Embed Size (px)
Citation preview
166...Tm.CAADA MEIA Aso-To ORA Ag 193
drainage tube in his case. Cutler and Beck statethat drains may be placed in the wound to thepericardium but preferably 'not into it. Row-lands stresses the use of an exit tube whencarrying out irrigation either at operation orafterwards. Failure to guarantee exit for theirrigating fluid has possibly been responsible fordeath from compression of the heart (cardiactamponnade). Rowlands also advises posturaldrainage by having the patient lie on his facefor a short time at intervals throughout the day.Prognosis.-In untreated cases the prognosis
is invariably fatal. In pneumonia, with a dis-tending pericardium bounded by unyieldingsolid lung, death comes quickly, with symptomsof acute circulatory failure-possibly due tocardiac compression.One is impressed by the attitude of resigna-
tion associated with this condition as summedup in the term "terminal pericarditis", and evenby the tragically sincere advice against surgicalinterference. Such a hopeless outlook is inreality unwarranted. Truesdale"1 collected 152cases treated by pericardiotomy from the world'sliterature, with a recovery rate of 58 per centfor the entire series, and a steady lowering inmortality the more' recent the cases in surgicalhistory. The outlook for future cases- withmodern antibacterial agents and supportivemeasures should be still brighter.
CONCLUSIONSThe pnemonia patient worsening rapidly with
circulatory failure may have empyema- of thepericardium.
There is need of research in the diagnosis ofthis condition.
If diagnosed, pyogenic pericarditis is amen-able to surgical treatment, which, though it mustbe carried out on a seriously ill patient, offersa brightening prospect of complete and lastingcure.
My thanks are due to Dr. W. W. Francis, of theOsler Library, for supplying many references in theoriginal, to Sister Valere of the Ottawa General Hospital,to my colleagues at the Ottawa Civic Hospital who somagnanimously communicated helpful studies of fatalcases,to the records' staffs of the Ottawa Civic andOttawa General Hospitals, and to the photographic de-partment, Ottawa Civic Hospital.
REFERENCES1. BEHREND, M. AND BOLEs, R. S.: Indications for the
operations of cardiolysis, pericardiotomy and peri-cardiectomy, J. Am. M. A88., 1937, 108: 1941.
2. BIGGER, I. A.: Suppurative pericarditis. Report ofeight cases treated surgically, South. M. J., 1937,30: 164.
3. COTTAM, G4.: A case of suppurative pericarditis, J.Am. M. Ass., 1933, 100: 287.
4. Cours, J. A. AND ROWLANDS, R. P.: A case ofpurulent pericarditis associated with empyema in achild aged two and a half years, Brst. M. J., 1904,1: 9.
5. CUTLER, E. C. AND BECK, C. S.: Surgery of the Heartand Pericardium in Nelson's Loose Leaf Surgery,Nelson & Sons, Toronto.
6. HEEL: Acute suppurative pericarditis, Ain. Surg.,1936, 104: 365.
7. KENNON: Infective- osteomyelitis, Surg. Gyn. A Obst.,1928, 47: No. 1, 44.
8. OGLE, C. AND ALLINGHAM, H.: A suggestion for amethod of opening the pericardial sac founded upona case of purulent pericarditis, The La'ncet, 1904, 1:106.
9. OSLER, W. AND McCaAu, T.: The Principles and Prac-tice of Medicine, Appleton, 9th ed., p. 758.
10. THOMAs, T. M.: A case of purulent pericarditis fol-lowing acute osteomyelitis, Arch. of Di8. ip Child.,1929, 4: 67.
11. TRUESDALE, P. E.: Low pericardiotomy for acute peri-carditis: Report of two cases and twenty-four newcases from the literature, New Eng. J. Med., 1933,208: 671.
12. TWINING, E. W.: Tomography, by means of a simpleattachment to the Potter Bucky couch, Brit. J.Radiol., 1937, 10: 112.
13. WHEELER, D.: Personal communication.
SPONTANEOUS GASTRODUODENAL FISTULA*
(REVIEW OF THE LITERzATURE WrrH REPORT OF A CASE)
By Louis J. NOTKINMontreal
MODERN textbooks are silent on the subjectof gastroduodenal fistula since no cases ap-
peared in the literature between 1868 and 1926.Six cases were described between 1842 and 1868and only 12 cases have been reported as gastro-duodenal fistule since 1926 to date of writing.When one considers the extent to which
ulceration of the stomach, a relatively common
-condition, may distort the adjacent parts and
* From the Department of Medicine, Jewish GeneralHospital, Montreal.
the frequency of chronic perforation in pepticulcer, it is surprising that so, few cases haveoccurred. It is very intriguing to speculate onthe reasons for the complete absence of suchcases between 1868 and 1926 and the apparentoccurrence of this condition within the last 93years in two periods separated by a free periodof 58 years. The question must remain unan-swered for the present.
CASE REPORTMr. J.T., office worker, aged 68, presented himself
for diagnosis and treatment on November 23, 1934. He
THE CANADIAN MEDIcALASSOCIATION JOURNAL166 [Aug. 1939
Aug. 1939] No.riu.: FISTUIA 1fi7
complained of abdominal pain of ten days ' duration,tarry stools and weakness for three days. He had beenin perfect health u:itil 20 years before, when he com-plained of symptoms typical of peptic ulcer, with hemna-temesis and melbna, for which he received adequatetreatment. About a year later the symptoms recurredand lasted a few months. Since then he had been welluntil 10 days prior to admission, when he began to com-plain of upper abdo cramp-like pains, coming on2% to 3 hours after meals, associated with belching, andrelieved by food. For three days prior to admission thepain was almost constant and most marked in the leftupper quadrant. The appetite was good. There was nonausea or vomiting. The bowels had always been regu-lar. There were no symptoms referable to other systems.He sought-admission because of progressive weakness.
Personal history.-The patient had had typhoid inhis youth. His habits were good.
Family history.-Irrelevant.-Physical examinatison. - Well-nourished and well-
developed. The chest was long and narrow; the lungsnormal. The heart was not enlarged. A long, harshsystolie murmur could be heard at all orifices, particularlywell at the apex. The pulse rate was 75 and the rhythmnormaL Blood pressure 140/70. The abdomen was softand nowhere tender; no masses or organs were palpable.The rectal examination was negative.
Urine: acid; specific gravity, 1.014; albumin, 0;glucose, 0; microscopically, occasional pus cells. Redblood cells, 3,600,000; white- blood cells, 10,200; Hgb.,62 per cent. Ewald test meal determinations were con-tinued for 1 hour at 15 minute intervals. Free RCI waspresent in the- fasting contents; both free and total acidvalues did not exceed 10 in all specimens. All stoolswere strongly positive for occult blood. The bloodWasermann was negative.
