Embed Size (px)
Citation preview

180 Injury, 12. 180-l 88 Printedin GreatBritain
Cardiac contusion in the patient with multiple injuries
Shmuel Katz, Zvi Gimmon (Goldschmidt) and Azai Appelbaum
Departments of Surgery and Cardiac Thoracic Surgery, Hadassah Hebrew University Hospital. Jerusalem
Summary We have treated 20 patients with multiple injuries and concomitant myocardial contusion. The diagnosis of myocardial contusion was based mainly on serial ECG tracings which showed arrhythmias, dynamic ischa- emit patterns or conduction disturbances. The clinical and laboratory findings of cardiac contusion are some- times indistinguishable from those found in multiple injuries. Furthermore, they are overshadowed by the overt manifestation of cerebral, thoraco-abdominal and skeletal injuries. Awareness and prompt diag- nostic measures are essential in the diagnosis ofcardiac injury. Strict cardiac monitoring following multiple trauma will prevent serious or even fatal outcome of cardiac injury.
INTRODUCTION IN this age of high speed travel, cardiac injury, due to non-penetrating chest and abdominal trauma, is recognized with greater frequency. With the increasing severity of blunt chest injuries, especially from steering wheels, cardiac involvement may occur in 15-76 per cent of accident victims (Leinoff, 1940; Sigler, 1942; Watson and Bartholomae, 1960; Jones et al., 1975). Although cardiac contusion is not usually fatal, it may be accompanied by life-endangering complications (Liedtke and DeMuth, 1973). Cardiac contusion may initially be unrecognized and become obvious only when serious cardiac malfunction is detected. Furthermore, its symp- toms are often overshadowed by the more obvious effects of associated cerebral, pulmon- ary, abdominal and musculoskeletal injuries (Blair et al., 197 1).
Records of 20 patients treated between 1975 and 1978 at the Hadassah University Hospital,
Jerusalem, for multiple injuries with con- comitant myocardial contusion, were reviewed (Table I). The presented cases demonstrate some of the diagnostic and therapeutic difft- culties concerning this clinical entity.
CASE REPORTS
Case 1 A 20-year-old man was injured in a road acident. On admission, he had mild dyspnoea. His blood pressure was 1 IO/70 mmHg and his pulse rate 120 per minute and regular. Both sides of the upper part of the chest had been injured. Chest radiographs revealed fractures of the ribs on both sides and a let? pneumothorax. The left side of the chest was drained by an intercostal tube and a water-seal bottle system. A few hours later, a right pneumothorax was found and drained as above. The serum transaminase was elevated. The ECG showed inverted T-waves and mild S-T elevations in the inferolateral wall leads. Two days later, there were still residual inverted T-waves in L,-AVF. After three years, the patient is asymptomatic and the ECG is normal. This patient had a minor. reversible cardiac injury.
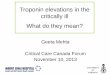
Case 2 A 66-year-old woman was hit by a bus while crossing the road. Her past history revealed mild hypertension, untreated, and chronic lung disease. On admission her blood pressure was 170/100 mmHg, and pulse rate 112 per minute with multiple ventricular premature contractions. The left hemithorax, neck and face were suffused by haematoma. The patient complained of persistent pain in the left sides of the chest and upper abdomen. Chest radiographs showed no abnormality. The serum enzymes were elevated and the ECG showed multiple ventricular premature contractions with diffuse ST-T changes (Fig. I). The VPCs were

