4- By measuring PISA radius it is important to hit
correctly the limit ot the hemisphere. Small errors
can produce important variations.
When feasible, the PISA method is highly
recommended to assess the severity of AR. It can
be used in both central and eccentric jets. The
window recommended is PLAX view for flow
convergence.
Input:
PISA Radius
AR VTI
Output:
AR EROA (Effective Regurgitant
Orifice Area) cm ²
AR R Vol (regurgitant volume)
mL/beat
①
Valvular regurgitation
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 59/80
g g
Aortic regurgitation: Jet deceleration rate (PHT)
The rate of deceleration of the diastolic regurgitant jet and the derived pressure half-time reflect the
rate of equalization of aortic and LV diastolic
pressures. With increasing severity of AR, aortic
diastolic pressure decreases more rapidly. Pressure
half-time is easily measured if the peak diastolic
velocity is appropriately recorded. A pressure half-
time 500 ms is usually compatible with mild AR
whereas a value 200 ms is considered consistent
with severe AR.
CW Doppler of the AR jet should be routinely
recorded but only utilized if a complete signal is
obtained. The PHT is influenced by chamber
compliance and pressure, for this reason it serves
only as a complementary finding for AR severity
assessment.
Input:
AR PHT - Aortic reg Pressure half-time (ms)
①
Valvular regurgitation
②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 60/80
Output:
EROA
R Vol.
RF (Regurgitant Fraction ) %
Aortic regurgitation: Flow quantitation - PW
g g
Quantitation of flow with pulsed Doppler for the
assessment of AR is based on comparison ofmeasurement of aortic stroke volume at the
LVOT with mitral or pulmonic stroke volume.
Total stroke volume (aortic stroke volume) can
also be derived from quantitative 2D
measurements of LV end-diastolic and end-
systolic volumes. EROA can be calculated from
the regurgitant stroke volume and the
regurgitant jet velocity time integral by CWDoppler. As with the PISA method, a regurgitant
volume ≥60 ml and EROA ≥0.30 cm2 are
consistent with severe AR. The quantitative
Doppler method cannot be used if there is more
than mild mitral regurgitation, unless the
pulmonic site is used for systemic flow
calculation. In general, a RF > 50 % indicatessevere AR. Volumetric measurements with PW
are Time consuming, and requires multiple
measurements, so the source of errors are
higher.Input:
LVOT PW profile (A5C)
LVOT diameter (PLAX)
Mitral inflow profile PW (A4C)
Mitral annulus diameter (max
opening MV (A4C)
②
Valvular regurgitation ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 61/80
g g
Aortic regurgitation: Aortic diastolic flow reversal PW
It is normal to observe a brief diastolic flow reversal
in the aorta. The flow reversal is best recorded in theupper descending aorta at the aortic isthmus level
using a suprasternal view, or in the lower descending
aorta using a longitudinal subcostal view. With
increasing aortic regurgitation both the duration and
the velocity of the reversal increase. Therefore, a
holodiastolic reversal is usually a sign of at least
moderate aortic regurgitation. A prominent
holodiastolic reversal with a diastolic time integral
similar to the systolic time integral is a reliable
qualitative sign of severe AR. However, reduced
compliance of the aorta seen with advancing age
may also prolong the normal diastolic reversal in the
absence of significant AR. In general, an end-
diastolic flow velocity > 20 cm/s is indicative of
severe AR.
①
Input:
End-diastolic velocity (cm/s)
Valvular regurgitation ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 62/80
g g
Mitral regurgitation: Vena Contracta (VC)
The vena contracta should be imaged in high-
resolution, zoom views for the largest obtainable
proximal jet size for measurements. The examiner
must search in multiple planes perpendicular to the
commissural line (such as the parasternal long-axis
view), whenever possible. The width of the neck or
narrowest portion of the jet is then measured. The
regurgitant orifice in MR may not be circular, and is
often elongated along the mitral coaptation line. Thetwo-chamber view, which is oriented parallel to the
line of leaflet coaptation, The width of the vena
contracta in long-axis views and its cross-sectional
area in short-axis views can be standardized from the
parasternal view.s A vena contracta 0.3 cm
usually denotes mild MR where as the cut-off for
severe MR has ranged between 0.6 to 0.8 cm.
Input:
MR VC width (cm)
①
Valvular regurgitation ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 63/80
g gMitral regurgitation: PISA
Most of the experience with the PISA method for
quantitation of regurgitation is with MR. Qualitatively,
the presence of PISA on a routine examination (at
Nyquist limit of 50-60 cm/s) should alert to the
presence of significant MR. Several clinical studies
have validated PISA measurements of regurgitant
flow rate and EROA. This methodology is more
accurate for central regurgitant jets than eccentric
jets, and for a circular orifice than a noncircular
