Embed Size (px)
Citation preview
• Investigate the mechanics of inhalation and exhalation of breath.
• Examine the regulation of the breathing cycle.
• Complete an experiment on respiratory function.
Breathing is the mechanism by which mammalsventilate their lungs. This ventilation relies on theprinciple that air will flow from a region of higherpressure to a region of lower pressure.
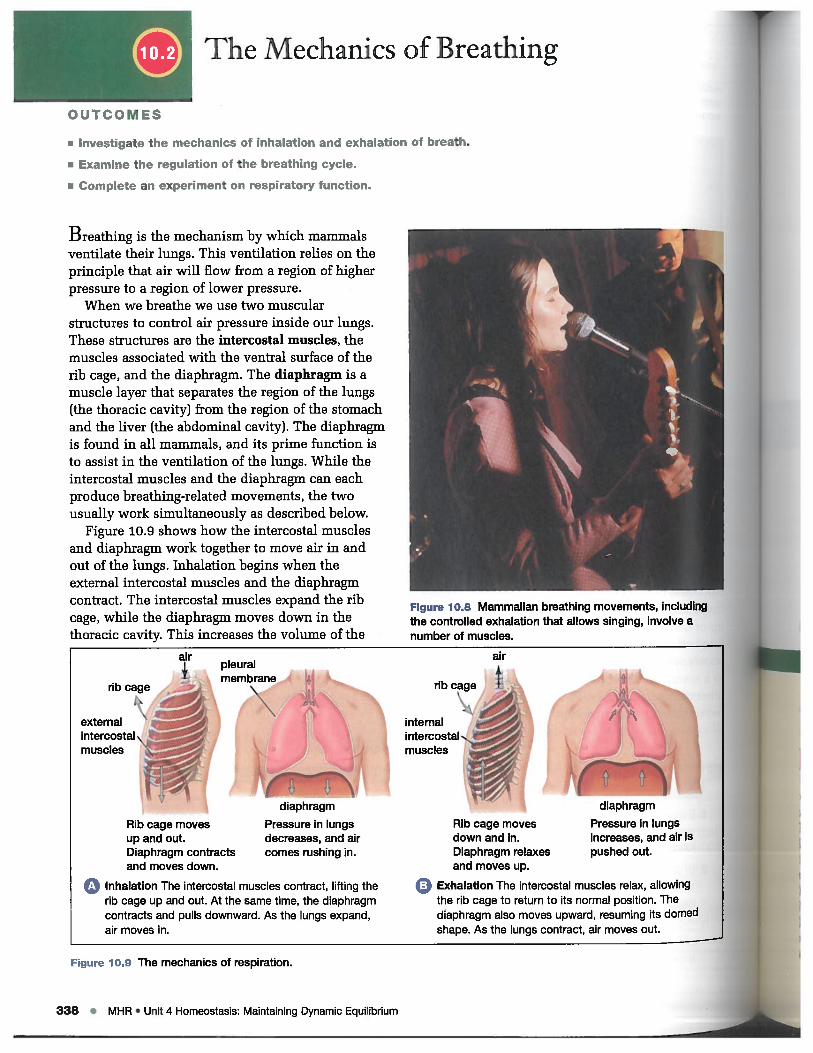
When we breathe we use two muscularstructures to control air pressure inside our lungs.These structures are the intercostal muscles, themuscles associated with the ventral surface of therib cage, and the diaphragm. The diaphragm is amuscle layer that separates the region of the lungs(the thoracic cavity) from the region of the stomachand the liver (the abdominal cavity). The diaphragmis found in all mammals, and its prime function isto assist in the ventilation of the lungs. While theintercostal muscles and the diaphragm can eachproduce breathing-related movements, the twousually work simultaneously as described below.
Figure 10.9 shows how the intercostal musclesand diaphragm work together to move air in andout of the lungs. Inhalation begins when theexternal intercostal muscles and the diaphragmcontract. The intercostal muscles expand the ribcage, while the diaphragm moves down in thethoracic cavity. This increases the volume of the
OUTCOMES
The Mechanics of Breathing
air.1 pleuralV membrane 4rib cage
41j\\
externalintercostaI\:;,;% (muscles
Rib cage movesup and out.Diaphragm contractsand moves down.
diaphragm
Pressure in lungsdecreases, and aircomes rushing in.
‘diaphragm
Pressure in lungsincreases, and air ispushed out.
0 Inhalation The intercostal muscles contract, lifting therib cage up and out. At the same time, the diaphragmcontracts and pulls downward. As the lungs expand,air moves in.
Rib cage movesdown and in.Diaphragm relaxesand moves up.
Figure 10.9 The mechanics of respiration.
0 Exhalation The intercostal muscles relax, allowingthe rib cage to return to its normal position. Thediaphragm also moves upward, resuming its domed
shape. As the lungs contract, air moves out. ii338 • MHR • Unit 4 Homeostasis: Maintaining Dynamic Equilibrium
thoracic cavity. Because the thoracic cavity isrelatively airtight, an increase in its volumeproduces a decrease in air pressure within thecavity. This decrease in pressure thaws the flexible
walls of the lungs outward into the thoracic cavity,causing the lungs to expand. As a result of thisexpansi0n the air pressure within the lungs is
lower than the air pressure in the externalenvironment. Air then enters the lungs, movingfrom the region of higher to lower pressure.
