Embed Size (px)
DESCRIPTION
Citation preview

429
From theArchives of the AFIP
This article meets the
criteriafor 1.0 credit
hour in Category 1 of
theAMA Physician’s
Recognition Award.
To obtain credit, see
the questionnaire at
the end oftbe article.
Bronchogemc Carcinoma:Radiologic-Pathologic Correlation1Melissa L. Rosado-de-Christenson, Lt Col, USAF, MC #{149}Philip A. Templeton, MD
CesarA. Moran, Maf, USAF, MC
Bronchogenic carcinoma is the leading cause of death from cancer in men
and women in the United States. Although the cause ofthis malignancy is
probably multifactorial, approximately 85% of lung cancer deaths are attrib-
utable to cigarette smoking. Patients may present with symptoms of airway
obstruction caused by central tumors, symptoms related to direct tumor in-
vasion of surrounding structures, or symptoms produced by distant metasta-
ses. There are four major cell types: adenocarcinoma, squamous cell carci-
noma, undifferentiated large cell carcinoma, and small cell carcinoma.
Adenocarcinoma and undifferentiated large cell carcinoma are generally pe-
ripheral lesions manifesting as solitary nodules or masses, whereas squa-
mous cell carcinoma and small cell carcinoma are typically central and may
manifest as hilar masses, atelectasis, or pneumonia. The prognosis for pa-
tients with bronchogenic carcinoma is poor, with an overall 5-year survival
of 10%-15%. In general, patients with squamous cell carcinoma have the
best prognosis, those with adenocarcinoma and undifferentiated large cell
carcinoma have an intermediate prognosis, and those with small cell carci-
noma have the worst prognosis.
U INTRODUCTIONThe term “bronchogenic carcinoma” is synonymous with the terms “lung cancer”
and “lung carcinoma. “ Its use has been criticized, since not all of these tumors onigi-
Abbreviations: H-E hematoxylin, PA = posteroanterior
Index terms: Adenocarcinoma, 60.3212 #{149}Lung neoplasms, 60.31 1, 60.320, 60.3214, 60.32 16
RadioGraphlcs 1994; 14:429-446
� From the Departments of Radiologic Pathology (M.L.R.) and Pulmonary and Mediastinal Pathology (CAM.), Armed
Forces Institute of Pathology, Bldg 54, Rm M.121, Alaska and Fern Sts, Washington, DC 20306-6000; the Department of
Radiology and Nuclear Medicine, Uniformed Services University ofthe Health Sciences, Bethesda, Md (M.L.R.); and the
Department of Radiology, University of Maryland Medical System, Baltimore (PAT.). Received October 25, 1993; revi.
sion requested November 12 and received December 15; accepted December 16. Address reprint requeststoM.L.R.
The opinions and assertions contained herein are the private views of the authors and are not to be construed as official
or as reflecting the views of the Department of the Air Force or the Department of Defense.
EdUor�s note-This material was previously presented at the American College of Radiology Categorical Course on Im.
agingofCancers on September 12, 1992. Figures lb. 3, 4a. 8c, 11, 14, 16b, 18, and 19b are reprinted, with permission,
from a chapter in an ACR syllabus (Rosado.de-Christenson ML, Moran CA. Primary lung cancer: pathology and present.
ing features. In: Bragg DG, Thompson WM, eds. Categorical course on imaging of cancers: diagnosis, staging, and fol.
low-up challenges. ACR 1992; 1-8).
C RSNA, 1994

430 U Continuing Education Volume 14 Number 2
nate in the bronchial epithelium. However,
the term is used by some pathologists to refer
to those primary malignant neoplasms of the
lung related to exposure to inhaled carcino-
gens, mainly cigarette smoke (1). We use this
term throughout this article.
Bronchogenic carcinoma is a disease of
great importance in both the United States
and the rest ofthe industrialized world. In the
United States, the number of deaths from this
malignancy increased by 440% between 1957-
1959 and 1987-1989 (2). Bronchogenic canci-
noma has become the leading cause of mor-
tality resulting from cancer in the United
States, the most common malignancy of men
in the world, and the leading cause of mortal-
ity from cancer in male patients in 35 differ-
ent countries (3). Bronchogenic carcinoma isthe sixth leading cancer in women worldwide,
and in 1987 it surpassed breast cancer as
the most common fatal malignancy of U.S.
women, accounting for 2 1 % of cancer-related
deaths in female patients (3-6). According to
American Cancer Society estimates, there
were 161,000 new cases and 143,000 deaths
from lung cancer in 1991 in the United States
(7,8). It is estimated that there will be
170,000 new cases ofbnonchogenic canci-
noma in 1993, with a projected male-female
ratioofl.4:1 (4).
Cigarette smoking is the most important
causative factor in the development of bron-
chogenic carcinoma, with approximately
80%-90% of deaths directly attributable to
tobacco use. The risk is related to the number
of cigarettes smoked, depth of inhalation, and
age at which smoking began (6,8). Passive
smoking by indirect exposure is also thought
to play a role and may account for 25% of
bronchogenic carcinomas in nonsmokers
(3,6). Cessation of smoking can reduce the
risk to approach that of the nonsmokingpopulation after a period of 10-20 years (6).
Radon gas may be the second leading con-
tnibuton to lung cancer and may be respon-sible for up to 20,000 deaths per year (9).Other important epidemiologic factors in-
elude occupational exposure to asbestos, ra-
diation exposure for uranium miners, expo-sure to other carcinogens, and concomitant
lung disease including chronic pulmonary
scans and pulmonary fibrosis (1,6,10).
U CLINICAL PRESENTATIONPatients with bronchogenic carcinoma are
typically men in the 6th or 7th decade of life
( 1 1). They commonly present with symptoms
produced by the primary tumor. Central tu-
mons may cause coughing, wheezing, hemop-
tysis, and pneumonia. Although a rare clinical
manifestation, diffuse lung involvement by
bronchioloalveolar carcinoma may produce
bronchorrhca, the expectoration of large
amounts ofmucus (5). With direct invasion of
local extnapulmonary structures such as the
panietal pleura, chest wall, and mediastinal
structures, patients may present with pleuritic
on local chest pain, dyspnea or cough, the
Pancoast syndrome, the superior vena cava
syndrome, on hoarseness (5, 1 1) . Patients may
also present with symptoms produced by dis-
tant metastases, typically to the central ncr-
vous system, bone, liver, or adrenal glands. In
addition, patients may present with pananeo-
plastic syndromes, that is, systemic manifesta-
tions of the primary tumor unrelated to dis-
tant metastases (5, 1 1, 12). These may include
cachexia of malignancy, clubbing and hyper-
trophic osteoarthropathy, nonbacterial throm-
boric endocanditis, migratory thrombophlebi-
tis, and various neunologic and cutaneous
syndromes. Paraneoplastic syndromes may
also be secondary to secretion of ectopic hon.
mones by tumor cells and may result in hypcr-
calcemia, the syndrome of inappropriate se-
cretion of antidiunctic hormone, Cushing
syndrome from corticotropin secretion, gync-
comastia, and acromegaly (5, 1 1 , 12). Approxi-
mately 10% of patients, usually those with
peripheral tumors, have no symptoms (1 1).
U HISTOLOGIC CLASSIFICATIONThe World Health Organization histologic
classification of lung tumors is based on mor-
phologic features identified with light micros-
copy. Primary tumors of the lung are classified
on the basis of their best differentiated areas
and are graded on the basis of their least dif-
ferentiated areas (13). Four cell types account
for oven 95% ofall primary lung neoplasms:
adenocarcinoma, squamous cell carcinoma,
undifferentiated large cell carcinoma, and
small cell carcinoma (14). Mixtures of these
cell types may occur within the same primaryneoplasm. Adenosquamous carcinoma (com-
bined adenocarcinoma and squamous cell
carcinoma) is the most common of these mul-
tidiffcrcntiatcd tumors. Combinations of
small cell and squamous cell carcinoma as
well as small cell and adenocarcinoma have
also been described (1,14-17).
A practical classification based on the treat-ment options for bronchogenic carcinoma
divides the histologic types into non-small
cell and small cell carcinomas. In fact, therapid growth and early metastatic spread of

