Embed Size (px)
Citation preview

Ir. J. Med. Sc. September, 1963, pp. 415-417 lllustrated Printed in the Republic of Ireland
CARCINOMA OF THE COLON, PRESENTING AS A SUBCUTANEOUS ABSCESS
By JosEPH HUGHES, F.R.C.S.I. City General Hospital, Stoke-on-Trent
C ARCINOMA of the colon, well known to present in a variety o~ ways, may mimic almost any other intra-a'bdominal disease. Accounting for about 7 per cent. of all cancers, it is the most
commonly Observed tumour of the colon. It spreads by (1) direct extension through bowel wall and the
adjacent parts, (2) invasion of the lymph-vessels and nodes, (3) by the venous system and (4) by transperitoneal implantation, or by seeding on to raw surfaces, traumatically or surgically produced.
Direct adhesion of the affected segment of the colon to adjacent structures is important from the standpoints of respecta,bility and prog- nosis and may be due to actual malignant invasion or to inflammation. Doekerty (1958) reported that attachment of colonic carcinomas to adjacent structures, such as the uterus, urinary bladder, stomach, small intestine, gall bladder and abdominal wall was on an inflam- matory basis in about one-third only of these cases. The malignant lesion may evolve by local spread to adjacent tissues and viscera before distant metastases occur.
Invasion of the parietes by carcinoma arising in the abdominal viscera or by metastases from such lesions does not preclude, of neces- sity, radical surgical excision. I t may be possible to excise the primary growth with its parietal and visceral extensions en masse, including all macroscopic evidence of neoplasm.
The following case report describes a carcinoma of the transverse colon presenting as a subcutaneous abscess of the anterior abdominal wall, with subsequent colocutaneous fistula.
A. E. , aged 53, c o m p l a i n e d o f c o n s t a n t lower a b d o m i n a l p a i n for t h ree weeks in S e p t e m b e r 1962, w h i c h he a sc r ibed to l i f t ing a h e a v y weigh t . He h a d no t i ced r ecen t c o n s t i p a t i o n a n d loss o f weigh t .
Clinical e x a m i n a t i o n on a d m i s s i o n , r evea led a h a r d m a s s , wh ich was s l igh t ly t e n d e r below t h e umbi l i cus . T he t e m p e r a t u r e was 99"6F. a n d the re was a leucocytos ls , 14,500 cells pe r cram. The a b d o m i n a l swel l ing was asp i ra ted , odour less p u s be ing w i t h d r a w n , t h i s be ing s ter i le on cul ture . Inc i s ion was m a d e over t he swel l ing wh ich was shown to be a th ick-wal led abscess of t he a b d o m i n a l wall , w i t h o u t d e m o n s t r a b l e deep connec t ions , a n d d ra inage was i n s t i t u t ed .
A l i t t le la ter , r ecur rence o f t he swel l ing w a s not iced , fol lowed b y a faecal f is tula, in the mid- l ine on t he an t e r io r a b d o m i n a l wal l j u s t below the umbi l i cus . There were no bowel s y m p t o m s b u t cons iderable clinical de t e r io ra t ion h a d occur red w i th d e h y d r a t i o n a n d loss o f weight . A b a r i u m e n e m a was ca r r i ed ou t a n d t h e r ad io log i s t ' s r epo r t s t a t e d :
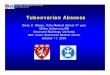
" B a r i u m flowed n o r m a l l y r o u n d to t h e c a e c u m w i t h o u t obs t ruc t ion . A t t he m i d - p o i n t of t he t r a n s v e r s e colon, t he r e was seen to be d i so rgan i sa t ion of t he m u c o s a l p a t t e r n a n d i r r egu la r i t y o f t he l umen . T h i s e x t e n d e d over a large s e g m e n t o f t he colon, a n d it is difficult to be ce r t a i n as to t he e x a c t ae t io logy of t h i s lesion.
415

416 IRISH JOURNAL OF MEDICAL SCIENCE
A. E . - - B a r i u m E n e m a C a r c k n o m a T r a n s v e r s e Colon,
The re is no ac tua l n a r r o w i n g of t h e l u m e n b u t t h i s does n o t exc lude t h e poss ib i l i t y o f n e o p l a s m in t h i s area. O n t h e whole , however , a p p e a r a n c e s are m o r e in keep ing w i t h a n i n f l a m m a t o r y lesion. T he re is also a sma l l a rea o f d ive r t i cu l i t i s in t h e pelvic colon. '~
A f t e r app rop r i a t e h y d r a t i o n a n d bowel p r epa ra t i on , ope ra t i on was p e r f o r m e d u n d e r genera l anae s the s i a . A wide e l l ip t ical inc i s ion a r o u n d t h e f i s tu la w a s m a d e a n d a m a s s i v e g r o w t h w a s f o u n d in t h e t r a n s v e r s e colon, f ixed to the an te r io r a b d o m i n a l wal l a n d i n v a d i n g t h e g r e a t e r c u r v a t u r e o f t h e s t o m a c h . T h e supe r io r a s p e c t o f t h e b l adde r w a s loosely a d h e r e n t to t h e m a s s .
A few en l a rged g l a n d s were seen in t h e mesoco lon a n d t he r e were no h e p a t i c m e t a s t a s e s . A s e g m e n t o f colon 17.5 em. long c o n t a i n i n g t h e n e o p l a s m , was resee ted , w i th i t s m e s e n t e r y a n d a t w o - t h i r d s g a s t r e c t o m y was also done , t r a n s v e r s e colon a n d s t o m a c h be ing r e m o v e d w i th t h e pa r i e t a l e x t e n s i o n of t he t u m o u r en bloc, a P o l y a - t y p e re t rocol ic a n a s t o m o s i s be ing p e r f o r m e d b e t w e e n t h e gas t r i c r e m n a n t a n d j e j u n u m . As e n d - t o - e n d a n a s t o m o s i s o f t he colon was cons ide red i nadv i sab l e a Pau l -Mikul icz ope ra t i on w a s pe r fo rmed , t he doub le -bar re l l ed e o l o s t o m y be ing b r o u g h t ou t in t he u p p e r end o f t h e incis ion. The re w a s no diff icul ty in d o s i n g t h e w o u n d wh ich hea l ed b y first i n t en t ion . Af t e r c r u s h i n g t he s p u r t h e co l o s t omy was s u b s e q u e n t l y c losed ex t r ape r i t onea l ly .
E x a m i n a t i o n of t h e r e s ec t ed s p e c i m e n showed an u l c e r a t e d c a r c i n o m a of t he colon 10 cm. • 6 cm. wide w h i c h s t r a d d l e d t h e a n t i m e s e n t e r i e border of t he colon. A probe r u n in t h r o u g h t h e f i s tu la a p p e a r e d in t h e d e p t h s of t h e ca rc inoma . The gas t r i c m u c o s a was n o t b r e a c h e d b y m a l i g n a n t in f i l t r a t ion b u t t h e m u s c l e coa t s of t h e s t o m a c h were inf i l t ra ted on macroscop ic e x a m i n a t i o n . No gross e n l a r g e m e n t of t h e l y m p h a t i c g l a n d a was found .

