Embed Size (px)
Citation preview

Cardiac Arrest Cardiac Arrest Cardiac Arrest AlgorithmAlgorithmAlgorithm
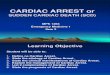
Cardiac Arrest Algorithm(Adult or Pediatric)
- Confi rm unresponsiveness and call for assistance- Confi rm cardiac arrest and begin CPR (C-A-B)
- Attach cardiac monitor/defi brillator
V-Fib or Pulseless V-Tach
Shock 1
CPR 2 minutes• IVorIOaccess
Shock 1
CPR 2 minutes• Epinephrineevery3-5min.• Consideradvancedairway
• Waveformcapnography
1
2
3
4
Shock 1
5
6
7
CPR 2 minutes• Amiodarone• Treatreversiblecauses
8
Shockable rhythm ?
YES
Shockable rhythm ?
YES
Asystole or PEA9
CPR 2 minutes• IVorIOaccess• Epinephrineevery3-5min.• Consideradvancedairway
• Waveformcapnography
10
Shockable rhythm ?
NO
CPR 2 minutes• Treatreversiblecauses
11
Shockable rhythm ?
NO YES
YES
• IfnosignsofROSC,gotobox10or11• IfROSC,gotopost-cardiacarrestcare
12
NO
NO
Go to box 5 or 7

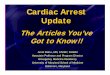
CPR 2010Matrix 2
CPR Quality Pushhard(atleast2inchesintheadult—at
leastonethirdoftheanterior–posteriordiam-eterofthechestininfants[about1½inches]andchildren[about2inches])—andfast(atleast100/min).Allowfullchestrecoilinbetweencompressions.
Switchcompressorevery2minutes.Avoidexcessiveventilation.MinimizeCPRinterruptions.
Compression-to-ventilationratio: Alladultandsingle-rescuerCPR:30:2 Two-rescuerinfantandchildCPR:15:2
BeginasynchronousCPRaftertheadvancedairwayhasbeeninserted.Useacompressionrateofatleast100/minandventilationsat8to10breaths/min(onebreathevery6to8seconds).
Waveformcapnography IfETCO
210mmHg,attempttoimprove
CPRquality
Drug Doses and Intervals
Epinephrine: Adult:1mgIV/IOevery3–5minutes Pediatric:
IV/IOdose:0.01mg/kg(0.1mL/kgof1:10,000solution)every3to5min
ETdose(ifnoIVorIO):0.1mg/kg(0.1mL/kgof1:1,000solution)
Vasopressin: Adult:40units(IV/IO)one timetoreplace
firstorseconddoseofepinephrine Pediatric:notapplicable
Amiodarone: Adult:300mginitialdose;150mgsecond
dose Pediatric:5mg/kgIVorIO;mayrepeat
twiceatsamedose;maximumof15mg/kg
Advanced Airway Insertsupraglotticairwaydeviceor
endotrachealtube. Usequantitativewaveformcapnographyto
confirmandmonitorETtubeplacement.
BeginasynchronousCPRaftertheadvancedairwayhasbeeninserted.Useacompressionrateofatleast100/minandventilationsat8to10breaths/min(onebreathevery6to8seconds).Donothyperventilate!
Defibrillation Energy
Adult: Biphasic:Manufacturerrecommendation
(120to200J);ifunknown,usemaximumavailable.Secondandsubsequentdosesshouldbeequivalent;higherdosesmaybeconsidered.
Monophasic:360J.
Pediatric: Firstshockat2J/kg;secondshockat4J/kg;
subsequentshocksatleast4J/kg. Maximumshock:10J/kgoradultenergysetting.
Reversible Causes Hypovolemia Hypoxia Hydrogenion(acidosis) Hypoglycemia(especiallyininfantsand
children) Hypokalemia/hyperkalemia Hypothermia Tensionpneumothorax Tamponade,cardiac Toxins(drugoverdose,poisoning) Thrombosis,pulmonary Thrombosis,coronary
Return of Spontaneous Circulation (ROSC)
AbruptandsustainedincreaseinETCO2
(typically40mmHg);palpablepulse. AssessBP.Obtain12-leadECG.Maintain
SpO294%. MaintainBPwithIV/IOfluidbolusor
vasopressor. Doesthepatientfollowcommands?
NoConsiderinducedhypothermia YesSTEMIorhighsuspicionofAMI
Advancedcriticalcare;coronaryreperfusion