Embed Size (px)
Citation preview

Original research n
Technical DevelopmenTs
Radiology: Volume 271: Number 1—April 2014 n radiology.rsna.org 239
cardiac arrythmias: Multimodal Assessment Integrating Body Surface ECG Mapping into Cardiac Imaging1
Hubert Cochet, MDRémi Dubois, PhDFrédéric Sacher, MDNicolas Derval, MDMaxime Sermesant, PhDMélèze Hocini, MDMichel Montaudon, MD, PhDMichel Haïssaguerre, MDFrançois Laurent, MDPierre Jaïs, MD
Purpose: To demonstrate the feasibility of comprehensive assess-ment of cardiac arrhythmias by combining body surface electrocardiographic (ECG) mapping (BSM) and imaging.
Materials and Methods:
This study was approved by the institutional review board, and all patients gave written informed consent. Twenty-seven patients referred for electrophysiologic procedures in the context of ventricular tachycardia (VT) (n = 9), Wolff-Parkinson-White (WPW) syndrome (n = 2), atrial fibrillation (AF) (n = 13), or scar-related ventricular fibril-lation (VF) (n = 3) were examined. Patients underwent BSM and imaging with multidetector computed tomog-raphy (CT) (n = 12) and/or delayed enhanced magnetic resonance (MR) imaging (n = 23). BSM was performed by using a 252-electrode vest that enabled the computation of epicardial electrograms from body surface potentials. The epicardial geometry used for BSM was registered to the epicardial geometry segmented from imaging data by using an automatic algorithm. The output was a three-di-mensional cardiac model that integrated cardiac anatomy, myocardial substrate, and epicardial activation.
Results: Acquisition, segmentation, and registration were feasible in all patients. In VT, this enabled a noninvasive assess-ment of the arrhythmia mechanism and its location with respect to the myocardial substrate, coronary vessels, and phrenic nerve. In WPW syndrome, this enabled under-standing of complex accessory pathways resistant to pre-vious ablation. In AF and VF, this enabled the noninvasive assessment of arrhythmia mechanisms and the analysis of rotor trajectories with respect to the myocardial sub-strate. In all patients, three-dimensional models were successfully integrated in navigation systems and used to guide mapping and ablation.
Conclusion: By combining information on anatomy, substrate, and electrical activation, the fusion of BSM and imaging en-ables comprehensive noninvasive assessment of cardiac arrhythmias, with potential applications for diagnosis, prognosis, and ablation targeting.
q RSNA, 2013
Online supplemental material is available for this article.
1 From the Departments of Cardiovascular Imaging (H.C., M.M., F.L.) and Cardiac Pacing and Electrophysiology (F.S., N.D., M. Hocini, M. Haïssaguerre, P.J.), Centre Hospitalier Universitaire/Université de Bordeaux, Hopital Cardiologique Haut Lévêque, Avenue de Magellan, 33604 Pessac, France; L’Institut de Rythmologie et de Modélisa-tion Cardiaque–Equipex Multimodal Platform for Specific Imaging in Cardiology, Centre Hospitalier Universitaire/Université de Bordeaux/Institut National de la Santé et de la Recherche Médicale U1045, Pessac, France (H.C., R.D., F.S., N.D., M.H., M.M., M.H., F.L., P.J.); and Institut National de Recherche en Informatique et Automatique Asclepios Research Team–Institut National de Recherche en Informatique et Automatique Sophia Antipolis, Sophia Antipolis, France (M.S.). From the 2013 RSNA Annual Meet-ing. Received June 10, 2013; revision requested August 5; revision received August 29; accepted September 10; final version accepted September 26. Supported by the Euro-pean Union Seventh Framework Program (FP7/2007-2013) under Grant Agreement HEALTH-F2-2010-261057 and Agence Nationale de la Recherche (grant ANR-10-IAHU-04). Address correspondence to H.C. (e-mail: [email protected]).
q RSNA, 2013
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.

240 radiology.rsna.org n Radiology: Volume 271: Number 1—April 2014
TECHNICAL DEVELOPMENTS : Body Surface ECG Mapping and Imaging for Assessment of Cardiac Arrythmias Cochet et al
focal atrial fibrosis. Patients with a con-traindication to contrast-enhanced MR imaging were excluded. In patients with VT, VF, or WPW syndrome, contrast-enhanced cardiac-gated multidetector CT and/or delayed contrast-enhanced MR imaging were performed unless contraindicated to assess both cardiac anatomy and focal myocardial fibrosis. Patients with a contraindication to both contrast-enhanced multidetector CT and MR imaging were excluded. In the total population, BSM data were com-bined with both multidetector CT data and delayed contrast-enhanced MR im-aging data in eight patients (five with VT, two with VF, and one with WPW syndrome), multidetector CT data only in four patients (all with VT), and de-layed contrast-enhanced MR imag-ing data only in 15 patients (13 with AF and one each with VF and WPW syndrome).
