Embed Size (px)
Citation preview
Carbapenemase-Producing Enterobacteriaceae (CPE) -
Navigating Uncharted Territory
Madeleine Ashcroft, Public Health Ontario
Safiyya Nazarali, Peel Public Health
September 19, 2018
IPAC–IT: NEW FRONTIERS IN INFECTION PREVENTION AND CONTROL!
PublicHealthOntario.ca
Objectives
Following this session, you should be able to:
• Define CPE and its importance
• Implement screening protocols for new admissions and residents returning from hospital
• Identify CPE cases (colonization and infection)
• Describe IPAC Measures for residents with CPE colonization and/or infection
• Educate residents and families on IPAC measures using PHO tools
PublicHealthOntario.ca
CPE – What is it? Carbapenems: A class of broad spectrum antibiotics that
are used for treating infection caused by resistant bacteria (e.g. ertapenem, meropenem, imipenem, doripenem) Carbapenemase Genes: Genes, made up of DNA, that
instruct the bacteria to make protein or enzyme called carbapenemase (genes: KPC, NDM, OXA, VIM, etc.) Carbapenemase: Enzymes that break down most
antibiotics including carbapenems Enterobacteriaceae: A large family of bacteria present
normally (part of gut flora) or pathogenically in the human intestinal tract (e.g., E.coli, Enterobacter, Klebsiella, etc.)
PublicHealthOntario.ca
Acronyms: CPO,CPE,CRE,CRO
C Carbapenems (antibiotics)
R Resistant
P Producing (carbapenemase enzyme)
O Organisms
E Enterobacteriaceae
• CPE is most worrisome – with ~ 50% mortality (infections)
PublicHealthOntario.ca
How is CPE Spread ?
5
• Most with CPE are colonized in the lower GI tract
• Direct contact: Unwashed hands
• Indirect Contact: Contaminated equipment and surfaces including sinks, shower drains, and endoscopes
• Infection: Enters at specific site and causes symptoms, e.g., pneumonia and UTI
PublicHealthOntario.ca
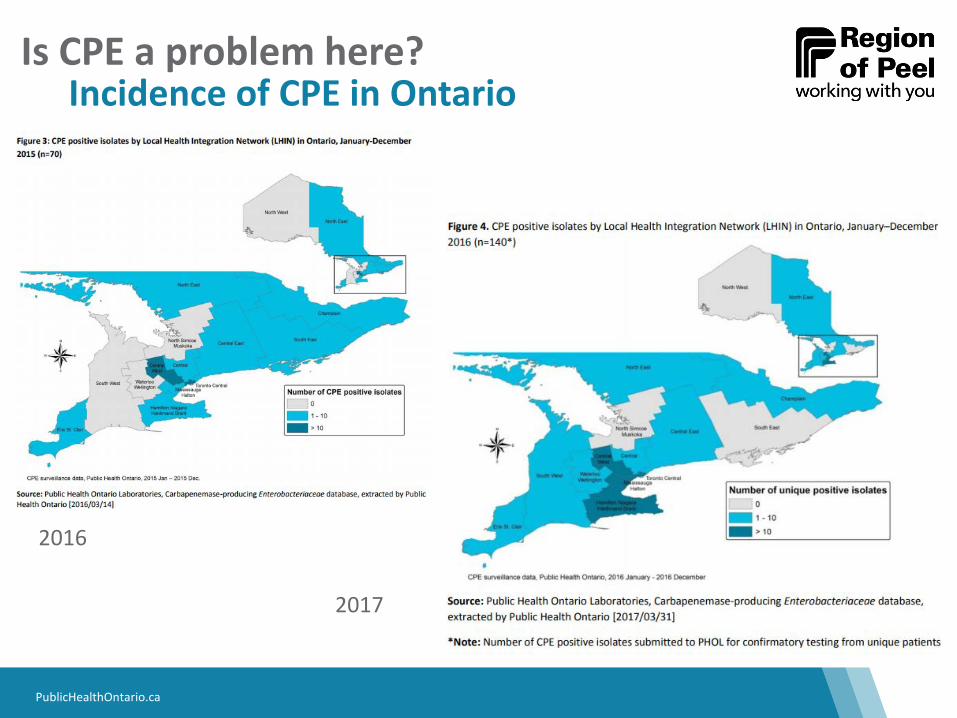
Incidence of CPE in Ontario
Is CPE a problem here?
