Embed Size (px)
Citation preview

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 1/24
1
VOL. 7, NO. 1 MARCH/APRIL 2
Dr. KevinGrumbach,MD, FAAFPProfessor and Chair
Dept. of Family andCommunity Medicine,UCSF
Optometry and Primary Care
CAPCI: Urgently RevitalizePrimary Care

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 2/24
22
Get MoreSupport
Larry Schwartz, M.D.Hill Physicians provider since 1985.
Uses Ascender preventive care reminders,
RelayHealth online communication tools
and Hill inSite to review eClaims and eligibility.
Get more information at www.HillPhysicians.com/Providers or contact:
Bay Area: Jennier Willson, regional director, (925) 327-6759, [email protected] Joaquin area: Paula Friend, regional director, (209) 762-5002, [email protected]
Sacramento area: Doug Robertson, regional director, (916) 286-7048, [email protected]
Practices afliated with Hill Physicians Medical Group retain their independence while enjoying
the support o a large, well-integrated network o providers. Hill’s advantages include:
tFast, accurate claims payments
tFree eReerrals, ePrescribing and online doctor-patient communications
tExperienced RN case management or complex, time-intensive cases
tDeep discounts on EPM and EHR solutions to help you meet the ederal mandate tEasy preventive care and disease management reminders or patients
tExtensive health resources that boost patient engagement
tHigh consumer awareness that builds practice volume
That’s why 3,800 independent primary care physicians, specialists and healthcare proessionals
have made Hill Physicians one o the nation’s leading Independent Physician Associations.
Get more or your practice and your patients by afliating with Hill Physicians Medical Group.
Hill Physicians’ 3,800 healthcare providers accept commercial HMOs rom Aetna, Alliance CompleteCare (Alameda County),
Anthem Blue Cross, Blue Shield, CIGNA, Health Administrators (San Joaquin), Health Net, United Healthcare WEST and
Western Health Advantage. Medicare Advantage plans in all regions. Medi-Cal in some regions or physicians who opt in.

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 3/24
3
• A 2009 New England Journal of Medicine study
concluded that rehospitalization is a frequent,costly and sometimes life-threatening event that is
associated with gaps in follow-up care.1
• Many studies suggest that end-of-life patients
who receive continuous curative care in lieu of
appropriate hospice or palliative care can
experience more pain and discomfort, a decreased
quality of life and even a shorter life span.2, 4
• At least two independent studies have shown
a 40 to 50 percent decrease in hospitalizationsfor patients who were appropriately and
willingly referred to hospice care.4, 5
A collaboration with VITAS Innovative
Hospice Care® benefits everyone involved:
• Interdisciplinary team— nurses, hospices aids,
social workers, chaplains, and physicians making
home visits as needed
• 24/7/365 availability— same day response, evenon weekends and holidays.
• VITAS Telecare— offers 24-hour direct
access to trained clinicians
• Intensive Comfort Care®— provides medical
management up to 24 hours per day
VITAS can help.
Serving California since 1995
For more information, please contact 1.800.723.3233 • VITAS.com
Curb Rising Hospital Costs
1 Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare Fee-for-Service Program. New England Journal of Medicine, 2009; 360:1418–1428.
2 Lynn J, Teno J, et al. Perceptions by family members of the dying experience of older and seriously ill patients. Annuals of Internal Medicine, 1997; 126:97–106.
3 Miller S, Mor V, et al. Does receipt of hospice care in nursing homes improve the management of pain at the end of life? Journal of American Geriatrics Society, 2002; 507–515.
4 Casarett D, Karlawish J, Morales K, Crowley R, Mirsch T, Asch DA. Improving the use of hospice services in nursing homes: A randomized, controlled trial. Journal of the American
Medical Association. 2005;294(2):211–217.
5 Gozalo PL, Miller SC. Hospice enrollment and evaluation of its causal effect on hospitalization of dying nursing home patients. Health Services Research. 2007; 42(2):587–610.
Leaders for a Reason
Frequent hospitalization of the terminally ill is a chronic condition
affecting medical groups and their patients:
Learn More
about how to
include hospice into
your care transition
model by calling
1.800.723.3233.

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 4/24
4
TA B L E O F C O N T E N T S
Notes From The President 5 Names In The News 14
Upcoming Events 17
Members List 18
CAPG Member Spotlight 22
CAPCI Aims to UrgentlyRevitalize Primary Care 7Optometry:A Visible Contributorto a Primary Care Team 15
A Vision for CAPCI 20
DEPARTMENTS:Publisher Valerie Okunami
CAPG Health Editor-in-Chief:Don Crane
Managing Editor:Lura Hawkins, MBA
Contributing writers:Blair BrysonDon CraneK evin Grumbach, MDElissa MaasWells Shoemaker, MD
Art Director Paul Galang
CAPG Health Magazine is published
byValerie Okunami MediaP.O. Box 674, Sloughhouse, CA 95683Phone 916.761.1853www.capghealth.org
Please send press releases and all other information related to this issue of CAPGHealth to [email protected] and /or c/o CAPG Health915 Wilshire Blvd., Suite1620Los Angeles, CA 90017
For advertising send email [email protected]
Subscription Rates:$32 per year; $58 two years; $3.00 single copy. Advertising rates on request.
Bulk third class mail paid inJeferson City, MOEvery precaution is taken to ensure theaccuracy o the articles published inCAPG Health Magazine.
Opinions expressed or acts supplied byits authors are not the responsibility o CAPG Health Magazine.
Copyright 2013, CAPG Health Magazine.All rights reserved. Reproduction inwhole or in part without writtenpermission is strictly prohibited.
FEATURES:
COVER STORY:Dr. Kevin Grumbach, MD, FAAFPProfessor and ChairDept. of Family andCommunity Medicine, UCSF 11

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 5/24
5
N O T E S F R O M T H E P R E S I D E N T
- am extremely proud to an-
nounce the creation o the Caliornia
Advanced Primary Care Institute (CAPCI),
a CAPG-sponsored nonproit educational
501(c3) oundation, which you can read
about in this issue o CAPG Health. The
new Foundation is supported by a broad
coalition o organizations rom the private
and public sectors as well as rom many segments o the healthcare community.
We believe this is the most comprehensive
collaborative eort ever to address the
alarming shortage o primary care physi-
cians. We also believe that the work we do
together will strengthen our structured
healthcare system and beneit society as
a whole.
Let me stress that CAPCI is an education-
al entity, not a political or lobbying organi-
zation. It brings together organizations as diverse as physician groups, health plans,
military and VA delivery systems, academ-
ics, hospitals and government agencies.
CAPG’s membership has already shown
its conidence in CAPCI by responding en-
thusiastically to a voluntary assessment to
help jumpstart the Foundation.
As exciting as this news is, we have
more. The 2013 CAPG Healthcare Coner-ence is certain to be a standout. Our ros-
ter o speakers is headed by President Bill
Clinton and includes a number o national
experts on healthcare. Please review the
advertisement in this magazine and sign
up early. The Conerence is June 6-9 at
the JW Marriott at L.A. Live in Downtown
Los Angeles. I look orward to seeing you there.
Sincerely,
Donald CranePresident and CEO
2 0 1 3 E D I T O R I A L C A L E N D A R
/dKZ/>WZdDEd^
ͻEŽƚĞƐ&ƌŽŵdŚĞWƌĞƐŝĚĞŶƚͻhƉĐŽŵŝŶŐǀĞŶƚƐͻEĂŵĞƐ/ŶdŚĞEĞǁƐͻW'DĞŵďĞƌ^ƉŽƚůŝŐŚƚͻ>ĞŐŝƐůĂƟǀĞhƉĚĂƚĞ
/^^h d,D Zd/>^ sZd/^/E' /d/KE> h h /^dZ/hd/KE
:ĂŶƵĂƌLJ
&ĞďƌƵĂƌLJ
DĂƌĐŚƉƌŝů
DĂLJ:ƵŶĞ
:ƵůLJƵŐƵƐƚ
^ĞƉƚĞŵďĞƌ
KĐƚŽďĞƌ
EŽǀĞŵďĞƌ
ĞĐĞŵďĞƌ
ĞĐĞŵďĞƌϳϮϬϭϮ
:ĂŶƵĂƌLJϯϭ
ƉƌŝůϮϲ
:ƵŶĞϭϰ
ƵŐƵƐƚƐϮ
KĐƚŽďĞƌϰ
EĞǁWŽůŝƟĐƐĂŶĚKůĚWƌŽďůĞŵƐ
,ĞĂůƚŚĐĂƌĞ
ZĞĨŽƌŵϮϬϭϯ
ĚǀĂŶĐĞĚWƌŝŵĂƌLJĂƌĞ
ZŝƐŝŶŐƚŽƚŚĞŚĂůůĞŶŐĞ
ϮϬϭϯW'ŶŶƵĂůŽŶĨĞƌĞŶĐĞ/ƐƐƵĞ
EŽǀĞůƉŚĂƌŵĂĐĞƵƟĐĂůĂƉƉƌŽĂĐŚĞƐŝŶĂƌĞĨŽƌŵŝŶŐ
ŚĞĂůƚŚƐLJƐƚĞŵŽŽƌĚŝŶĂƚĞĚĂƌĞŽŶĂŽŵŵƵŶŝƚLJ^ĐĂůĞ
dŚĞWƌŽŵŝƐĞŽĨKƐ
,ĞĂůƚŚ/dŽŶŶĞĐƟŶŐƚŚĞ
WƌŽŵŝƐĞĂŶĚƚŚĞWƌĂĐƟĐĂů
ĞĐĞŵďĞƌϭϮϮϬϭϮ
&ĞďƌƵĂƌLJϭ
DĂLJϯ
:ƵŶĞϮϭ
ƵŐƵƐƚƐϵ
KĐƚŽďĞƌϭϭ
,ĞĂůƚŚŝƐƉĂƌŝƟĞƐŽŶĨĞƌĞŶĐĞ
ĂŶĚEĂƟŽŶĂůWĂLJ&Žƌ
WĞƌĨŽƌŵĂŶĐĞ^Ƶŵŵŝƚ
W'ŽŶĨĞƌĞŶĐĞϮϬϭϯ
KŽŶŐƌĞƐƐ
For information about advertising or special promotions, contact Valerie Okunami at 916-761-1853.For editorial guidelines, email [email protected]