Katz et al.: Cardiac Contusion 181
controlled by intravenous administration of procaina- mide (Pronestyl) 1 mg/kg followed by a maintenance dose of Pronestyl and a week of oral quinidine sulphate.
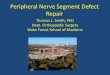
On the third day, in view of the persistent tachy- cardia and the left upper abdominal tenderness, peritoneal puncture was performed. A small amount of bloody fluid was aspirated. Explorative laparotomy revealed a small tear in the spleen which was removed. The postoperative course was uneventful. The ECG on the seventh day was normal (Fig. 2). On follow-up, the patient is completely asymptomatic.
Different types of arrhythmias may occur with cardiac contusion.
Case 3 A 69-year-old woman was hit by a car. On admission her blood pressure was 170/70 mmHg, and pulse rate 96 per minute and regular. Examination revealed fractures of the ribs, both limbs and pubis. A right pneumothorax was drained by intercostal tube and an under water-seal. The ECG on admission was normal. The next day, while being observed in the Respiratory Intensive Care Unit, a 4-minute episode of tachycardia of 200 per minute occurred. Serial ECGs after this episode showed elevation of the ST segment in leads III and AVF, with depression in V,-V,; these changes gradually reverted to normal. Three weeks later Q waves appeared in the inferior leads. One year later the
Table/. Details of 20 patients with multiple injuries and concomitant myocardial contusion
Patient Age (yr) Sex
Concomitant injuries ECG Follow-up
1 20
2
3
4
5 36
66
69
19
6 75
7 21
8 32
9 21
Fracture of ribs Lt pneumothorax Rt pneumothorax Contusion of
shoulder Face, neck and
chest haematoma Tear in spleen Laceration of face Fracture of ribs Fracture of lower limb Fracture of pubis Rt pneumothorax Fracture of sternum Fracture of ribs Lt pneumothorax Tear innominate artery Haemopericardium Laceration of face Fracture of acetabulum
Fracture of ribs Lt pneumothorax Head injury Fracture of humerus Fracture of clavicle Superior vena cava
syndrome Contusion of lung Laceration of face Widening of mediastinum Normal aortogram Laceration of scalp Rt pneumothorax Fracture of ribs Fracture of lumbar process Haematuria
ST-T changes 3 yr lnferolateral Asymptomatic
Multiple VPCs ST changes
Sinus tachycardia ST-T changes 0 wave AC. Ml
Diffuse ST-T changes
Transient A-V block
Diaphragmatic Ml
Sinus tachycardia T-changes
Rt axis dev.
PVCS
T-changes
VI -V,
2 yr Asymptomatic Normal ECG
1 yr Asymptomatic 0 wave Old Ml
2 yr Asymptomatic Normal ECG
3 mth Chest pain Asynergy of It
ventricle 2 yr intermittent
chest pain 0 - L3, AVF
2 yr Normal ECG
2 yr Asymptomatic Lt ant. hemiblock
2 yr Asymptomatic Normal ECG
2 yr Asymptomatic Normal ECG

182
Table I. (contd)
Injury: the British Journal of Accident Surgery Vol. 1 ~/NO. 3
Patient Age Concomitant (yrj Sex injuries ECG Follow-up
10 27
11 17
12 46
13 42
14 32
15 18.5
16 15
17 36
18 42
19
20
47
30
F
M
M
M
M
M
M
M
M
F
M
Fracture of skull Lt pneumothorax Fracture of femur
Fracture -dislocation L, Fracture of calcaneus Fracture of tibia and fibuia Haematuria Fracture of sternum
Head injury Haematuria
Fracture of skull Contusion of lung Fracture of humerus
Fracture of mandible Loss of consciousness
Lung contusion Haematoma of chest
wall Fracture of ribs Haematuria
Fracture of ribs Haematuria
D, - D,, Fracture of femur
Fracture of nose Laceration of face Fracture of pelvis Haematuria
ST-T changes
Multiple VPCs
T-changes
V,-Vs Multiple VPCs
ST-T changes
Rt B8B
ST-T changes Inferior wall
T-changes Inferior wall
PVCs resolved
Atrial fibrillation Diffuse T-changes
ST-T changes VPCS
Died 20 h after admission
Brain stem injury
1 yr Asymptomatic Normal ECG
3 yr Asymptomatic
3 yr Asymptomatic Normal ECG Died, 36 h
after admission Brain stem
injury 3yr. Asymptomatic Rt BBB
resolved
3 v Asymptomatic Normal ECG
2 yr Asymptomatic Q - L3. AVF 2yr Asymptomatic Normal ECG
3 yr Asymptomatic Normal ECG
1 yr Asymptomatic Normal ECG
patient is completely asymptomatic and the ECG shows an old inferior infarction.
Strict monitoring of the patient with multiple injuries is necessary for diagnosis of delayed appear- ance of cardiac complications.
Case 4 A 19-year-old man was involved in a road accident. On admission his blood pressure was 100/70 mmHg, and pulse rate 120 per minute. There were signs of injury in the left side of his chest. Chest radiographs revealed fractures of the sternum and 1st to 4th left ribs, a lefi pneumothorax and widening of the mediastinal shadow. Aortography demonstrated an extravasation ofcontrast medium from the innominate artery. Coeliac angiography suggested intracapsular
haematoma of the spleen. The ECG showed transient 1st degree A-V block and mild ST elevation and T-wave changes. Median stemotomy revealed a haemopericardium, contusion of the right coronary artery and a tear with a wide pulsating haematoma of the innominate artery. The innominate artery was replaced by an &mm Dacron graft. Exploratory laparotomy was negative. The ECG showed gradual resolution of the ST changes. The patient was dis- charged two weeks later with a normal ECG. After two years, the patient is asymptomatic and the ECG is normal.
This case represents one of the combined thoracic and cardiac injuries which necessitated operation.
Case 5 A healthy 36-year-old man sustained a steering wheel