The reverse muscular movement expels air from
the lungs. The diaphragm relaxes, returning to adome-shaped curve. The external intercostal muscles
also relax, while the internal intercostal musclescontract to help pull the rib cage back to its originalposition. These changes create a higher pressurein the thoracic cavity, which causes the lungs toshrink and results in a higher pressure in the lungs.in turn, air moves out through the trachea.
Carbon Dioxide InInhaled and Exhaled Air
In 1111 II’. qO(I will observe the difteronce between theconcentration of carbon dioxide in inhaled and in exhalndair HI .i iI(jht a wooden splint and place it in a glass jarheldiur ii itil the flame goes out. Add a sir rail an run it oflimewai,
‘ to the tar and shake. Record your observations.Nov l’”i’uEr an Erlenmeyer flask by pouring in a small
‘“liii of in inwater, inserting a two-holerl rebber stepperInto its routh, and inserting a glass tube through one et theholes I oil one branch ci a robber Y-tuhn into the etherhole. t II hO a second tlrrs in lii sariro way, inserting theOtho I. rh it the sauiu Y-tuhe. II ri one flask intralirdana lI,.,,a , irxlralral “ Erich shut the branch of thu
Exchange of GasesExternal respiration takes place in the lungs. As inthe other respiratory systems you have examined,the exchange of oxygen and carbon dioxide takesplace across cell membranes. The alveoli andadjacent capillaries each have walls that are onlya single cell thick, so they can allow the diffusionof these gases. For inhaled oxygen to enter thebloodstream, it must first dissolve in the fluidlining of each alveolus.
Under normal conditions, the concentrationof oxygen in inhaled air is greater than theconcentration of oxygen in the blood of thecapillaries entering the lung area. In contrast,the carbon dioxide concentration is greater in theblood than in inhaled air. Thus oxygen diffusesacross the capillary wall into the bloodstream andcarbon dioxide moves from the capillaries across
Y-tubo that leads to the ‘exhaled” flask, and inhale deeply
through the Y-tobo. You should be drawing air through the
“inhaled” tlask. Now pinch shut the branch of the Y-tube
that leads trorrr the “inhaled” flask, open the branch that
leads to the “exhaled” flask, and exhale through the Y-tuhe.
You should be exhaling through the “exhaled” flask, Repeat
rintil you see a change in the limewater in one or both
flasks. Record your data,
Analyze
Describe the differences between the two flasks at the end
of your experiment. Explain your findings with refereoce to
the exchange of gases (luring respiration. What purpose
does the wooden splint serve in this exporinront? Are there
any ,ariablos that might rrrt be a O ii rtml for in this
experiment?
I
L
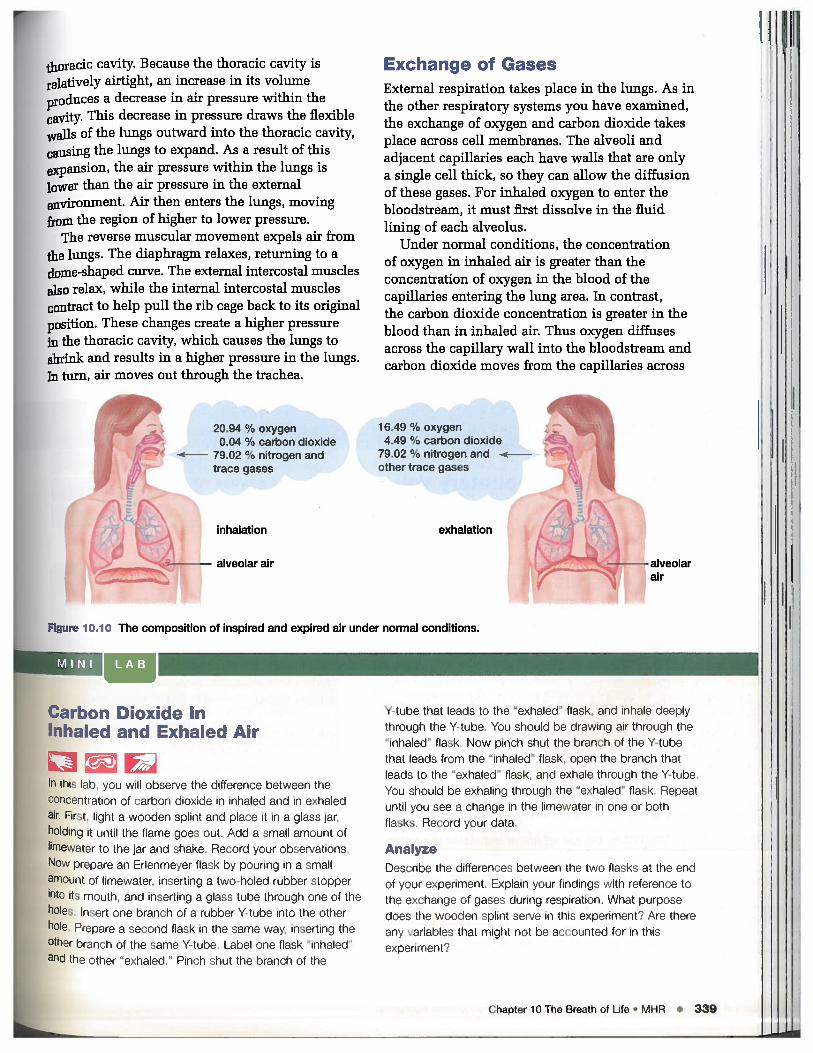
20.94 % oxygen0.04 % carbon dioxide
e 79.02 o,/ nitrogen andtrace gases
inhalation
alveolar air
16.49 % oxygen4.49 %, carbon dioxide
79.02 % nitrogen andother trace gases
exhalation
FIgure 10.10 The composition of inspired and expired air under normal conditions.