CARCINOMA OF THE COLON, PRESENTING AS A SUBCUTANEOUS ABSCESS 417
The pathological report s ta ted tha t microscopic examina t ion of the colonic neoplasm showed a well-differentiated adenocareinoma with m a n y mitotic figures, superficially infil trating the muscle coat of the colon.
The mucosa of the s tomach was normal, bu t the muscle coats were invaded by a poorly-differentiated carcinoma, the cells of which were arranged in sheets and trabeeulae with only slight a t t emp t at acinus formation. By using F.A.S. s ta in on the section of the s tomach it was shown tha t mue in was formed by the cells of the anaplast ic carcinoma indicat ing its colonic origin. Fur ther sections showed cont inui ty between the different- iated and undifferentiated neoplastic areas.
None of the lymph nodes examined showed evidence of metas tas i s . There was no evidence of mal ignancy in sections of the peri-fistular skin and subeutaueous t issues.
Discussion Early reports of cases of carcinoma of the colon involving the
abdominal wall ,were presented by Thurnem, Hobson, Hill, Hurley and Bidwell. Menninger and Holden (1925) and Gratiot and Nunes in 1944 described cases of carcinoma of the sigmoid, rupturing into the anterior abdominal wall and Bloodgoo~l described a case of caeeal carcinoma with similar parietal involvement.
Brunschwig (1947) described thirteen cases of in tra-abdominal car- cinoma, eight of which involved the colon, with invasion of various quadrants of the anterior abdominal wall. Resection of all macroscopic tissue was performed in one stage and this author followed the generally accepted principles of fashioning full-thickness sliding flaps in dealing with resulting defects.
Merrill, Dockerty and Waugh (1950) reviewed over 4,900 cases of colonic carcinoma over a period of 40 years at the Mayo Clinic and recorded that involvement of the abdominal wall occurred in 2.4 per cent. of this number. They reviewed a group of thirty cases with abdominal wall perforation, in which resection was performed with hope of cure. The right part of the colon held nineteen of these growths, the left portion ten and the transverse colon one. The hospital mortality was 10 per cent. and recurrent carcinoma of the anterior abdominal wall is known to have developed in one-third of the cases. Of those who recovered from the resection, 20 per cent. survived five or more years.
Shucksmith (1963) has described two cases of colonic carcinoma pre- senting with subcutaneous abscess. In both patients the carcinoma had encircled the colon and as yet no obstructive symptoms had developed.
The above case report of a lesion presenting primarily as a sub- cutaneous abscess, illustrates again a difficulty of early diagnosis of carcinoma of the colon.
Acknowledgements I wish to t h an k Mr. R. E. Norrish, Consul tant Surgeon, for permiss ion to publish
this ease-report, Dr. J. A. ]-I. Brown for the pathological report, Dr. W. E. C. Anderson for the radiological report and the radiographs and Dr. E. C. Bowcock for the photographs.
Referenece Bloodgood, J . C. (1932), Ann Surg. 95, 590. Brunschwig, A. (1947), Surg. Gy~. Obs. 84, 723. Coller, F. A. and Berry, 1:r L. (1947), J. A . M . A . 135, 1061. Dockerty, M. B. et al. Ann. Surg. 147(1) Jan . 1958. Gilehrist, R. K. and David, V. C. (1948), Surg. Gyn. Obs. 86, 359. Gratiot, J. I-I. and Nunes, A. J. (1944), Amer. J. Surg. 66, 265. Mayo, C. I-I. and Schlicke, C. P. (1942), Surg. Gyn. Obs. 74, 83. ~Ienninger, W. C. and I-Iolden, I-I. G. M. J. & Record. Aug. 5 (1925). Merrill, J . G., Docke~y, 1VI. B., Waugh, J. M. (1950), Surgery. 28, 662. Sugarbaker, E. D. (1946), Ann. Surg. 123, 1036. Shucksmith, It . (1963), Brit. J. Surg. No. 223, 514.