March 1994 Rosado-de-Christenson et al U RadioGraphics U 431
, . . . .5.; � -
,:( , .. ., - . � . ;� .� I � � � . ..__.4 I.,
�. L .. . ‘�. . - -.. � ..�‘:� � � � � .- , ‘-��‘� ,
� . , :‘�‘ - ��t’ �: . ‘ . , � ,
� f S #{149}� �
� � �‘�* ��::� � � ,� � � #{149}#{149}�� - ,�l- � �
�?#{149},,i � ,‘ ‘ f� � y �- ,.: � �-�-i�;�
*� ,4� � ,. 4J#{248}’�S
� :�
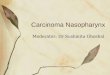
Figure 1. Adenocarcinoma.(a) High-power photomicrograph
(original magnification, x 1 50; he-
matoxylin-eosin [ H-E I stain) shows
a well-differentiated adenocarci-
noma characterized by the forma-
tion ofglands and papillary struc-
tunes (*). Note the desmoplastic
reaction and fibrosis that surrounds
the glandular elements (f). (b) Cut
surface of an adenocarcinoma of the
night lower lobe shows a well-mar-ginated, lobulated, subpleural, pe-
nipheral lung mass.
small cell carcinoma, as well as its responsive-
ness to chemotherapy and radiation therapy
are unique features that distinguish it from
the non-small cell carcinomas (4, 18). Never-
theless, to describe the varied nadiologic
manifestations and pathologic features of
bronchogenic carcinomas, we discuss each of
the four cell types separately.
. AdenocarcinomaAdenocarcinoma is the most frequently diag-
nosed cell type and accounts for approxi-
mately 50% of all bronchogenic carcinomas
(4) . The increasing frequency of adenocarci-
noma and the decrease in the diagnosis of
squamous cell carcinoma have been observed
since the middle 1960s and are believed to
represent an actual change in the biologic
features of these cell types rather than a re-
flection of modern changes in diagnostic cni-tenia. Adenocancinoma is also the most corn-
mon cell type seen in women and nonsmokers.Although it is weakly associated with cigarette
smoking, most patients with adenocarcinomahave a history of tobacco use. Adenocarcinoma
has also been associated with concomitant
lung diseases that produce focal or diffuse
fibrosis, including tuberculosis, pulmonary
infarction, chronic interstitial pneumonitis
and fibrosis, sclenoderma, bnonchiectasis,
chronic pneumonia, and honeycomb lung
(1,10,13,14,17,19).
Microscopically, adcnocarcinomas arc char-
actenized by the formation of glands and pap-
illary structures (Fig la). The neoplastic cells
have round to oval nuclei, prominent flu-
cleoli, and moderate amounts of cytoplasm.
Histochemical stains (mucicarmine) are useful
for demonstration of the characteristic intra-
and extracellulan mucosubstance (14,17).
These tumors have been associated with lung
scars. The degree of scarring can be extensive,
suggesting a preexistent scar and giving rise to
the concept of ‘ ‘scar carcinoma. ‘ ‘ Although a
small number of adenocarcinomas probably
arise in scar tissue, there is evidence that in
the majority of cases the fibrosis on scar ne-
suits from a desmoplastic host reaction in-
cited by the tumor (14,15,17,20,21) (Fig la).