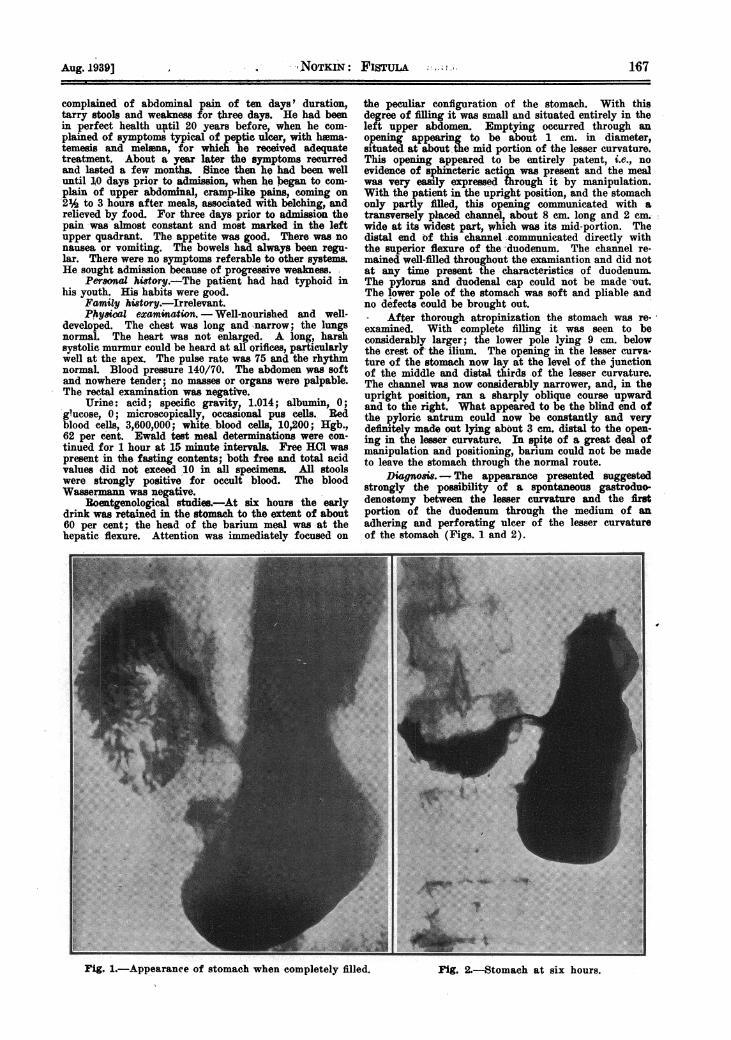
Roentgenological studies.-At six hours the earlydrink was retained in the stomach to the extent of about60 per cent; the head of the barium meal was at thehepatic flexure. Attention was immediately focused on
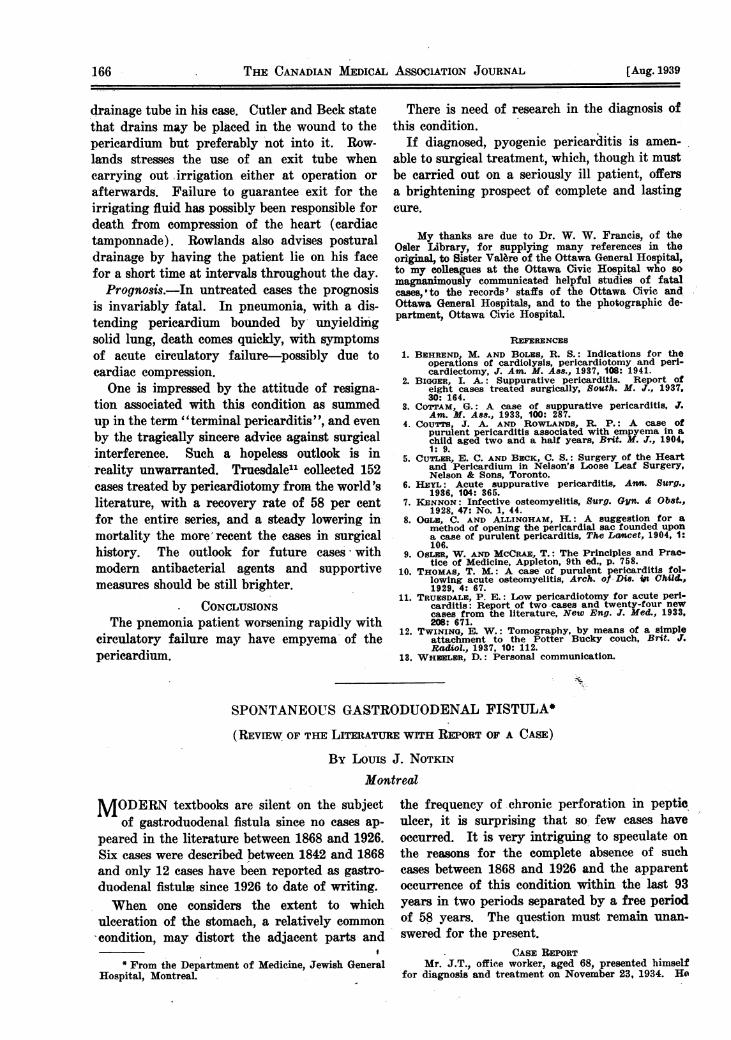
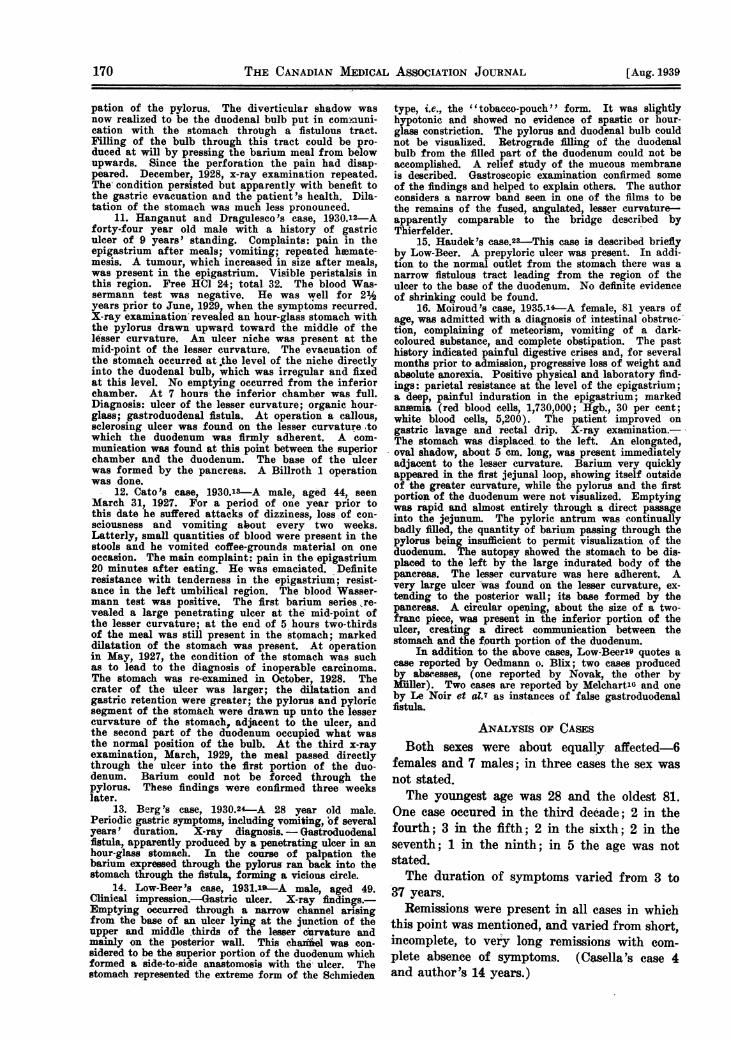
the peculiar configuration of the stomach. With thisdegree of filling it was small and situated entirely in theleft upper abdomen Emptying oecurred through anopening appearing to be about 1 cm. in diameter,situated at about,the mid portion of the lesser curvature.This opening appeared to be entirely patent, i.e., noevidence of sphincteric actiqn was present and the mealwas very easly ereed lrough it by manipulation.With the patient in the upright position, and the stomachonly partly filled, this opening communicated with atransversely placed channel, about 8 cm. long and 2 cm.wide at its widest part, which was its mid-portion. Thedistal end of this channel -communicated directly withthe superior fiexure of the 'duodenum. The channel re-mained well-filled throughout the examiantion and did notat any time present the characteristics of duodenum.The pylorus and duodenal cap could not be made -out.The lower pole of the stomach was soft and pliable andno defects could be brought out.