2016
2017
PublicHealthOntario.ca
CPE is now reportable
7
Effective May 1, 2018:
• CPE colonization and infection are now included in the regulations for reporting diseases of public health significance (DOPHS) and reportable to the local public health unit
• First isolate only
• All confirmed cases of CPE require investigation to determine if nosocomial transmission of CPE has occurred and to identify the source of transmission
PublicHealthOntario.ca
Preliminary Reports - Caveats
8
• New system – voluntary to mandatory public reporting
• Date entry challenges
• Data reflects previous positives
• New cases may come to light
PublicHealthOntario.ca 9
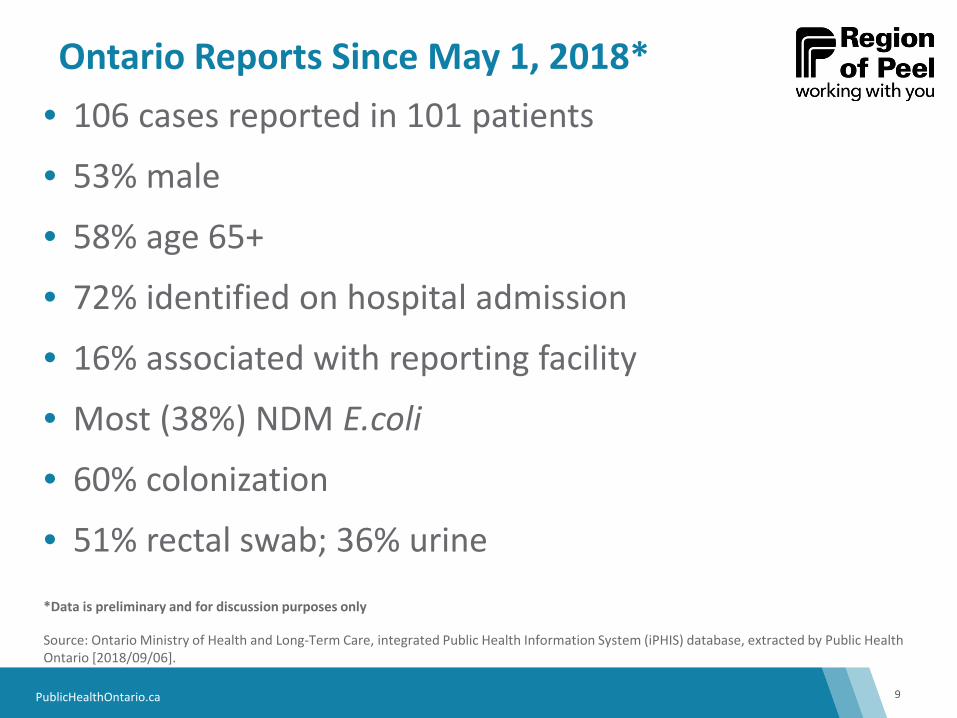
• 106 cases reported in 101 patients
• 53% male
• 58% age 65+
• 72% identified on hospital admission
• 16% associated with reporting facility
• Most (38%) NDM E.coli
• 60% colonization
• 51% rectal swab; 36% urine
*Data is preliminary and for discussion purposes only
Source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2018/09/06].