4
alveolarair
Chapter 10 The Breath at Life • MEIR • 339

the alveoli into the lung. The composition of inhaledand exhaled air is illustrated in Figure 10.10 on theprevious page.
Lung CapacityThink about the difference between your normalbreathing and a deep breath, such as a heavy sighor a yawn. Under normal conditions, your regularbreathing does not use up the full capacity of yourlungs. As your body’s needs increase, such as whenyou exercise, the volume of air drawn in can alsoincrease.
The different volumes of air drawn in or pushedout by the lungs are distinguished as follows. (Seealso Figure 10.11.)
Tidal volume is the volume of air inhaled andexhaled in a normal breathing movement.
Inspiratory reserve volume is the additionalvolume of air that can be taken in, beyond aregular or tidal inhalation.
Expiratory reserve volume is the additionalvolume that can be forced out of the lungs, beyonda regular or tidal exhalation.
Vital capacity is the total volume of gas that can bemoved in or out of the lungs. It can be calculatedas tidal volume + inspiratory reserve volume +
expiratory reserve volume = vital capacity.
Residual volume is the amount of gas that remainsin the lungs and the passageways of the respiratorysystem even after a full exhalation. This volumenever leaves the respiratory system; if it did, thelungs and respiratory passageways would collapse.Because the residual volume is not exchanged withair from the external environment, it has littlevalue for gas exchange.
Measuring Respiratory Volumes
measure your own respiratory vokiine.
Pre-lab Questions
• What medical purposes could he served by nleasiirrrigrespiratory vcftimes?
a What variables might affect the measurement ofrespiratory volumes in a single individual? Does this
investigation control for these variables?
Problem
[law can you use a spirometer, which measures air as itis exhaled, to determine the volume of air you inhale on
a normal or deep breath?
Prediction
Lirslii what porcrtittqu of your vital rapacity isru ;urilrrd by your lidal rilriiou
CAUTION: Do not inhale or exhale to the pointof faintness.
Procedure
SKILL FOCUS
Pertorming and recording
Analyzing and interpreting
Communicating results j
1. Set the spirnmetei gauge to zero and insert a clean
mouthpiece. Put on the nose plug.
2. Inhale normally, then exhale normally into thespirometer. Record this value as your tidal volume.
3. Reset the spirometer. Inhale and exhale normally. At
the end of the normal exhalation, put the spirometer
mouthpiece into your mouth and exhale as much as
you can into the spirorneter. Make sure you do this
all in one breath. Record this value as your
expiratory reserve volume.
4. Reset the spirometer. Inhale as deeply as you can,
and then exhale normally into the spirometer. Do
not force the exhalation. Ri ord this value as your
insPiiarcrri; capavit
5. To calculate your inspiratory reserve ‘joiunle,
vulrniart your tidal .‘ulriniiu fronnr your inspiratory
uapalt\. Recorrl this value as your nnspiratoryreserve co/nine.
6. Calculate ‘our viral capacity by iricliiig your
lOSpiranV:r’ ie5er e volume. ui Iiii i reserve
ire run tirtal .‘ luinru Rer;orr I lOin value as
yor ir calculated r rOi/ i/ar itt
Investigation 1 0.A
Respir atory volumes vary from individual to individual. In tn/s investigation, you will
Materials
iran. plugnritpjraia forspiromerer :jr I I c/C1 rosai nlr it 11)01 itpieces
5
I
340 • it iiii ‘ I hill I riorneostasis 1 rri.ri1 I iiirimi I_/triIt)rinII
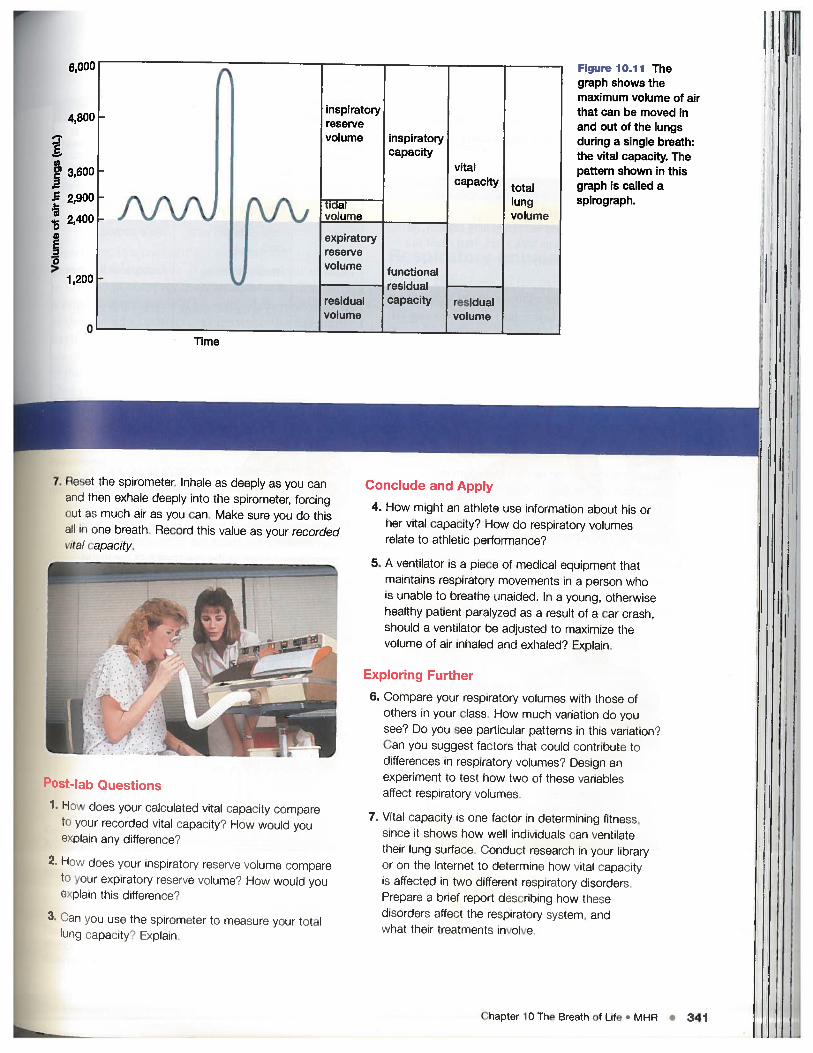