After thorough atropinization the stomach was re-examined. With complete filling it was seen to beconsiderably larger; the lower pole lying 9 cm. belowthe crest of the ilium. The opening in the lesser curva-ture of the stomach now lay at the level of the junctionof the middle and distal thirds of the lesser curvature.The channel was now considerably narrower, and, in theupright position, ran a sharply oblique course upwardand to the right. What appeared to be the blind end o'fthe pyloric antrum could now be constantly and verydefinitely made out lying about 3 cm. distal to the open-ing in the lesser curvature. In spite of a great deal ofmanipulation and positioning, barium could not be madeto leave the stomach through the normal route.
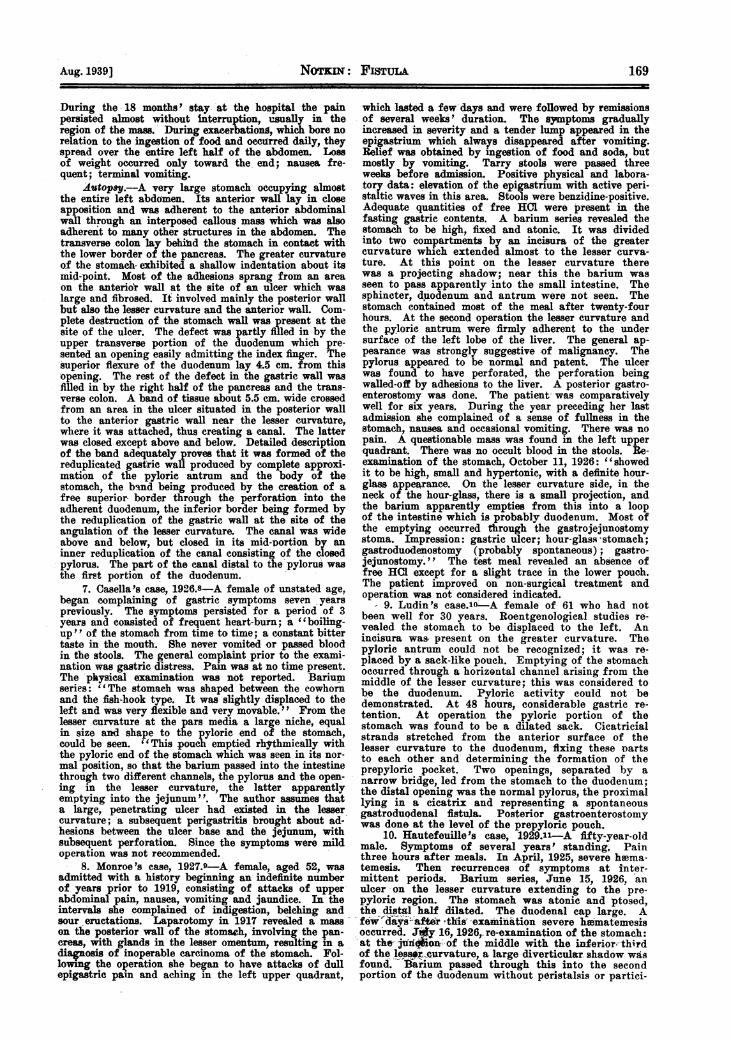
Diagno&s .- The appearance presented suggestedstrongly the possibility of a spontaneous gastroduo-denostomy between the lesser curvature and the firstportion of the duodenum through the medium of anadhering and perforating ulcer of the lesser curvatureof the stomach (Figs. 1 and 2).
Fig. 1.-Appearance of stomach when completely filled.
CM.
*:
:...::::
:e.:
.:
::.:
-- :-
:-
Aug. 1939] -,NOTKIN: FisTuiA :: -, 1-67
IlFig. 2.-Stomach at six hours.