orifice. Flow convergence should be optimized fromthe apical view, usually the fourchamber view, using
a zoom mode. For determination of EROA, it is
essential that the CW Doppler signal be well aligned
with the regurgitant jet. Poor alignment with an
eccentric jet will lead to an underestimation of
velocity and an overestimation of the EROA.
Generally, an EROA 0.4 cm2 is consistent withsevere MR, 0.20-0.39 cm² moderate, and 0.20 cm²
mild MR.
Input:
PISA Radius
MR VTI
Output:
MR EROA (Effective Regurgitant
Orifice Area) cm²
MR R Vol (regurgitant volume)mL/beat
①
Valvular regurgitation
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 64/80
In most patients, maximum MR velocity is 4 to 6 m/sdue to the high systolic pressure gradient between
the LV and LA.The velocity itself does not provide useful information
about the severity of MR. However, the contour
of the velocity profile and its density are useful. A
truncated, triangular jet contour with early peaking
of the maximal velocity indicates elevated LA
pressure or a prominent regurgitant pressure wave in
the LA. The density of the CW Doppler signal is a
qualitative index of MR severity. A dense signal that
approaches the density of antegrade flow suggests
significant MR, whereas a faint signal, with or without
an incomplete envelope represents mild or trace
MR. Using CW Doppler, the tricuspid regurgitation jet
should be interrogated in order to estimatepulmonary artery systolic pressure. The presence of
pulmonary hypertension provides another indirect
clue as to MR severity and compensation to the
volume overload.
g gMitral regurgitation: Continuous wave doppler
Input:
MR VTI
Output:
MR Peak velocity (m/s)
①
Valvular regurgitation
②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 65/80
g gMitral regurgitation: Mitral to Aortic TVI ratio
In the absence on mitral stenosis, the increase in
transmitral flow that occurs with increasing MRseverity can be detected as higher flow velocities
during early sistolic filling (increased E velocity). In
the absence of mitral stenosis, peak E velocity > 1.5
m/s suggest severe MR. Conversely, a dominant A
wave (Atrial contraction) basically excludes severe
MR. The PW doppler mitral to aortic TVI ratio is also
used as an easily measured index for the
quantification of the isolated pure organic MR. Mitral
inflow doppler tracings are obtaines at the mitral
leaflet tips and aortic flow at the annulus level in the
apical four-chamber view. A TVI ratio > 1.4 strongly
suggest severe MR whereas a TVI ratio < 1 is in
favor of mild MR.
Both the pulsed Doppler mitral to aortic TVI ratio and
the systolic pulmonary flow reversal are specific forsevere MR. They represent the strongest additional
parameters for evaluating MR severity.
Input:
Mitral VTI
Aortic VTI
Output:
Mitral to Aortic VTI ratio
②
Valvular regurgitation
②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 66/80
g gMitral regurgitation: Pulmonary venous flow
Pulsed Doppler evaluation of pulmonary venous flow
pattern is another aid for grading the severity of MR.
In normal individuals, a positive systolic wave (S)
followed by a smaller diastolic wave (D) is classically
seen in the absence of diastolic dysfunction. With
increasing severity of MR, there is a decrease of the
S wave velocity. In severe MR, the S wave becomes
frankly reversed if the jet is directed into the sampled
vein. As unilateral pulmonary flow reversal can occurat the site of eccentric MR jets, sampling through all
pulmonary veins is recommended, especially during
transoesophageal echocardiography. Although,
evaluation of right upper pulmonary flow can often be
obtained using TTE, evaluation is best using TEE
with the pulse Doppler sample placed about 1 cm
deep into the pulmonary vein.
Both the pulsed Doppler mitral to aortic TVI ratio and
the systolic pulmonary flow reversal are specific for
severe MR. They represent the strongest additional
parameters for evaluating MR severity.
Pulmonary venous flow is a qualitativeparameter, no measurements have to be
done.
Valvular regurgitation ②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 67/80
Output:
MR EROA
MR R Vol.
MR RF (Regurgitant Fraction ) %
g g
Input:
LVOT PW profile (A5C)
LVOT diameter (PLAX)
Mitral inflow profile PW (A4C)
Mitral annulus diameter (max
opening MV (A4C)
Mitral regurgitation: Flow quantitation - PW
Pulsed Doppler tracings at the mitral leaflet tips
are commonly used to evaluate LV diastolicfunction. Patients with severe MR often
demonstrate a mitral inflow pattern with a
dominant early filling (increased E velocity) due
to increased diastolic flow across the mitral
valve, with or without an increase in left atrial
pressure. In severe mitral regurgitation without
stenosis, the mitral E velocity is higher than thevelocity during atrial contraction (A velocity),
and usually greater than 1.2 m/sec. For these
reasons, a mitral inflow pattern with an A- wave
dominance virtually excludes severe MR.
Volumetric measurements with PW are Time
consuming and not recommended as first level
method to quantify MR severity.