Figure 10.11 Thegraph shows themaximum volume of airthat can be moved inand out of the lungsduring a single breath:the vital capacity. Thepattern shown in thisgraph is called aspirograph.
Post.4I Questions
1. H lees your calculated vital Capacity i;umpai etc i recurrfe I vital calac ity? How would voe ‘I in any ilifteren no!
2. H does yin ir inspiratery FOCtS ‘i )luine cC mto ynji uxpli EitC-Ci-y innervn volume? How woulil youC lii ibis (iittei ence
3. Can you so the spiroineter to measure your iiiIll’ ii
Conclude and Apply
4. How might an athlete use information about his orher vital capacity? How do respiratory volumesrelate to athletic performance?
5. A ventilator is a piece of medical equipment thatmaintains respiratory movements in a person whois unable to breathe unaided. In a young, otherwisehealthy patient paralyzed as a result of a car crash,should a ventilator be adjusted to maximize thevolume of air inhaled and exhaled? Explain.
Exploring Further
6. Compare your respiratory volumes with those ofothers in your class. How much variation do yousee? Do you see particular patter us in this variation?Can you suggest factors that could contribute todifferences in respiratocy volumes? Design anexperiment to test how two of these variablesaffect respiratory volumes.
7. Vital capacity is one factor in determining fitness.since it shows how well individuals nun ventilatetheir lming surface. Conduct research in your libraryor on the Ii itornet to ieterniino how vital capacityis alluded in two dlftrmreIt respiratory dsordersPio1mi ii a brief I eporl lccm ml miiiq how thesedisorders affect the respiralorv system, andnlimif lliit imatnoirts involve.
(Thiiptf.r ill Thp Rrnnth nfl t • MUR • 341
6,00U
4,800
3,600
2,900
2,400I1 1
1,200
n
inspiratoryreservevolume inspiratory
capacityvitalcapacity total
lungvolume
_________
volume
expiratoryreservevolume functional
residualresidual Capacity residualvolume volume
Time
7. P-u the spirometer. Inhale as deeply as you canaim. I herr exhale deeply into the spirorneter, forcingcmi as much air as you can. Make sure you do thisii in one breath. Record this value as your recordedVi(-i’ apacity
I,

Table 10.1 reviews the path of air throughthe main structures involved in mammaliangas exchange. The rate at which oxygen can betransferred into the blood stream for transport tothe rest of the body is called respiratory efficiency.
WEB LINK
www.mcgrawhill .ca/Iinks/atlbiologyTo learn more about athletes and increasing lung capacity, goto the web site above and click on Web Links. How could youwork to improve your lung capacity?
Table 10.1Path of air in the body
SECTION REVIEW
1. Explain the role played by the diaphragm ininspiration and expiration. Suppose that as a resultof an automobile accident, the diaphragm of apassenger is punctured. How would this affectthe victim’s ability to breathe?
2. How would you use the apparatus shown here toexplain to a group of young students how air entersand leaves the lungs? Assume that these studentsare not yet familiar with the concept of pressure.
rubber stopper
3. Distinguish between the concepts of respiratoryefficiency and respiratory capacity. What is therelationship between the two?
4. Produce a Concept Map that relates what you havelearned about the structures of the mammalianrespiratory system to the mechanics of breathing.
5. Create a flow chart to show how gas exchangeoccurs in the human lung. Begin your flow chartwith inhaled 02.
6. Copy the graph below into your notebook. Fill in theblank spaces to the right of the graph to explain whatis being represented by this spirograph.