16 Tl CAADA MEIA ASOITO JORA [Ag 1939
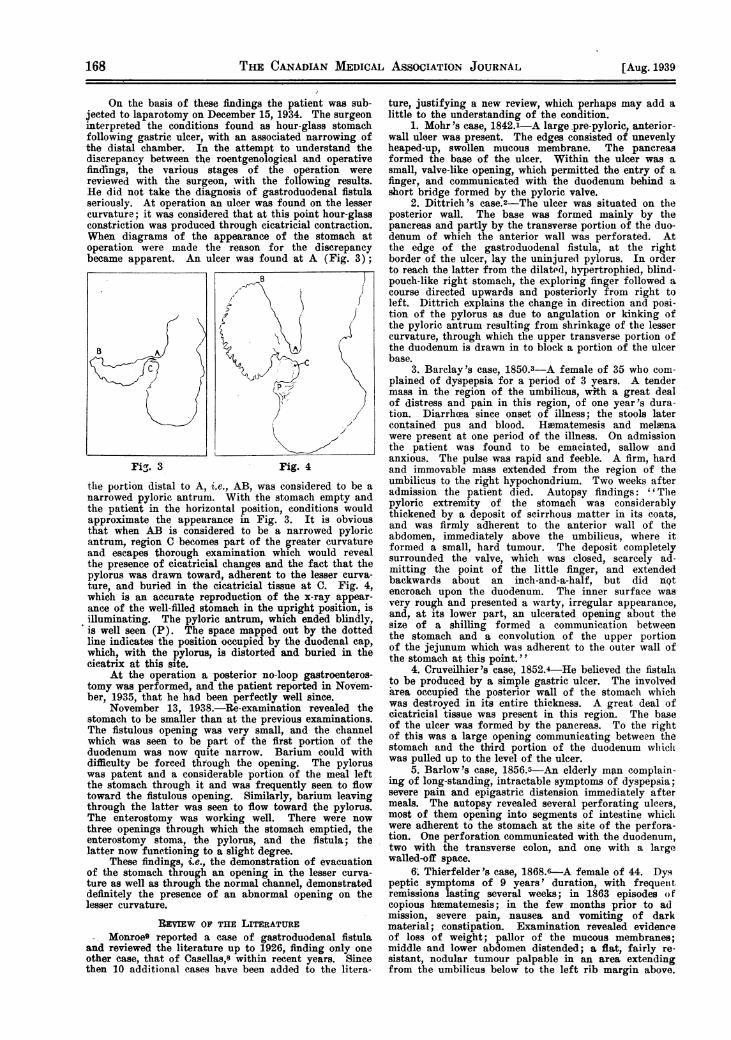
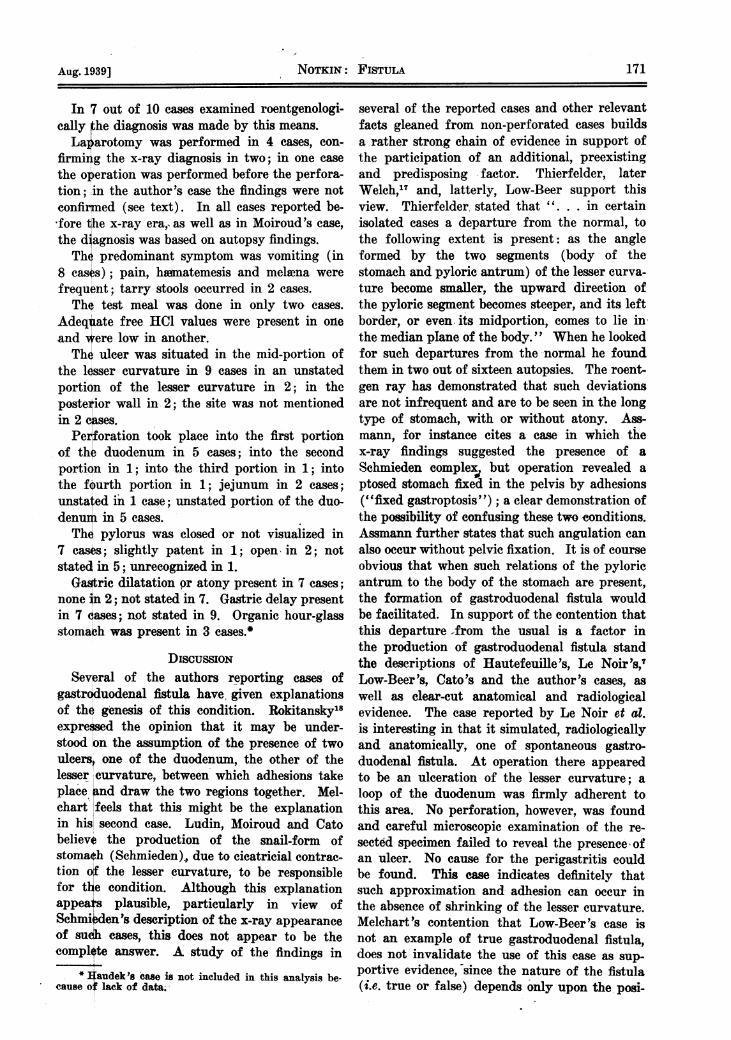
On the basis of these findings the patient was sub-jected to laparotomy on December 15, 1934. The surgeoninterpreted the conditions found as hour-glass stomachfollowing gastric ulcer, with an associated narrowing ofthe distal chamber. In the attempt to understand thediscrepancy between the roentgenological and operativefindings, the various stages of the operation werereviewed with the surgeon, with the following results.He did not take the diagnosis of gastroduodenal fistulaseriously. At operation an ulcer was found on the lessercurvature; it was considered that at this point hour-glassconstriction was produced through cicatricial contraction.WVhen diagrams of the appearance of the stomach atoperation were made the reason for the discrepancybecame apparent. An ulcer was found at A (Fig. 3);
Fia. 3 Fig. 4
the portion distal to A, i.e., AB, was considered to be anarrowed pyloric antrum. With the stomach empty andthe patient in the horizontal position, conditions wouldapproximate the appearance in Fig. 3. It is obviousthat when AB is considered to be a narrowed pyloricantrum, region C becomes part of the greater curvatureand escapes thorough examination which would revealthe presence of cicatricial changes and the fact that thepylorus was drawn toward, adherent to the lesser curva-ture, and buried in the cicatricial tissue at C. Fig. 4,which is an accurate reproduction of the x-ray appear-ance of the well-filled stomach in the upright position, isilluminating. The pyloric antrum, which ended blindly,is well seen (P). The space mapped out by the dottedline indicates the position occupied by the duodenal cap,which, with the pylorus, is distorted and buried in thecicatrix at this site.
At the operation a posterior no-loop gastroenteros-tomy was performed, and the patient reported in Novem-ber, 1935, that he had been perfectly well since.
November 13, 1938.-Re-examination revealed thestomach to be smaller than at the previous examinations.The fistulous opening was very small, and the channelwhich was seen to be part of the first portion of theduodenum was now quite narrow. Barium could withdifficulty be forced through the opening. The pyloruswas patent and a considerable portion of the meal leftthe stomach through it and was frequently seen to flowtoward the fistulous opening. Similarly, barium leavingthrough the latter was seen to flow toward the pylorus.The enterostomy was working well. There were nowthree openings through which the stomach emptied, theenterostomy stoma, the pylorus, and the fistula; thelatter now functioning to a slight degree.
These findings, i.e., the demonstration of evacuationof the stomach through an opening in the lesser curva-ture as well as through the normal channel, demonstrateddefinitely the presence of an abnormal opening on thelesser curvature.
REVIEW OF THE LITERATUREMonroe9 reported a case of gastroduodenal fistula
and reviewed the literature up to 1926, finding only oneother case, that of Casellas,8 within recent years. Sincethen 10 additional cases have been added to the litera-
ture, justifying a new review, which perhaps may add alittle to the understanding of the condition.
1. Mohr 's case, 1842.1-A large pre-pyloric, anterior-wall uleer was present. The edges consisted of unevenlyheaped-up, swollen mucous membrane. The pancreasformed the base of the ulcer. Within the ulcer was asmall, valve-like opening, which permitted the entry of afinger, and communicated with the duodenum behind ashort bridge formed by the pyloric valve.