Katz et al.: Cardiac Contusion 183
Fig. 1. Electrocardiogram of Case 2 on admission: sinus tachycardia, ventricular premature contractions with ST-T changes.
Fig. 2. Electrocardiogram of Case 2 on the seventh day following injury: normal sinus rhythm, with no signs of ischaemia.
injury. On admission, his blood pressure was 160/100 mmHg, his pulse rate 120 per minute and regular. There were signs of injury to the right side of the chest but no fracture. Chest radiographs showed a normal cardiothoracic ratio. There were small bi- lateral pleural effusions with no fracture of sternum or ribs. Pelvic radiography revealed a chip fracture of the acetabulum. The SGOT was 1480 units (n=50), LDH 650 units (n=200) and CPK 88 units (n=7). These values gradually returned to normal during the subsequent week. The ECG showed inferior and
anterior ST-T wave changes. Serial ECG recordings revealed the typical evolution pattern of acute infarc- tion. His convalescence was uneventful apart from complaints of recurrent pain in the chest without electrocardiographic or biochemical evidence of extension of the myocardial damage. These symptoms disappeared and he was discharged 25 days later.
After four months, he was readmitted because of persistent complaints of weakness on exertion, with episodes of palpitations. Physical examination and laboratory findings were normal. The ECG showed an

184 Injury: the British Journal of Accident Surgery Vol. 1 Z/No. 3
Fig. 3. Electrocardiogram of Case 6 on admission: sinus tachycardia diffuse ST-T changes in the infero- lateral leads.
Fig. 4. Electrocardiogram of Case 6 performed a year later: within normal limits.
old inferior infarction with normal ST segments and T-waves. Exercise testing did not show myocardial ischaemia. Cardiac catheterization was performed. The left ventricular pressure was 115/2-l 5 mmHg and the end diastolic pressure increased to 24 mmHg after angiography. LetI ventriculography showed a slightly enlarged left ventricle with asynergy of the inferior wall involving 20 per cent of the left ventricular circumference. The ejection fraction was 56 per cent. Selective coronary cineangiography showed com- pletely normal major coronary arteries. An ECG
performed one year later showed an old inferior infarc- tion. The patient still complains of intermittent chest pain.
A transient injury to a coronary artery is one of the suggested mechanisms causing ischaemic myocardial damage and later formation of ventricular aneurysm. This patient had mild myocardial dysfunction, a sequel of cardiac injury.
Case 6 A 75-year-old man was hit by a car. On admission his

Katz et al.: Cardiac Contusion 185
Table I!. Mechanism of injury in 20 patients with Tab/e l/1. Associated injuries in 20 patients with cardiac contusion cardiac contusion
Mechanism of injury No. Injury No.
Automobile accident 12 Pedestrian accident 6 Other 2 Total 20
Chest Fracture of rib Fracture of sternum Fracture of clavicle Mediastinum: great
7 2 1
Male = 15, female = 5. Mean age = 35.6 k 17.8 years.
blood pressure was 120/80 mmHg, and his pulse rate was 72 per minute and regular. He had mild dyspnoea and tenderness over the left chest wall. Chest radio- graphs revealed fractures in the 3rd to 6th ribs with some subcutaneous emphysema. A few hours later, a left pneumothorax was found and drained. The ECG showed T-wave changes in the diaphragmatic and lateral wall (Fig. 3). Blood enzymes were slightly elevated. The patient was discharged a week later. The ECG findings were related to long standing ischaemic heart disease. A year later the patient was admitted for elective ooeration. The ECG then showed no sinns of
vessel injuries 2 Contusion of lung 3 Haemopneumothorax 6
Total 21
Other Fracture of spleen Head injury Haematuria Fracture of pelvis Fracture of long bone Fracture of spine Fracture of face
Total
:
: 6 3 6
30
ischaemia(Fig. 4). In the aged patient, the ECG fmdings of cardiac
Tab/e IV. ECG changes in 20 patients with cardiac
trauma are sometimes erroneously related to the basic contusion
ischaemic heart disease and the diagnosis of cardiac contusion is missed. ECG changes No.
DISCUSSION The heart is related to the anterior chest wall, the thoracic vertebrae and the great vessels. The possibility of cardiac injury should be suspected in all patients who have thoracic and abdominal injuries, especially those involved in automobile accidents. The various means of injury, acceleration/deceleration, compression and incrensed intra-abdominal or intra-thoracic pressure, explain the occurrence of cardiac injury among patients with multiple injuries (Jones et al., 1975). It should be emphasized that the diagnosis of myocardial contusion is fre- quently missed or delayed, as attention is mainly directed toward other severe injuries (Blair et al., 197 1). In our series of 20 patients with multiple injuries (Table II), there was an average of 2.5 associated extracardiac injuries per patient (Table III).
Fracture of the rib, haemopneumothorax and contusion of the lung are the most common thoracic injuries. Facial and head injuries, fractures of long bones and haematuria are the main associated non-thoracic injuries (Table IZl). The clinical and laboratory features of
lschaemic pattern (ST-T changes, Q wave)
Tachycardia (over 1 OO/min)
VPC Conduction disturbance
14
5 6 3
cardiac contusion are similar to those of myo- cardial infarction. Pain in the chest, dyspnoea and tachycardia following cardiac contusion are indistinguishable from those occurring in multiple injury. The paucity of characteristic physical findings establishes the electrocardio- graph as the most reliable diagnostic tool (Liedtke and DeMuth, 1973). Serial ECG trac- ing with dynamic S-T changes, transient arrhythmias and disturbances of conduction support the diagnosis of cardiac contusion (Table IL’). Repeated determination of serum enzymes, CPK, LDH, SGOT are of little diagnostic value because of associated soft tissue injury. The MB-CPK iso-enzyme was not identified in any patient in our series. Tech- necium scan of the heart is still unreliable (Brantigan et al., 1978). Coronary angiography