Ontario Reports Since May 1, 2018*
PublicHealthOntario.ca
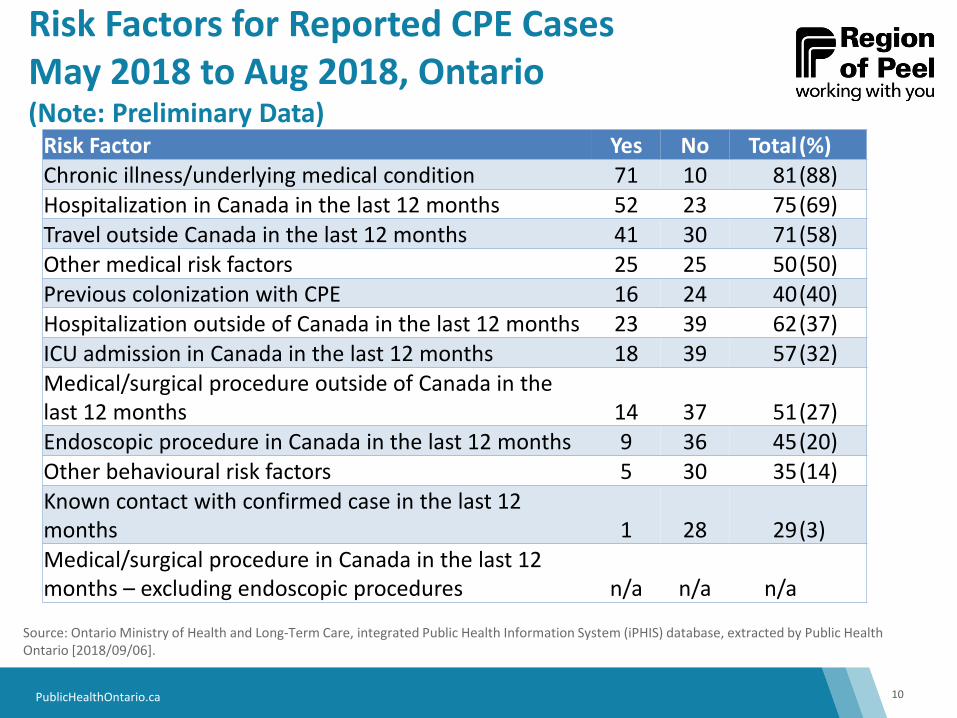
Risk Factors for Reported CPE Cases May 2018 to Aug 2018, Ontario (Note: Preliminary Data)
10
Source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2018/09/06].
Risk Factor Yes No Total (%) Chronic illness/underlying medical condition 71 10 81 (88) Hospitalization in Canada in the last 12 months 52 23 75 (69) Travel outside Canada in the last 12 months 41 30 71 (58) Other medical risk factors 25 25 50 (50) Previous colonization with CPE 16 24 40 (40) Hospitalization outside of Canada in the last 12 months 23 39 62 (37) ICU admission in Canada in the last 12 months 18 39 57 (32) Medical/surgical procedure outside of Canada in the last 12 months 14 37 51 (27) Endoscopic procedure in Canada in the last 12 months 9 36 45 (20) Other behavioural risk factors 5 30 35 (14) Known contact with confirmed case in the last 12 months 1 28 29 (3) Medical/surgical procedure in Canada in the last 12 months – excluding endoscopic procedures n/a n/a n/a
PublicHealthOntario.ca
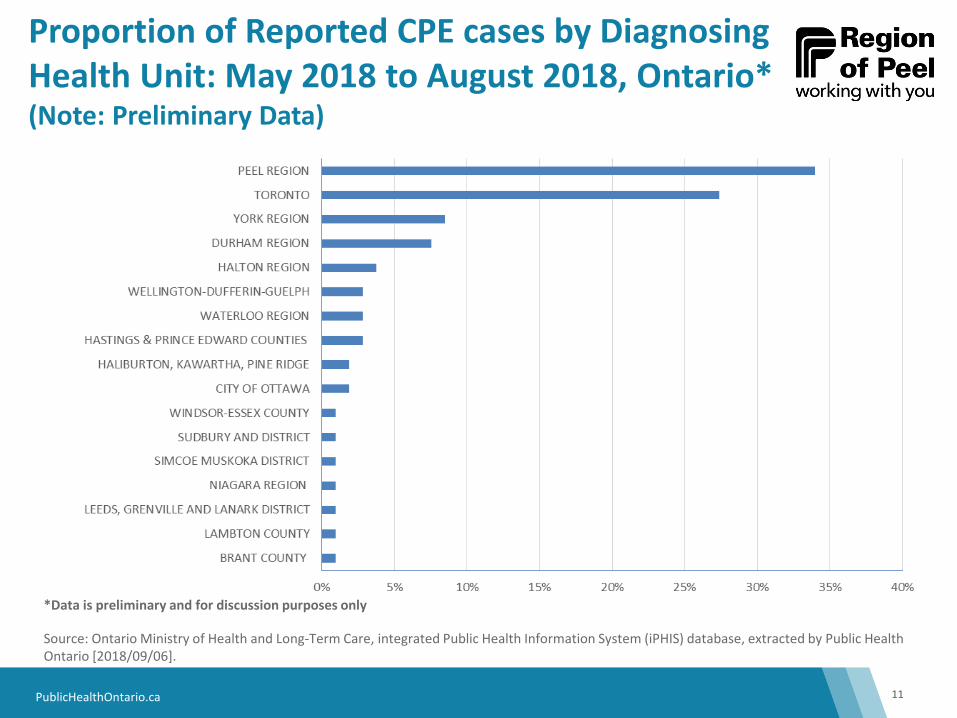
Proportion of Reported CPE cases by Diagnosing Health Unit: May 2018 to August 2018, Ontario* (Note: Preliminary Data)