BSM ProceduresBody surface mapping is a recent tech-nology that enables noninvasive and real-time assessment of cardiac electri-cal activity (6). It combines the acqui-sition of a large array of body surface potentials by using a multielectrode
of cardiac arrhythmias by combining BSM and imaging.
Materials and Methods
PopulationThis study was approved by the Insti-tutional Ethics Committee of the Uni-versity Hospital of Bordeaux (Pessac, France), and all patients gave written informed consent. Twenty-seven pa-tients (mean age, 55 years 6 14 [stan-dard deviation]; range, 14–71 years; five female patients) referred for in-vasive electrophysiologic studies were prospectively enrolled. The population was composed of nine patients with scar-related ventricular tachycardia (VT), two patients with Wolff-Parkin-son-White (WPW) syndrome resistant to previous ablation, 13 patients with persistent atrial fibrillation (AF), and three patients with scar-related ven-tricular fibrillation (VF). The substrate was ischemic in all patients with VF. In patients with VT, it was ischemic in five, related to arrhythmogenic right ventricular cardiomyopathy (ARVC) in three, and related to postmyocarditis in one. All patients underwent BSM with a 252-electrode vest and nongated and nonenhanced multidetector CT for lo-calization. In patients with AF, delayed contrast-enhanced MR imaging was performed to assess the distribution of
Cardiac electrical disorders are a major cause of human morbidity and mortality worldwide (1,2).
Because standard 12-lead surface elec-trocardiography (ECG) cannot be used to accurately locate and characterize most arrhythmias, invasive procedures are often required to collect data with intracardiac contact electrodes. Car-diac mapping has direct implications for diagnosis, prognosis, and, even more importantly, the guidance of catheter ablation therapy (3–5). Re-cent developments in noncontact map-ping technology now allow noninvasive three-dimensional (3D) assessment of cardiac activation (6). Body surface ECG mapping (BSM) involves the use of a multielectrode vest to collect body surface potentials and computed to-mography (CT) to precisely locate in three dimensions each electrode with respect to the heart. These two sets of information are then used to compute a large array of epicardial unipolar electrograms. On the other hand, con-trast material–enhanced cardiac-gated multidetector CT can depict cardiac anatomy with high spatial resolution, and delayed contrast-enhanced mag-netic resonance (MR) imaging can be used to assess focal myocardial fibro-sis, the substrate involved in most car-diac arrhythmias (7). We hypothesized that this structural information would be complementary to that provided by BSM. Therefore, we developed soft-ware to load, process, and register data from different modalities and to export the resulting patient-specific multimodal 3D models into 3D map-ping systems to assist intracardiac catheter navigation. The aim of this study was to demonstrate the feasi-bility of comprehensive assessment
Implications for Patient Care
n Body surface mapping and im-aging fusion can be used to locate ventricular tachycardia circuits with respect to cardiac anatomy and myocardial substrate.
n Body surface mapping and im-aging fusion can be used to locate rotor trajectories with respect to cardiac anatomy and myocardial substrate in cardiac fibrillation.
n Body surface mapping and im-aging fusion can be used to locate accessory pathways of un-usual location in Wolff-Parkin-son-White syndrome.
Advances in Knowledge
n Body surface electrocardio-graphic mapping can be com-bined with other cardiac imaging modalities.
n Integration of body surface map-ping into cardiac imaging enables a comprehensive assessment of cardiac arrhythmias.
Published online before print10.1148/radiol.13131331 Content code:
Radiology 2014; 271:239–247
Abbreviations:AF = atrial fibrillationARVC = arrhythmogenic right ventricular cardiomyopathyBSM = body surface ECG mappingECG = electrocardiography3D = three-dimensionalVF = ventricular fibrillationVT = ventricular tachycardiaWPW = Wolff-Parkinson-White
Author contributions:Guarantors of integrity of entire study, H.C., R.D., M. Hocini, P.J.; study concepts/study design or data acquisition or data analysis/interpretation, all authors; manuscript drafting or manuscript revision for important intellectual content, all authors; manuscript final version approval, all authors; literature research, H.C., R.D., M.S., M.M.; clinical studies, H.C., R.D., F.S., N.D., M.S., M. Hocini, M. Haïssaguerre, F.L., P.J.; experimental studies, R.D., M.M.; statistical analysis, R.D.; and manuscript editing, H.C., R.D., F.S., M. Hocini, M.M., F.L., P.J.
Conflicts of interest are listed at the end of this article.

Radiology: Volume 271: Number 1—April 2014 n radiology.rsna.org 241
TECHNICAL DEVELOPMENTS : Body Surface ECG Mapping and Imaging for Assessment of Cardiac Arrythmias Cochet et al
and was preceded by an inversion time scout acquisition to set the inversion time that provided appropriate signal cancellation in the healthy myocardium. Typical imaging parameters were as follows: voxel size, 1.25 3 1.25 3 2.5 mm; flip angle, 22°; repetition time msec/echo time msec, 6.1/2.4; inver-sion time, 260–320 msec (depending on the results of an inversion time scout acquisition performed immediately be-fore data acquisition); and parallel im-aging with a generalized autocalibrating partially parallel acquisitions technique with an acceleration factor of two, 42 reference lines, and an acquisition time of 5–10 minutes, depending on the pa-tient’s heart and breath rate.