b. C.
432 U Continuing Education Volume 14 Number 2
Figure 2. Adenocancinoma in an asymptomatic58-year-old male smoker with a radiographic ab-
normality found incidentally on a preoperative
radiograph obtained before cataract surgery.
(a) Posteroantenior (PA) chest radiograph shows a
lobulated 1.5-cm solitary nodule (arrow) in theright upper lobe overlying the first anterior rib.
(b) Chest computed tomographic (CT) scan (lung
window) shows large bullae surrounding a well-
marginated, lobulated soft-tissue nodule. (c) Cut
surface of the tumor demonstrates the nodule (ar-
rowhead) within the collapsed bullae. Histologic
evaluation revealed a poorly differentiated adeno-
carcinoma with central fibrosis.
On gross examination, adenocarcinoma
typically manifests as a peripheral, subpleural
nodule or mass that usually results in retrac-
tion of the overlying pleura. Like most lung
cancers, adenocarcinoma typically affects the
upper lobes and exhibits an expansile (so-called hilic) growth pattern that destroys and
displaces the adjacent lung panenchyma. The
borders of the tumor may be rounded, lobu-
lated, or poorly defined. Lobulation reflects
the histologic heterogeneity oflung cancer
and results from differential growth rates in
different areas within the tumor (Fig ib). Ill-
defined bonders may relate to invasion of the
adjacent lung, fibrosis, or interstitial edema
(22-24).The typical radiologic manifestation of ad-
enocancinoma is a solitary pulmonary nodule
on mass that may have well-manginated, lobu-
lated, irregular, or poorly defined borders
(Figs 2, 3). Peripheral adenocancinomas may
directly invade the pleura and grow cincum-
fenentially around the lung, thus mimicking
diffuse malignant mesothelioma on initial cx-
amination (19). Thin-section CT ofsmall (<2
cm) peripheral carcinomas manifesting as soli-
tary pulmonary nodules may demonstrate airbronchograms or air bnonchiolograms in 65%
of cases. This finding may help differentiate
these bronchogenic carcinomas from benign
lung tumors (25).
CT can also demonstrate chest wall invasion
by peripheral pulmonary lesions (Fig 3). How-even, absence of direct evidence of extrapul-monary involvement does not necessarily cx-
dude it (26). CT is less accurate than the
clinical presence of local chest pain in the cx-
clusion of chest wall invasion. Magnetic reso-
nance (MR) imaging may allow the distinction
of tumor from adjacent chest wall muscula-
ture and may improve the accuracy of CT inthe demonstration of chest wall invasion.

a. b.
a.Figure 4. Bronchioboalveolar carcinoma. (a) High-power photomicrognaph (original magnification, x 150;H-E stain) demonstrates the lepidic growth pattern. Columnar peglike cells line the alveolar walls. The pul-monary interstitium (arrows) remains intact. (b) Cut surface demonstrates a heterogeneous parenchymallesion that resembles a consolidation.
March 1994 Rosado-de-Christenson et al U RadioGraphics U 433
Figure 3. Adenocarcinoma in a 41-year-old man with right shoulder pain for several months. (a) Apical br-dotic chest radiograph demonstrates a right apical mass with poorly marginated borders. (b) Chest CT scan
(lung window) shows a homogeneous peripheral right upper lobe mass with irregular borders. There is tu-mon involvement of a posterior rib (arrow). An en bloc resection of the right upper lobe and the involvedchest wall was performed.
Chest wall involvement is best seen as in-
creased signal intensity on T2-weighted MR
images (27).
Lung cancer has been reported to occur in
close relation to preexisting bullac and maymanifest as a nodular opacity within the bulla
(Fig 2), thickening ofthe bulla wall, change in
the size of the bulla, or spontaneous pneumo-
thorax (28). In the study by Tsutsui et al (28),12 of 25 lung cancers associated with bullac
were adenocarcinomas.
Bronchioloalveolar carcinoma represents a
subtype of adenocancinoma that accounts for
approximately 2%-6% of all lung neoplasms,
although its frequency may be increasing
(14). The tumor is characterized by wdll-dif-
fenentiated histologic features and is typicallylocated peripherally beyond a recognizable
bronchus. Microscopically, these tumors cx-
hibit the so-called lepidic pattern of growth,
which is characterized by cuboidal or colum-
nan peglike cells that line the walls ofdistal air
spaces. The pulmonary interstitium is re-
spected and serves as a ‘ ‘scaffolding’ ‘ for tu-
mon growth (24) (Fig 4). Bronchioloalveolar

5a. Sb.
6a. 6b.
434 U Continuing Education Volume 14 Number 2
Figures 5, 6. (5) Bronchioloalveolar carcinoma in a 56-year old man with no symptoms. (a) PA chest ra-diograph demonstrates an ill-defined peripheral nodule in the left lower lung zone. (b) Chest CT scan dem-
onstrates a subpleural lobulated solitary pulmonary nodule in the left lower lobe. A 2-cm bronchioboalveolarcarcinoma was found at surgery. (6) Bronchioloalveolar carcinoma in a 39-year-old man with blood-tinged
sputum and pleuritic chest pain. (a) PA chest radiograph demonstrates a cavitary consolidation of the lingu-
bar segment of the left upper lobe. (b) Chest CT scan (lung window) demonstrates a cavity within the paren-
chymal consolidation. Air bronchograms are seen near the cavity. At surgery, an 8.4 x 6.4 x 3.5-cm cavitary
bronchioloalveolar carcinoma with direct extension to the visceral pleura was found. Although radiologic
studies may show a pneumonic pattern, the most common manifestation of bnonchioboabveolar carcinoma is
that ofa solitary pulmonary nodule.
carcinomas may exhibit tracheobronchial dis-
semination as neoplastic cells detach from the
primary tumor and attach to alveolar septa
elsewhere in the lung, commencing growth in
a new location. The cells commonly produce
abundant mucus (29-31).
The most common nadiologic manifestation
of the bronchioloalvcolan subtype of adeno-
carcinoma is that of a well-circumscribed pe-niphenal solitary pulmonary nodule or mass
(31) (Fig 5). Cavitation, an infrequent finding
in adenocarcinomas, may be seen in bron-
chioloalvcolan carcinoma (Fig 6). In the study
by Theros (24), which reviewed 1,267 periph-
crab primary neoplasms of the lung, bnonchio-