186
and ventriculography (Case 5) demonstrated dyskinesia of the diaphragmatic wall of the left ventricle with patent coronary arteries, thus providing some diagnostic and prognostic information concerning the significance of traumatic myocardial injury (Katz et al., 1979).
The care of a patient with cardiac contusion includes prompt evaluation and treatment of the concomitant injuries, strict monitoring and immediate treatment of the specific cardiac complications including any arrhythmia, congestive heart failure and conduction distur- bance. When acute surgical conditions such as ventricular septal defect, valvular damage and dysfunction or coronary artery occlusion cause significant deterioration of the cardiac state, a life-saving operation is required. These patients should be carefully followed since a delayed complication like an aneurysm of the left ventricle may appear months or years later (Doty et al., 1974)
Increased awareness and understanding of this kind of injury and better diagnostic methods should eliminate much of the confusion con- cerning this clinical entity and should result in its being more frequently diagnosed. Extensive use of cardiac monitoring, ECG radiography of the chest, cardiac output and cardiac catheteriz- ation will not only increase the frequency of
Injury: the British Journal of Accident Surgery Vol. 1 ~/NO. 3
diagnosis, but should reduce the serious and even fatal complications of cardiac injuries in the patient with multiple injuries.
REFERENCES Blair E., Topuzlu C. and Davis J. H. (197 1) Delayed or
missed diagnosis in blunt chest trauma. .I. Trauma 11,129.
Brantigan C. O., Burdick D., Hopeman A. R. et al. (1978) Evaluation of technetium scanning for myocardial contusion. J. Trauma 18,460.
Doty D. B., Anderson A. E., Rose E. F. et al. (1974) Cardiac trauma: clinical and experimental correla- tions of myocardial contusion. A&. Surg. 180,452.
Jones J. W.. Hewitt R. L. and Drananas T. (197% Cardiac cbntusion: a capricious Hyndrome.‘ Ann: Surg. 181,567.
Katz S., Gimmon (Goldschmidt) Z., Lewis B. S. et al. (1979) Coronary angiography after traumatic myo- cardial contusion. J. Trauma 19, 125.
Leinoff H. D. (1940) Direct nonpenetrating injuries of the heart. Ann. Intern. Med. 14,653.
Liedtke A. J. and DeMuth W. E. (1973) Non- penetrating cardiac injuries: a collective review. Am Heart J. 86,687.
Sigler L. H. (1942) Trauma of the heart due to nonpenetrating chest injuries. Report of cases with recovery or long survival. JAMA 114,855.
Watson J. H. and Bartholomae W. M. (1960) Cardiac injury due to nonpenetrating trauma. Ann. Intern. Med. 52,871.
Requests for reprints should be addressed to: Dr S. Katz, Department of Surgery, Hadassah Hospital, PO Box 12000, Jerusalem, Israel.