Embed Size (px)
Citation preview

Carbohydrate Intake: A Risk Factor for Biliary Sludge and Stones During Pregnancy
Alan C. Wong, MD, MPHCynthia W. Ko, MD, MS
Department of MedicineDivision of Gastroenterology
Seattle, Washington
Introduction
• Gallstone disease results in >700,000 cholecystectomies each year.
• Female gender is a risk factor, and pregnancy is a high risk period for gallstone formation.
• Gallbladder (GB) disease is the most common non-obstetrical cause of maternal rehospitalization in the first 60 days after delivery.
• Carbohydrate intake has been linked to increased risk of cholecystectomy in women.
• The effect of carbohydrate consumption on GB disease during pregnancy is unclear.

Study Aim
To determine the effect of dietary carbohydrate intake on the formation of biliary sludge and stones during pregnancy.

- Prospective study
- Cohort of pregnant women
- Exposure:Carbohydrate consumption during pregnancy, determined by food frequency questionnaire.
- Outcome:Formation of new GB sludge/stones, determined by serial GB ultrasound.
Study Design – General Overview

Consecutive women attending 1st obstetrics clinic (n = 8,929)
Eligible and interested (n = 4,897)
Gallstones on entry GB ultrasound (n = 208)
Had cholecystectomy (n = 33)
Did not complete dietary questionnaire (n = 184)
Fewer than two GB ultrasounds (n = 1,402)
Included in analysis (n = 3,070)
Age <18, poor language comprehension, >20 weeks pregnant, declined to participate (n = 4,032)
1st trimester(10-12 weeks)
2nd trimester(17-19 weeks)
Post-partum(4-6 weeks)
3rd trimester(26-28 weeks)
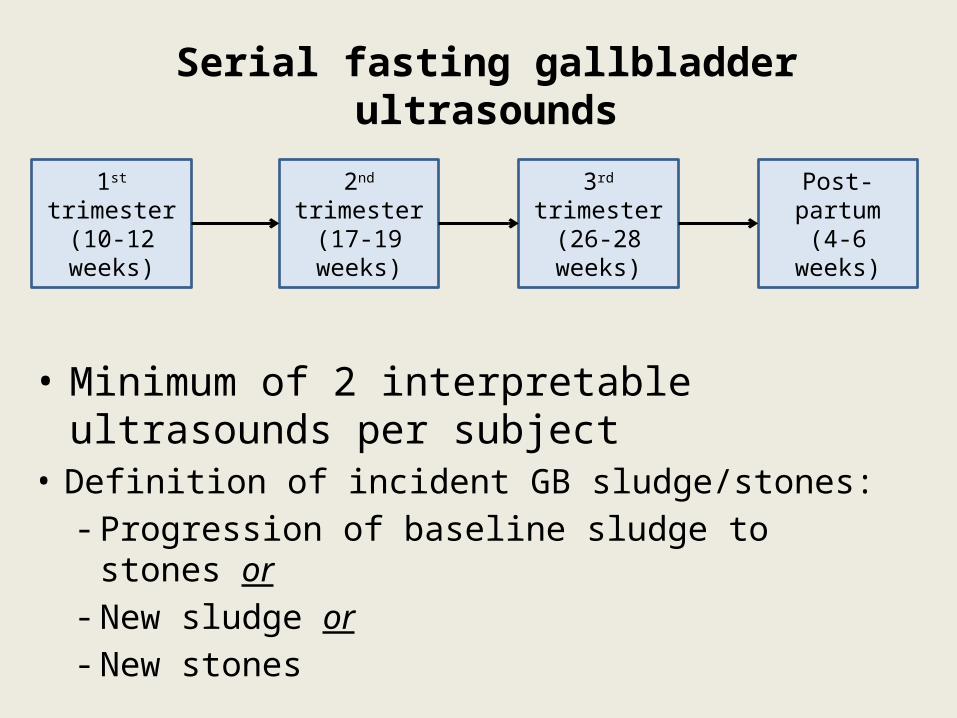
Serial fasting gallbladder ultrasounds
• Definition of incident GB sludge/stones:- Progression of baseline sludge to stones or- New sludge or- New stones
• Minimum of 2 interpretable ultrasounds per subject

