-
Abas, KristineAlfelor, RemelouAraneta, LoisBagacay, Julius**
-
30 year old male FilipinoGeneral manager of JollibeeCHIEF
COMPLAINT: Difficulty of Breathing
**
-
HISTORY OF PRESENT ILLNESS**
-
SALIENT FEATURES(+) Easy fatigability(+) Shortness of breath
when at work(+) Palpitations accompanied by chest pain occurring
even at restProgression of symptomsNo relief with Seretide(-)
Fever(-) Smoker(+) nonproductive cough for 3 weeks esp when
supine(+) episodes of near syncope(+) swelling of both feet(+)
maternal history of heart disease (died at 45yrs old)*
**
-
REVIEW OF SYSTEM(+) nonproductive cough for 3 weeks especially
when supine(+) episode of near-syncope few weeks ago(+) swelling of
both feet(-) fever, (-)headache/dizziness, (-) abdominal pain, (-)
changes in bowel character, (-) dysuria, (-) joint pain
**
-
PHx: nonsmoker, no intake of alcoholic beverage, currently works
as a manager in Jollibee
Past Medical Hx: (-) hypertension, diabetes, allergies(+) asthma
recently diagnosed and maintained on Seretide BID
Family Hx:, (-) HPN, diabetes, asthma(+) heart disease mother,
died at 45 years old**
-
PHYSICAL EXAMINATIONGeneral Survey: conscious, coherent,
ambulatory, very anxiousVital Signs: BP=90/60, HR=102/min
(irregularly irregular)RR= 24/min, Temp: 36.8oCWeight: 46 kg,
Height: 155cm, BMI= 19.0HEENT: pink palpebral conjunctivae, no
cervical lymphadenopathyicteric scleraeSkin:good skin turgor, no
lesionsNeck: no carotid bruits, brisk upstroke of carotid pulse,
JVP=5 cm at 30o**
-
PHYSICAL EXAMINATIONLungs: equal chest expansion, no
retractions, equal tactile fremitus both lung fields, resonant to
percussion on both lung fields(+) fine basilar crackles on both
lung fieldsCardiac:(+) RV heave, no thrills, apex beat at the 5th
ICS 2 cm lateral to the left midclavicular line, loud S1 at apex,
prominent P2 at the base, (+) gr 3/6 middiastolic rumble at
apexExtremities: (+) gr 1 bipedal edema, dorsalis pedis pulse (+2),
no clubbing, no cyanosis**
-
Additional PE that should be done:Presence of oral ulcersMitral
FaciesJoint tendernessSubcutaneous nodulesAbdominal examNeurologic
exam**
-
**
-
Other PE findings to be done:Presence of oral ulcersMitral
faciesJoint tendernessSubcutaneous nodulesAbdominal examNeurologic
exam**
-
DIFFERENTIAL DIAGNOSISMitral Valve DiseaseMitral StenosisMitral
RegurgitationAtrial MyxomaAsthmaChronic Obstructive Pulmonary
Disease (COPD)PRIMARY WORKING IMPRESSION:MITRAL VALVE
STENOSIS**
-
DIAGNOSTICS**
-
LABS CBC FBS: 80Hgb 12 Creatinine: 1.0Hct 0.48 Na 142, K 3.5,
SGPT 40WBC 10 seg 55% Urinalysis: lympho 45% Spec grav 1.030plt
230,000 (-)sugar, WBC, RBC
-
Additional Diagnostics2D EchocardiographyHolter Monitoring
-
**
-
**
-
**
-
**
-
DIAGNOSISUnderlying Etiology: Rheumatic Fever Anatomical
Abnormalities: Mitral Valve Stenosis3) Physiologic Disturbances:
Right Congestive Heart Failure4) Functional Disability: NYHA Class
IV**
-
Pathophysiology
-
Pathophysiology
PathogenesisAssociated signs and symptomsMitral Stenosis(+)3/6
middiastolic murmur at apex, Loud S1
LA fails to empty blood to LVLA enlarges(+)LA enlargement on
radiographDecrease LV filling = decrease CO
(+)Easy fatigability, Dyspnea on exertion
Increase pressure in pulmonary veins
-
Pathophysiology
PathogenesisAssociated signs and symptomsLA failure causes
pulmonary hypertension and edema(+)Paroxysmal nocturnal dyspnea,
progressive dyspnea, fine bibasilar crackles on both lung fields,
non productive cough, (+)prominent pulmo vasc Increase pressure in
pulmonary arteriesRV needs to increase effort in pumping blood to
pulmonary vessels (+)RV heave, (+)possible RV enlargement on chest
X-ray causing displacement of apex beat to 2 cm lateral to left MCL
5th ICS, (+)Prominent P2 at baseRV contributes to pulmonary
congestion and later on fails
-
Pathophysiology
PathogenesisAssociated Signs and SymptomsRA unable to pump blood
to RV due to increase pressure in the RV. RA soon failsRight heart
failure causes pooling of blood to the venous side of the
circulation (+)grade 1 bipedal edema
-
**
-
MITRAL STENOSIS: ManagementGoals of Medical Treatment:
Prevention / Treatment of ComplicationsMonitorPrevention of
recurrent infection
-
Pharmacologic approach:Symptom Control:Beta blockers,
nondihydropyridine calcium channel blockers, or digoxin for rate
control of AFCardioversion for new-onset AF and HFDiuretics for
HF.