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 68/80
Valvular regurgitation
①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 69/80
Tricuspid regurgitation: Flow convergence (PISA)
Although providing quantitative assessment, clinical
practice reveals that the flow convergence method israrely applied in TR. This approach has been
validated in small studies. The apical four-chamber
view and the parasternal long and short axis views
are classically recommended for optimal visualization
of the PISA. The area of interest is optimized by
lowering imaging depth and the Nyquist limit to ∼15 –
40 cm/s. The radius of the PISA is measured at mid-systole using the first aliasing. Qualitatively, a TR
PISA radius >9 mm at a Nyquist limit of 28 cm/s
alerts to the presence of significant TR whereas a
radius <5 mm suggests mild TR. An EROA ≥ 40 mm2
or a R Vol of ≥45 mL indicates severe TR.
When feasible, the PISA method is reasonable to
quantify the TR severity. An EROA ≥ 40 mm2 or a R
Vol ≥ 45 mL indicates severe TR.
Input:
TR PISA Radius
TR VTI
Output:
TR EROA (Effective Regurgitant
Orifice Area) cm²
TR R Vol (regurgitant volume)
mL/beat
② Valvular regurgitation

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 70/80
Tricuspid regurgitation: CW jet velocity
Recording of TR jet velocity provides a
useful method for noninvasivemeasurement of RV or pulmonary artery
systolic pressure. It is important to note
that TR jet velocity, similar to velocity of
other regurgitant lesions, is not related to
the volume of regurgitant flow. In fact,
massive TR is often associated with a
low jet velocity ( 2m/s), as there is near
equalization of RV and right atrial
pressures, conversely, mild regurgitation
may have a very high jet velocity, when
pulmonary hypertension is present.
Similar to MR, the features of the TR jet
by CW Doppler that help in evaluatingseverity of regurgitation, are the signal
intensity and the contour of the
velocity curve.
Input:
TR flow profile
Valvular regurgitation
②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 71/80
Tricuspid regurgitation: Anterograde velocity of tricuspid inflow
A small degree of tricuspid regurgitation
(TR) is present in about 70% of normalindividuals. Pathologic regurgitation is
often due to right ventricular (RV) and
tricuspid annular dilation secondary to
pulmonary hypertension or RV
dysfunction. Primary causes of TR
include endocarditis, carcinoid heartdisease, Ebstein’s anomaly, and
rheumatic disease.
Similar to MR, the severity of TR will
affect the early tricuspid diastolic filling (E
velocity). In the absence of tricuspid
stenosis, the peak E velocity increases inproportion to the degree of TR. Tricuspid
inflow Doppler tracings are obtained at
the tricuspid leaflet tips. A peak E velocity
≥1 m/s suggests severe TR
Input:
E wave velocity
Valvular regurgitation ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 72/80
Pulmonary regurgitation: Jet width - CFM
Minor degrees of pulmonary regurgitation
(PR) have been reported in 40-78% of
patients with morphologically normal
pulmonary valves and no other evidence
of structural heart disease Pathologic
regurgitation is infrequent, and should be
diagnosed mainly in the presence of
significant structural abnormalities of the
right heart. Color Doppler flow mappingis the most widely used method to
identify PR. A diastolic jet in the RV
outflow tract, beginning at the line of
leaflet coaptation and directed toward the
right ventricle is diagnostic of PR.
Although this measurement suffers froma high inter-observer variability, a jet
width that occupies >65% of the RV
outflow tract width measured in the same
frame is in favour of severe PR.
Input:
Color Jet width (white)
RVOT width (yellow)
Output:
Jet to RVOT width ratio (%)
Valvular regurgitation ①