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 6/24
6
CAPG Healthcare Conference
10TH ANNUAL
JUNE 6–9, 2013JW MARRIOTT AT LA LIVE IN DOWNTOWN LOS ANGELES
WWW.CAPG.ORG/CONFERENCE2013
Presented by the California Association of Physician Groups
E XCI TI NG
N E W V E N U E!
Registration Is Now Open!

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 7/24
7
CAPCI Aims to Urgently RevitalizePrimary Care
continued on next page
By Wells Shoemaker, MD,
CAPG Medical Director
4 rimary Care is the cornerstone
for all of CAPG’s and, indeed, all of California’s healthcare delivery systems. Primary care also
sets the foundation for virtually every goal of
healthcare reform. Sadly, California faces a serious erosion of primary care workforce
at the same time that our state braces for a
daunting bulge in chronic illnesses and the long awaited opportunity to serve millions of
previously uninsured individuals and families
through reform.
In January, 2013, a new, broadly inclu-sive organization, the California Advanced
Primary Care Institute (CAPCI), launched a
multi-pronged effort to improve the appeal
of primary care as a career choice and elevate
the performance of our primary care teams to
respond to society’s pressing needs.
California’s primary care workforce willshrink by 30% in the next 5-8 years as a conse-
quence of two converging misfortunes. Baby
Boomer primary care physicians, for years the
load-bearing stalwarts among the internists,
family physicians, and pediatricians, are retir-ing. Newly trained clinicians have been pro-gressively choosing other medical disciplines, cutting the “reinforcements” down to half what they were 15 years ago.
Given the time it takes to train doctors,
advanced practice nurses, and physician’s as-sistants, this impending shortfall cannot be
entirely avoided.
Restoring the “numbers” is not realistic, and
we can’t solve this crunch but installing new
bearings on the old hamster wheel. We will
have to use scarce resources in smarter ways, many of them embedded in the concept of the MedicalHome…with new “street smarts.”
California’s primary care doctors will need
to practice team care in deed, not just PR,
sharing responsibilities intentionally. They
need information technology that answers questions and opens doors without exasper-ating time waste. They need to view patient empowerment as perhaps the most powerful
of allmedical tools. They’ll need to feel proud
of their work and simultaneously accept the humble culture of continual improvement.
That’s asking a lot from folks who are work-ing until8 PM already! They’llneed better cen-
tral support and fewer non-clinical demands
upon their time. To avoid hypocrisy in “well-
California Advanced
Primary CareInstitute Opened Operations In
January, 2013
CAPCI willmarshal California’s collective experience in educa-tion, clinical science, coordinat-ed care, ethical management, and cultural responsiveness to drive sustainably improved per-formance of our primary care delivery systems for all people
who live in our State.
• By expanding the medicalhome promise to make ad-vanced, patient-centered care a reality on a community wide scale, CAPCI willhelp to restore the appeal of primary care as a career choice for promising young professionals.
• CAPCI will serve as the State’s best informed, most inclusive source of knowledge to agen-
cies seeking to further the Triple Aim of Better Health, Better Care, and Better Af-fordability.
• CAPCI recognizes the urgency of this mission as the threat-ened constriction in work-force overlaps with the wel-come opportunity to serve millions of newly covered in-dividuals through healthcare reform.

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 8/24
8
The list o CAPCI’s Steering Coun-cil and Executive Management Committee’s members reads like a “Who’s Who” o primary care in Caliornia. They have the will, the experience, and the juice to get things done. CAPCI’s goals are
congruent with our organization’s strategic plan, especially transorm-ing medical practices to the Patient Centered Medical Home (PCMH) /team-based model o care.
Susan Hogeland, CAE Executive Vice President,California Academy of Family Physicians
Conspicuously, no previous California
effort has succeeded in changing primary care workforce dynamics on a large scale.
What is CAPCI doing that offers hope for a different outcome? Two answers: Inclu-sivity and Scope.
1. Inclusivity. Instead o looking through the keyhole o a single in-terest, CAPCI has engaged private sector delivery systems, community clinics, military and VA systems, and independent doctors. However, reining the delivery system is not
Kick Starting Primary Care: How it happened
CAPG sponsored a statewide
consensus meeting in April, 2012, eaturing the “Big Tent”philosophy o attention to as many angles as possible.
The core development team emerged rom that meeting, and ater 6 months work, CAPCI emerged with its name, its mis-sion, and early unding.
CAPCI convened its irst ple-nary Steering Council meeting in January, 2013, and all “Four
P’s” now have active work-groups.
CAPCI is chartered as a non-proit 501c3 oundation under the sheltering wing o the CAPG Educational Foundation. CAPCI has received kick-start unding through a contribution rom each o CAPG’s member groups, ollowed by a plan-ning grant rom the Caliornia HealthCare Foundation. Sub-
sequent unding through The Caliornia Endowment and the Caliornia Academy o Family Practice has put CAPCI deinite-ly “on the road.”
enough. CAPCI will also eature es-
sential voices o academic teaching centers, primary care academies (am-ily practice, internal medicine, and pediatrics), advanced practice nurse clinicians and physician’s assistants. Add Health Plans private and public, public health, employers, state and ederal government, quality improve-
ment organizations, and healthcare oundations to reach a critical mass. CAPCI is committed to hearing and heeding the Patient Voice early in every strategy.
Redesign Is Now Essential:Lance Lang MDIt is exciting to accept the chal-
lenge to support practice redesign eorts across Caliornia. The core o this eort will include team based care, improved access to care, and enhanced partnership with pa-tients…all with the goal o a more eective and satisying practice.
Lance Lang MD, Medical Direc-tor, CAPCI and also CaliforniaQuality Collaborative
continued from page 7
continued on next page
The Right People: Susan Hogeland
ness” counseling, these workers need a healthi-er, more family-friendly work-life balance.
The training environment is going to
change, and Dr. Grumbach is lighting the way.
“If we are going to transform primary care to provide superb, patient-centered
care to every Californian, we will need
to fundamentally change our approach
to training the people who work in pri-mary care. CAPCI represents an unprec-edented partnership between practice
organizations and training institutions to
equip the workforce for the innovative
care models that will drive excellence
in primary care throughout California.”Kevin Grumbach, MD, Professor and Chair,UCSF Department of Family and Commu-nity Medicine.