11
*Data is preliminary and for discussion purposes only
Source: Ontario Ministry of Health and Long-Term Care, integrated Public Health Information System (iPHIS) database, extracted by Public Health Ontario [2018/09/06].
PublicHealthOntario.ca
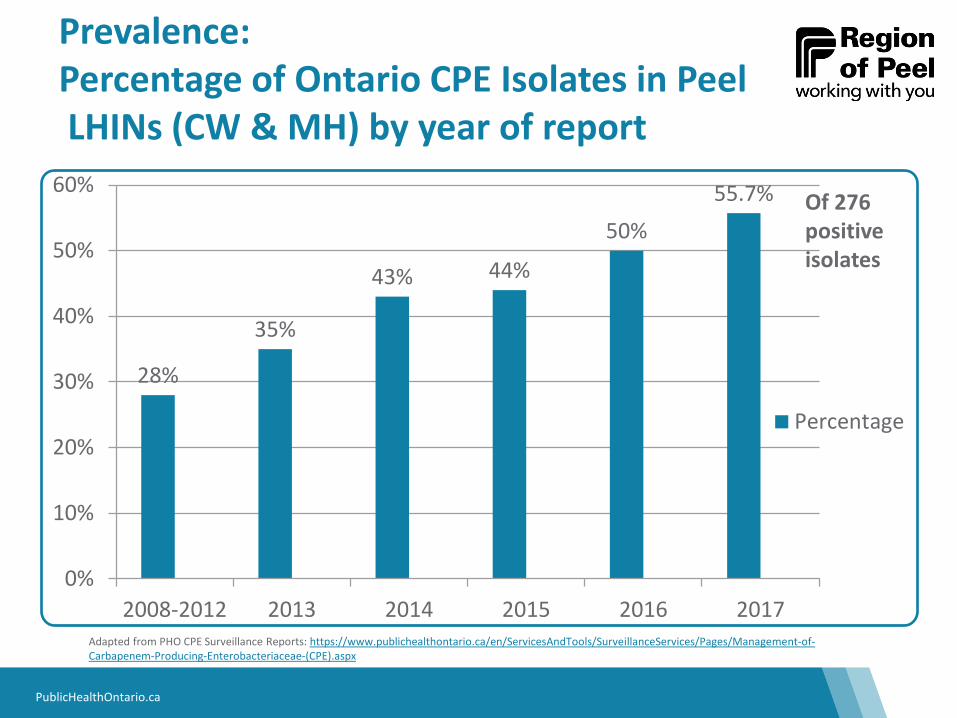
Prevalence: Percentage of Ontario CPE Isolates in Peel LHINs (CW & MH) by year of report
28%
35%
43% 44%
50% 55.7%
0%
10%
20%
30%
40%
50%
60%
2008-2012 2013 2014 2015 2016 2017
Percentage
Adapted from PHO CPE Surveillance Reports: https://www.publichealthontario.ca/en/ServicesAndTools/SurveillanceServices/Pages/Management-of-Carbapenem-Producing-Enterobacteriaceae-(CPE).aspx
Of 276 positive isolates
PublicHealthOntario.ca
Peel Data
13
• 34 cases since May 1st, 2018
• 65% of cases ≥ 60 years of age
• Urine and rectal swabs are the most common specimens
• 73% of cases identified from Acute Care
*Data is preliminary and for discussion purposes only ** Data extracted from iPHIS , Aug. 2018

PublicHealthOntario.ca 14
Peel Data: Disease Status May 1, 2018-August 16, 2018
53% 44%
3%
Colonized Infected Unspecified