-
Natural HistoryWarfarin for AF or thromboembolismPCN for RF
prophylaxis
-
Mitral valvotomy is indicated in symptomatic [New York Heart
Association (NYHA) Functional Class IIIV]2 ways: PMBV and Surgical
Valvotomy
-
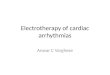
Date of download: 8/26/2013Copyright The American College of
Cardiology. All rights reserved.From: ACC/AHA 2006 Practice
Guidelines for the Management of Patients With Valvular Heart
Disease: Executive Summary: A Report of the American College of
Cardiology/American Heart Association Task Force on Practice
Guidelines (Writing Committee to Revise the 1998 Guidelines for the
Management of Patients With Valvular Heart Disease) Developed in
Collaboration With the Society of Cardiovascular Anesthesiologists
Endorsed by the Society for Cardiovascular Angiography and
Interventions and the Society of Thoracic SurgeonsJ Am Coll
Cardiol. 2006;48(3):598-675.
doi:10.1016/j.jacc.2006.05.030Management strategy for patients with
mitral stenosis and mild symptoms. *The committee recognizes that
there may be variability in the measurement of mitral valve area
(MVA) and that the mean transmitral gradient, pulmonary artery
wedge pressure (PAWP), and pulmonary artery systolic pressure
(PASP) should also be taken into consideration. There is
controversy as to whether patients with severe mitral stenosis (MVA
less than 1.0 cm2) and severe pulmonary hypertension (PH; PASP
greater than 60 mm Hg) should undergo percutaneous mitral balloon
valvotomy (PMBV) or mitral valve replacement (MVR) to prevent right
ventricular failure. CXR indicates chest X-ray; ECG,
electrocardiogram; echo, echocardiography; LA, left atrial; MR,
mitral regurgitation; MVG, mean mitral valve pressure gradient;
NYHA, New York Heart Association; PAP, pulmonary artery pressure;
2D, 2-dimensional.
Figure Legend:
-
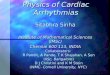
Date of download: 8/26/2013Copyright The American College of
Cardiology. All rights reserved.From: ACC/AHA 2006 Practice
Guidelines for the Management of Patients With Valvular Heart
Disease: Executive Summary: A Report of the American College of
Cardiology/American Heart Association Task Force on Practice
Guidelines (Writing Committee to Revise the 1998 Guidelines for the
Management of Patients With Valvular Heart Disease) Developed in
Collaboration With the Society of Cardiovascular Anesthesiologists
Endorsed by the Society for Cardiovascular Angiography and
Interventions and the Society of Thoracic SurgeonsJ Am Coll
Cardiol. 2006;48(3):598-675.
doi:10.1016/j.jacc.2006.05.030Management strategy for patients with
mitral stenosis and moderate to severe symptoms. *The writing
committee recognizes that there may be variability in the
measurement of mitral valve area (MVA) and that the mean
transmitral gradient, pulmonary artery wedge pressure (PAWP), and
pulmonary artery systolic pressure (PASP) should also be taken into
consideration. It is controversial as to which patients with less
favorable valve morphology should undergo percutaneous mitral
balloon valvotomy (PMBV) rather than mitral valve surgery (see
text). CXR, chest X-ray; ECG, electrocardiogram; echo,
echocardiography; LA, left atrial; MR, mitral regurgitation; MVG,
mean mitral valve pressure gradient; MVR, mitral valve replacement;
NYHA, New York Heart Association; 2D, 2-dimensional.
Figure Legend:
-
**
-
**ACC/AHA PRACTICE GUIDELINESEXECUTIVE SUMMARYACC/AHA 2006
Practice Guidelines for the Management of Patients With Valvular
Heart Disease: Executive SummaryA Report of the American College of
Cardiology/AmericanHeart Association Task Force on Practice
Guidelines(Writing Committee to Revise the 1998 Guidelines for the
Management of Patients With Valvular Heart Disease)
-
**ACC/AHA PRACTICE GUIDELINESEXECUTIVE SUMMARYACC/AHA 2006
Practice Guidelines for the Management of Patients With Valvular
Heart Disease: Executive SummaryA Report of the American College of
Cardiology/AmericanHeart Association Task Force on Practice
Guidelines(Writing Committee to Revise the 1998 Guidelines for the
Management of Patients With Valvular Heart Disease)
-
Outlook (Prognosis)The outcome varies. The disorder may be mild,
without symptoms, or may be more severe and eventually disabling.