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 9/24
9
Revitalizing primary care is para-mount for all of us. In San Diego, multiple stakeholders have come together to create “systems” of care that serve the entire popula-tion and improve care in each sec-tor. K ey participants have included
the four major delivery systems (K aiser, Scripps, Sharp, and UCSD), the military health systems (Navy andVA), our Councilof Community
Clinics (FQHCs), San Diego County
Health and Human Services, and a number of commercial, senior, and
Medi-Cal health plans.
We have focused centrally on
advancing primary care through
patient-centered medical home
models. Allmembers of this multi-stakeholder collaborative agreed
that primary care must be the foundation for our health system, provided in a team-based fashion,
with an emphasis on management of chronic disease, prevention, and
improved access. For perhaps the first time these typically separate entities have:
• shared practice innovations as well as disappointments,
• collaborated on initiatives to enhance team-based ap-
Primary Care as a Community Endeavor: John Jenrette MD
proaches to care,
• identified community resourc-es to improve case manage-ment efforts,
• focused on identification and
management of patients with chronic disease and behavioralhealth needs.
CAPCI promises to extend col-laborations of this nature throughout other parts of California.
John Jenrette MD, CEO SharpCommunity Health Group, and Chair, CAPG Board of Directors
Never has such a broad platform been
established, and none too soon. With
the crunch bearing down, every one of those parties “has a dog in this race.”
2. Ambitious Scope of Engagement. Previous efforts have looked at only
one or two facets of the challenge, for
example, payment disparities or pa-perwork burden. CAPCI believes that simultaneous efforts need to be made
in 4 distinct areas in order to turn this
around.
We call those the “Four P’s.”
1. Pipeline. Change the training
environment and the appeal of primary care as a career choice
for physicians and other clinical
professionals. (See Dr. Grumbach’s
detailed analysis elsewhere in this issue.)
2. Practice redesign. Practice
with team mentality for greater efficiency, better information, modern communication, and
central attention to the patient experience. This is the promise of the Medical Home, but it needs to
expand beyond individual offices to reach community wide scale. In
California, any effort to redesign
must centrally embrace California’s unique cultural diversity.
3. Payment. Bluntly, this is all talk unless payment is aligned with the
modernized practices to deliver the core of healthcare reform. In
California with literally dozens of payors, hundreds of benefit designs, a mix of capitation and
fee-for-service, no one approach
has enough “heft” to inf luence
behavior change at the practice
level. CAPCI aims to reach a “tip-ping point” of purchaser strategies, building upon the “United Nations”
forum of the Integrated Healthcare Association and expanding that to
additional stakeholders.
4. Policy. American healthcare policy has been pinning so many tails on
the donkey over the last 60 years that we can’t see the donkey any more. The hodgepodge of as-sumptions, regulations, and “con-ventional wisdom” has landed the
USA lower than 20th in the world
in nearly every public health meas-ure. Intelligent policy, this time
informed by a broad-based con-
sensus of contributors with prag-matic experience, will need to help
policy makers become enablers for progress.
Why does CAPCI believe simultaneous thrusts on all Four P’s are necessary? Previ-ous efforts failed because they only touched
several of these key underpinnings. Having
gone through med school owning a small
foreign car of some notoriety for reliability, I’d say that rest restoring California’s primary care workforce is like reviving a disabled car. You can repair the engine and change the
oil, but without 4 good tires, reliable brakes, and a steering wheel, you won’t get very far.
Primary care revitalization needs all of the Four P’s.
Notably, many of these elements overlap
with Governor Brown’s Let’s Get Healthy California initiative, starting also in 2012
under Secretary Diana Dooley’s leadership
with with Don Berwick’s key support, is now
auspiciously drilling deeper in 2013. The
System Redesign workgroup will share a great deal of torque with CAPCI.

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 10/24
10
CAPCI GovernanceFebruary, 2013
Executive Management Committee:
Alan Glaseroff MD, Professor, Director Stanford Coordinated CareDavidNace MD, President, Patient Centered Primary Care Collaborative (PCPCC)Diane Stewart, Pacific Business Group on HealthDonCrane, CEO, CAPG
John Jenrette MD, CEO of Sharp Community MedicalGroup in San DiegoKevin Grumbach MD, Professor and Chair, Department of Family Practice, UCSFLance LangMD, MedicalDirector, CaliforniaQuality Collaborative (CQC)
Sharon Levine MD, The Permanente Medical GroupSusan Hogeland, EVP, California Academy of Family PhysiciansTomWilliams DrPH,CEO, Integrated Healthcare Association (IHA)Wells Shoemak er MD, MedicalDirector, CAPG,& co-chair, CQC
Steering Council includes the EMC members and:
Angela Minniefield MPA, Charles Drew University of Medicine& ScienceBeth Grivett PAC, American Assn of Physicians AssistantsBetsy StapletonRN FNP (Patient leadership strategy consultant, Humboldt County)Betsy Thompson MD DrPH MedicalDirector CMS Pacific Region
BobMoore MD,CMO, Partnership HealthPlan of California (Medi-CalManaged Care)DavidQuack enbush, California Primary Care Association (CPCA)Heather Young RNPhD, Dean, UC Davis School of NursingHector Flores MD, White Memorial & Family Care SpecialistsLarry Shore MD, MedicalHome Pilot, Brown& Toland Physicians, SFLaura Dolata, MSN, FNP-BC, Director, Ambulatory & Specialty Programs, San Diego VA
Mary Fermazin MD, MedicalDirector, HSAG, California’s MedicareQIOMary FoleyRNPhD, Director, UCSF Center for Nursing Research and Innovation
Mik eBelman MD, Senior MedicalDirector, Anthem Blue CrossMollyCoye MD, UCLA Innovations Officer, former CA Health Services Director
Neil Solomon MD, Senior MedicalDirector, Health NetRonChapman MD, Director, California Department of PublicHealthSunnyRamchandani MD LCDR, US Navy Medicine West

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 11/24
11
continued on next page
By Kevin Grumbach MD, FAAFP
%ter decades o neglect, the nation has rediscovered that primary care is the oundation or high perorming health care.
President Obama understands that suc-cessul implementation o the Aordable Care Act depends on robust primary care.
In a health reorm town hall in 2010, he stated, “It used to be that most o us had a amily doctor; you would consult with that amily doctor; they knew your history, they knew your amily, they knew your children, they helped deliver babies. How do we get more primary physicians, number one; and number two, how do we give them more power so that they are the hub around which a patient-centered medical system exists? ”
We need to answer the President’s ques-tions!
Leaders o corporate America, strug-gling with how to purchase better value health coverage or their employees, also
“get it.” Testiying beore the House Ways and Means Committee in 2009, Randy McDonald, Senior Vice President at IBM, commented, “What is the single most im-portant thing to ix in health care? Primary care. Strengthen primary care–transorm it
and pay dierently using a model like thePatient Centered Medical Home.”
But here is the problem: What i primarycare medical homes become an impera-
tive, but there is no one home at the medi-cal home?
Primary care aces the challenge o adepleted and oten demoralized primarycare workorce. Only hal as many US medi-cal school graduates are entering amilymedicine residency programs today as 15
years ago. During the same period, thenumber o residents completing training ininternal medicine and planning to practiceas general internists rather than enteringsubspecialty ields dropped by 50%. Simi-lar trends are occurring among graduateso physician assistant programs.
While policymakers do not agree on theexact extent o the primary care workorceshortage, most agree that it is large. TheAssociation o American Medical Collegesprojects a shortage o 29,800 primary care
C O V E R S TO R Y
Restoring the Joy of Primary Care
“...physicians have amongthe highest rates of profes-sional burnout of all special-ties. Far too many primary care practices are ill-designed
to meet the demands of high performing, 21st Century primary care, with the conse-quence that patient needs arebeing inadequately met.”