Ultrasonographic Definitions:1) Sludge: low-level echoes, shift with positional changes, no post-acoustic shadowing.
2) Stones: high-amplitude echoes, >2 mm in diameter, post-acoustic shadowing present.
Interpretation:- Technicians had specific training in GB ultrasound- Images reviewed by 1 of 2 radiologists

Measurement of Carbohydrate Intake
1st trimester 2nd trimester Post-partum3rd trimester
Dietary Questionnaire
- Validated food frequency questionnaire
- Daily consumption (g/day) of total carbohydrate, starch, sucrose, galactose, fructose, lactose, and maltose.
3rd trimester
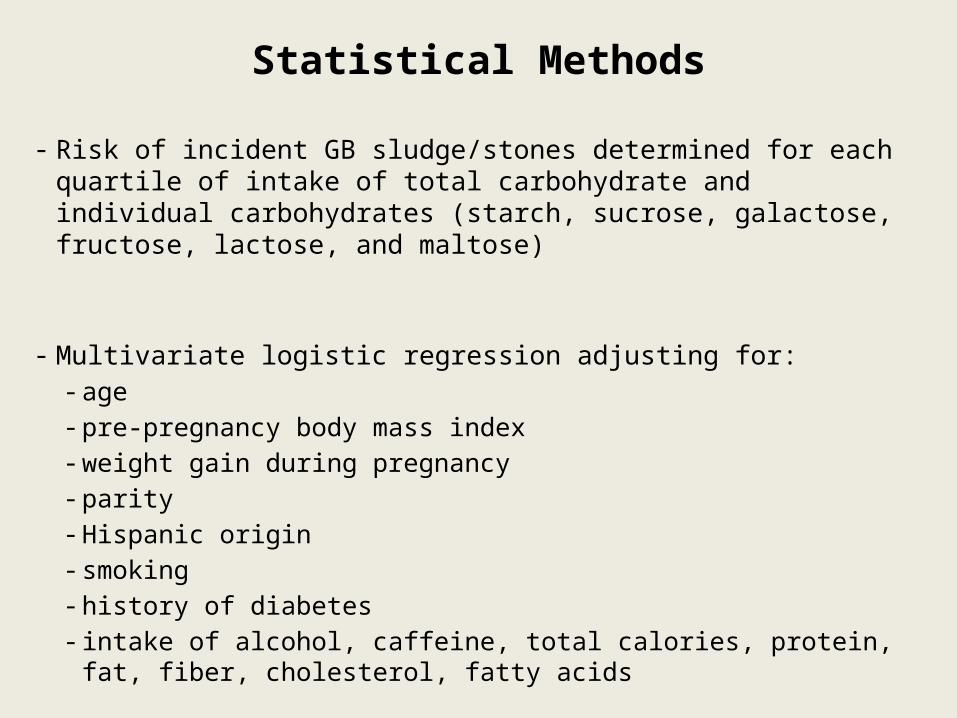
Statistical Methods
- Risk of incident GB sludge/stones determined for each quartile of intake of total carbohydrate and individual carbohydrates (starch, sucrose, galactose, fructose, lactose, and maltose)
- Multivariate logistic regression adjusting for: - age - pre-pregnancy body mass index- weight gain during pregnancy- parity - Hispanic origin - smoking- history of diabetes - intake of alcohol, caffeine, total calories, protein, fat, fiber, cholesterol,
fatty acids

Results

Results
Incidence of GB disease = 10.2%
• New sludge = 5.1%
• New stones = 2.8%
• Baseline sludge to stones = 2.3%

Characteristics of Study Subjects
Results
No new sludge/stones New sludge/stones P - value
n = 2756 n = 314
Hispanic origin (%) 10.4 17.8 0.001
BMI pre-pregnancy (kg/m2) 24 27 <0.0001
Weight gain during pregnancy (kg) 14.6 12.6 <0.0001
Caffeine intake (mg/day) 40 50 0.018
Alcohol intake (g/day) 0.1 0.5 0.038
No significant difference between groups:- history of diabetes- gestational diabetes- intake of calories, fat, fiber