Segmentation and RegistrationData processing was performed by using MUSIC software (multimodality software for specific imaging in cardi-ology, L’Institut de Rythmologie et de Modélisation Cardiaque, University of Bordeaux, Institut National de Recher-che en Informatique et Automatique Sophia Antipolis, Sophia Antipolis, France). The software is a solution that was developed in house and built on the open-source medInria software architecture (http://med.inria.fr). Data processing consisted of the following four steps: multidetector CT–MR im-aging fusion, image segmentation, 3D modeling of each segmented object, and BSM integration. Image segmenta-tion in patients with ventricular issues was performed on short-axis reformats. Segmentation in patients with atrial is-sues was performed on transaxial sec-tions. When both cardiac multidetector CT and delayed contrast-enhanced MR imaging had been performed, data sets were fused by using landmark regis-tration prior to segmentation (16). A first set of points was applied in each Digital Imaging and Communications in Medicine series (CT and MR imaging) on consistent anatomic landmarks, and registration accuracy was then assessed on a fused series, with MR imaging data overlaid on CT images, by measur-ing the distance between the two en-docardial borders. In case this distance was greater than 1 mm, additional
activation during sinus rhythm. In pa-tients with VT or WPW syndrome, epicardial electrograms were processed to derive activation maps, as described previously (14). In patients with AF or VF, a phase-mapping algorithm was applied to visualize rotor activity, and automatic tracking of singularity points was applied to visualize rotor core tra-jectories (10).
Cardiac CTCardiac multidetector CT was per-formed by using a contrast-enhanced cardiac-gated method with a 64-section scanner (Somatom Definition). Images were acquired during the first pass of 120 mL of an iodinated contrast me-dium (iomeprol [400 mg iodine per milliliter], Bracco, Milan, Italy) injected at the rate of 4 mL/sec without an ad-ditional saline flush to obtain homoge-neous enhancement of the four cardiac chambers. Typical parameters were as follows: gantry rotation time, 330 msec; temporal resolution, 83 msec; number of detector rows, 64; section thickness, 0.6 mm; tube voltage, 100–120 kV; and typical tube current, 600 mAs with a dose modulation protocol. Mean effec-tive radiation dose was 10.2 mSv 6 6.2 in the study population. Patients who were also undergoing MR imaging were examined during an expiratory breath hold and were placed in the supine po-sition with arms along the body in the CT scanner, in the exact same position as the one used for MR imaging.
MR ImagingDelayed enhanced MR imaging was per-formed with a 1.5-T system (Magnetom Avanto; Siemens, Erlangen, Germany) equipped with a 32-channel cardiac coil. Images were acquired by using a respiratory-navigated inversion recov-ery–prepared cardiac-gated 3D turbo fast low-angle shot sequence with fat saturation that was initially developed for atrial imaging and allows improved spatial resolution (15). Image acqui-sition was initiated 15 minutes after the intravenous injection of a gadolin-ium-based contrast medium (gadoter-ate meglumine, Dotarem; Laboratoire Guerbet, Aulnay-sous-Bois, France)
vest with a thoracoabdominal CT ac-quisition to define the precise location of each electrode with respect to the heart. An algorithm solves an inverse problem to reconstruct unipolar epicar-dial electrograms from these two sets of data (8). Because of its real-time and whole-heart nature, the method needs only a single heartbeat to assess the whole cardiac activation. The out-puts are 3D images of cardiac electrical activity. This technology was validated in animals (8,9) and was recently ap-plied in humans in the context of atrial (10,11) and ventricular (12) arrhyth-mias, as well as dyssychronous heart failure (13). In the current study, BSM was performed by using a commercially available system (CardioInsight Tech-nologies, Cleveland, Ohio). A 252-elec-trode vest positioned on the patient’s thorax and abdomen was used to col-lect body surface potentials. The locali-zation of each electrode with respect to the epicardium was performed immedi-ately prior to mapping by using multi-detector CT with a 64-section scanner (Somatom Definition; Siemens, Forch-heim, Germany) and a nonenhanced and nongated protocol. Mean radiation exposure was 4.9 mSv 6 2.9. Segmen-tation and labeling of all electrodes was performed automatically. Segmentation of the atrial (in patients with AF) or ventricular (in other patients) epicar-dium was performed manually. The reconstruction of epicardial unipolar data from body surface potentials was achieved by using a method described elsewhere (6,8). In patients with VT, BSM was aimed at acquiring sponta-neous VT, or, if this was not available, spontaneous or isoproterenol-induced ectopic beats consistent with the clini-cal VT morphology. In patients with AF (all of whom had persistent AF), BSM was aimed at acquiring 10 seconds of fibrillation segmented in several pauses to exclude QRS complexes from the mapping period. In patients with VF, BSM was aimed at mapping several sec-onds of fibrillation induced by a shock on the T wave during implanted cardio-verter defibrillator testing. In patients with WPW syndrome, BSM was aimed at mapping spontaneous ventricular

242 radiology.rsna.org n Radiology: Volume 271: Number 1—April 2014
TECHNICAL DEVELOPMENTS : Body Surface ECG Mapping and Imaging for Assessment of Cardiac Arrythmias Cochet et al
multimodal 3D models were success-fully integrated in clinical mapping systems and were used to assist intra-cardiac mapping or ablation.