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 12/24
12
physicians in 2015, growing to a deicit o 65,800 in 2025. Our own research in Cali-ornia conducted or the Caliornia Health-Care Foundation indicates that only 16 o the state’s 58 counties currently meet the minimum supply o primary care physi-cians considered adequate--at least 1 pri-mary care physician or every 1700 people. As millions o Caliornians gain insurance coverage in January, 2014, the state aces a major challenge assuring there will be adequate primary care capacity to deliver access to care or the newly insured.
Why is this happening?
What explains the decline o the primary care workorce? Some o it is undoubtedly attributable to a medical education culture at US medical schools that celebrates spe-cialization and biomedical research and discourages student interest in primary care. I continue to hear rom medical stu-dents about a aculty member or resident in a non-primary care ield telling them that they were “too smart” to become a amily physician. But almost certainly the most powerul actors in luencing medi-
cal student career choices are those in the
practice environment.
A key environmental actor is physician compensation. Students don’t make it into medical school without being able to count, and the growing income gap between primary care and specialist physi-cians is not lost on students.
A study reported in JAMA ound that residency match rates are highly correlated with the average earnings o physicians in the specialty; the higher the average earn-ings o a specialty, the more likely the spe-cialty is to ill its residency programs with US medical school graduates. Another
study perormed or the ederal Council on Graduate Medical Education showed that over the past 30 years, the percentage o medical graduates planning careers in pri-mary care ebbs and lows in parallel with therelative earning power o primary care physicians relative to specialists.
The Aordable Care Act took some mod-
est steps to enhance payments or primary care, including a 10% Medicare bonus or primary care. Eective this year, ACA man-
dates that Medicaid programs pay at least Medicare rates or primary care. However,
continued from page 11 physician groups in Caliornia will need toask what they can do to address the prima-
ry care-specialty income gap to recruit newphysicians into primary care. Some largemedical groups are already reaching wellbeyond the 10% Medicare bonus to attractnew primary care physicians. For example,the Permanente Medical Group is oeringsalaries to new primary care graduates wellabove community standards, along withinterest-ree loans contingent on retentionin the group.
The second major discouraging practiceenvironment actor is the dysunctionalnature o many primary care practices. It
is not uncommon or UCSF medical stu-dents to remark to me about their amilymedicine clerkship, “I so admired the no-ble work being done by my primary carepreceptor. She is a wonderul doctor. But Icould never see mysel working so hard…in such an unsupportive environment.”
A recent national study conirmed thatprimary care physicians have among thehighest rates o proessional burnout oall specialties. Far too many primary carepractices are ill-designed to meet the de-
continued on next page

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 13/24
13
mands o high perorming, 21st Century primary care, with the consequence that patient needs are being inadequately met. The primary care clinicians know that, and they are experiencing rustration and burnout.
Transorm the ability to deliver the pa-tient service doctors envisioned when they made their career choice, and the doctors will respond.
Mak e that a Quadruple Aim
The wave o transormation o primary care has been condensed into the Triple Aim o better health, better patient experi-ence, and more aordable costs. I believe that the transormation o primary care is really about achieving the a ourth aim: Make primary care a joyul and sustainable career.
Call it what you will—Patient Centered Medical Homes, Advanced Primary Care, or just Darn Good Primary Care—the goalis clear and essential or meeting the needs o the public and renewing the primary care workorce. The transormation in-cludes several elements—what my UCSF colleague Tom Bodenheimer reers to as the “Ten Building Blocks o High Perorm-
ing Primary Care.” These include:
1. engaged practice leadership
2. data-driven improvement
3. new team-based models where health proessiona ls and allied health workers share the care and practice at the top o their skill
4. innovative approaches to coordinat-ing care or complex, high risk and high utilizing patients, and
5. moving beyond ace-to-ace encoun-
ters towards a more encompassing view o patient touches that includes web-enabled virtual visits and other modalities.
There is Hope
The spirit o innovation and improve-ment inusing primary care is starting to kindle renewed excitement and inter-est in primary care among students and residents. Trainees are eager to engage in the process o reinventing primary care—helping to create their own uture as the
next generation o primary care clinicians.
Those o us who are educators are keenly interested in ensuring that our learners are trained in practices that embrace innova-tion and advanced primary care models. We
need training sites that demonstrate that primary care is a highly satisying and do-able job …and engage learners in practice improvement. We look to physician groups in Caliornia to partner with us in the educa-tional enterprise and make their exemplary primary care practices teaching sites.
For our own part, we recognize the need to transorm primary care practices in academic health centers—many o which are hardly paragons o advanced primary care. But even academic health centers are inected with the spirit o primary
care transormation. The University o Caliornia Oice o the President is hosting leaders rom all ive University o Caliornia medical centers and medical schools in March or an unprecedented UC summit on primary care delivery reorm. Last year, the Stanord School o Medicine appointed its irst ever Assistant Dean o Primary Care. Schools o nursing, pharmacy, dentistry and allied health are also actively involved in reorming their training and practice models to align with the principles o high perorming primary care.
The Interdependent 4Ps
I am pleased to serve as a member o thesteering committee or the newly ormedCaliornia Advanced Primary Care Institute,and delighted that CAPG is playing such
a pivotal role in launching CAPCI. As aneducator, I am particularly interested in thePipeline component that is one o CAPCI’s“4P” priority areas.
But in truth, advances in the primarycare workorce pipeline will be highlydependent on success in CAPCI’s other 3Ps: Payment reorm, Practice Redesign,and Policy. Strengthening the primary
care pipeline will require new methods orcompensating primary care physicians andclosing the primary care-specialty earningsgap, transormed practice models thatmake primary care a proessiona lly reward-
ing job, and the policy changes needed tosupport reorms in payment and practice.Physician groups in Caliornia have a criti-cal role to play in renewal and reorm oprimary care in the state.
Dr. Grumbach is Professor and Chair, De- partment of Family and Community Medi-cine at UCSF. A frequent contributor to the
national primary care literature and debate,he helped to craft CAPCI’s approach to pri-mary care revitalization and serves as Chair of CAPCI’s broadly inclusive Steering Council.

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 14/24
14
USC RECRUITS TWO RE-NOWNED NEUROSURGEONS TO BOLSTER MULTIDISCIPLI-NARY SPINE CARE CENTER
The University o Southern Caliornia an-
nounces the recruitment o two esteemed spine surgeons who will play critical roles in expanding a multi-disciplinary, academic-based spine center at the K eck MedicalCenter o USC. John C. Liu, M.D., and Frank Acosta, M.D., join other neurosurgical and orthopedic spine experts at USC and began seeing patients on February 1, 2013.
Liu, a recognized leader and considered a pioneer in minimally invasive surgicaltechniques or the spine, has been named proessor o neurosurgery and director o the spine division at the K eck School
o Medicine o USC. Acosta, a ellowship-trained neurosurgeon in complex spine deormity, has been named associate pro-essor o neurosurgery at the K eck School.
JEFFREY WASSERMAN NAMED NEW VICE PRESIDENT AND DIRECTOR OF RAND HEALTH
Jeffrey Wasserman, a health policy expert who has led efforts to strengthen the Unit-ed States’ preparedness for a major health
event, has been named vice president and
director of the health research division at the RAND Corporation, RAND President and
CEO Michael D. Rich announced.
Wasserman is a longtime RAND re-searcher and a widely recognized expert on health policy issues. He has led eorts to create the National Health Security Strategy, a ederal project to prepare the nation’s health system to respond to large-scale incidents, such as a terrorist attack or
N A M E S I N T H E N E W Sa pandemic disease outbreak that could pose a major threat to the public’s health.
He was co-principal investigator o RAND’s Comprehensive Assessment o Re-orm Eorts (COMPARE) initiative, created
to help evaluate healthcare reorm propos-als. The health system models created by that project are being used by many gov-ernment agencies to help guide adoption o the ederal Aordable Care Act.
NEW CEDARS-SINAI CLINICPROVIDES EXPERTISE INPEDIATRIC NEUROGENETIC, NEUROMUSCULAR DISORDERS
Southern Caliornia pediatricians, pedi-atric neurologists and parents o children
with inherited neurological diseases or nerve-related muscle disorders have a new resource or expert diagnostics, genetictesting, and state-o-the-art research and treatment acilities: Cedars-Sinai’s newly opened Pediatric Neurogenetics and Neu-romuscular Clinic.
Many pediatric neurological disorders –especially rare ones – are hard to diagnose because symptoms can be nonspeciic and routine tests inconclusive, according to clinic co-directors Robert H. Baloh, MD, PhD , who treats and studies neuromuscular dis-orders, and Tyler M. Pierson, MD, PhD , an expert in child neurology who researches genes and molecular mechanisms that cause neurological disorders.
“When an inant or child shows signs o a disorder o the brain, spinal cord, nerves or muscles, a pediatrician or pediatric neu-rologist in the community usually would like to reer them to a specialty clinic at a large treatment and research center, but many o these disorders have overlapping
symptoms, making it diicult to knowwhich clinic is most appropriate. Our clinicremoves this burden because research andtreatment experts rom several disciplinesevaluate each child’s case to develop test-ing and ollow-up strategies. As we reach a
diagnosis, the appropriate expert takes thelead, coordinating ongoing care with thereerring physician,” said Baloh, directoro Neuromuscular Medicine in the Depart-ment o Neurology.
Pierson said the clinic is designed toefficiently help parents coping with unex-pected and often heartbreaking situations.Physicians or parents may find out moreabout the PediatricNeurogenetics and Neu-romuscular Clinic by calling (310) 248-8960.
OUTDOOR FAST-FOOD ADS LINKED TO OBESITY
Researchers rom the University o Cali-ornia, Los Angeles ound that people livingin areas with the most outdoor ood adver-tising were more likely to be obese thanresidents o areas without these signs andbillboards. Although they didn’t say the adscause weight gain, they did note a “modest
but clinically meaningul increased likeli-hood o obesity.”
“Obesity is a signiicant health problem,so we need to know the actors that con-
tribute to the overeating o processed ood,”Dr. Lenard Lesser, who conducted the studywhile he was a Robert Wood Johnson Foun-dation clinical scholar in the UCLA Depart-ment o Family Medicine, said in a Universitynews release.
For the study, published online January10 in the journal BMC Public Health, the re-searchers examined 200 census tracts romtwo densely populated areas. One area wasin Los Angeles, the other was in New Orle-ans. High- and low-income individuals livedin both places.
They detected an increased likelihoodo obesity in neighborhoods with the mostoutdoor ast-ood ads. “For instance, in atypical census tract with about 5,000 peo-ple, i 30 percent o the outdoor ads weredevoted to ood, we would expect to ind anadditional 100 to 150 people who are obese,compared with a census tract without anyood ads,” explained Lesser.
The researchers said more studies areneeded in other locations to investigate thelink between outdoor ast-ood ads and riskor obesity. UCLA team members monitor antibiotic use. CAPG’s Case Studies in Excellence 2013 coming in May.