Complications may be severe or life threatening. Mitral stenosis is
usually controllable with treatment and improved with valvuloplasty
or surgery.Possible ComplicationsAtrial fibrillation and atrial
flutterBlood clotsto the brain (stroke), intestines, kidneys, or
other areasCongestive heart failurePulmonary edemaPulmonary
hypertension
**
-
**
-
**
General Data: 30 year old Filipino male from MakatiChief
Complaint: difficulty of breathing
*HPI: 2 months prior to consult, the patient started to note
easy fatigability and shortness of breath when at work, forcing him
to take frequent breaks. He also noted palpitations accompanied by
chest pain occurring even at rest. One month prior to consult, he
noted progression of symptoms, now occurring more frequently and
with less activity. He also noted waking up from sleep due to not
getting enough air. When he consulted his family doctor, he was
given Seretide inhaler to be used twice a day. Symptoms persisted
despite medications, prompting present consult.
SERETIDE = Fluticasone + Sameterol ( Not used for acute asthma
symptoms) *ROS: (+) nonproductive cough for 3 weeks especially when
supine, (-) fever, (-) headache/dizziness, (+) episode of
near-syncope few weeks ago, (-) abdominal pain, (-) changes in
bowel character, (-) dysuria, (+) swelling of both feet, (-) joint
pain
(+) nonproductive cough for 3 weeks especially when supine =
PAROXYS(+) episode of near-syncope few weeks ago(+) swelling of
both feet*PHx: nonsmoker, no intake of alcoholic beverage,
currently works as a manager in JollibeePast Medical Hx: (+) asthma
recently diagnosed and maintained on Seretide BID, (-)
hypertension, diabetes, allergies**** It is important to ask the
patient if he had a history of scarlet fever or sore throat that
was poorly treated before way back 5-10 years agoFamily Hx: (+)
heart disease mother, died at 45 years old, (-) HPN, diabetes,
asthma**** Ask the patient the specific cause of death of the
patient, his mother dying early due to heart disease can be an
indication that the patient might have a congenital heart disease
such as
*Physical Exam:General Survey: conscious, coherent, ambulatory,
very anxiousVital Signs: BP=90/60HR=102/min, irregularly
irregularRR=24/minTemp: 36.8oCWeight: 46 kgHeight: 155cmHEENT: pink
palpebral conjunctivae, icteric sclerae, no cervical
lymphadenopathySkin: good skin turgor, no lesionsNeck: no carotid
bruits, brisk upstroke of carotid pulse, JVP=5 cm at 30oVery
anxious = caused by difficulty of breathing or not feeling well,
agitationBP = hypotensive = HR = tachycardic, irregularly irregular
(atrial fibrillation???) = compensation for low cardiac outputRR =
tachypnic = compensation for low cardiac output BMI =
healthy46/2.425 = 18.9 = healthy weight range for asians (asian
diabetes initiative)Icteric sclerae = jaundiceJVP=5 cm at 30o =
increased right atrial pressure/ central venous pressureIcteric
sclerae = jaundice (liver damage)
*Lungs: equal chest expansion, no retractions, equal tactile
fremitus both lung fields, resonant to percussion on both lung
fields, (+) fine bibasilar crackles on both lungfieldsCardiac: (+)
RV heave, no thrills, apex beat at the 5th ICS 2 cm lateral to the
left midclavicular line, loud S1 at apex, prominent P2 at the base,
(+) gr 3/6 middiastolic rumble at apexExtremities: (+) gr 1 bipedal
edema, dorsalis pedis pulse (+2), no clubbing, no cyanosis
Fine basilar crackles = wet lungs, PULMONARY EDEMA(+) right
ventricular heaves = increase AV impulseprominent P2 at the base =
pulmonics component of second heart sound accentuated, pulmonary
hypertensionGrade 3/6 Mid diastolic rumble (apex) = disproportion
between valve orifice sizes and flow rate in mitral/tricuspid
valves; duration is index of severity of valve obstructionGrade 1
Bipedal edema = Right Heart FailureLoud S1 (apex) = position of
mitral leaflets (onset ventricular systole)*Subc nodules in severe
carditis of RFMitral facies of MSNeuro exam and oral ulcers for SLE
>>>SOAP BRAIN MD mnemonics
Duration of murmur = correlates to severity of MS S2 OS interval
= varies inversely with severity of MS
**Cardiac FindingsUsually normal or slightly enlarged
cardio-thoracic ratioStraightening of left heart borderConvexity of
left heart border 2 to enlarged atrial appendage--only in rheumatic
heart disease Small aortic knob from decreased cardiac outputDouble
density of left atrial enlargementRarely, right atrial enlargement
from tricuspid insufficiency
**The information given was not enough to diagnose the
underlying etiology.. If it is based on statistics, the etiology
would be Rheumatic Fever. The patients mother also had a heart
disease and died early indicating that the patient might have this
congenital predisposed to have rheumatic fever. Test should lse be
done to prove that it is cause by rheumatic fever or disease. These
test are the following: Antistreptolysin O Antibodies, C-Reactive
Protien, Sedimentary Rate. Congenital Mitral stenosis can also be
considered but the patient should manifest the symptoms on earlier
age. **