Results in Scar-related VTThe site of earliest ventricular epicardial activation was successfully displayed in all nine patients with scar-related VT. Spontaneous clinical VT was directly mapped in three patients, giving access to the arrhythmia mechanism and the isthmus location with respect to myo-cardial substrate, coronary arteries, and phrenic nerve. Figure E1 (online) shows example images in a patient with dilated cardiomyopathy after myocardi-tis. In five patients, spontaneous clinical VT could not be obtained during BSM and was therefore indirectly assessed by means of the mapping of ventricular ectopic beats of consistent morphology. Figure E2 (online) shows example im-ages in a patient with ARVC. In all five patients with ischemic VT, the earliest epicardial exit was located within the substrate segmented from imaging—that is, scarring from delayed contrast-enhanced MR imaging data (n = 3) or wall thinning from multidetector CT data (n = 2). In all three patients with ARVC, the earliest epicardial exit was located within areas of right ventricular fat density, as revealed by the segmen-tation of multidetector CT data (n = 3). In the patient with postmyocarditis VT, the earliest epicardial exit was lo-cated within areas of wall thinning, as revealed by the segmentation of multi-detector CT data.
Results in WPW Syndrome Resistant to prior AblationThe site of earliest ventricular epicar-dial activation was successfully dis-played in the two patients with WPW syndrome. This enabled the localiza-tion of accessory pathways of unusual location and their relationship with surrounding anatomic structures, as well as the scarring from prior abla-tion procedures. In the first patient (a 32-year-old man), this allowed for precise characterization of a pre-ex-citation site that was located imme-diately below the aortic cusp and was
scaling) that modifies one surface to best match the other in a least-squares sense. In this study, this algorithm was implemented in the open-source visu-alization toolkit software environment (VTK; Kitware, New York, NY). More details on the validation of the ICP al-gorithm can be found in the literature (21,22). The accuracy of registration was assessed by measuring the mean distance between both epicardial sur-faces after registration. Once regis-tered, BSM scalars corresponding to electrical data were projected along the perpendicular direction and were mapped over the epicardial geometry derived from imaging. To minimize in-terpolation errors during projection, epicardial surfaces were modeled with high spatial resolution (.105 triangles). The output was a 3D model integrating high-definition cardiac anatomy, abnor-mal myocardial substrate, and electri-cal activation data. Three-dimensional models were integrated into catheter localization platforms (CARTO 3; Bio-sense Webster, Diamond Bar, Calif) and were used to assist 3D navigation of intracardiac catheters during map-ping and ablation procedures. This method for patient-specific multimodal-ity assessment of cardiac arrhythmias is illustrated in Figure 1.
Results
FeasibilityThe MUSIC software allowed multi-modal data processing and registration in all patients. In patients examined with both cardiac-gated multidetector CT and delayed contrast-enhanced MR imaging (n = 9), registration between data sets was in all cases successfully achieved with submillimetric accuracy. After BSM, epicardial geometry was registered to the epicardial geometry derived from cardiac-gated imaging, the mean distance between surfaces was 3.3 mm 6 2.3 for atrial studies and 3.0 6 2.3 for ventricular studies. The total processing time, including the time for segmentation and registration, was typically less than 1 hour. In all patients, the resulting patient-specific
points were added in the two series, and registration and fusion were then performed again until submillimetric accuracy was reached. The MR imag-ing data set was then resampled in the same matrix and orientation as the CT series. Segmentation was subsequently performed on these registered multide-tector CT and MR imaging data sets. On multidetector CT images, the blood pool was segmented by using region growing and was used to derive endo-cardial segmentations. The coronary arteries were also segmented by using region growing, with additional manual segmentation for distal branches when necessary. The epicardium, coronary sinus, and phrenic nerve were seg-mented manually by using linear inter-polation to save processing time, with regions of interest (ROIs) being man-ually drawn on several sections only. In patients with an ischemic substrate and a contraindication to MR imaging, the substrate was assessed on multide-tector CT images by using automatic segmentation of wall thinning (17). In patients with ARVC, the substrate was assessed on multidetector CT im-ages by using automatic segmentation of right ventricular intramyocardial fat (18). On MR images, the endocardium and epicardium were segmented man-ually. Segmentation was performed by using ROI interpolation for patients with ventricular