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 15/24
15
8 he future of primary care in the
United States is team care...where all mem-
bers practice close to the limits of their train-
ing and experience, with rapid information
exchange and tightly coordinated respons-
es. We have superb examples in California
for the shared responsibility between MD’s,
DO’s, PharmD’s, Podiatrists, Advanced Prac-
tice Clinicians, RD’s, educators, and other
disciplines.
K arin Meng OD has practiced clinical op-
tometry in the Bay Area for 27 years, and we
shared this dialogue regarding the potentialrole for optometrists (OD’s) in the expanded
primary teams of the next decade.
Dr. Shoemaker: Dr. Meng, can you de- scribe the differences between ophthal-mology and optometry in training and daily work?
Dr. Meng: Sure. After obtaining an under-
graduate degree, ophthalmologists earn an
MD degree after 4 years of medical school.
This is followed by a 1 year transitional in-
ternship, which can be in any branch of med-
Optometry: A Visible Contributor toa Primary Care Team
icine, followed by a 3 year surgical residency.
Many ophthalmologists pursue additional
fellowship training, such as retina, glaucoma, cornea, or neuro.
Doctors of optometry (OD’s), after com-
pleting an undergraduate degree, complete
4 years of optometry school and frequently
a 1 year non-surgical residency. Years 1 and
2 include course work very similar to general
medical education. Many programs involve
adjunct faculty from medical programs pro-
viding instruction in anatomy, physiology,
and clinicalmedicine. Years 3 and 4 focus on
clinical education. Students graduate with
2,500-3,000 patient encounters. Additional
residency adds at least 1,200 patient en-counters to that count. These include a mix
of post-surgical, medical, and routine visits.
• The central focus of ophthalmology is
surgery and management of complex
diseases of the eye. These specialists do
precious work, and their schedules are
typically heavily committed, including
time in the OR.
• Doctors of optometry provide the lion’s
share of routine care (>70% of all eye
care visits) with a growing focus on
medical and primary care adjunctive
evaluations such as diabetes. Most OD’s
spend 20% of their clinic day on medical
and post-surgical conditions, althoughsome run much higher.
Dr. Shoemaker: For many physicians,the eye is a mysterious place...with its ownarcane nomenclature, elaborate tools of the trade, and huge stakes as possibly ourmost treasured organ system. All primarycare physicians use a hand held ophthal-moscope, which is rather limited, frankly.Very few PCP’s have access to a slit lamp...or know how to use one. What are the toolsthat allow an optometrist to accuratelyidentify problems that a PCP struggles to
see?
Dr. Meng: All OD’s routinely employ
a slit lamp. This instrument offers a 3 di-
mensional, magnified view of the anterior
segment of the eye to detect corneal abra-
sions, foreign bodies, conjunctivitis, iritis,
cataracts, etc. We use f luorescein staining to
distinguish conditions such as early herpetic
keratitis. It’s hard to make these distinctions
with a hand held ophthalmoscope, which
offers only a 2 dimensional view. The cor-
rect treatment for these conditions...and the
avoidance of damaging complications...can
depend completely on making the correctinitial diagnosis.
OD’s also use a condensing lens to view
the retina and optic nerve in great detail...
critical for diabetic exams, retinal tears, and
hypertensive retinopathy. A gonioscopy
lens is employed to check the angles of the
eye for glaucoma. A tonometer is an at-
tachment to the slit lamp that measures the
pressure of the eye. K eratometers are also
standard equipment, which measures the
curvature of the cornea. This device is useful
continued on next page
An interview with
Wells Shoemaker, MD
Karen Meng, OD

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 16/24
16
for fitting contact lenses and also detecting
keratoconus. That’s not the whole list, but
you get the picture.
Dr. Shoemaker: OK, optometrists cer-
tainly prescribe glasses and contacts, and these are typically low stress, scheduled appointments. But beyond that...can youdescribe the capabilities in every optome-trist’s office to diagnose and manage acutediseases of the eye?
Dr. Meng: All OD’s in California can diag-
nose mild to severe eye problems such as
serious eye infections, inf lammations of the
eye, trauma, foreign bodies, and glaucoma,
using the tools we described earlier.
Most visits for acute problems can be
treated by the OD, but others are referred. The OD recognizes the urgency of certain
situations and can communicate effectively
with the ophthalmologist when time is of the
essence.
We see our patients more frequently than
you might think. Current statistics indicate
that 99.4 million eye exams are performed
yearly as compared with 27.5 million general
physical exams nationwide. Routine exams
address known issues, such as diabetes, but
in many cases they can detect early signs of
eye disease and ocular signs of systemic con-
ditions such as hypertension or dyslipidemia.
Dr. Shoemaker: It sounds like a great opportunity for an OD, using an integrated
record system, to reinforce sound medical advice and identify patient concerns that
might go on for months otherwise. What would it look like if an optometrist were aformal member of a modern primary careteam?
Dr. Meng: Clear task definition and lines
of communication, for starters. In the past,
OD’s have not actively forged relationshipswith primary care medicine, and that would
take some personal work to change. The
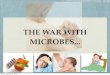
The healthy retina
Macular Degeneration Diabetic Retinopathy is one of the leading causes of blindness.
continued from page 15
continued on next page

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 17/24
17
U P C O M I N G E V E N T SCAPG Contracts Committee (No Cal)March 21, 2013
Oak land, CA*
CAPG Contracts Committee (So Cal)March 28, 2013
Los Angeles, CAPG Oice *
CAPG Health Information Technology CommitteeApril 9,2013
Web-ex /Teleconerence *
CAPG Public Relations/MarketingCommitteeApril 16,2013
Los Angeles, CAPG Oice *
CAPG Inland Empire Regional
CommitteeApril 17, 2013
Riverside, CA *
CAPG Human Resources CommitteeApril 23,2013
Los Angeles, CAPG Oice *
CAPG San Diego Regional CommitteeApril 24,2013
San Diego, CA *
CAPG Pharmaceutical Care CommitteeApril 30,2013
Los Angeles, CAPG Oice *
CAPG General Membership (So Cal)May 7, 2013
Los Angeles, CAPG Oice *
CAPG State Government ProgramsCommitteeMay14,2013
Los Angeles, CAPG Oice *
CAPG Medical Policy CommitteeMay14,2013
Los Angeles, CAPG Oice *
CAPG General Membership (No Cal)May16,2012
Oak land, CA *
2013 Annual CAPG HealthcareConferenceJune 6-9, 2013JW Marriott, LA LIVE
www.CAPG.org /conerence2013
2013 Health Care Provider ConferenceJune 13-14,2013 The Westin, San Diego
www.hasc.org /2013WellnessConerence
* For more inormation contact CAPG at (213) 642-CAPG
continued from page 13
potential is definitely there.
Given the geographic distribution and
spread among urban, suburban, and rural ar-
eas, OD’s are well positioned to enhance the
primary care network. Utilizing the roughly
5,000 doctors of optometry, even to a partial
degree, would help soften the impact of the
impending PCP workforce shortage.
Dr. Shoemaker: Interesting! If such a
remodeled team were tested, what would
you suggest might be an optimum ratio of
primary care physicians to OD’s?
If the intended use for OD’s is specialty
care and routine eye care, that ratio would
likely range from 15:1 to 10:1. That might
change if OD’s were included in more team-
based chronic care management.
Dr. Shoemaker: Sounds like an worthy
study! CAPG’s member groups uphold carecoordination as their key contribution tobetter care. Fully integrated groups could relatively quickly create “pods” of primary care doctors with optometrists in the samebuilding or campus for same day consulta-tion. But...how might that look in an IPA?
IPA’s could create a virtual “eye home”
where OD’s and ophthalmologists work in a
protocol-defined partnership to offer a cost
efficient model. A fair number of the routine,
chronic care visits as well as common acute
eye problems would easily fit with forms that
could be electronically shared and incorpo-
rated into a shared medical record.
There are definitely a number of clinical
problems where the right tools and the right
diagnosis can make a big difference in pa-tient outcomes...and these generally require
reliable, same day visits. OD’s in a “medical
neighborhood” would need to guarantee
this!
Dr. Shoemaker: Thank you, Dr. Meng.
In my 25 years in primary care pediatrics,I used to shudder with the child with theunilateral inflamed eye. Once burnedby missed herpes or intentional trauma,always anxious. I would definitely havewelcomed this kind of help. We’ll see whatthe future holds!
If you have an event to submit for this column, please do so at [email protected] Please includethe name of the event, the date, location and where to get additional information.