a. b.
�“ � ‘V . �
March 1994 Rosado-de-Christenson et al U RadioGraphics U 435
Figure 7. Bronchioboalveolar carcinoma in a 35-year-old woman with a chronic pulmonary consolidation.
(a) PA chest radiograph shows a right middle lobe consolidation. (b) PA chest radiograph obtained 1 #{189}yearslater shows bibasilar multinodular consolidations with air bronchograms, which represented tracheobron-chial tumor dissemination. The surgical clips over the right lower lung were placed during the initial biopsy.
loalveolar carcinoma was the second most
common cell type (after squamous cell carci-noma) to radiographically demonstrate cavita-
tion. The lepidic pattern of tumor growth may
result in lesions of heterogeneous radiologic
opacity, with air bronchograms and poorly
manginated borders mimicking pneumonia
(29-31) (Figs 6, 7a). Less commonly, patternsof multiple nodules (Fig 7) or extensive con-
solidation involving one on more lobes may be
seen (1 1,29-32). High-resolution CT may
demonstrate air attenuation and pseudocavi-
tation within the nodules corresponding to
small bronchi and cystic spaces (33). Patientswith extensive consolidation on multifocal
disease have a poor prognosis (29-31).
. Squamous Cell CarcinomaSquamous cell carcinoma accounts for ap-
proximately one-third of all bronchogenic can-
cinomas (4). This cell type is strongly associ-
ated with cigarette smoking. Its histogenesis is
thought to relate to chronic inflammation andinjury of the bronchial epithelium, which can
result in squamous metaplasia. This may sub-
sequently progress to dysplasia, carcinoma
in situ, and ultimately invasive carcinoma
(1,5, 10). Squamous cell carcinoma is the only
cell type in which in situ changes are necog-
nized, and thus it may be diagnosed with cyto-
logic examination of the sputum of affected
patients. Therefore, it is the most common
cell type diagnosed when it is radiologically
occult (1,14,17). Unfortunately, less than 1%
of bronchogenic carcinomas are detected at
this stage (4). Squamous cell carcinoma is also
the most common cell type associated withhypercalccmia. The hypercalcemia is thought
to be caused by a parathyroid hormone-like
substance produced by the tumor (17).

�,
�*, �
), :,�,.�:.
.�v � ,�-,
.-. . -�-,..\ \:
,#{149}�� . ,
a. b.
C. d.
436 U Continuing Education Volume 14 Number 2
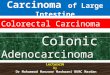
Figure 8. Squamous cell carcinoma. (a) High-power photomicrograph (original magnification, X 150; H-Estain) shows neoplastic cells with moderate amounts of eosinophilic cytoplasm. Well-differentiated keratiniz-
ing areas (arrowheads) are seen intermixed with the malignant cells. (b) Gross specimen shows an irregular,
exophytic, endobronchial mucosal tumor that partially obstructs the lumen of the main stem bronchus. The
tumor invaded the bronchial wall and the adjacent lung parenchyma. Scale is in centimeters. Linear chest
tomogram (C) and bronchogram (d) show the characteristic growth pattern of these tumors in a patient with
a squamous cell carcinoma of the night main stem bronchus. Note the irregular narrowing (arrow) of the
bronchial lumen, which may result in postobstructive pneumonia or atelc�sis.
� � � � � ., .
‘ � #J%� � �
q’S�,#{149} � � ., ,U-..’�:‘� ‘ � . �
� d?t.pj. 1�i � �;. -.�. 4 , c’.:�:.c:� . ‘� ‘. , .. �
.- .. . #{149}� *.� :‘ l� ,,�.. ‘. .4-..,..’ � -. ‘,
L��#{149} ,
� � ‘ � I ,,,�, �, � . b
. ‘I ..- ‘ � - - ..� .. :‘ �‘ � ‘A” �
Microscopically, squamous cell carcinoma is
characterized by the presence of intercellular
bridges (fine parallel lines between the bor-
dens ofcontiguous cells), individual cell kera-tinization (characterized by intense eosino-
philia ofindividual cells), and the formation
of keratin pearls (laminated whorls of cosino-
philic cells) in well-differentiated tumors
(13,14,16,17,19) (Fig 8a). The term “squa-

a. b.
March 1994 Rosado-de-Christenson et al U RadioGrapbics U 437
Figure 9. Squamous cell carcinoma in a 57-year-old man. PA (a) and lateral (b) chest radiographs demon-
strate a complete consolidation of the right upper lobe. At bronchoscopy, an endobronchial tumor of the
r � t main stem bronchus was identified.
mous’ ‘ means flat and refers to the flattened
appearance of the tumor cells. Because squa-
mous cell carcinoma mimics the differentia-
tion of the epidermis by producing keratin, it
is also called epidermoid carcinoma (1). Squa-
mous cell carcinoma incites a strong inflam-
matory host response with resultant adhe-
sions, across which the tumor can invade
adjacent structures (15).
Squamous cell carcinomas are centrally lo-cated within the main, lobar, and segmental
bronchi in approximately two-thirds of cases.
On gross examination, these endobronchial
tumors range from a focal irregular growth in
the bronchial mucosa to a polypoid mass that
obstructs on narrows the bronchial lumen(1,14,34) (Fig 8b). Virtually all central squa-
mous cell carcinomas can be identified on
endoscopic examination (13, 15). These tu-
mors commonly grow through the bronchial
wall, subsequently invading adjacent lymph
nodes or lung parenchyma (1 1,16). Central
necrosis is very common and may result in
cavitation (1 1).
The typical radiologic manifestations of
central squamous cell carcinomas are the ne-
suIt of the total or partial bronchial obstruc-
tion that these endoluminal lesions produce
(Fig 8c, 8d). Bronchial obstruction may ne-
suit in a postobstructive pneumonia (Fig 9).
Therefore, all cases of pneumonia occurring
in adults should be followed to complete na-
diologic resolution to exclude the presence
of a causative endobronchial lesion such asbronchogenic carcinoma.
Lobar or complete lung atelectasis may also
result from these central endobronchial Ic-
sions (Figs 10, 11). Because ofthe presence
of a central mass, the lobe is unable to corn-
pletely collapse and a bulging contour of the
atelectatic lung may be produced by the pni-
mary tumor, giving rise to the radiographic “S
sign of Golden” (32). Early lesions may mani-
fest with lobular thickening of the bronchial
wall (32,35). Larger tumors may produce a
hilar on penihilan mass (1 1). Approximately
one-third of squamous cell carcinomas are
peripheral and appear as solitary pulmonarynodules or masses (14).
Squamous cell carcinoma is the most corn-
mon cell type to produce cavitation, which
occurs in approximately 10% ofcases (10).
The inner wall of the cavity is typically thick
and irregular (1 1) (Fig 12). Peripheral squa-mous cell carcinoma is also the most common
cell type to cause the Pancoast syndrome,