2. Dittrich's case.2-The ulcer was situated on theposterior wall. The base was formed mainly by thepancreas and partly by the transverse portion of the duo-denum of which the anterior wall was perforated. Atthe edge of the gastroduodenal fistula, at the rightborder of the ulcer, lay the -uninjured pylorus. In orderto reach the latter from the dilated, hypertrophied, blind-pouch-like right stomach, the exploring finger followed acourse directed upwards and posteriorly from right toleft. Dittrich explains the change in direction and posi-tion of the pylorus as due to angulation or kinking ofthe pyloric antrum resulting from shrinkage of the lessercurvature, through which the upper transverse portion ofthe duodenum is drawn in to block a portion of the ulcerbase.
3. Barclay 's case, 1850.3-A female of 35 who com-plained of dyspepsia for a period of 3 years. A tendermass in the region of the umbilicus, with a great dealof distress and pain in this region, of one year's dura-tion. Diarrhoea since onset of illness; the stools latercontained pus and blood. Haematemesis and melwnawere present at one period of the illness. On admissionthe patient was found to be emaciated, sallow andanxious. The pulse was rapid and feeble. A firm, hardand immovable mass extended from the region of theumbilicus to the right hypochondrium. Two weeks afteradmission the patient died. Autopsy findings: "Tlhepyloric extremity of the stomach was considerablythickened by a deposit of scirrhous matter in its coats,and was firmly adherent to the anterior wall of theabdomen, immediately above the umbilicus, where itformed a small, hard tumour. The deposit completelysurrounded the valve, which was closed, scarcely ad-mitting the point of the little finger, and extendedbackwards about an inch-and-a-half, but did nQtencroach upon the duodenum. The inner surface wasvery rough and presented a warty, irregular appearance,and, at its lower part, an ulcerated opening about thesize of a shilling formed a communication betweenthe stomach and a convolution of the upper portionof the jejunum which was adherent to the outer wall ofthe stomach at this point. "
4. Cruveilhier 's case, 1852.4-He believed the fistulato be produced by a simple gastric ulcer. The involvedarea occupied the posterior wall of the stomach whichwas destroyed in its entire thickness. A great deal ofcicatricial tissue was present in this region. The baseof the ulcer was formed by the pancreas. To the rightof this was a large opening communicating between thestomach and the third portion of the duodenum wlhiciwas pulled up to the level of the ulcer.
5. Barlow's case, 1856.5-An elderly man complain-ing of long-standing, intractable symptoms of dyspepsia;severe pain and epigastric distension immediately aftermeals. The autopsy revealed several perforating ulcers,most of them opening into segments of intestine whichwere adherent to the stomach at the site of the perfora-tion. One perforation communicated with the duodenum,two with the transverse colon, and one with a largewalled-off space.
6. Thierfelder's case, 1868.6-A female of 44. Dyspeptic symptoms of 9 years' duration, with frequezi tremissions lasting several weeks; in 1863 episodes ofcopious haematemesis; in the few months prior to admission, severe pain, nausea and vomiting of darkmaterial; constipation. Examination revealed evidenceof loss of weight; pallor of the mucous membranes;middle and lower abdomen distended; a flat, fairly re-sistant, nodular tumour palpable in an area extendingfrom the umbilicus below to the left rib margin above.
THF, CANADUN MEDIcALAssocIATION JOURNAL168 [Aug. 1939
Aug.19391 NoTKIN: FISTULA 169
During the 18 mouths' stay -at the hospital the painpersisted almost without interruption, wusally in theregion of the mass.' During exacerbationg, which bore norelation to the ingestion of food and occurred daily, theyspread over the entire left half of the abdomen. Losof weight occurred only toward the. end; nausea fre-quent; terminal vomiting.
Autopsy.-A very large stomach occupying almostthe entire left abdomen. Its anterior wall lay in closeapposition and was adherent to the anterior abdominalwall through an interposed callous mass which was alsoadherent to many other structures in the abdomen. Thetransverse colon lay behiad the stomach in contact withthe lower border of the pancreas. The greater curvatureof the stomach exhibited a shallow indentation about itsmid-point. Most of the adhesions sprang from an areaon the anterior wall at the site of an ulcer which waslarge and fibrosed. It involved mainly the posterior wallbut also the lesser curvature and the anterior wall. Com-plete destruction of the stomach wall was present at thesite of the ulcer. The defect was partly filled in by theupper transverse portion of the duodenum which pre-sented an opening easily admitting the index finger. Thesuperior flexure of the duodenum lay 4.5 cm. from thisopening. The rest of the defect in the gastric wall wasfilled in by the right half of the pancreas and the trans-verse colon. A band of tissue about 5.5 cm. wide crossedfrom an area in the ulcer situated in the posterior wallto the anterior gastric wall near the lesser curvature,where it was attached, thus creating a canal. The latterwas closed except above and below. Detailed descriptionof the band adequately proves that it was formed of thereduplicated gastric wall produced by complete approxi-mation of the pyloric antrum and the body of thestomach, the band being produced by the creation of afree superior border through the perforation into theadherent duodenum, the inferior border being formed bythe reduplication of the gastric wall at the site of theangulation of the lesser curvature. The canal was wideabove and below, but closed in its mid-portion by aninner reduplication of the canal consisting of the closedpylorus. The part of the canal distal to tie pylorus wasthe first portion of the duodenum.
7. Casella's case, 1926.8-A female of unstated age,began complaining of gastric symptoms seven yearspreviously. The symptoms persisted for a period of 3years and consisted of frequent heart-burn; a "boiling-up" of the stomach from time to time; a constant bittertaste in the mouth. She never vomited or passed bloodin the stools. The general complaint prior to the exami-nation was gastric distress. Pain was at no time present.The physical examination was not reported. Bariumseries: "The stomach was shaped between the cowhornand the fish-hook type. It was slightly displaced to theleft and was very flexible and very movable. " From thelesser curvature at the pars media a large niche, equalin size and shape to the pyloric end of the stomach,could be seen. "This .pouch emptied rhythmically withthe pyloric end of the stomach which was seen in its nor-mal position, so that the barium passed into the intestinethrough two different channels, the pylorus and the open-ing in the lesser curvature, the latter apparentlyemptying into the jejunum". The author assumes thata large, penetrating ulcer had existed in the lessercurvature; a subsequent perigastritis brought about ad-hesions between the ulcer base and the jejunum, withsubsequent perforation. Since the symptoms were mildoperation was not recommended.