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 18/24
18
O R G A N I Z A T I O N AORGANIZATIONAL MEMBERS
Accountable HealthCare IPAGeorge M. Jayatilaka, MD, President& CEODruvi Jayatilaka, Vice President
Advanced MedicalManagement, Inc.K athy Hegstrom, President
• Access Medical Group • Future Care IPA • Pre-mierCare IPA • Seoul Medical Group • Southern Caliornia Medical Coalition •
Afnity MedicalGroupRichard Sankary, MD, PresidentScott Ptacnik, COO
AllCare IPA*Randy Winter, MD, PresidentMatt Coury, CEO
All Care MedicalGroupSamuel Rotenberg, MD, Medical DirectorCraig K aner, Administrator
Allied Physicians of California Thomas Lam, MD, CEOK enneth Sim, MD, CFO AltaBates Medical Group *Richard L. Oken, MD, President and Chairman of the BoardEvan Moore, Vice President, East Bay Region AltaMed Health ServicesCorporation*Martin Serota, MD, Chie Medical OfcerCastulo de la Rocha, JD, President /CEO
AppleCare Medical Management*Surendra Jain, MD, Chie Medical OfcerVinod Jivrajka, MD, President /CEO
Arch Health PartnersScott Flinn, MD, Chie Medical OfcerVictoria Lister, CEO
Bak erseld Family Medical CenterJu Hwan Lee, MD, Medical Director
BayValley MedicalGroup, Inc. *Eric K ohleriter, MD, President /Medical DirectorShelley Horwitz, Chie Executive Ofcer
Beaver Medical Group *Charles Payton, MD, VP Medical Administration /CMOJohn Goodman, President /CEO Brown& Toland Physicians *Andrew M. Snyder, MD, Chie Medical OfcerRichard Fish, CEO
California Pacic Physicians MedicalGroup, Inc.Dien V. Pham, MD, Chie Executive OfcerCarol Houchins, Administrator
CareMore MedicalGroupDonald Furman MD. Chie MedicalOfcer
Tom Tancredi, Dir. o Practice Operations
Catholic Health Initiatives*Stephen Spare, MD, President and CMOJames Slaggert, VP Physician Practice Management
Cedars-Sinai Medical Group *Stephen C. Deutsch, MD, Chie Medical Director
Thomas D. Gordon, CEO
Children’s Physicians MedicalGroup Tanya Dansky, MD, CEO and Medical DirectorLeonard K ornreich, MD, Board President
Chinese Community HealthCareAssociationEdward A. Chow, MD, Executive DirectorPolly Chen, Director o Operations
Choice MedicalGroup IPAManmohan Nayyar, MD, PresidentBlair Bryson, IPA Administrator
Cigna MedicalGroupJames Burrell, MD, Chie Medical OfcerEdward K im, President and General Manager
CMSCAP Management SystemsMegan North, CEO
• AK M Medical Group • Amvi Medical Group •Exceptional Care Medical Group • Family Choice Medical Group • Family Health Alliance • Huntington Park Mission Medical Group • Medicina Familia Medical Group • New Horizon MedicalGroup • Noble Community Medical Associates • OmniCare MedicalGroup • Premier Physician Network • United Care Medical Group •
Community HealthCenter Network Melissa Marshall, MD, Chie Medical Ofcer Ralph Silber, CEO DCHS Medical FoundationDean M. Didech, MD Chie Medical OfcerErnest Wallerstein, CEO
DesertOasis Healthcare*Marc Hofng, MD, MedicalDirectorDan Frank, Chie Operating Ofcer
Dignity HealthK arl Ulrich, MD, Chie Physician Executive
Bruce Swartz, SVP, Physician Integration
Empire Physicians MedicalGroup*Steven Dorman, MD, PresidentYvonne Sonnenberg, Executive Director
Facey Medical Foundation *Erik Davydov, MD, Medical DirectorBill Gil, President /CEO
GoldenEmpire ManagedCare, Inc. *c. Vincent Phillips, MD PresidentRobert Severs, CEO
Good Samaritan MedicalPracticeAssociationNupar K umar, MD, MedicalDirector Cynthia Guzman, CEO
GreaterNewport Physicians MedicalGroup, Inc. *Alan Puzarne, COODiane Laird, CEO
HealthCare Partners*Robert Margolis, MD, Managing Partner, CEOMatthew Mazdyasni, Executive Vice President
Heritage ProviderNetwork *Richard Merkin, MD, PresidentRichard Lipeles, Chie Operations Ofcer
• Afliated Doctors o Orange County • Bakerseld Family Medical Group • Caliornia Coastal Physician Network • Caliornia Desert IPA • Desert Oasis Healthcare • Greater Covina Medical Group • Heritage Physician Network • Heritage Victor Valley Medical
Group • High Desert Medical Group • Regal MedicalGroup • Sierra Medical Group •
High Desert MedicalGroupCharles Lim, MD, FACP, Medical DirectorAnthony Dulgero , MD, Assistant Medical Director
HillPhysicians MedicalGroup, Inc. * Tom Long, MD, Chie Medical OfcerDarryl Cardoza, CEO
Independence MedicalGroupArmi Lynn Walker, MD, Medical DirectorGary M. Bohamed, Executive Director
Inland HealthCare Group, Inc.Carey Paul, MD, PresidentLisa Perko, Controller
John Muir Physician Network Ravi Hundal, MD, Medical DirectorLee Huskins, Interim CEO /Sr.VP / COO Lak eside Community Healthcare
K erry Weiner, MD, Chie Medical OfcerJonathan Gluck, Counsel
Lak eside Medical Group, Inc.
Lak ewood IPAStevenVillalobos, MD, Medical DirectorCynthia Guzman, CPA, Chie Executive Ofcer
• Alamitos IPA • St. Mary IPA • Brookshire IPA •
Loma LindaUniversity HealthCareJ. Todd Martell, MD, Medical DirectorJane Arden, Director, Quality Management
MaxiMed IPAAlejandro Gonzalez, DO, Medical DirectorJacob Tchamanian, CEO
McKinley MedicalGroup, Inc.Stanley Schwartz, MD, PresidentJohn Mukherjee, CEO
MED3000Gary Pro ett, MD, Medical DirectorLynn Stratton Haas, CEO
• SeaView IPA • Valley Care IPA •
Med Point ManagementRick Powell, MD, Medical DirectorK imberly Carey, Administrator
• Apollo Healthcare • Bella Vista MedicalGroup IPA •Centinela Valley IPA • El Proyecto Del Barrio, Inc. •Global Care MedicalGroup • HealthCare LA IPA •
Mission Community IPA • Riverside Family Health Medical Group • Watts Health Care Corporation •
MemorialHealthCare IPARonald Zent, MD, Medical DirectorK urt Tamaru, MD, CMO /Interim CEO
MemorialCare MedicalGroup *Mark Schaer, MD, Chie Medical OfcerPatrick E. K apsner, CEO Meritage Medical Network J. David Andrew, MD, Medical DirectorJoel Criste, CEO
Midcoast Care Inc., AMedicalGroupJohn Okerblom, MD, PresidentBarbara Cheever, Executive Director