lOa lOb.
1 la. 1 lb.
llc.
438 U Continuing Education Volume 14 Number 2

Figure 12. Squamous cell carcinoma in a 72-year-old manwith left arm pain, chest pain, and increasing dyspnea.
(a) PA chest radiograph demonstrates a large rounded cavi-tary mass with an air-fluid level in the superior segment of
the left lower lobe. Note the nodular, irregular contour ofthe inner wall of the cavity. (b) Contrast-enhanced chest CT
scan (mediastinal window) demonstrates the air-fluid level
within the lesion and the irregular aspect of its inner wall.
(c) Cut surface ofthe resected left lower lobe demonstrates
the cavitary neoplasm. Scale is in centimeters.
C.
�-- g
March 1994 Rosado-de-Christenson et al U RadioGraphics U 439
4Figures 10, 11. (10) Squamous cell carcinoma in a 63-year-old woman with dysphagia and weight loss.
(a) Frontal chest radiograph demonstrates opacification of the left hemithorax and ipsilateral mediastinalshift consistent with complete atelectasis of the left lung. Lack of visualization of the left main stem bronchus
suggests central occlusion. (b) Contrast-enhanced chest CT scan (mediastinal window) demonstrates a soft-
tissue mass (in), which narrowed and obstructed the left main stem bronchus, left lung atebectasis, and left
pleural effusion. At bronchoscopy, a circumferential, friable obstructing endobronchial lesion was found.
(11) Squamous cell carcinoma in a 62-year-old man with left shoulder pain. (a, b) Thin-section chest CT
scans (lung window) show an endobronchial nodule (arrow in a) within the right lower lobe bronchus.
There is involvement of the adjacent lung parenchyma with associated volume loss of the night lower lobe.
Note the bobulated mass (arrowhead in b) that displaces the major fissure. (C) Gross specimen of the re-
sected right lower lobe shows the endobronchial component of the tumor (arrow) and the large parenchy-
mal mass (m).

C- d.
440 U Continuing Education Volume 14 Number 2
Figure 13. Adenosquamous carcinoma in a 68-year-old man with chest wall pain on the night side. (a) PAchest radiograph shows a right apical mass with associated destruction of the posterior aspects of the first
and second ribs. A large soft-tissue component is also present in the supraclavicular region. (b) Contrast-
enhanced chest CT scan demonstrates a large apical soft-tissue mass that destroys the adjacent ribs and di-rectly invades the right axillary region. At surgery, a poorly differentiated adenosquamous carcinoma was
found. (c) Coronal MR image (repetition time was 600 msec; echo time was 20 msec 1600/201) from another
patient with a Pancoast tumor demonstrates extrapulmonary invasion of the tumor into the soft tissues of the
chest wall (arrow). The roots ofthe brachial plexus are well visualized and are not involved by the tumor
(arrowhead). (Reproduced, with permission, from reference 27.) (d) Gross specimen ofa Pancoast tumor
shows that the peripheral apical tumor grows through the visceral pleura and has a large extrapulmonarycomponent.
characterized clinically by pain or atrophy of
muscles of the ipsilatenal upper extremity due
to involvement of the lower brachial plexus,
and Horner syndrome due to involvement of
the sympathetic chain and the stellate gan-
gI ion (5). Pancoast tumors account for less
than 3% ofall bronchogenic carcinomas (4).
These lesions may manifest radiologically as
apical masses, apical pleural thickening, or
asymmetric apical pleural thickening and may
be associated with bone destruction and soft-
tissue invasion (11,36,37) (Fig l3a).
CT may demonstrate central tumors as amass within the airway, narrowing of the air-
way lumen, on focal peribronchial thickening
(35) (Figs lOa, 1 la). CT may also help in dis-
tinguishing the primary tumor from adjacent
atelectatic or consolidated lung. The tumor
may produce a bulge in the involved atelec-
tatic lung, which suggests the presence of an
underlying mass (Fig 1 ib). Differential con-

March 1994 Rosado-de-Christenson et al U RadioGraphics U 441
trast material enhancement of tumor versus
collapsed lung may be seen. CT also allows
the evaluation of the mediastinum and adja-
cent structures for staging (19) (Fig 13b). Di-rect coronal and sagittal MR images are supe-
nor to CT scans in the evaluation of Pancoast
tumors because they allow visualization of the
anatomy of the adjacent chest wall. The sub-
clavian artery, brachial plexus, vertebral bod-
ics, and spinal canal can be visualized andassessed for tumor involvement. Ti-weighted
coronal and sagittal MR images arc a useful
adjunct to CT scans, resulting in improved
diagnostic accuracy in the preoperative evalu-
ation of patients with Pancoast tumors (1 1,
38-40) (Fig 13c).
. Undifferentiated Large CellCarcinomaUndifferentiated large cell carcinoma nepre-
sents less than 5% of all bronchogenic carci-
nomas (4). These tumors grow rapidly and
metastasize early. They are strongly associated
with smoking.
With bight microscopy, the tumor cells ap-
pear large; have abundant cytoplasm, largenuclei, and prominent nucleoli; and grow in
uniform sheets (Fig 14). The histologic diag-
nosis of undifferentiated large cell carcinomais one of exclusion, given only to primary ma-
lignant neoplasms of the lung that lack fea-
tunes of squamous, glandular, on small cell
differentiation (1,14,34,41). The frequency of
Figure 14. Undifferentiated large cell carcinoma.
High-power photomicrograph (original magnifica-tion, X 150; H-E stain) shows large tumor cells with
large nuclei, prominent nucleoli, and a moderate
amount of cytoplasm. There are no microscopic fea-
tures ofdifferentiation for the other three cell types.
this diagnosis decreases when large amounts
of tissue arc available for histologic evaluation(17). With ultrastructural analysis, approxi-
matcly 80% of undifferentiated large cell car-
cinomas previously diagnosed with light mi-
croscopy demonstrate electron microscopic
features of adenocarcinoma; features of squa-
mous cell carcinoma and other tumors are
seen in many ofthc remaining 20% (14,34).
Giant cell carcinoma is a subtype of undif-
fercntiatcd large cell carcinoma composed of
pleomorphic giant cells with bizarre shapes.
Approximately 40% of the cells are multi-
nucleated. Red and white blood cells are typi.
cally seen within the cytoplasm of the giant
tumor cells. Giant cell carcinoma has a pan-
ticularly aggressive behavior and a very poor
prognosis (14, 16, 19,34).
Undifferentiated large cell carcinomas are
usually bulky tumors typically greaten than 3cm in diameter. They are soft and have large
areas of necrosis. Undifferentiated lange cell
carcinomas are typically located in the lung
periphery, but central lesions arc not uncom-mon. Involvement oflange bronchi is seen in
approximately 50% ofcentral lesions (1,16).
The typical nadiologic appearance of these
neoplasms is that of a large peripheral lung
mass (Figs 15, 16).