Structure Description Function
Hollow spaces in nose Filter, warm, moisten airNasal cavities
Pharynx
Glottis
Larynx
Trachea
Bronchi
Bronchioles
Lungs
Chamber connecting oraland nasal cavihes tolarynx
Opening to larynx
Organ containing vocalcords
Flexible tube linkinglarynx and bronchi
Tracheal divisions to lungs
Branched tubes frombronchi to alveoli
Soil, spongy organs inthoracic cavity
Connection to surroundingregions
Air passage to larynx
Sound production
Passage of air to bronchi
Passage of air to lungs
Passage of air to eachalveolus
Gas exchange
I
air tight chamber
glass
Bellj:r
IL— rubber membrane
E
E
handle to pull rubbermembrane down
342 a MHR • Unit 4 Homeostasis: Maintaining Dynamic Equilibrium

Respiratory Health
• Identify how respiratory diseases affect the homeostasIs of organisms.•Jnvest9ate different respiratory disorders.
• predict the impact of environmental factors such as allergens on the
PneumoniaAlveoli fill with thick fluid,making gas exchange difficult.
BronchitisAirways are inflamed due toinfection (acute) or due to anirritant (chronic). Coughingbrings up mucus and pus.
AsthmaAirways are inflamed due toIrritation, and bronchiolesConstrict due to muscle spasms.
EmphyasmaAlveoli burst and fuse intoenlarged air spaces. Surface areafor gas exchange is reduced.
Figure 1O12 Lower respiratory tract disorders. Exposure to infectious pathogensand/or air pollutants, including cigarette and cigar smoke, causes the diseases anddisorders shown here.
0UTCOMES
resprt0rY system.
Breathing is a constantly occurring and usuallyi.mremarkable process. It is only when our abilityto breathe is compromised in some way that wenotice its importance. The respiratory systemis oneof the primary connections between the externalenvironment and our internal environment. Sincewe can’t control our breathing process, the qualityof the external environment as well as personallifestyle choices can have an enormous impacton the health of our lungs and our entire bodies.
Respiratory ImpairmentAs you have seen in the previous sections, therespiratory system works efficiently to accomplishthe gas exchange that humans need in order to live.Disorders of the respiratory system can causesignificant impairment in our ability to breathe andexchange oxygen for carbon dioxide. Figure 10.12highlights some of the more common disorders ofthe respiratory system. More than three million
Chapter 10 The Breath of Life • MHR 343

carcinomas, or tumours.
Canadians of all ages must cope with seriousrespiratory diseases. The following pages describesome of the common respiratory system disorders.
Lung Cancer
Lung cancer, which is the unconliolled and invasivegrowth of abnormal cells in the lungs, is the leadingcancer killer of both men and women in NorthAmerica. Figure 10.13 compares cancerous lungtissue with healthy lung tissue. As the carcinoma,or malignant tumour, grows, abnormal cells continueto multiply and take over healthy tissue. Deathis not usually caused by difficulty in breathing,however; it is typically the result of cancer movingout of the lungs and into the brain and other partsof the body, as shown in Figure 10.14.
Most cases of lung cancer — approximately87 percent — are the result of cigarette smoking.Many substances contained in tobacco smoke arecarcinogens, or cancer-causing agents. Thesesubstances irritate the cells of the lungs, causingthem to become anaplastic (simpler or lessdifferentiated) and form cancerous tumours.Stopping smoking can reduce the risk of cancer asthe abnormal cells are replaced with normal, non-irritated cells. Carcinogens can also be found insecond-hand smoke, which is the smoke exhaledfrom a smoker’s lungs and the smoke from the endof a burning cigarette. Second-hand smoke is amajor cause of lung cancer in non-smokers.
Another cause of lung cancer is exposure to radon,a heavy gaseous radioactive element formed from
thE
I{aanbuoil1wnil.
Al:lin
1wcal1wByincaiwe
Figure 10.13 (A) A normal lung showing healthy red tissue. (B) Diseased lungsshowing black tissue resulting from heavy smoking. The white areas are
respiratory epithelial cells
reserve cells —
connective tissue —
lymphatic vessel —j
blood vessel
brEcaiincdeinpa‘is.Spbcisprcaithc
7•j
Figi
ho’1wis
smooth muscle-: -
Figure 10.14 The large ball of cells in the centre of theimage is a carcinoma that has developed from the interiorsurface cells of the human lung. The carcinoma continuesto grow and invade surrounding tissues, including lymphatic
‘— blood vessel
metastatic cells
and blood vessels present in the lung. These vessels, whichcirculate through the body, carry the cancerous cells, calledmetastatic cells, to new locations where they can grow andcontinue to invade new tissues.
A344 MHR • Unit 4 Homeostasis: Maintaining Dynamic Equilibrium
the decay of radium that is used in radiotherapy.
gadon which is found in small quantities in rocks
d soil, can rise through the soil and enterildings by way of cracks in the foundation and
other openings such as pipes, drains, and gaps ininsulation. Radon is colourless and odourless, and
must be measured using specially designed kits.Approximately 12 percent of lung cancers are
linked to radon exposure.Although changes in lung tissue can occur
jmediately upon exposure to carcinogens, lung
cancer can take years to develop. Unfortunately,
lung cancer has few symptoms in its early stages.