8. Monroe 's case, 1927.9-A female, aged 52, wasadmitted with a history beginning an indefinite numberof years prior to 1919, consisting of attacks of upperabdominal pain, nausea, vomiting and jaundice. In theintervals she complained of indigestion, belching andsour eructations. Laparotomy in 1917 revealed a masson the posterior wall of the stomach, involving the pan-creas, with glands in the lesser omentum, resulting in adiajuosis of inoperable carcinoma of the stomach. Fol-lowmg the operation she began to have attacks of dullepigastric pam and aching in the left upper quadrant,
which lasted a few days and were followed by remissionsof several weekg ' duration. The symptoms graduallyincreased in severity and a tender lump appeared in theepigastrium- which always disappeared after vomiting.Belief was obtained by ingestion of food and soda, butmostly by vomiting. Tarry stools were passed threeweeks before admission. Positive physical and labora-tory data: elevation of the epigastrium with active peri-staltic waves in this area. Stools were benzidine-positive.Adequate quantities of free Hal were present in thefasting gastric contents. A barium series revealed thestomach to be high, fixed and atonic. It was dividedinto two compartments by an incisura of the greatercurvature which extended almost to the lesser curva-ture. At this point on the lesser curvature therewas a projecting shadow; near this the barium wasseen to pass apparently into the small intestine. Thesphincter, duodenum and antrum were not seen. Thestomach contained most of the meal after twenty-fourhours. At the second operation the lesser curvature andthe pyloric antrum were firmly adherent to the undersurface of the left lobe of the liver. The general ap-pearance was strongly suggestive of malignancy. Thepylorus appeared to be normal and patent. The ulcerwas found to have perforated, the perforation beingwalled-off by adhesions to the liver. A posterior gastro-enterostomy was done. The patient was comparativelywell for six years. During the year preceding her lastadmission she complained of a sense of fullness in thestomach, nausea and occasional vomiting. There was nopain. A questionable mass was found in the left upperquadrant. There was no occult blood in the stools. Re-examination of the stomach, Oetober 11, 1926: "showedit to be high, small and hypertonic, with a definite hour-glass appearance. On the lesser curvature side, in theneck of the hour-glass, there is a small projection, andthe barium apparently empties from this into a loopof the intestine which is probably duodenum. Most ofthe emptying occurred through the gastrojejunostomystoma. Impression: gastric ulcer; hour-glass stomach;gastroduodenostomy (probably spontaneous); gastro-jejunostomy." The test meal revealed an absence offree HCL except for a slight trace in the lower pouch.The patient improved on non-surgical treatment andoperation was not considered indicated.
9. Ludin 's case.1o-A female of 61 who had notbeen well for 30 years. Roentgenological studies re-vealed the stomach to be displaced to the left. Anincisura was present on the greater curvature. Thepylorie antrum could not be recognized; it was re-placed by a sack-like pouch. Emptying of the stomachocaurred through a horizontal channel arising from themiddle of the lesser curvature; this was considered tobe the duodenum. Pyloric activity could not bedemonstrated. At 48 hours, considerable gastric re-tention. At operation the pyloric portion of thestomach was found to be a dilated sack. Cicatricialstrands stretched from the anterior surface of thelesser curvature to the duodenum, fixing these partsto each other and determining the formation of theprepyloric pocket. Two openings, separated by anarrow bridge, led from the stomach to the duodenum;the distal opening was the normal pylorus, the proximallying in a cicatrix and representing a spontaneousgastroduQdenal fistula. Posterior gastroenterostomywas done at the level of the prepyloric pouch.
10. Hautefeuille's case, 1929.11-A fifty-year-oldmale. Symptoms of several years' standing. Painthree hours after meals. In April, 1925, severe hwma-temesis. Then recurrences of symptoms at inter-mittent periods. Barium series, June 15, 1926, anulcer on the lesser curvature extending to the pre-pyloric region. The stomach was atonic and ptosed,the distal half dilated. The duodenal cap large. Afewdaysfart -this" examination severe hematemesisoccurred. JFty 16, 1926,. re-examination of the stomach:at the-jViAeqn _of the middle with the inferiior;-thirdof the lesr curvature, a large diverticular shadow wasfound. l-3nrium passed through this into the secondportion of the duodenum without peristalsis or partici-
Aug. 1939] NoTKnq: FisTLTiA 169
17 H AAINMDCA SOITO ORA [Aug. 1939
pation of the pylorus. The diverticular shadow wasnow realized to be the duodenal bulb put in com-auni-cation with the stomach throtigh a fistulous tract.Filling of the bulb through this tract could be pro-duced at will by pressing the barium meal from belowupwards. Since the perforation the pain had disap-peared. December, 1928, x-ray examination repeated.The condition persisted but apparently with benefit tothe gastric evacuation and the patient's health. Dila-tation of the stomach was much less pronounced.
11. Hanganut and Dragulesco 's case, 1930.12-Aforty-four year old male with a history of gastriculcer of 9 years' standing. Complaints: pain in theepigastrium after meals; vomiting; repeated heamate-mesis. A tumour, which increased in size after meals,was present in the epigastrium. Visible peristalsis inthis region. Free HCI 24; total- 32. The blood Was-sermann test was negative. He was well for 2%years prior to June, 1929, when the symptoms recurred.X-ray examination' revealed an hour-glass stomach withthe pylorus drawn upward toward the middle of thelesser curvature. An ulcer niche was present at themid-point of the lesser curvature. The evacuation ofthe stomach occurred at the level of the niche directlyinto the duodenal bulb, which was irregular and fixedat this level. No emptying occurred from the inferiorchamber. At 7 hours- the inferior chamber was full.Diagnosis: ulcer of the lesser curvature; organic hour-glass; gastroduodenal fistula. At operation a callous,sclerosing ulcer was found on the lesser curvature towhich the duodenum was firmly adherent. A com-munication was found at this point between the superiorchamber and the duodenum. The base of the ulcerwas formed by the pancreas. A Billroth 1 operationwas done.
12. Cato's case, 1930.12-A male, aged 44, seenMarch 31, 1927. For a period of one year prior tothis date he suffered attacks of dizziness, loss of con-sciousness and vomiting about every two weeks.Latterly, small quantities of blood were present in thestools and he vomited coffee-grounds material on oneoccasion. The main complaint: pain in the epigastrium20 minutes after eating. He was emaciated. Definiteresistance with tenderness in the epigastrium; resist-ance in the left umbilical region. The blood Wasser-mann test was positive. The first barium series re-vealed a large penetrating ulcer at the mid-point ofthe lesser curvature; at the end of 5 hours two-thirdsof the meal was still present in the stomach; markeddilatation of the stomach was present. At operationin May, 1927, the condition of the stomach was suchas to lead to the diagnosis of inoperable carcinoma.The stomach was re-examined in October, 1928. Thecrater of the ulcer was larger; the dilatation andgastric retention were greater; the pylorus and pyloricsegment of the stomach were drawn up unto the lessercurvature of the stomach, adjacent to the ulcer, andthe second part of the duodenum occupied what wasthe normal position of the bulb. At the third x-rayexamination, March, 1929, the meal passed directlythrough the ulcer into the first portion of the duo-denum. Barium could not be forced through thepylorus. These findings were confirmed three weekslater.
13. Berg's case, 1930.24-A 28 year old male.Periodic gastric symptoms, including vomiting,of severalyears' duration. X-ray diagnosis.- Gastroduodenalfistula, apparently produced by a penetrating ulcer in anhour-glass stomach. In the course of palpation thebarium expressed through the pylorus ran back into thestomach through the fistula, forming a vicious circle.