16a. 16b.
Figures 15, 16. (15) Undifferentiated large cell carcinoma in a 61-year-old woman with blood-streakedsputum and weight loss. (a) PA chest radiograph demonstrates a large peripheral mass of the left upper lobe,
which abuts the pleural surface and has a bobubated contour. (b) Cut surface of the gross specimen demon-
strates a 7-cm tumor that extends to the pleural surface. (16) Undifferentiated large cell carcinoma in a
57-year-old man with weight loss, orthopnea, and a painful palpable mass of the anterior chest wall on the
left side. (a) Contrast-enhanced chest CT scan (mediastinal window) demonstrates a large mass of heteroge-
neoUs attenuation, which produces mass effect on the mediastinal structures. (b) Cut surface of the neoplasm
shows a large central area of necrosis, which corresponds to the areas of central decreased attenuation seen
442 U Continuing Education Volume 14 Number 2
with CT. At surgery. chest wall tumor invasion was seen.
. Small Cell CarcinomaSmall cell carcinoma accounts for approxi-
mately 15% ofbronchogenic carcinomas (4).
Small cell carcinoma is strongly associated
with cigarette smoking. It is a rapidly growing
neoplasm characterized by early and wide-
spread metastases (1,15,19).
Microscopically, small cell carcinoma is
characterized by small, uniform, oval cellswith scant cytoplasm. The nuclei are round on
oval with a stippled chromatin and absent
nucleoli. The neoplastic cells may be arranged
in cords, clusters, or sheets (Fig 17a). Thereare numerous mitoses and large areas of ne-
crosis. An extensive crushing artifact is fre-
quently seen in bronchial biopsy specimens.
The crush artifact probably results from the
scant tumor stroma and the lack of desmo-
plastic reaction in these lesions (1,11,14,17,
19,34).
Although some have used the term synony-
mously with small cell carcinoma, ‘ ‘oat cell
carcinoma’ ‘ is actually a morphologic subtype
of small cell carcinoma characterized by uni-
form small cells with small dense hypcrchro-

March 1994 Rosado-de-Christenson et al U RadioGraphics U 443
matic nuclei, absent nucleoli, and scant cyto-
plasm (19). The histologic features ofoat cell
carcinoma may be secondary to generalized
tissue ischemia, since it is typically described
in autopsy specimens. Promptly fixed biopsy
material usually does not exhibit these fea-
tunes (19). Approximately 20% ofsmall cell
carcinomas also contain elements of non-
small cell histologic types. The most frequent
coexistent histologic type is squamous cell
carcinoma (19).Small cell carcinomas together with carci-
noid tumors have been classified as ‘ ‘ neuro-
endocrine neoplasms’ ‘ of the lung. The cells
in small cell carcinoma may contain neurose-
cretony (dense cone) granules similar to those
found in bronchial cancinoid. These tumors
arc thought to be related to the amine precun-
son uptake and decanboxylase cells of the
bronchial epithelium, which has led to their
classification as Kulchitsky cell carcinomas(42,43). The postulated neural crest origin of
these cells is no longer widely accepted. In-
stead, it is believed that these tumors are de-
nived from primitive endodermal cells that
can differentiate into neuroendocrinc cells
(17). Small cell carcinoma is the most corn-
mon cell type to cause a clinical hormone syn-
drome by secreting ectopic hormones. Themost commonly seen syndromes are Cushing
syndrome and the inappropriate secretion of
antidiuretic hormone (12,14,16,43).
Approximately 90% of small cell carcinomas
arc located centrally within lobar and main
stem bronchi. Although these tumors anise in
the bronchial mucosa, they tend to grow inthe submucosa and subsequently invade the
penibronchial connective tissues, maintaining
a smooth-appearing mucosal surface on endo-
scopic examination. The tumor is bulky and
soft, with extensive necrosis and hemorrhage.
Although extrinsic bronchial compressionmay occur, endobronchial lesions arc rare
(1 1 , 16). Small cell carcinoma produces littlehost response and can spread easily through
tissues, invade adjacent structures and lymph
nodes, and disseminate along lymphatic
routes (Fig 17b). Peripheral lesions are rare
and are usually associated with regional
spread to hilan and mediastinal lymph nodes
(17).