issues and section-by-section for patients with atrial issues. Atrial and ventricular focal fibrosis was segmented by using adaptive histogram thresholding with algorithms described elsewhere (15,19,20). Each segmented structure was then modeled as a 3D mesh computed in vtk format (Kitware, New York, NY). Integration of electri-cal data was achieved by registering the BSM epicardial mesh derived from non-enhanced and nongated thoracoabdom-inal CT acquisitions with the epicardial mesh derived from contrast-enhanced cardiac-gated imaging. This registration was automatically achieved by using an iterative closest points (ICP) algorithm. The ICP algorithm matches each vertex on one surface with the closest surface point on the other, then applies the transformation (translation, rotation,

Radiology: Volume 271: Number 1—April 2014 n radiology.rsna.org 243
TECHNICAL DEVELOPMENTS : Body Surface ECG Mapping and Imaging for Assessment of Cardiac Arrythmias Cochet et al
DiscussionThis study introduced a multimodal in-tegrative approach that combines elec-trical and structural data to noninva-sively characterize cardiac arrhythmias. Registration between BSM, cardiac-gated multidetector CT, and/or delayed contrast-enhanced MR imaging is fea-sible by using dedicated software. In scar-related VT, it enables noninvasive panoramic assessment of the arrhyth-mia before or during the procedure, allowing for mechanism identification and localization of circuits with re-spect to cardiac anatomy and the myo-cardial substrate. In WPW syndrome
Results in Cardiac AF and VFIn all patients, rotor activity was success-fully detected, and automatic tracking of phase singularities enabled the visualiza-tion of rotor core trajectories over the epicardium. The fusion between BSM and delayed contrast-enhanced MR im-aging enabled the analysis of the rela-tionship between rotor trajectories and myocardial fibrosis. These multimodal data were integrated in 3D mapping systems and were used to assist AF abla-tion procedures targeting rotor regions. Figure 3 shows an example of structure-function relationships in a patient with persistent AF.
subsequently successfully targeted with ablation. The second patient (a 14-year-old girl) had a history of two VF episodes related to WPW syndrome and resistance to three prior ablation procedures, including one with epi-cardial access. A right atrial divertic-ulum was found at multidetector CT, and its implication in ventricular pre-excitation was demonstrated at BSM. Extensive scarring was found around the tricuspid annulus at delayed con-trast-enhanced MR imaging but none was found in the diverticulum area. Findings in this patient with WPW syndrome are illustrated in Figure 2.
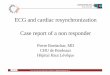
Figure 1
Figure 1: Multimodality assessment of cardiac arrhythmias by combining BSM with other cardiac imaging modalities. The method combines different cardiac data sets acquired with, A, contrast-enhanced ECG-gated multidetector CT, B, high-spatial-resolution delayed contrast-enhanced MR imaging, and, C, BSM performed by using a multielectrode vest. D, Cardiac structures are segmented from multidetector CT data by using automatic and semiautomatic tools. E, Myocardial fibrotic substrate is segmented on delayed contrast-enhanced MR imaging data by using histogram thresholding. F, A large array of unipolar epicardial electrograms is computed from body surface potentials acquired with the vest and is used to display 3D activation maps. G, All processed data are registered to derive a patient-specific 3D model that combines cardiac anatomy, myocardial substrate, and epicardial activation data.

244 radiology.rsna.org n Radiology: Volume 271: Number 1—April 2014
TECHNICAL DEVELOPMENTS : Body Surface ECG Mapping and Imaging for Assessment of Cardiac Arrythmias Cochet et al
structures. Because of its ability to characterize myocardial tissue, delayed-enhanced MR imaging is considered to be the reference for the assessment of myocardial fibrotic substrate (25).
In scar-related VT, this study shows that multidetector CT and MR imaging data on cardiac anatomy and the myo-cardial substrate can be combined with the arrhythmia mechanism as assessed with BSM and that this information can be made available in 3D mapping systems to assist therapy. The feasi-bility of image integration has already been described in AF and VT ablation procedures (26,27). We demonstrate that electrical information can also be embedded, and that combining high-definition structural and functional data has incremental value. Although an effect on procedural duration and patient outcome remains to be docu-mented, the impact on patient care seems obvious, particularly in the con-text of poorly tolerated or nonsustained
because it enables real-time and whole heart assessment of cardiac activation. These elements are key for nonmap-pable arrhythmias and mandatory for revealing the mechanisms of cardiac fibrillation (10). In this context, the method will likely become part of the standard assessment of cardiac ar-rhythmias in the near future.