14. Low-Beer's case, 1931.19L-A male, aged 49.Clinical impression.-Gastric ulcer. X-ray findings-Emptying occurred through a narrow channel arisingfrom the base of an ulcer lying at the junction of theupper and middle thirds of the lesser curvature andmainly on the posterior wall. This chaniiel was con-sidered to be the superior portion of the duodenum whichformed a side-to-side anastomosis with the' ulcer. Thestomach represented the extreme form of the Schmieden
type, i.e., the "tobacco-pouch" form. It was slightlyhypotonic and showed no evidence of spastic or hour-glass constriction. The pylorus and duodenal bulb couldnot be visualized. Retrograde filling of the duodenalbulb from the filled part of the duodenum could not beaccomplished. A relief study of the mucous membraneis described. Gastroscopic examination confirmed someof the findings and helped to explain others. The authorconsiders a narrow band seen in one of the films to bethe remains of the fused, angulated, lesser curvature-apparently comparable to the bridge described byThierfelder.
15. Haudek's case.23-This case is described brieflyby Low-Beer. A prepyloric ulcer was present. In addi-tion to the normal outlet from the stomach there was anarrow fistulous tract leading from the region of theulcer to the base of the duodenum. No definite evidenceof shrinking could be found.
16. Moiroud's case, 1935.14.-A female, 81 years ofage, was admitted with a diagnosis of intestinal obstruc--tion, complaining of meteorism, vomiting of a dark-coloured substance, and complete obstipation. The pasthistory indicated painful digestive crises and, for severalmonths prior to admission, progressive loss of weight andabsolute anorexia. Positive physical and laboratory find-ings: parietal resistance at the level of the epigastrium;a deep, painful induration in the epigastrium; markedaniemia (red blood cells, 1,730,000; Hgb., 30 per cent;white blood cells, 5,200). The patient improved ongastric lavage and rectal drip. X-ray examination.-The stomach was displaced to the left. An elongated,oval shadow, about 5 cm. long, was present immediatelyadjacent to the lesser curvature. Barium very quicklyappeared in the first jejunal loop, showing itself outsideof the greater curvature, while the pylorus and the firstportion of the duodenum were not visualized. Emptyingwas rapid and almost entirely through a direct passageinto the jejunum. The pyloric antrum was continuallybadly filled, the quantity of barium passing through thepylorus being insufficient to permit visualization of theduodenum. The autopsy showed the stomach to be dis-placed to the' left by the large indurated body of thepancreas. The lesser curvature was here adherent. Avery large ulcer was found on the lesser curvature, ex-tending to the posterior wall; its base formed by thepancreas. A circular opening, about the size of a two-franc piece, was present in the inferior portion of theulcer, creating a direct communication between thestomach and the fourth portion of the duodenum.
In addition to the above cases, Low-Beerl9 quotes acase reported by Oedmann o. Blix; two cases producedby abseesses, (one reported by Novak, the other byMuller). Two cases are reported by Melchartlo and oneby Le Noir et al.7 as instances of false gastroduodenalfistula.
ANALYSIS OF CASESBoth sexes were about equally affected-6
females and 7 males; in three cases the sex wasnot stated.The youngest age was 28 and the oldest 81.
One case occured in the third decade; 2 in thefourth; 3 in the fifth; 2 in the sixth; 2 in theseventh; 1 in the ninth; in 5 the age was notstated.The duration of symptoms varied from 3 to
37 years.Remissions were present in all cases in which
this point was mentioned, and varied from short,incomplete, to very long remissions with com-plete absence of symptoms. (Casella's case 4and author's 14 years.)
THE .CANADUN MEDicALAssocIATION JOURNAL170 [Aug. 1939
Au.13]NnN ITI 7
In 7 out of 10 cases examined roentgenologi-cally the diagnosis was made by this means.La arotomy was performed in 4 cases, con-
firmi g the x-ray diagnosis in two; in one casethe operation was performed before the perfora-tion; in the author's case the findings were notconfirmed (see text). In all cases reported be-fore the x-ray era,, as well as in Moiroud's case,the diagnosis was based on autopsy findings.Th predominant symptom was vomiting (in
8 cas s); pain, haffnatemesis and melwena werefrequent; tarry stools occurred in 2 cases.The test meal was done in only two cases.
Adeq ate free HCI values were present in oneand were low in another.The ulcer was situated in the mid-portion of
the lesser curvature in 9 cases in an unstatedportion of the lesser curvature in 2; in theposterior wall in. 2; the site was not mentionedin 2 cases.
Perforation took place into the first portionof the duodenum in 5 cases; into the secondportion in 1; into the third portion in 1; intothe fOurth portion in 1; jejunum in 2 cases;unstated in 1 case; unstated portion of the duo-denumn in 5 cases.The pylorus was closed or not visualized in
7 cases; slightly patent in 1; open in 2; notstated in 5; unrecognized in 1.
Gastric dilatation or atony present in 7 cases;none in 2; not stated in 7. Gastric delay presentin 7 gases; not stated in 9. Organic hour-glassstomaeh was present in 3 cases.*
DiscussIoNSeveral of the authors reporting cases of
gastroduodenal fistula have, given explanationsof the genesis of this condition. Rokitansky'8expreused the opinion that it may be under-stood on the assumption of-the presence of twoulcerst one of the duodenum, the other of thelesser curvature, between which adhesions takeplace and draw the two regions together. Mel-chart 'feels that this might be the explanationin his second case. Ludin, Moiroud and Catobelieve the production of the snail-form ofstomaeh (Schmieden), due to cicatricial contrac-tion o the lesser curvature, to be responsiblefor th condition. Although this explanationappea plausible, particularly in view ofSchmieden's description of the x-ray appearanceof suOh cases, this does not appear to be thecompl te answer. A study of the findings in
* audek 's case is not included in this analysis be-cause o: lack of data.