l8a. 18b.
444 U Continuing Education Volume 14 Number 2
19a. 19b.
Figures 18, 19. (18) Small cell carcinoma in a 41-year-old woman with persistent cough and weight loss.(a) PA chest radiograph shows a lobulated right hilar mass. (b) Frontal linear chest tomogram shows smooth
narrowing of the bronchus intermedius due to extrinsic compression by the hilar mass, which represented
lymph node metastases from small cell carcinoma. (19) Small cell carcinoma in a 72-year-old man with a his-
tory ofdyspnea. (a) Chest CT scan demonstrates a spiculated nodule in the right upper lobe. (b) Contrast-
enhanced chest CT scan (mediastinal window) shows massive mediastinal lymphadenopathy secondary tolymph node metastases.
The typical radiographic manifestation of
small cell carcinoma is a hilar or penihilar
mass that is frequently associated with mcdi-
astinal widening (Fig 18). The mass may be
caused by the primary tumor, metastases to
hilar lymph nodes, or a combination of both.
The primary tumor may not be evident, and
nodal enlargement may be the dominant ab-
normality on radiographs. Rarely, small cell
carcinoma may manifest as a solitary pulmo-
nary nodule or mass (1 1) (Fig 19a).
CT depicts evidence of mediastinal lymph
node involvement in the majority of cases.The degree of mediastinal involvement is typi-
cally greater than is evident on chest radio-
graphs. CT is particularly helpful in the evalu-
ation of disease in the anterior mediastinum,
the subcarinal region, and the penicardium.
Narrowing and displacement of major vessels
and bronchi, pleural effusions, unsuspected
panenchymal lesions, direct mcdiastinal inva-
sion, and evidence of metastatic disease may
also be seen (Figs 19, 20). Postobstructive
pneumonia and atelectasis have also been ob-
served (44). Small cell carcinoma is the most
common primary lung cancer causing superior
vena cava obstruction secondary to extrinsic
vascular compression by the tumor, endolu-
minal thrombosis, on invasion (5,32,43) (Fig
20).

a. b.
March 1994 Rosado-de-Christenson et al U RadioGraphics U 445
Figure 20. Small cell carcinoma in a 69-year-old man with a history of neck swelling, malaise, and mild dys-pnea on exertion. (a) Frontal chest radiograph shows a large multilobular mass of the right hilus and medias-tinum, with mass effect on the mediastinal structures. (b) Contrast-enhanced chest CT scan (mediastinal
window) demonstrates tumor involvement of the mediastinum. There is lack of visualization of the superior
vena cava secondary to occlusion by the tumor. Multiple collateral vessels (arrowheads) are visualized in the
superior mediastinum and chest wall.
U THERAPY AND PROGNOSISThe curative therapy for bronchogenic carci-
noma is complete surgical resection of the
primary tumor before the development of
systemic metastatic disease. Surgical therapy
is generally reserved for patients with non-
small cell histologic types. In cases of exten-
sive resectable disease, adjuvant chemothen-
apy and radiation therapy may be utilized.
Most unresectable non-small cell carcinomas
are treated with combinations of chemo-
therapy and radiation therapy (4).
Surgical resection may be considered in
selected patients with small cell carcinomawhen the tumor manifests as a solitary pulmo-
nary nodule in the absence of metastases. Oc-
casionally, patients undergo resection before
the diagnosis of a small cell histologic type.
These patients subsequently undergo adju-
vant chemotherapy and radiation therapy(4, 18). Because most patients with small cell
carcinoma have disseminated disease when
they are seen initially, the preferred therapy
for these tumors is chemotherapy. Radiationtherapy may be added for patients with metas-
tases to the central nervous system and for
control of local bulky disease, particularly for
those patients with superior vena caval ob-
struction and spinal cord compression. Al-
though patients may dramatically respond to
systemic therapy and radiation therapy mi-
tially, most patients still die with recurrent
small cell carcinoma (18).Despite recent advances in surgical, local,
and systemic therapies of bronchogenic carci-
nomas that invade extrapulmonary structures,
overall 5-year survival remains at approxi-
mately 10%-15% (4). In general, because
prognosis is directly related to the tumor
stage at the patient’s initial examination,
squamous cell carcinoma has the best pnogno-sis and small cell carcinoma the worst. The
subgroup of patients with bronchioloalveolar
carcinoma that manifests as a solitary pulmo-
nary nodule also has a good prognosis. Usu-
ally, adenocarcinoma and undifferentiated
large cell carcinoma have an intermediate
prognosis (1,34).
U REFERENCES1 . Churg A. Tumors of the lung: In: Thurlbeck WM.
ed. Pathology of the lung. Stuttgart, Germany:Thieme, 1988; 311-423.
2. Gnitz ER. Lung cancer: now, more than ever, a
feminist issue. CA CancerJ Clin 1993; 43:197-199.
3 . Stanley K, Stjernsw#{228}rd J . Lung cancer: a world-
wide health problem. Chest 1989; 96(suppl): ls-5s.
4. Martini N. Operable lung cancer. CA CaneerJ Clin
1993; 43:201-2 14.
5. Gnippi MA. Clinical aspects oflung cancer. Semin
Roentgenol 1990; 25:12-24.
6. AronchickJM. Lung cancer: epidemiology and riskfactors. Semin Roentgenol 1990; 25:5-11.
7. Rubin SA. Lung cancer: past, present, and future. JThorac Imaging 1991; 7:1-8.
8. Garfinkel L, Silverberg E. Lung cancer and smok-
ing trends in the United States over the past 25
years. CA CanccrJ Clin 1991; 41:137-145.
9. Samet JM, Nero AVJr. Sounding board: indoor
radon and lung cancer. N EnglJ Med 1989; 320:
591-594.
10. Matthews MJ. Morphology of lung cancer. Semin
Oncol 1974; 1:175-182.
1 1 . Fraser RG, Pare JAP, Pare PD, Fraser RS, Genereux