Nutrient Adjusted Odds Ratio 95% Confidence Interval
Total carbohydrate 2.295 1.130 - 4.661
Starch* 1.812 1.002 - 3.277
Fructose* 2.054 1.183 - 3.568
Galactose* 0.664 0.441 - 0.999
Results
Carbohydrate consumption and the risk of incident gallstone disease
* With additional adjustment for total carbohydrate intake
- Adjusted for: age, pre-pregnancy BMI, weight gain, parity, Hispanic origin, smoking, history of diabetes, intake of alcohol, caffeine, calories, protein, fat, fiber, cholesterol, fatty acids
- Highest quartile of intake compared to lowest quartile

Quartile 1 Quartile 2 Quartile 3 Quartile 40
0.5
1
1.5
2
2.5
Total carbohydrate Starch Fructose Galactose
Odd
s Ra
tio
*
*
*
*
**
Carbohydrate consumption and the risk of incident gallstone disease
* P < 0.05, compared to Quartile 1

Discussion
↑ cortisol↑ estrogen
↑ progesterone↑ human placental lactogen
Pregnancy

↑ cortisol↑ estrogen
↑ progesterone↑ human placental lactogen
Pregnancy
Hyperinsulinemia+
Insulin resistance

↑ cortisol↑ estrogen
↑ progesterone↑ human placental lactogen
Pregnancy
Hyperinsulinemia+
Insulin resistance
Postprandial insulin ↑ 3-fold
Basal insulin↑ 2-fold
Insulin sensitivity↓ 50-70%

↑ cortisol↑ estrogen
↑ progesterone↑ human placental lactogen
Pregnancy
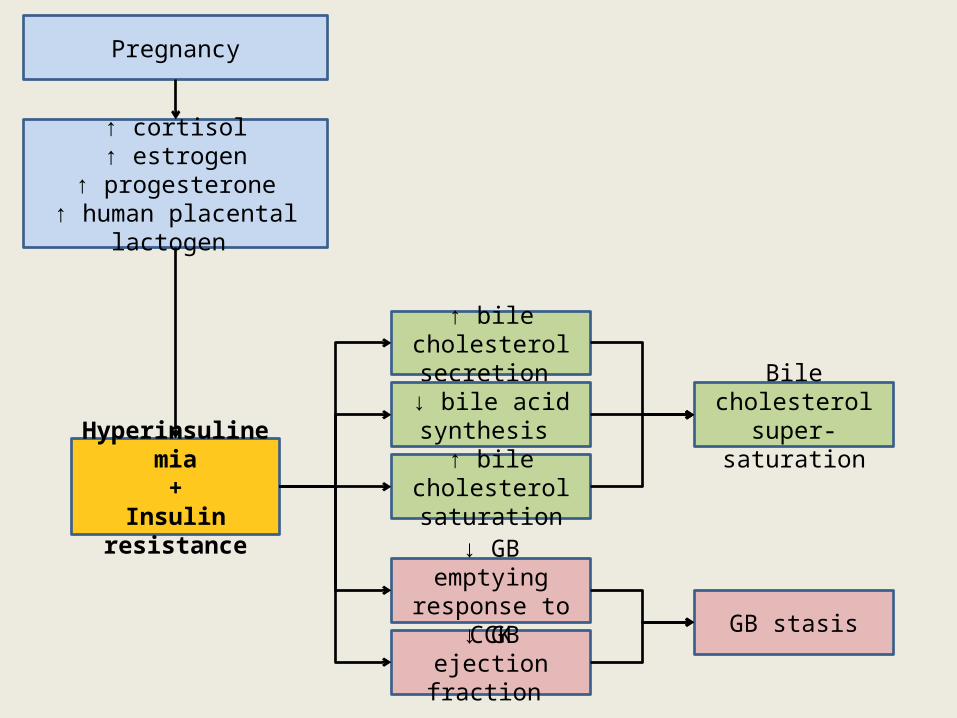
Bile cholesterol super-saturation
↑ bile cholesterol saturation
↑ bile cholesterol secretion
↓ bile acid synthesis
Hyperinsulinemia+
Insulin resistance
↑ cortisol↑ estrogen
↑ progesterone↑ human placental lactogen
Pregnancy
Bile cholesterol super-saturation
GB stasis
↑ bile cholesterol saturation
↑ bile cholesterol secretion
↓ bile acid synthesis
↓ GB ejection fraction
↓ GB emptying response to CCK
Hyperinsulinemia+
Insulin resistance