Because of its 3D nature, there is no obstacle to combining BSM with other cardiac imaging modalities such as multidetector CT and MR imaging. A multimodal approach would be par-ticularly suited for the assessment of cardiac arrhythmias because the organ is characterized by multiple interde-pendent functions and because the vast majority of arrhythmias occur in structurally diseased hearts (1,24). Be-cause of its high spatial resolution and simplicity of segmentation, contrast-en-hanced ECG-gated cardiac multidetec-tor CT is considered to be the reference method for the assessment of cardiac
resistant to prior ablation, it enables the characterization of complex acces-sory pathways of unusual location and the localization of pre-excitation sites with respect to scarring from previous ablations. In AF and VF, it enables the first description of rotor core location with respect to myocardial fibrosis in humans in vivo.
BSM offers the opportunity to over-come the limitations of 12-lead ECG and may prove superior to invasive contact electrophysiologic mapping procedures for the diagnosis and risk stratification of cardiac arrhythmias. In addition to its invasive nature, con-tact mapping allows only for a sequen-tial acquisition of electrophysiologic signals and is therefore limited when the arrhythmia is not inducible, is not sustained, or is poorly tolerated (23). BSM can be regarded as a technologic breakthrough in the management of cardiac arrhythmias, not only because of its noninvasive nature but also
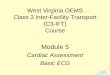
Figure 2
Figure 2: Multimodality assessment and catheter ablation guidance in 14-year-old girl with WPW syndrome that was resistant to prior abla-tion. The patient experienced two sudden cardiac arrests related to VF episodes. Surface 12-lead ECG showed right-sided ventricular pre-exci-tation resistant to three ablation procedures, including one with an epicardial approach. A, Contrast-enhanced ECG-gated cardiac multidetector CT showed a right-atrium diverticulum emerging from the inferior insertion of the right appendage and extending toward right ventricular free wall. B, These anatomic data were combined with the ventricular activation data acquired by using BSM and demonstrated that the diverticulum was hosting the accessory pathway. C, The patient-specific model was integrated into a 3D mapping system to guide the ablation. Ablation was performed at the diverticulum ostium (arrow in C), resulting in successful termination of, D, ventricular pre-excitation.

Radiology: Volume 271: Number 1—April 2014 n radiology.rsna.org 245
TECHNICAL DEVELOPMENTS : Body Surface ECG Mapping and Imaging for Assessment of Cardiac Arrythmias Cochet et al
vivo, have identified important drivers as sustained spiral waves of propaga-tion—the so-called rotors (29). There-fore, the ability to predict or directly visualize the sites where rotors are sustainably observed (ie, anchoring), would be of great interest for individ-ually tailoring therapy. Real-time and whole-heart mapping with BSM allows, for the first time, a panoramic visuali-zation of rotor activity during cardiac fibrillation (10). The interstitial fibrosis present in the left atrial wall in patients with AF provides an ideal heteroge-neous substrate for circuit reentry and rotor activity (30). Therefore, it seems reasonable to assume that the combi-nation of BSM with MR imaging data on structural remodeling should lead to
our results support the use of nonin-vasive testing to characterize accessory pathways that are frequently of unusual location (28).
In AF and VF, the fusion between imaging and BSM offers for the first time an opportunity to study the rela-tionship between the arrhythmia mech-anism and the fibrotic substrate in vivo. In addition to the incremental knowl-edge, this could have substantial impact on patient care. Complex cardiac fibril-lations such as the one encountered in patients with chronic AF is supposed to be sustained by discrete sources po-tentially amenable to ablation therapy. Studies involving computer modeling and optical mapping on tissue samples, as well as electrophysiologic mapping in
arrhythmias that are not accessible to conventional sequential contact map-ping. In addition to multidetector CT and MR imaging, other cardiac imaging modalities might be relevant for the as-sessment of cardiac arrhythmias, such as positron emission tomography and 3D echocardiography. The processing and integration of these data sets will be implemented in MUSIC software in the near future.
In WPW syndrome, our study sug-gests that combining imaging and BSM is feasible and allows the accurate local-ization of the ventricular pre-excitation site. WPW syndrome is usually not a problem for diagnosis or for treatment (5). However, in the setting of WPW syndrome that is resistant to ablation,
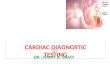
Figure 3
Figure 3: A–D, Multimodality assessment of AF in 58-year-old man. A, Areas of focal fibrosis within the atrial wall were segmented on high-spatial-resolution delayed contrast-enhanced MR imaging data by using histogram thresholding. This segmentation was used to derive, B, a patient-specific model displaying the distribution of focal fibrosis over a biatrial surface. C, Real-time and whole-heart activation was explored at BSM during 10 seconds of AF by using a multielec-trode vest. D, Phase mapping demonstrated rotor activity in the posterior wall of the left atrium. E, After automatic tracking of phase singularity points, the tra-jectories of all observed rotors were registered to MR imaging data. Trajectories were color-coded according to rotor likelihood to enable visualization of the sites where rotors were anchoring. This multimodality assessment enables, for the first time, an analysis of the relationships between rotor activity and myocardial fibrosis in cardiac fibrillation.