446 U Continuing Education Volume 14 Number 2
(,P. Neoplastic disease of the lung. In: Fraser RG.
ParejAP, Pare PD, Fraser RS, (k-ncreux GP, eds. Di-
agnosis ofdiseases ofthe chest. 3rd ed. Philadel-phia, Pa: Saunders, 1989; 1327-1699.
12. Boyars MC. Clinical manifestations ofcarcinoma of
the lung. j Thorac Imaging 1991; 7:21-28.
1 3 . The World Health Organization histological typing
oflung tumours. 2nd ed. Amj Clin Pathol 1982;
77:123-136.
1’. Haquc AK. Pathology ofcarcinoma oflung: an up-
date on current concepts. j Thorac Imaging 1991;
7:9-20.15. Yesner R, Carter I). Pathology ofcarcinoma of the
lung: changing patterns. Clin Chest Med 1982;
3:257-289.
16. Ca�-ter D, Eggleston jC. Bronchogenic carcinoma.
In: Hartmann WH, Cowan WR, eds. Atlas of tumor
pathology: tumors of the lower respiratory tract,
fasc 17. ser 2. Washington. DC: Armed Forces Insti-
tute ofPathobogy, 1980; 59-161.
17. Pietra GG. The pathology ofcarcinoma of the
lung. Semin Roentgenol 1990; 25:25-33.
18. HinsonJAJr. Perry MC. Small cell lung cancer. CA
CancerJ Clin 1993; 43:216-225.
19. Yesner R. Histopathology oflung cancer. Semin
Ultrasound CT MR 1988; 9:4-26.
20. Bakris (;L, Mulopulos GP. Korchik R, Ezdinli EZ, Ro
j, Yoon B. Pulmonary scar carcinoma: a clinico-
pathologic analysis. Cancer 1983; 52:493-497.
2 1 . Madni JA, Carter D. Scar cancers of the lung: origin
and significance. Hum Pathol 1984; 15:625-631.
22. Heitzman ER, Markarian B, Raasch BN, Carsky EW,
Lane EJ, Berlow ME. Pathways of tumor spread
through the lung: radiologic correlations with
anatomy and pathology. Radiology 1982; 144:3-14.
23. Heitzman ER. Pulmonary neoplasm: radiologic-pathologic correlations of lung tumor interface. In:
Heitzman ER, ed. The lung: radiologic-pathologic
correlations. 2nd ed. St Louis, Mo: Mosby. 1984;
353-421.24. Theros EG. Varying manifestations of peripheral
pulmonary neoplasms: a radiologic-pathologic cor-relative study. AJR 1977; 128:893-9 14.
25. Kuriyama K, Tateishi R, Doi 0, et al. Prevalence of
air bronchograms in small peripheral carcinomas of
the lung on thin-section CT: comparison with be-
nign tumors. AiR 1991; 156:921-924.
26. Glazer HS, Duncan-MeyerJ, Aronberg DJ, Moran jF,
Levitt RG, Sagel 55. Pleural and chest wall invasion
in bronchogenic carcinoma: CT evaluation. Radiol-
ogy 1985; 157: 191-194.
27. White CS, Templeton PA. Radiologic manifesta-
tions ofbronchogenic cancer. Clin Chest Med 1993;
14:55-67.28. Tsutsui M, Araki Y, Shirakusa T, Inutsuka S. Char-
actenistic radiographic features of pulmonary carci-
noma associated with large bulla. Ann Thorac Surg
1988; 46:679-683.
29. Hill CA. Bronchioloalveolar carcinoma: a review.
Radiology 1984; 150: 15-20.
30. Epstein DM, Gefter WB, Miller WT. Lobar bron-
chioloalveolar cell carcinoma. AJR 1982; 139:463-
468.3 1 . Epstein DM. Bronchioloalveolar carcinoma. Semin
Roentgenol 1990; 25:105-111.
32. Romney B, AustinJHM. Plain film evaluation of
carcinoma ofthe lung. Semin Roentgenol 1990; 25:
45-63.33. Adler B, Padley 5, Miller RR, MUller NL. High-reso-
lution CT ofbronchioloalveolar carcinoma. AJR
1992; 159:275-277.
34. Hammar SP. Common neoplasms. In: Dail DH,
Hammar SP, eds. Pulmonary pathology. New York,
NY: Springer-Verlag, 1988; 727-845.
35. Foster WLjr, Roberts LJr, McLendon RE, Hill RC.
Localized penibronchial thickening: a CT sign of oc.
cult bronchogenic carcinoma. AJR 1985; 144:906-
908.36. O’Connell RS, McLoud TC, Wilkins EW. Superior
sulcus tumor: radiographic diagnosis and workup.
AJR 1983; 140:25-30.
37. Urschel HCJr. Superior pulmonary sulcus carci-
noma. Surg Clin North Am 1988; 68:497-509.
38. Naidich DP, Zerhouni EA, Siegelman 55. Lobar
collapse. In: Naidich DP, Zerhouni EA, Siegelman
55, eds. Computed tomography and magnetic reso-
nance of the thorax. 2nd ed. New York, NY: Raven,
1991; 197-232, 275-302.
39. Heelan RT, Demas BE, CaravelbiJF, et al. Superior
sulcus tumors: CT and MR imaging. Radiology 1989;
170:637-641.40. McLoud TC, Filion RB, Edelman RR, ShepardJO.
MR imaging of superior sulcus carcinoma. J Comput
Assist Tomogr 1989; 13:233-239.
4 1 . Mackay B. Poorly differentiated and undifferenti-
ated lung tumors. Chest 1989; 96(suppl):38s-39s.
42. Forster BB, Muller NL, Miller RR. Nelems B, Evans
KG. Neuroendocrine carcinomas ofthe lung: clini-
cal, radiologic, and pathologic correlation. Radiol-
ogy 1989; 170:441-445.
43. MUller NI, Miller RR. Neuroendocrine carcinomas
ofthe lung. Semin Roentgenol 1990; 25:96-104.
44. PearlbergJL, Sandler MA, LewisJWJr, Beute GH,Alpern MB. Small-cell bronchogenic carcinoma:
CTevabuation.AJR 1988; 150:265-268.
Answers forJanuary 1994 CME Test 1
The answers for the test on Malignant Vascular Tumors oftbe Liver: Radiologic-Patbologic Cor-relation, published in the January issue ofRadioGrapbics (RadioGraphics 1994; 14: 153-166), aregiven below.
i.e 2.d 3.c 4.d 5.b 6.c 7.d 8.a 9.b l0.d
Answers forJanuary 1994 CME Test 2
The answers for the test on FocalLungDisease: CTandHigb-Resolution CTApplications, pub-lished in thejanuary issue ofRadioGrapbics (RadioGraphics 1994; 14: 169-181), are given below.
1.b 2.d 3.d 4.d 5.c 6.a 7.d 8.a 9.c l0.d




![Inflammation and cancer: How hot is the link? · carcinoma [30], colon carcinoma, lung carcinoma, squamous cell carcinoma, pancreatic cancer [31,32], ovarian carcinoma biochemical](https://img.pdfslide.us/doc/110x75/5fcdd6c81c76a34db570e7e6/iniammation-and-cancer-how-hot-is-the-link-carcinoma-30-colon-carcinoma.jpg)