By the time symptoms appear, the cancer is usually
in an advanced state. Typical symptoms of lungcancer include: chronic cough, coughing up blood,weight loss and a loss of appetite, shortness ofbreath, chest pain, and fever without a knowncause. When these symptoms appear in anindividual, a medical diagnosis is required todetermine their cause, as they are also commonin other respiratory ailments. Doctors review thepatient’s medical history to establish if any cancerrisk factors are present, and will order several tests.Specialized x-rays, called CT scans, may help tolocate abnormalities in the lungs. This technologyis advancing constantly, and there is now aprocedure called a helical low-dose CT scan thatcan detect the early stages of lung cancer whenthe tumours are still very small.
far and the cancer has not begun to spread. Not alltumours can be removed, however, so therapeuticprocedures will probably be used. These includeradiation therapy, which employs a form of high-energy x-ray that kills cancer cells. Radiationtherapy is often used in combination withchemotherapy, which involves using medicationsthat are effective in destroying cancer cells. Thedrugs may be injected directly into the body ormay be taken in pill form. Radiation therapy andchemotherapy target cancer cells but also killhealthy cells in the area of the cancer. The sideeffects include hair loss and severe nausea.
Pneumonia
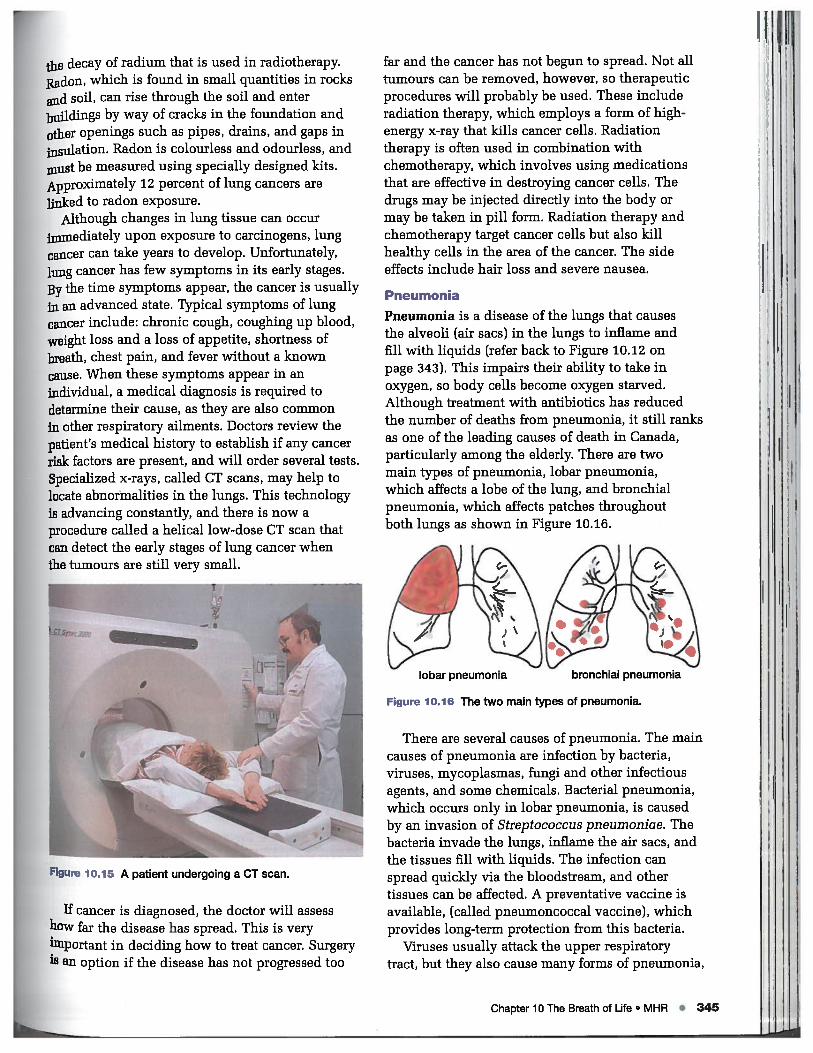
Pneumonia is a disease of the lungs that causesthe alveoli (air sacs) in the lungs to inflame andfill with liquids (refer back to Figure 10.12 onpage 343). This impairs their ability to take inoxygen, so body cells become oxygen starved.Although treatment with antibiotics has reducedthe number of deaths from pneumonia, it still ranksas one of the leading causes of death in Canada,particularly among the elderly. There are twomain types of pneumonia, lobar pneumonia,which affects a lobe of the lung, and bronchialpneumonia, which affects patches throughoutboth lungs as shown in Figure 10.16.
There are several causes of pneumonia. The maincauses of pneumonia are infection by bacteria,viruses, mycoplasmas, fungi and other infectiousagents, and some chemicals. Bacterial pneumonia,which occurs only in lobar pneumonia, is causedby an invasion of Streptococcus pneumoniae. Thebacteria invade the lungs, inflame the air sacs, andthe tissues fill with liquids. The infection canspread quickly via the bloodstream, and othertissues can be affected. A preventative vaccine isavailable, (called pneumoncoccal vaccine), whichprovides long-term protection from this bacteria.
Viruses usually attack the upper respiratorytract, but they also cause many forms of pneumonia,
lobar pneumonia
Figure 10.16 The two main types of pneumonia.
bronchial pneumonia
Figure 10.15 A patient undergoing a CT scan.
If cancer is diagnosed, the doctor will assesshow far the disease has spread. This is veryl]iiportant in deciding how to treat cancer. Surgeryis an option if the disease has not progressed too
Chapter 10 The Breath of Life . MHR • 345

particularly in children. Viral pneumonias are often
associated with a secondary bacterial infection.