246 radiology.rsna.org n Radiology: Volume 271: Number 1—April 2014
TECHNICAL DEVELOPMENTS : Body Surface ECG Mapping and Imaging for Assessment of Cardiac Arrythmias Cochet et al
imaging for cardiac electrophysiology and arrhythmia. Nat Med 2004;10(4):422–428.
7. Kléber AG, Rudy Y. Basic mechanisms of car-diac impulse propagation and associated ar-rhythmias. Physiol Rev 2004;84(2):431–488.
8. Oster HS, Taccardi B, Lux RL, Ershler PR, Rudy Y. Noninvasive electrocardiographic imaging: reconstruction of epicardial po-tentials, electrograms, and isochrones and localization of single and multiple electro-cardiac events. Circulation 1997;96(3): 1012–1024.
9. Burnes JE, Taccardi B, Rudy Y. A noninva-sive imaging modality for cardiac arrhyth-mias. Circulation 2000;102(17):2152–2158.
10. Haissaguerre M, Hocini M, Shah AJ, et al. Noninvasive panoramic mapping of hu-man atrial fibrillation mechanisms: a fea-sibility report. J Cardiovasc Electrophysiol 2013;24(6):711–717.
11. Shah AJ, Hocini M, Xhaet O, et al. Validation of novel 3-dimensional electrocardiographic mapping of atrial tachycardias by invasive mapping and ablation: a multicenter study. J Am Coll Cardiol 2013;62(10):889–897.
12. Wang Y, Cuculich PS, Zhang J, et al. Noninvasive electroanatomic mapping of human ventricular arrhythmias with elec-trocardiographic imaging. Sci Transl Med 2011;3(98):98ra84.
13. Ploux S, Lumens J, Whinnett Z, et al. Non-invasive electrocardiographic mapping to improve patient selection for cardiac resyn-chronization therapy: beyond QRS duration and left bundle branch block morphology. J Am Coll Cardiol 2013;61(24):2435–2443.
14. Dubois R, Labarthe S, Coudière Y, et al. Global and directional activation maps for cardiac mapping in electrophysiology. Com-put Cardiol 2012;39:349–352.
15. Oakes RS, Badger TJ, Kholmovski EG, et al. Detection and quantification of left atrial structural remodeling with delayed-enhance-ment magnetic resonance imaging in patients with atrial fibrillation. Circulation 2009; 119(13):1758–1767.
16. Cochet H, Komatsu Y, Sacher F, et al. Integra-tion of merged delayed-enhanced magnetic resonance imaging and multidetector com-puted tomography for the guidance of ven-tricular tachycardia ablation: a pilot study. J Cardiovasc Electrophysiol 2013;24(4): 419–426.
17. Komatsu Y, Cochet H, Jadidi A, et al. Re-gional myocardial wall thinning at multi-detector computed tomography correlates to arrhythmogenic substrate in postinfarc-tion ventricular tachycardia: assessment of
No relevant conflicts of interest to disclose. M. Hocini No relevant conflicts of interest to dis-close. M.M. No relevant conflicts of interest to disclose. M. Haïssaguerre Financial activities related to the present article: is a shareholder in CardioInsight Technologies. Financial activities not related to the present article: has benefited from a grant from Boston Scientific. Other re-lationships: none to disclose. F.L. No relevant conflicts of interest to disclose. P.J. Financial ac-tivities related to the present article: is a share-holder in CardioInsight Technologies. Financial activities not related to the present article: has benefited from a grant from Boston Scientific. Other relationships: none to disclose.
References 1. Zipes DP, Wellens HJ. Sudden cardiac
death. Circulation 1998;98(21):2334–2351.
2. Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med 2002;113(5):359–364.
3. Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 Guidelines for Man-agement of Patients With Ventricular Ar-rhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart As-sociation Task Force and the European So-ciety of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in col-laboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation 2006;114(10):e385–e484.
4. Fuster V, Rydén LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorpo-rated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2011;123(10):e269–e367.
5. Blomström-Lundqvist C, Scheinman MM, Al-iot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraven-tricular arrhythmias: executive summary—a report of the American College of Cardiol-ogy/American Heart Association Task Force on Practice Guidelines and the European So-ciety of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Supraventricular Arrhythmias). Circu-lation 2003;108(15):1871–1909.
6. Ramanathan C, Ghanem RN, Jia P, Ryu K, Rudy Y. Noninvasive electrocardiographic
the definition of new ablation targets in these two devastating diseases that are currently poorly accessible to specific therapy.
The main limitation of this study was the absence of systematic correla-tion with procedural findings or patient outcome. However, the aim of this work was to assess the feasibility of combin-ing BSM with other cardiac imaging modalities and to illustrate how this strategy can accommodate the spec-trum of the most difficult cardiac elec-trical disorders encountered in clinical practice. Therefore, procedural results are only described qualitatively, owing to the heterogeneity of the diseases. For each of these diseases, the impact of the approach on procedural manage-ment and patient outcome should be thoroughly addressed in future studies.