*Data is preliminary and for discussion purposes only ** Data extracted from iPHIS , Aug. 2018
PublicHealthOntario.ca
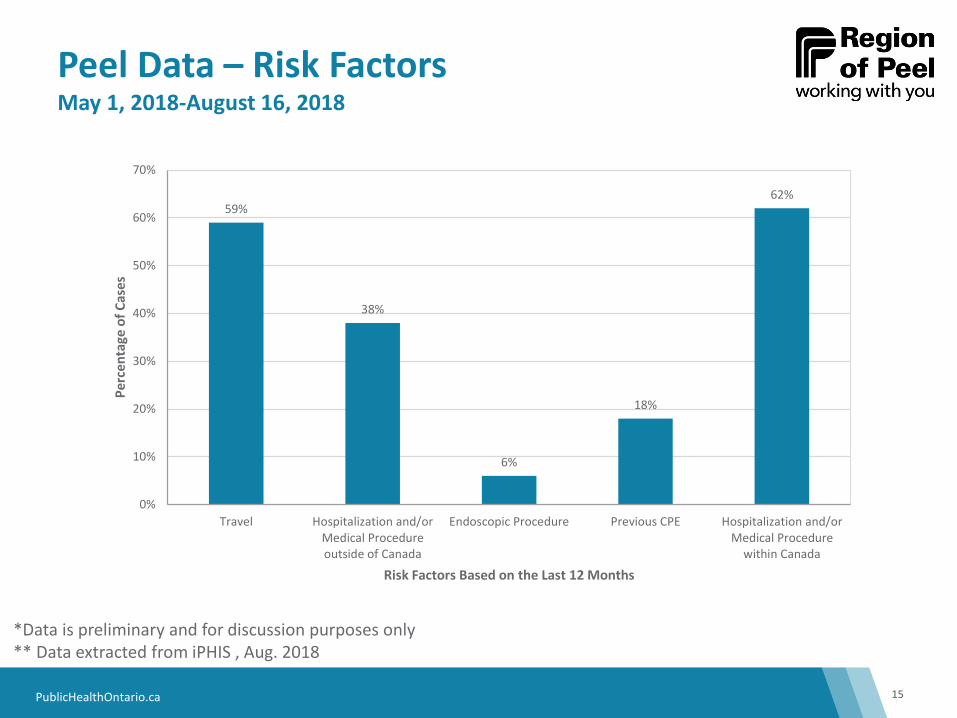
Peel Data – Risk Factors May 1, 2018-August 16, 2018
15
59%
38%
6%
18%
62%
0%
10%
20%
30%
40%
50%
60%
70%
Travel Hospitalization and/orMedical Procedureoutside of Canada
Endoscopic Procedure Previous CPE Hospitalization and/orMedical Procedure
within Canada
Perc
enta
ge o
f Cas
es
Risk Factors Based on the Last 12 Months
*Data is preliminary and for discussion purposes only ** Data extracted from iPHIS , Aug. 2018
PublicHealthOntario.ca
Recommended Screening for CPE
16
• Previously colonized or infected with CPE
• In the past 12 months been in receipt of health care • On the U.S. eastern seaboard region (e.g., New York City) • Greece • Israel • Indian subcontinent
• Travel to the Indian subcontinent in the past 12 months (even without exposure to health care)
• Receipt of care in any hospital that has reported transmission of CPE
• Contact of a known case of CPE
PublicHealthOntario.ca
Screening Specimens
17
• Rectal swab or Stool
AND, if indicated
• Urine
• Wounds
PublicHealthOntario.ca
Let’s Chat…
18
• How many of you attended last year?