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 19/24
19
Molina Medical Centers Steve O’Dell, Regional Vice President Gloria Calderon, Vice President
Monarch HealthCare *Bart Asner, MD, CEOJay Cohen, MD, President /Executive Chairman
Muir MedicalGroup, IPASteve K aplan, MD, PresidentUte Burness, RN, CEO NAMMCalifornia*Leigh Hutchins, President, COOElizabeth Haughton, Vice President, Legal A airs
• Coachella Valley Physicians o PrimeCare, Inc., •Mercy Physicians Medical Group • Primary Care Associated Medical Group, Inc. • PrimeCare MedicalGroup o Chino • PrimeCare o Citrus Valley •PrimeCare o Corona • PrimeCare o Hemet Valley Inc• PrimeCare o Inland Valley • PrimeCare o Moreno Valley • PrimeCare o Redlands • P rimeCare o Riverside • PrimeCare o San Bernardino • PrimeCare o Sun City • PrimeCare o Temecula • Redlands Family Practice Medical Group, Inc. •
Omnicare MedicalGroupAshok Raheja, MD, Medical Director
Toni Chavis, MD, President
Pacic IPA Thomas Chiu, MD, PresidentPeder Lindblom, Executive Director
The Permanente MedicalGroup, Inc.Oakland(North)*Sharon Levine, MD, Associate Executive DirectorGerard Bajada, VP /Director, Financial Services
Physicians DataTrustAnthony Ausband, President Lisa Serratore, Chie Operations Ofcer
•Greater Tri-Cities IPA •Noble AMA IPA • St.Vincent IPA •
Physicians MedicalGroup of SantaCruz*Marvin Labrie, CEONancy Greenstreet, MD, Medical Director
PIH Health PhysiciansK athleen Barry, MD, Sr. MedicalDirector, ClinicalOperations
Tom Mahowald, President
Pioneer MedicalGroup, Inc. *Jerry Floro, President John K irk, CEO
Preferred IPAof CaliforniaMark Amico, MD, Medical Director
Zahra Movaghar, Administrator Prospect Medical GroupPrasad Jeereddi, MD, ChairmanMark Marten, COO
• AMVI /Prospect Health Network • Gateway MedicalGroup • Genesis Healthcare • Nuestra Familia MedicalGroup • Prospect Corona • Prospect HealthSource •Prospect Huntington Beach Prospect Northwest Orange County • Prospect Orange County • Prospect Proessional Care • Prospect Van Nuys •
Providence MedicalManagement ServicesMarvin K anter, MD, Chie Physician Integration OfcerJoan Rose Baranov, Chie Operating Ofcer
• K orean American Medical Group • Providence Care Network •
River City MedicalGroup, Inc.Jose Abad, MD, President /Medical DirectorLoren Douglas, CEO
Riverside Medical ClinicSteven Larson, MD, ChairmanJudy Carpenter, President /COO Riverside Physician Network Paul Snowden, COOHoward Saner, CEO
St. Joseph Heritage HealthcareK haliq Siddiq, MD, Chie Medical OfcerC.R. Burke, Chie Executive Ofcer
SanBernardino MedicalGroup Thomas Hellwig, MD, PresidentJames Malin, CEO
San Diego Physicians MedicalGroup
James Cordell, MD, PresidentJoyce Cook, CEO
San LuisObispo Select IPABarbara Cheever, Executive Director
Sansum Clinic *K urt Ransoho , MD, Medical Director /CEOVince Jensen, COO SantaClaraCounty IPA (SCCIPA)*J. K ersten K rat, MD, President o the BoardRandall Frakes, Chie Executive Ofcer
SantéHealth System, Inc Daniel Bluestone, MD, Medical DirectorScott B. Wells, CEO
ScrippsCoastalMedical Center*Louis Hogree, MD, APC, Chie MedicalOfcer
Tracy Chu, Assistant Vice President o Operations
SharpCommunity MedicalGroup *John Jenrette, MD, Chie Executive OfcerChristopher McGlone, Chie Operating Ofcer
• Graybill Medical Group SharpRees-Stealy MedicalGroup *Donald C. Balour, III, MD, Chie Medical OfcerStacey Hrountas, Senior VP & Chie Executive Ofcer
Southern California Permanente MedicalGroup*Mark Bird, MD, Sr. Physician ExecutiveJames Malone, Medical Group Administrator
Sutter Health Foundations & Afliated Groups *Je rey Burnich, MD, SVP & Executive Ofcer, Sutter Medical Network Brian Roach, President, Mills Peninsula Division o PAMF
• Palo Alto Medical Foundation • Sutter MedicalFoundation • Sutter North Medical Foundation •Sutter West Medical Group • Sutter North MedicalGroup • Sutter Medical Group • Sutter Region MedicalFoundation • Sutter Independent Physicians • Solano Regional Medical Group • Sutter Gould Foundation •Camino Medical Group • Sutter Gould Medical Group • Santa Cruz Medical Clinic • Sutter MedicalFoundation—North Bay • Sutter Medical Group o the Redwoods • Physician Foundation—Caliornia PacicMedical Center •
SynerMed, Inc. *George Ma, MDJames Mason, President & CEO
• Angeles IPA • Crown City Medical Group • EHS Inland Valleys IPA • EHS Medical Group – CentralValley • EHS Medical Group – Los Angeles • EHS
Medical Group – Sacramento • Employee Health Systems • MultiCultural IPA • Southern Caliornia Children’s Network •
Talbert MedicalGroup *K eith Wilson, MD, President& CEO Torrance Hospital IPANorman Panitch, MD, PresidentStephen J. Linesch, CEO U.C.L.A. MedicalGroup *Sam Skootksy, MD, MedicalDirectorDavid Hartenbower, MD, COO
USC Care Medical Group, Inc.Donald Larsen, MD, Chie Medical OfcerK eith Gran, CEO
CORPORATE PARTNERS
Adventist Health Physicians Network Anthem Blue Cross o CaliorniaBoehringer Ingelheim Pharmaceuticals, Inc.Merck & Co.Novartis PharmaceuticalsNovo Nordisk SCAN Health Plan
ASSOCIATE PARTNERS
abbvie
ActavisAmgen Inc.AstraZeneca PharmaceuticalsCardiovascular Consultants, LTDCrescent Healthcare, Inc.Daiichi SankyoEisai, Inc.GenPath DiagnosticsGenomic HealthGlaxoSmithKlineJohnson & Johnson Family o CompaniesK indred Healthcare, Inc.NORCAL Mutual Insurance CompanyPzer, Inc.Ralphs Grocery CompanySanoSunovion Pharmaceuticals Inc.Vitas Healthcare Corporation o Caliornia
AFFILIATE PARTNERS
AlturaAscender Sotware, LLCClarity Health ServicesChildrens Hospital Los Angeles Medical GroupDPS HealthMedVentive Inc.MedVision, Inc. MZI HealthCare, LLCRedlands Community HospitalSaint Agnes Medical GroupSullivan /Luallin, Inc.Unlimited Innovations, Inc. Ventegra, LLC
M E M B E R S & P A R T N E R S

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 20/24
20
. oining the CAPCI team is truly an honor. For the last 36 years, I have been
drawn to eorts about change, ocusing
on campaigns to both improve the pub-
lic’s health and the quality o healthcare
patients receive. CAPCI provided the op-
portunity to jump in and take on one o
the greatest challenges or healthcare and
health in general: revitalizing primary care
in Caliornia.
It’s Personal & Professional
My husband is a pediatrician who or
most o his proessional lie worked in solo practice in the San Joaquin Valley. He was
able to “be there” when our twin daugh-
ters were born, but didn’t get to be there
with them much over the next ew years
o their lives as he built his practice. Our
amily enjoyed its irst vacation when our
daughters were almost seven.
He loved what he did and his patients
loved him. However, he wasn’t home or
most meals with the amily and didn’t see
our daughters much on weekends either.
While he loved the time with his patients,
he wasn’t getting to be Dad. He eventu-ally made a change and joined a group
practice, not to change his income, but to
improve the quality o lie or himsel and
his amily.
I’ve lived the challenges oten described
or primary care. I want to see primary care
attract a new group o clinicians who value
the critical role it plays in our healthcare
and health systems. I want to see primary
care become an exciting, livable specialty
that is valued by those who train our clini-
cians, by those who make the policy deci-
sions, and by those who choose clinicalmedicine as their lie course. That’s where
CAPCI comes in.
CAPCI as an Organization
Our nation is poised to undergo the
most dramatic change in its healthcare sys-
tem since the start o Medicare almost ity
years ago. A key element o this change
process will be recasting the role and unc-
tion o primary care. Caliornia provides
the model or this change through its in-
tegrated healthcare in community health
By Elissa Maas, MPH
Executive Director CAPCI
A Vision for CAPCIcenters, chartered private organizations,
and military systems.
As CAPCI’s Executive Director, I want to
see us drive the agenda that primary care
is the oundation or healthcare delivery.
With our credibility and credentials, we can
play a lead role in helping policy makers,
healthcare providers, patients, and payors
develop and embrace new approaches to
organize the primary care team. To make
this happen, CAPCI will bring together
organizations rom a broad spectrum o
interests to share their experiences and
expertise to strengthen and revitalize pri-
mary care through our 4P’s: Pipeline, Prac-
tice Redesign, Payment, and Policy.
CAPCI’s Impact
CAPCI is embarking upon both a short
and a long-term transormation o primary
care.
i We envision that CAPCI will help to
inorm policies that anchor and
sustainably support primary care
practice.
i Members o the healthcare team,
working at the top o their game, willbecome the norm or primary care,
with the patient as the heart and soul
o that team.
i Primary care physicians, with
sophisticated supports, can expand
their roles to manage patients with
more complex health needs.
i Organizations which in the past may
have worked in separate silos…or
which competed without cooperat-
ing…will nd success by working in
partnership to strengthen primary
care in their communities.
i
Community initiative can accelerate collaboration among local healthcare
systems and improve overall health.
A change o this magnitude will require
the entire healthcare community to sup-
port one another’s eorts so that individu-
als and communities receive the care they
need. We have plenty o work in store!
Partnership WorksWe intend to engage our many partners to build an eective,
diverse, primary care workorce providing quality, culturally re-sponsive, aordable care across the continuum o care…on a community-wide scale. CAPCI will provide the training, tools, and support or healthcare organizations to implement advanced pri-mary care principles and practices.
Elissa Maas MPH, Executive Director, CAPCI