Viral pneumonias tend to be less serious than other
forms of pneumonia, and usually last a shorter
period of time.Mycoplasma pneumonia is a type of pneumonia
caused by mycoplasmas, which are the smallestfree-living agents of disease in humans.Mycoplasmas possess characteristics of bothbacteria and viruses, and have not yet been clearly
classified as one or the other. Patients suffering
from mycoplasma pneumonia may require a longrecovery period and be very weak for a long time.
Asthma
Asthma is a chronic obstructive lung disease that
can develop at any age. Asthma is characterized by
extreme sensitivity of the lungs to certain triggers
that cause the airways to react and become
obstructed. The effects of asthma vary, and may
be very mild or extremely severe. In extreme cases,
daily attacks can cause major restrictions of lifestyle
or may even lead to death. Less that one quarter
of children affected by asthma outgrow theirsymptoms by adulthood. This disorder is a leading
cause of childhood hospitalization in Canada.Asthma symptoms usually occur in episodes,
or “asthma attacks.” Although the attacks areoccasional, the underlying inflammation causing
the narrowing of the airways is constant. During an
attack, three changes occur in the lungs: the airway
swells, the bronchial muscles tighten, andincreased amounts of mucous are secreted into the
airway. All of these changes obstruct the airway,
making breathing difficult.Asthma attacks may start suddenly as a result
of exposure to a trigger, or they may take hours, or
even days, to develop. The most commonly reported
triggers in Canada include colds and chest infections;
exercise and sports; exposure to pollen, flowers,
grass, plants, or trees. Common triggers alsoinclude exposure to tobacco smoke, dust, cold air,
pets, mould or mildew, and outdoor air pollution
(see Figure 10.17).
Asthma can be managed through lifestylechanges and the use of medications. When asthma
is diagnosed in an individual, that person’s maintriggers must be determined. Treatment includesreducing contact with those triggers. As well asrecommending testing for common allergens, thephysician will most likely suggest that the patientmaintain an “asthma diary” to record thecircumstances surrounding each asthma attack.
Figure 10.17 The most common triggers for an asthma
attack as reported to Health Canada’s most recent student
lung health survey.
In addition to identifying and removing exposure
to triggers, it is usually necessary to use medications.
Asthma medications reduce the underlyinginflammation of the airways, thus reducing the
narrowing of the airways and preventing respiratory
obstruction. Two main types of medications are
prescribed. The first type, anti-inflammatory agents3
helps prevent attacks by delaying or interrupting
the inflammation. Anti-inflammatory agents also
diminish ongoing inflammation and end attacks.
The second type of medication, bronchodilators,
relax the bronchial muscles and thus open up
the airways (see Figure 10.18 on page 348).
Asthma and the Environment
Besides the gases that we need for survival, the
air we breathe contains many different particles.
Some of these particles are removed in the upper
respiratory tract during inhalation, but many arebreathed deep into the lungs. For people with
asthma, these particles can cause an allergic reaction
that triggers an asthma attack. The particles include
Once the triggers have been established, the asthmasufferer’s enviromnent can be altered to minimizethe exposure to certain triggers.
izras
Tobacco smoke
Dust
• MHR • Unit 4 Homeostasis: Maintaining Dynamic Equilibrium

jung Cancer —
The Common CausesDo you know which cancer is the most preventable?
Lung cancer is the most avoidable of all cancers, but it
remains the leading cause of cancer death for men and
women in Canada. Nearly one third of the cancer deaths
in men and one quarter of cancer deaths in women are
caused by lung cancer. The Canadian Cancer Society
estimates that 20 800 Canadians (12 000 men and 8 800
women) will be diagnosed with lung cancer this year.
Types of Lung Cancer
There are two major types of this disease: non-small cell
lung cancer and small-cell lung cancer. The non-small
variety is the most common, making up 80 percent of
lung cancers. Non-small cell lung cancer consists of
three main forms: adenocarcinomas, squamous cell
carcinomas, and large cell carcinomas. When non-small
cell lung cancer is localized, all three forms have thepotential for cure through surgery. Small-cell lung cancer
starts in the hormonal cells, usually in the central part
of the lung. This type of cancer is not usually treatable
by surgery.
Sadly, the number one cause of lung cancer iscompletely avoidable. Smoking cigarettes and othertobacco products leads to more cases of lung cancerthan any other single factor. The more a person smokesand the longer they smoke, the greater is their risk ofgetting lung cancer. Though the risk of lung cancer dropsas soon as a smoker quits, it remains higher than the riskof a person who has never smoked. After 15 years of notsmoking, a former smoker will still be twice as likely tocontract lung cancer than will a non-smoker. There is noway to “safely” smoke during the teenage years and notbe at risk of long-term consequences. The CanadianGovernment places warnings in a prominent location onall cigarette packages to ensure that smokers are clearon the health risks of smoking.
Second-hand SmokeSmokers are not the only people affected by theirtobacco use. The smoke that people exhale and thesmoke from the end of their cigarettes cause lung cancer,respiratory infections, and asthma in non-smokers too.This second-hand smoke — also known as environmentaltobacco smoke — contains an estimated 4000 chemicals.Health Canada has identified an incredible 42 of thesesubstances as carcinogens, or known cancer-causingagents. One of most highly carcinogenic substances on
Earth is benzopyrene. This yellow crystalline carcinogenic
hydrocarbon is found in coal tar and as a product ofincomplete combustion of chemicals. Benzopyrene is
also found in cigarette smoke. Formaldehyde, which is
commonly used to preserve dead organisms such as
lab animals, is another component of tobacco smoke.