• How many homes have experience with a CPE colonized resident?
• Are you screening for CPE on admission/re-admission?
• Has anyone had a nosocomial case of CPE?
• Have any homes conducted a CPE point prevalence?
• Do you have policies and procedures for AROs that include CPE?

PublicHealthOntario.ca
Scenarios
19
PublicHealthOntario.ca
Scenario # 1: Part A
20
You’ve received a lab report for a resident with a confirmed CPE in his urine. What now?!
PublicHealthOntario.ca
1. Prevent the Spread of CPE
21
• Initiate contact precautions • Gloves and gowns for direct resident care
• Private room accommodation
• Ensure adherence to hand hygiene
• Dedicate toileting - this is essential! • Private washroom or commode
• Dedicate resident equipment • Any equipment that cannot be dedicated must be thoroughly
cleaned and disinfected prior to use with another resident
Scenario # 1: Part A Continued
PublicHealthOntario.ca
1. Prevent the Spread of CPE
22
• Hand hygiene sinks for hand washing only • Body fluids and bath water should not be disposed in these
sinks
• Consider the use of chlorhexidine for bathing
• The resident can leave their room and go to the dining room and participate in community activities • Residents should always be reminded/helped to clean their
hands prior to leaving their room, before meals, or before they participate in any community activities.
Scenario # 1: Part A Continued
PublicHealthOntario.ca 23
Can we cohort residents with CPE?
Scenario # 1: Part A Continued
PublicHealthOntario.ca
1. Prevent the Spread of CPE: Accommodation
24
• A private room is always preferred
• Residents with the same gene of CPE (e.g. KPC) may share a room
• Preferably same organism too (e.g., E. coli)
Scenario # 1: Part A Continued
PublicHealthOntario.ca
1. Prevent the Spread: Duration of Precautions
25
• Follow up screening (rectal swabs) of 97/137 CRE patients post-discharge
• Time to clear – mean 387 days (95% CI; 312-463)
• Infected and colonized patients remain in contact precautions for entire hospital stay (PIDAC)
Scenario # 1: Part A Continued
PublicHealthOntario.ca
2. Investigate
26
• Case Definition: Laboratory confirmation of CPE (colonization or infection) by an Ontario microbiology laboratory
• All confirmed cases of CPE require investigation
• Overall, you want to identify if there is evidence to suggest that the case is associated with your home
Scenario # 1: Part A Continued
PublicHealthOntario.ca
2. Investigate
27
• Reason for specimen collection • Admission screen, clinical specimen, contact of a case
• Infection versus colonization? • If infected: signs, symptoms and onset date
• Medical risk factors: • Underlying medical conditions, medical/surgical procedures in last 12
months both within and outside Canada, endoscopy in Canada, hospitalization within and outside Canada, ICU admission in Canada in last 12 months, previous CPE colonization
• Behavioural risk factors: • Known contact with CPE case in last 12 months • Travel outside Canada in last 12 months
Scenario # 1: Part A Continued
PublicHealthOntario.ca
3. Reporting Requirements
28
For confirmed cases:
• An Infection Control Specialists (ICS) from the Region of Peel will reach out to you
For questions/concerns:
• CDI liaison is available to answer questions/concerns or they will direct you to an ICS
Communication: Open lines of communication are important
• Ensure that internal leadership team is aware of the CPE case • Most responsible person for infection prevention and control • Director of care/supervisor • Charge nurse/supervisor
Scenario # 1: Part A Continued
PublicHealthOntario.ca
Scenario #1: Part B
29
You’ve received a lab report of a resident with a CPE in their urine.
The resident has been sharing a room with another resident.
What now?!
PublicHealthOntario.ca
4. Contact Screening
30
Direct Contacts Unit Point Prevalence
• A minimum 3 sets of specimens should be taken on taken on different days, with at least one taken 21 days after last exposure
• Should be conducted following the identification of a single case on a unit
Scenario # 1: Part B Continued
PublicHealthOntario.ca
Scenario #1: Part C
31
You’ve received a lab report of a resident with a CPE in their urine.