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 21/24
21
A breakout session will look at the Advanced Primary Care and Medical Home concepts through three lenses:
$'9$1&('35,0$5<&$5(
ZLOODJDLQWDNHDFHQWHUVWDJHLQ&$3*·V$QQXDO0HHWLQJ
-XQHLQ/RV$QJHOHV
KEVINGRUMBACH MD, eatured in this issue,
will expand upon the “Pipeline”issues involving the training envi-ronment. Beyond improving the
raming and appeal o primary care, what must be changed in tradi-
tional training to prepare new PCPs or the team roles and system thinking o the next decade.
JOHN JENRETTE MD, principal in one o
Caliornia’s six pioneer ACO’s, willdescribe Advanced Primary Care as a community wide interest, eaturing the cross-linking in-
novations o San Diego County’s community clinics, public health, private sector organizations,
military, and VA.
DAVID NACE MD,
President o the Patient Centered Primary Care Collaborative and senior leader in McK esson, willdescribe industry’s
multi-state stake in the success o modernized
primary care.

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 22/24
22
Advertisers Index:
BROWN & TOLAND....Outside Back Cover
HILL PHYSICIANS..........Inside Front Cover
VI TAS......................................................Page 3
Blair Bryson, AdministratorChoice Medical Group
Blair Bryson, Administrator
Choice Medical Group
& lair resides in Riverside, CA, is
married, and the ather o our children. He
is a graduate o Brigham Young University,
where he earned a degree in Accounting.
Prior to his career in healthcare, Blair
worked in public accounting, banking and
as an analyst evaluating and integrating
business acquisitions. He stumbled into
healthcare by accident when he was hired
as a consultant by an Inland Empire physi-
cian who had ormed an IPA. He was given the task o creating a business plan or the
new IPA. That engagement has led to 17
years o experiences in healthcare man-
agement in the Caliornia managed care
industry. Lacking a clinical background, Blair has used his experience in other in-
dustries to ocus on healthcare systems
and processes. He noted that many other
industries had already deployed more ma-
ture and consistent processes than man-
aged care had in the nineties.
In 1999, Blair teamed with the ounders
o Unlimited Innovations to create one
o the irst online portals widely used or
healthcare inormation technology. He
created the use case architecture that pio-
neered online access or eligibility, reerrals
and claims management, which enhanced the timely delivery o care. This system is
still in use or more than 300,000 patients.
Blair’s company, Raven Resources, provides
administrative, compliance and technol-
ogy support to medical groups that serve
more than 100,000 patients contracted
with every major health plan in Caliornia.
Blair is currently serving as the Adminis-
trator or Choice Medical Group. Choice
has been recognized as having achieved
“Elite” status with the Caliornia Associa-
tion o Physician Groups in our o the last
ive years, including 2012. Blair continues to enjoy the challenges o making “health-
care processes work ”. As Administrator
or Choice, he sees the challenges the PCP
aces as an independent provider, and
believes that now more than ever, IPAs
can serve the PCP and the patient by lev-
eraging best practices and technologies
to achieve improvements in quality and
proitability. Blair is a committed advocate
o participation in CAPG, CQC and other
industry groups through which solutions
are shared.
C A P G M E M B E R S P O T L I G H T
“...now more than ever,IPAs can serve the PCP and the patient by lever-aging best practices and
technologies to achieveimprovements in quality and profitability. “

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 23/24
23
VOL.4,NO.3
Dr. Keith WilsonStayingThe Course -navigatinghealthcare today
Transportation Creates HealthierCommunities
Preventing Hospital Admissionsand Re-admissions
SPRING 2010|SPECIAL CONFER
Reserve Your Ad SpaceNow InCAPG Health’sHigh Profile,
AnnualConferenceEdition
$GGLWLRQDOFRSLHVRI&$3*
+HDOWKDUHGLVWULEXWHG
WRDOOFRQIHUHQFH
DWWHQGHHV
*HW\RXUEXVLQHVVLQIURQW
RINH\KHDOWKFDUH
GHFLVLRQPDNHUV
6KRZFDVH\RXUQHZ
SURGXFWRUVHUYLFH
&XVWRPDGYHUWLVLQJ
SURJUDPVDYDLODEOH
For more informationemail [email protected] call 916.761.1853
IMPORTANT: Ad deadline is Friday, May 1, 2013!
VOL.4,NO. 3 SPRING2010 SPECIAL CONFER
VOL. 5, NO. 3
The InnovationCenter: The JourneTo Lower Costs AndBetter CareRichard Gilfllan, M.D.
Healthcare Mergers AndAcquisitions
Employers View OnHealthcare Reorm
Creating a Common VisionO Accountable Care
SPECIAL CONFERENCE EDITIONVOL. 5, NO. 3 SPECIAL CONFERENCE EDITION
VOL. 6, NO. 4 MA
The Ever-ChanginHealthcareLandscapeDonald Berwick, MD
Demystiying ComplexCare Management
Pioneer ACO Creation &Implementation
SPECIAL CONFERENCE EDITION
Conference 2013 Theme: REFORM, INNOVATION
AND ACCOUNTABILITY THE FUTURE IS NOW

7/28/2019 CAPGMarApr2013 OD Article(3)
http://slidepdf.com/reader/full/capgmarapr2013-od-article3 24/24
/HDGLQJWKHZD\IRUZDUG
3UDFWLFLQJPHGLFLQHLQWRGD\¶VHQYLURQPHQWLVGLI¿FXOW%URZQ7RODQG3K\VLFLDQVLVOHDGLQJWKH
ZD\IRUZDUGLQKRZSK\VLFLDQVSUDFWLFHDQGSURYLGHFDUH:HFRQWLQXHWR¿QGLQQRYDWLYHZD\VWR
LPSURYHSUDFWLFHZRUNÀRZVFRQQHFWLYLW\DQGFROODERUDWLRQDFURVVKHDOWKFDUHSDUWQHUV
:HDUHRQHRIKHDOWKFDUHRUJDQL]DWLRQVQDWLRQZLGHWREHVHOHFWHGDVD0HGLFDUH3LRQHHUDFFRXQW
DEOHFDUHRUJDQL]DWLRQ:HDUHDGYDQFLQJSULPDU\FDUHWKURXJKRXUSDWLHQWFHQWHUHGPHGLFDOKRPH
0\+HDOWK0HGLFDO*URXSZKLFKZDVUHFHQWO\QDPHGD/HYHO3&0+
%URZQ7RODQGLVFRPPLWWHGWRSUHVHUYLQJWKHLQGHSHQGHQWSK\VLFLDQSUDFWLFHE\SURYLGLQJVWURQJ
OHDGHUVKLSH[FHOOHQWVXSSRUWDQGLQQRYDWLYHFDUHSURJUDPVWRDGYDQFHSDWLHQWFDUH
)RUPRUHLQIRUPDWLRQRQ%URZQ7RODQG3K\VLFLDQVSOHDVHYLVLWRXUZHEVLWHDW
ZZZEURZQDQGWRODQGFRP