several of the reported cases and other relevantfacts gleaned from non-perforated cases buildsa rather strong chain of evidence in support ofthe participation of an additional, preexistingand predisposing factor. Thierfelder, laterWelch,'7 and, latterly, Low-Beer support thisview. Thierfelder. stated that ". . . in certainisolated cases a departure from the normal, tothe following extent is present: as the angleformed by the two segments (body of thestomach and pyloric antrum) of the lesser curva-ture become smaller, the upward direction ofthe pyloric segment becomes steeper, and its leftborder, or even its midportion, comes to lie inthe median plane of the body. " When he lookedfor such departures from the normal he foundthem in two out of sixteen autopsies. The roent-gen ray has demonstrated that such deviationsare not infrequent and are to be seen in the longtype of stomach, with or without atony. Ass-mann, for instance cites a case in which thex-ray findings suggested the presence of aSchmieden complex2 but operation revealed aptosed stomach fixed in the pelvis by adhesions("fixed gastroptosis") ; a clear demonstration ofthe possibility of confusing these two-onditions.Assmann further states that such angulation canalso occur without pelvic fixation. It is of courseobvious that when such relations of the pyloricantrum to the body of the stomach are present,the formation of gastroduodenal fistula wouldbe facilitated. In support of the contention thatthis departure from the usual is a factor inthe production of gastroduodenal fistula standthe descriptions of Hautefeuille's, Le Noir's,TLow-Beer's, Cato's and the author's cases, aswell as clear-cut anatomical and radiologicalevidence. The case reported by Le Noir et at.is interesting in that it simulated, radiologicallyand anatomically, one of spontaneous gastro-duodenal fistula. At operation there appearedto be an ulceration of the lesser curvature; aloop of the duodenum was firmly adherent tothis area. No perforation, however, was foundand careful microscopic examination of the re-sected specimen failed to reveal the presence, ofan ulcer. No cause for the perigastritis couldbe found. This case indicates definitely thatsuch approximation and- adhesion can occur inthe absence of shrinking of the lesser curvature.Melchart 's contention that Low-Beer's case isnot an example of true gastroduodenal fistula,does not invalidate the use of this case as sup-portive evidence, since the nature of the fistula(i.e. true or false) depends only upon the posi-
NoTKiN: FISTULA 171Aug. 1939]
172~~~~TiCAAINMDCLASCTINJUNL[u.13
tion of the ulcer on the lesser curvature and itsrelation to the pylorus. In Hautefeuille's casethe preexisting factor of ptosis and atony appearto be mainly responsible for bringing about thenecessary approximation of the parts, since it isdifficult to believe that adequate shrinkage, aswell as perforation, could occur in the periodof one month. Ptosis and atony, particularlywith the patient confined to bed (as was prob-able in this case because of the h&ematemesis atthis time), would favour apposition of the parts,adhesion and ultimately perforation. In theauthor's case the snail-form of stomach is defi-nitely not present. Apart from the general ap-pearance of the stomach, which reveals nodefinite evidence of shortening of the lessercurvature, the position of the duodenum indi-cates that there has not been an upward-pullingof this segment. In the upright position, withthe stomach full, the new opening, which liesde'finitely above the pylorus, is found at thelevel of the 3rd lumbar vertebra, while thesuperior flexure lies at the level of tthe first. Adrawing-up of the duodenum with a subsequentdilatation of the greater curvature to accom-nodate the gastric stasis induced by the result-ing mechanical hindrance to evacuation is hereuntenable. Definitely, a certain degree of ptosisand atony must have been present before, orearly in the onset of, the organic lesion.
Obviously four main factors play a part inthe production of gastroduodenal fistula; thechronicity of the ulcer, with periods of exacer-bated activity; subsequent extreme shortening ofthe longitudinal fibres of the stomach initiatedin rare cases of gastric ulcer; involvement of thehepatogastrie and hepatoduodenal ligaments inthe inflammatory process; reduction of the anglebetween the descending and ascending portionsof the. stomach, such as occurs in the atonicorgan. A combination of any of the last threefactors with the first can lead ultimately to theproduction of a gastroduodenal' fistula not neces-sarily associated with the Schmieden type ofstomach. The form ultimately. taken by theorgan must depend !upon the combination ofthe factors involved.
Several facts gleaned from a; review of thecases reported woul-d seem to indicate that ifthis is not nature's attempt to produce, a eurecertainly many, of the patients enjoyed a vary-ing period of freedom from symptoms followihgthe -ecurrence of w a fistula. This leads to thethought that in eertain typ'es of -peptic ulcergastroduodenostomny may coneeivably be the
operation of choice. The retention in thisprocedure of two factors present normally, i.e.,the reception of the acid chyme by an organaccustomed to it and the reflux of alkaline duo-denal contents into the stomach, is an advantagethat does not need to be stressed. The objectioncan be raised that the cases with spontaneousgastroduodenal fistula were not well, and activityof the ulcers must have been present sincehiematemesis and meltena occurred in some ofthese cases shortly before death. It must beremembered that in these cases the anastomosisoccurred through a perforated ulcer; that pre-ceding this perforation adhesions were formedinvolving not only the site of the ulcer and theadjacent duodenum but also more distant parts;and lastly that emptying of the stomach occursthrough a perforated ulcer, which is certainlynot conducive to the healing of this ulcer. Whenone considers that under such conditions someof the patients received the benefit of long re-missions, one cannot help speculating on thepossible advantages of gastroduodenostomythrough healthy gastric tissue.
SUMMARYA case of spontaneous gastroduodenal fistula
is reported. As far as can be ascertained, acomplete review of the literature is given. Thetheories regarding the factors underlying thiscomplication are discussed. The question of thepossible advantages of gastroduodenostomy incertain cases of gastric ulcer arises from a studyof these cases.
REFERENCES1. MOHR: Caspar's Wchnschr., No. 16, 1842, quoted by
Thierfelder.2. DITECH: Prager Vierteljahr8chr., Vol. 13, quoted by
Thierfelder.3. BARCLAY: Meedical Times & Gaz., 1850, 2: 439.4. CRUVEILHIER: Traite d'anat. path. gen., Bailliere,
Paris, 1852, 2: 539.5. BARLOW, G. H.: Manual of Practical Medicine,
Churchill, London, 1856, p. 422.6. THIEFELDER: Deut. Arch. f. k1in. Med., 1868, 4: 33.7. LE NOIR, N. P. et al.: Arch. de mal. de i'appareil
digestif, 1926, 16: 935.'8.dCAS9LLAS, P. R.: J. Am. M. Ass., 1926, 87: 1393.9. MONROE, R. T.: Am. J. M. Sc., 1927, 174: 599.
10. LUDIN: Arch. f. Verdauungskrank., quoted by Mel--* *rt.
11. HAUTEFEUILLE: Arch. des mal. de i'appareil digestif,1929; 19:-1273&:.
12. HANGANUT, M. AND DRAGULESCO, J.: Arch. des mal. dei'appareil digestif, 1930,' 20: 711.
13. CArO, E. T.: J. Coll. Surgecom, Australia. 1930, 2: 414.14. MoIRouD, P.: La Presse Medicale, 1935, 63: 1249.15. LE NOIR, N. P. et al.: Soci&t6 Gastro-Enterologique,
19s6.16. MELCHART, F.: Fortschr. a. d. Gebiete d. Roentgen-
strahien, 1931, 44: 335.17. WELCH, W. H.: Pepper's System of Medicine,
*Siunders, Phila., 1885, 2: 507.18. VON ROKITANSKY, K.: Lehrbuch der pathol. Anat.,
Braumuller, Wien, 3 Aufl., bd. 3, 1861, s. 168.19. LoW-BEER, A.: Fortschr. a. d. Geb. d. Roentgen-
strahlen, 1931, 43: 435.20. OEPDMANN 0. BLIX, P.: Quoted by Low-Beer.21. NOVAK: ibid.22. MULLER: ibid.23. HAUDEK, ibid.24. BERG, H. H.:' Roentgen-Untersuchungen am Innen-
relief des Verdauungskanals, 'Ieipzig, 1930, p. 26.
THE CA.NADIAN MEDIcAL AssocIATION JOURNAL172 [Aug. 1939