In conclusion, BSM can be combined with other cardiac imaging modalities, providing a comprehensive noninvasive assessment of cardiac arrhythmias. This multimodal information can be made available in 3D mapping systems to as-sist catheter ablation therapy of complex atrial, supraventricular, or ventricular arrhythmias. It enables the identifica-tion of arrhythmia mechanisms and the localization of circuits or sources with respect to cardiac anatomy and myo-cardial substrate. In cardiac fibrillation, the method enables for the first time the localization of rotor trajectories with re-spect to cardiac anatomy and myocar-dial substrate. Further studies should be performed to assess the impact of this approach on procedural management and patient outcome.
Disclosures of Conflicts of Interest: H.C. No relevant conflicts of interest to disclose. R.D. Fi-nancial activities related to the present article: none to disclose. Financial activities not related to the present article: is a consultant for and owns stock or stock options in CardioInsight Technologies. Other relationships: none to dis-close. F.S. Financial activities related to the pre-sent article: none to disclose. Financial activities not related to the present article: is a consultant for Sorin Group; is on the speakers bureaus of Biosense Webster, Bayer Healthcare, St Jude Medical, Sorin Group, and Medtronic; received compensation for travel and accommodation ex-penses for a Heart Rhythm meeting; institution has grants or grants pending with Medtronic. Other relationships: none to disclose. N.D. No relevant conflicts of interest to disclose. M.S.

Radiology: Volume 271: Number 1—April 2014 n radiology.rsna.org 247
TECHNICAL DEVELOPMENTS : Body Surface ECG Mapping and Imaging for Assessment of Cardiac Arrythmias Cochet et al
structural and electrical substrate. Circ Ar-rhythm Electrophysiol 2013;6(2):342–350.
18. Cochet H, Komatsu Y, Jadidi AS, et al. Automatic myocardial fat quantification at contrast-enhanced cardiac MDCT in ar-rhythmogenic right ventricular cardiomyop-athy: initial validation vs controls [abstr]. Heart Rhythm 2013;S235–S290.
19. Amado LC, Gerber BL, Gupta SN, et al. Accurate and objective infarct sizing by con-trast-enhanced magnetic resonance imaging in a canine myocardial infarction model. J Am Coll Cardiol 2004;44(12):2383–2389.
20. Roes SD, Borleffs CJ, van der Geest RJ, et al. Infarct tissue heterogeneity assessed with contrast-enhanced MRI predicts spon-taneous ventricular arrhythmia in patients with ischemic cardiomyopathy and implant-able cardioverter-defibrillator. Circ Cardio-vasc Imaging 2009;2(3):183–190.
21. Zhang Z. Iterative point matching for regis-tration of free-form curves and surfaces. Int J Comput Vis 1994;13(2):119–152.
22. Pomerleau F, Colas F, Siegwart R, Magnenat S. Comparing ICP variants on real-world data sets. Auton Robots 2013;34(3):133–148.
23. Callans DJ, Zado E, Sarter BH, Schwartzman D, Gottlieb CD, Marchlinski FE. Efficacy of radiofrequency catheter ablation for ventric-ular tachycardia in healed myocardial infarc-tion. Am J Cardiol 1998;82(4):429–432.
24. Burstein B, Nattel S. Atrial fibrosis: mech-anisms and clinical relevance in atrial fibril-lation. J Am Coll Cardiol 2008;51(8):802–809.
25. Kim RJ, Wu E, Rafael A, et al. The use of contrast-enhanced magnetic resonance im-aging to identify reversible myocardial dys-function. N Engl J Med 2000;343(20):1445–1453.
26. Reddy VY, Malchano ZJ, Holmvang G, et al. Integration of cardiac magnetic reso-nance imaging with three-dimensional electroanatomic mapping to guide left ventricular catheter manipulation: feasi-bility in a porcine model of healed myo-
cardial infarction. J Am Coll Cardiol 2004;44(11):2202–2213.
27. Malchano ZJ, Neuzil P, Cury RC, et al. In-tegration of cardiac CT/MR imaging with three-dimensional electroanatomical map-ping to guide catheter manipulation in the left atrium: implications for catheter abla-tion of atrial fibrillation. J Cardiovasc Elec-trophysiol 2006;17(11):1221–1229.
28. Sacher F, Wright M, Tedrow UB, et al. Wolff-Parkinson-White ablation after a prior failure: a 7-year multicentre experi-ence. Europace 2010;12(6):835–841.
29. Jalife J, Berenfeld O, Mansour M. Mother rotors and fibrillatory conduction: a mech-anism of atrial fibrillation. Cardiovasc Res 2002;54(2):204–216.
30. Zlochiver S, Muñoz V, Vikstrom KL, Taf-fet SM, Berenfeld O, Jalife J. Electrotonic myofibroblast-to-myocyte coupling increases propensity to reentrant arrhythmias in two-dimensional cardiac monolayers. Biophys J 2008;95(9):4469–4480.