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 73/80
Pulmonary regurgitation: Vena contracta (VC)
Although the vena contracta width is
probably a more accurate method thanthe jet width to evaluate PR severity by
colour Doppler, it lacks validation studies.
As for other regurgitations, the same
limitations are applicable. The shape of
the vena contracta is complex in most
cases.
Input:
PR VC width (cm)
Valvular regurgitation
②

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 74/80
Pulmonary regurgitation: Jet density and deceleration rate
CW Doppler is frequently used to measurethe end-diastolic velocity of PR and thus
estimate pulmonary artery end-diastolic
pressure. However, there is no clinically
accepted method of quantifying pulmonary
regurgitation using CW Doppler. Similar to
AR, the density of the CW signal provides
a qualitative measure of regurgitation. A
rapid deceleration rate, while consistent
with more severe regurgitation, is
influenced by several factors including RV
diastolic properties and filling pressures.
A pressure half-time < 200 ms is
consistent with severe PR.
Input:
PR PHT
Output:
Deceleration rate (ms)

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 75/80
Prosthetic valves

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 76/80
Prosthetic aortic valves: doppler investigation (formulas previously described)
Doppler echocardiography of
the valve
- Peak velocity gradient
- Mean gradient
- Contour of the jet velocity, AT
(acceleration time)
- DVI (doppler velocity index) *
- EOA (Effective orifice area)
- Presence, location, and
severity of regurgitation
Pertinent cardiac chambers - LV size, function, and Hypertrophy
* DVI = VLVO / VPrAV . DVI is the Ratio of respective VTIs, and can
be approximated as the ratio of the respectivepeak velocities. (simplified continuity equation)
DVI = Doppler Velocity Index
VLVO = Subvalvular (LVOT) velocity
VPR AV = Max velocity across the valve
Prosthetic valves

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 77/80
Doppler echocardiography of
the valve
- Peak early velocity
- Mean gradient
- Heart rate at the time of Doppler
- Pressure half-time
- DVI*: (Doppler velocity index)
- EOA (Effective oriffice area)
- Presence, location, and severityof regurgitation†
Other pertinent
echocardiographic and doppler
parameters
- LV size and function
- RV size and function
- Estimation of pulmonary arterypressure
* DVI = VPrMV / VLVO DVI is the Ratio of respective VTIs, and can
be approximated as the ratio of the respectivepeak velocities. (simplified continuity equation)
Prosthetic mitral valves: doppler investigation (formulas previously described)
VPRMV = Max velocity across the prosthetic mitral valve
Prosthetic valves

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 78/80
Doppler echocardiography of
the valve
- Peak velocity/peak gradient
- Mean gradient
- DVI *
- EOA*
- Presence, location, and severityof regurgitation
Related cardiac chambers - RV size, function, and hypertrophy
- RV systolic pressure
* Theoretically possible to measure. Few data exist.
Prosthetic pulmonary valves: doppler investigation (formulas previously described)
Prosthetic valves

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 79/80
Doppler echocardiography of
the valve
- Peak early velocity
- Mean gradient
- Heart rate at time of Doppler
assessment
- Pressure half-time
- VTIPRTV / VTILVO *
- EOA
- Presence, location, and severity of TR
Related cardiac chambers,
inferior vena cava and hepaticveins
- RV size and function
- Right atrial size
- Size of inferior vena cava and
response to inspiration- Hepatic vein flow pattern
Prosthetic tricuspid valves: doppler investigation (formulas previously described)
* Feasible measurements of valve function, similar to mitral prostheses,
but no large series to date.
VTIPRTV: Velocity Time Integral Prosthetic Tricuspid Valve
VTILVO: Velocity Time Integral LVOT

8/12/2019 Cardiac Measurements Guidelines | AHA and EAE
http://slidepdf.com/reader/full/cardiac-measurements-guidelines-aha-and-eae 80/80