Children are especially vulnerable to the dangers ofsecond-hand smoke. Children’s lungs are still developingand are more easily damaged than adult lungs by thechemicals in second-hand smoke. In young children,particularly those under 18 months, second-hand smokecauses lower respiratory tract infections such aspneumonia and bronchitis, ear infections, reduced lungfunction, and many other serious illnesses. It also triggersor worsens episodes of asthma, which may result inhospitalization.
Smoking during pregnancy presents serious health risks
for children. Babies born to mothers who smoke tend to
weigh less than other newborns, and are more likely to
die during birth. After birth, babies exposed to second
hand smoke have a higher incidence of Sudden Infant
Death Syndrome (SIDS) than other newborns.
DON’TPOISON USWARNING: Second-hand smokecontains carbon monoxide, ammonia.fonnaldehyde, henzo[a]pyrene andnitrosamines. These chemicals canharm your children.
Health canada
An example of a government cigarette warning label.
Reducing the Risk
At present, health experts have not established a safe
level of exposure to second-hand smoke. But it is usually
easy for you and your family to protect yourselves fromthe dangers of second-hand smoke. Just avoid areaswhere people smoke, especially indoors, If you are asmoker and are not able to quit at this time, keep trying
to stop and make sure you smoke only outdoors.Cigarette smoke stays in a room for hours afterwards,even it the windows are open and the room is ventilated.Avoid smoking in a car, where the chemicals are confinedto a very small space. And if you smoke, see your doctor
right away for help in quitting — for your own goodhealth and the health of those around you.
ioIogyMagazine TECHNOLOGY • SOCIETY • ENVIRONMENT
Chapter 10 The Breath of Life • MHR • 347

spores from mildews and inoulds, which form inareas of high humidity and which are often allergens.Another common particle is dust. Each speck ofdust contains thousands of dust mites. Pets areanother common source of airborne particles. Petdander (minute scales shed from hair, feathers, orskin) is another common allergen. Certain foodscan also be allergens that trigger asthmatic attacks.
Outdoor air quality depends on geography. Inmany cases, asthma sufferers must remain indoorswhen an “air alert” is given. Common pollutantsin the outdoor air include ozone (03), nitrogendioxide (NO2), and sulfur dioxide (SO2). Vehicleemissions account for a great deal of the outdoorpollutants, so people living in urban areas with ahigh density of vehicles may experience greaterexposure to this pollution.
The most common strategy for preventing orreducing the influence of these particles is toidentify the specific ones that are allergenic andthen remove them from the asthmatic persons’senvironment. For example, removing pets from thehome and reducing the humidity at home in order
I
1. Explain what lung cancer is. Describe how acarcinoma forms, and how it causes death.
2. Describe two common causes of lung cancer. Makeup an educational pamphlet describing two stepsthat could be taken to avoid these factors.
3. Compare and contrast three different forms ofpneumonia. What are the treatment options foreach of the different forms?
4, Design a questionnaire that would find out whether ornot people suffered from asthma, and if so, what the
to lessen mould and mildew are good first steps. Itis also important to reduce exposure to dust anddust mites by placing mattresses and pillowswithin airtight covers, washing bedding every weekin hot water, and removing wall-to-wall carpeting,rugs, curtains, and upholstered or soft furniture.
In some instances, odours or fumes may causean allergic reaction and trigger an asthmatic attack.Sources include perfumes, petrochemical fumes,room deodorizers, cleansers, paints, and baby ortalcum powders. As with airborne particles, thebest strategy is to minimize contact with any ofthese substances.
Obstructive Respiratory Disorders
Obstructive respiratory disorders are disorderswhere the air does not flow freely in the airways,and the amount of time to inhale or exhale isgreatly increased. Asthma, described above, isan obstructive respiratory disorder. A commondisorder of this type is chronic bronchitis, wherethe airways are inflamed and filled with mucous(refer back to Figure 10.12 on page 343).Commonly, a cough brings up the mucous andinfection is likely to occur. Smoking is the mostcommon cause of chronic bronchitis.
Emphysema is another disorder of this typeand it is chronic and incurable. The alveoli aredistended and their walls are so damaged that thesurface available for gas exchange is reduced andless oxygen is available to the brain and tissues.The elasticity of the lung tissue is reduced so theforce behind exhaling is also reduced, making itadditionally difficult to breath. The only treatmentoptions for emphysema are reducing or eliminatingsmoking, exercise, some drugs to help the alveoliwork, and supplemental oxygen. These can allslow the progression of the disease and makethe symptoms less extreme.
possible triggers could be. The questionnaire shouldbe aimed at students in your school.
5. Describe different ways that asthma can bemanaged. Include medications as well as lifestylechoices. Explain how each way works to improvean asthmatics’ breathing.
6. Choose two respiratory disorders listed in thischapter and discuss why breathing is difficultwith these conditions.
Figure 10.18 Some individuals use asthma inhalers to helpwith the symptoms of an asthma attack.
a SECTION REVIEW
rI
I348 • MHR • Unit 4 Homeostasis: Maintaining Dynamic Equilibrium