The Environmental Services Manager comes to you to ask if any special cleaning is required.
How should you respond?
PublicHealthOntario.ca
5. Environmental Cleaning
32
• Routine cleaning and disinfection products are sufficient
• Consider enhanced sink cleaning and disinfection with enzymatic and sporicidal agents • Regularly (e.g., twice weekly) • Discharge/transfer cleaning for CPE room
• Appendix 7: Sample Procedure for Enhanced Shower and Sink Cleaning • PIDAC: Best Practices for Environmental Cleaning for Infection
Prevention and Control, April 2018
Scenario # 1: Part C Continued
PublicHealthOntario.ca
Scenario #2
33
A resident is returning to your LTCH and is now newly colonized with CPE.
1. How do you accommodate him/her?
2. Is funding for private rooms a barrier?
PublicHealthOntario.ca
High Intensity Needs Fund (HINF)
34
• A home may be eligible for reimbursement under HINF only when funding is not available through other sources and there is a need that cannot be adequately met without accessing the fund
• HINF can be used for those who occupy either a long stay bed or an interim short-stay bed
• The fund may be used for residents who require isolation related to infectious diseases where additional precautions are indicated
PublicHealthOntario.ca
Scenario #3
35
Your local hospital is asking you to accept a new resident who has CPE.
• Are you obliged to accept this resident?
PublicHealthOntario.ca
Before you Say No…
36
Some things to consider:
1. Can you accommodate a private room?
2. Are there residents who can be cohorted to create a private room?
3. Is there another resident with the same CPE gene that can be cohorted with the new resident?
PublicHealthOntario.ca
Scenario #4
37
• A family member of a resident with CPE has many questions and concerns. What tools and resources are available to support the home staff in answering the family members questions?
PublicHealthOntario.ca 38
Resources
PublicHealthOntario.ca
Thank You! Any Questions??
39
PublicHealthOntario.ca
Key References
40
• Public Health Ontario. Carbapenemase-producing Enterobacteriaceae (CPE). Available from https://www.publichealthontario.ca/en/BrowseByTopic/InfectiousDiseases/Pages/IDLandingPages/carbapenamase-producing-enterobacteriaceae.aspx
• Provincial Infectious Diseases Advisory Committee. Routine practices and additional precautions. Available from https://www.publichealthontario.ca/en/BrowseByTopic/InfectiousDiseases/PIDAC/Pages/Routine_Practices_Additional_Precautions.aspx
PublicHealthOntario.ca
Additional References
41
• Centers for Disease Control. Facility guidance for control of Carbapenem-resistant Enterobacteriaceae (CRE): November 2015 Update: CRE Toolkit. Available from http://www.cdc.gov/hai/pdfs/cre/CRE-guidance-508.pdf
• Mariappan S, Sekar U, Kamalanathan A. Carbapenemase-producing Enterobacteriaceae: Risk factors for infection and
impact of resistance on outcomes. Int J Appl Basic Med Res. 2017 Jan-Mar; 7(1): 32–39. Available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5327604/
• Parker VA, Logan CK, Currie B. Carbapenem-Resistant Enterobacteriaceae (CRE) control and prevention toolkit. (Prepared by Boston University School of Public Health and Montefiore Medical Center under Contract No. 290-2006-0012-l.) AHRQ Publication No. 14-0028. Rockville, MD: Agency for Healthcare Research and Quality. April 2014. Available from http://www.ahrq.gov/sites/default/files/publications/files/cretoolkit.pdf
PublicHealthOntario.ca
Additional Resources
42
• Public Health England. Acute trust toolkit for the early detection, management and control of Carbapenemase-producing Enterobacteriaceae. 2013. Available from http://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1317140378646
• World Health Organization. Global action plan on antimicrobial resistance. 2015. Available from http://apps.who.int/iris/bitstream/10665/193736/1/9789241509763_eng.pdf?ua=1





