↑ cortisol↑ estrogen
↑ progesterone↑ human placental lactogen
Pregnancy
Bile cholesterol super-saturation
GB stasis
↑ bile cholesterol saturation
↑ bile cholesterol secretion
↓ bile acid synthesis
↓ GB ejection fraction
↓ GB emptying response to CCK
Hyperinsulinemia+
Insulin resistance
Carbohydrates

↑ cortisol↑ estrogen
↑ progesterone↑ human placental lactogen
Pregnancy
Bile cholesterol super-saturation
GB stasisCarbohydrates
↑ bile cholesterol saturation
↑ bile cholesterol secretion
↓ bile acid synthesis
↓ GB ejection fraction
↓ GB emptying response to CCK
Hyperinsulinemia+
Insulin resistance

↑ cortisol↑ estrogen
↑ progesterone↑ human placental lactogen
Pregnancy
Bile cholesterol super-saturation
GB stasis
↑ bile cholesterol saturation
↑ bile cholesterol secretion
↓ bile acid synthesis
↓ GB ejection fraction
↓ GB emptying response to CCK
Hyperinsulinemia+
Insulin resistance
Carbohydrates

Fructose
Fructose
– does not require insulin for uptake into cells
– stimulates less insulin release than glucose
– largely metabolized in the liver

Fructose
leptin resistance↑ leptin level
hepatic lipogenesis↑ triglyceride
hepatic insulin resistance

Fructose
leptin resistance↑ leptin level
hepatic lipogenesis↑ triglyceride
hepatic insulin resistance
Gallstone disease

Limitations
1) Only one dietary time point
2) GB ultrasounds were done at varying stages of pregnancy
3) No serum insulin/leptin levels

• High intake of total carbohydrate, starch, and fructose is associated with increased risk of developing biliary sludge/stones during pregnancy.
• Dietary modification during pregnancy may reduce this risk.
Conclusion

References• American Gastroenterological Association. The burden of gastrointestinal diseases. Bethesda, MD: The American
Gastroenterological Association, 2001.• Lydon-Rochelle M et al. Association between method of delivery and maternal rehospitalization. JAMA. 2000
May 10;283(18):2411-6.• Tsai CJ et al. Glycemic load, glycemic index, and carbohydrate intake in relation to risk of cholecystectomy in
women. Gastroenterology. 2005 Jul;129(1):105-12.• Nakeeb A et al. Insulin resistance causes human gallbladder dysmotility. J Gastrointest Surg. 2006 Jul-
Aug;10(7):940-8; discussion 948-9.• Gielkens HA et al. Effect of insulin on basal and cholecystokinin-stimulated gallbladder motility in humans. J
Hepatol. 1998 Apr;28(4):595-602.• Dubrac S et al. Insulin injections enhance cholesterol gallstone incidence by changing the biliary cholesterol
saturation index and apo A-I concentration in hamsters fed a lithogenic diet. J Hepatol. 2001 Nov;35(5):550-7.• Biddinger SB et al. Hepatic insulin resistance directly promotes formation of cholesterol gallstones. Nat Med.
2008 Jul;14(7):778-82. Epub 2008 Jun 29.• Butte NF. Carbohydrate and lipid metabolism in pregnancy: normal compared with gestational diabetes mellitus.
Am J Clin Nutr. 2000 May;71(5 Suppl):1256S-61S.• Wang HH et al. New insights into the molecular mechanisms underlying effects of estrogen on cholesterol
gallstone formation. Biochim Biophys Acta. 2009 Nov;1791(11):1037-47.• Wu Z et al. Progesterone inhibits L-type calcium currents in gallbladder smooth muscle cells. J Gastroenterol
Hepatol. 2010 Dec;25(12):1838-43. • Miller A et al. Dietary fructose and the metabolic syndrome. Curr Opin Gastroenterol. 2008 Mar;24(2):204-9.• Ko CW et al. Incidence, natural history, and risk factors for biliary sludge and stones during pregnancy.
Hepatology. 2005 Feb;41(2):359-65.
This study is supported by National Institutes of Health (NIH) grant DK 46890

Thank You