Embed Size (px)
Citation preview
Inpharma 1345 - 6 Jul 2002
Capecitabine proves its worth in colorectal, breast cancer– Salmon K –
The oral fluoropyrimidine agent capecitabine [‘Xeloda’; Roche] has shown efficacy in the treatment of solidtumours, such as colorectal cancer and breast cancer. Capecitabine use is also associated with fewer adverseeffects, and greater tolerability and efficacy, than other standard cancer therapies. However, newerantineoplastic therapies, such as capecitabine, tend to be more costly than older therapies, and studies thatcompare overall cost effectiveness of such drugs with older therapies are therefore of great interest to healthcarepayers. At the 7th Annual Meeting of the International Society for Pharmacoeconomics and Outcomes Research[Arlington, Virginia, US; May 2002], two studies providing an economic evaluation of capecitabine werepresented at sessions dedicated to cancer research.
A recent US Government Accounting Office report researchers. They say these savings conferred bystated that reimbursement patterns associated with IV capecitabine, relative to fluorouracil-based, therapychemotherapy regimens account for excessive were mainly realised through a reduction in costshealthcare costs in the Medicare system. Administration related to antiemetics ($US83 vs $US999),of an oral agent, such as capecitabine, would avoid the chemotherapy ($US2416 vs $US8499) and anti-complications and related costs associated with IV infectives ($US18 vs $US69). Patients who receivedtherapy in cancer patients. capecitabine also spent fewer cancer-related days in
hospital than patients who received the fluorouracil-Warranted in colorectal cancer? based regimen (0.76 vs 0.87 days per patient). TheAn analysis of costs and outcomes associated with researchers conclude that, due to its superior costoral capecitabine therapy versus comparison therapies effectiveness, capecitabine ‘offers the best cost solutionwas undertaken by Dr RW Baran from Roche with current standards of care’ and ‘should be integratedLaboratories, Inc., US, and associates, and presented at into standards of care in colorectal cancer’.the second of two large poster sessions.1 TheirCombined treatment for metastatic breastretrospective study used medical and retail pharmacy
claims data for the period between August 1997 and cancerJune 2000 for 271 patients with metastatic colorectal In patients with breast cancer, both capecitabine andcancer, to assess costs and outcomes associated with docetaxel [‘Taxotere’; Rhone-Poulenc Rorer] have beentreatment. Patients formed two study cohorts based on shown to have considerable single-agent activity.therapy received: Individually, the two drugs have distinct mechanisms of• oral capecitabine (n = 78) action which limit the overlap of key toxicities.• IV fluorouracil plus folinic acid with or without Combination treatment with capecitabine plus
irinotecan (n = 193). docetaxel was compared with single-agent docetaxel forThree therapy subgroups comprised the fluorouracil 511 patients with breast cancer in a study conducted by
comparison cohort: Dr John Hornberger from Acumen, LLC and Stanford• IV fluorouracil plus folinic acid [leucovorin; n = 78] University School of Medicine, US, and colleagues, and• IV fluorouracil plus folinic acid plus irinotecan (n = presented at a podium session.2,** The cost
37) effectiveness associated with the therapies was assessed• IV fluorouracil plus folinic acid followed by from the perspective of a US health delivery
irinotecan (n = 78) organisation. They constructed a Markov model for acohort of female patients with unresectable metastaticLower total direct costsbreast cancer refractory to standard therapy (paclitaxelThe results of the analysis revealed that there was no or an anthracycline) and a life-expectancy of at least 3significant difference in time to treatment months. Patients received treatment with oraldiscontinuation between capecitabine or fluorouracil capecitabine 1250 mg/m2 twice daily on days 1–14 plusrecipients, but the mean estimated per-patient survival IV docetaxel 75 mg/m2 on day one (n = 255), or IVwas greater in the capecitabine, relative to the docetaxel 100 mg/m2 on day one, for 3-weekly cycles forfluorouracil, cohort (607 vs 564 days). The average per- at least 6 weeks. The researchers note that the dosagepatient costs for professional cancer care were was modified ‘according to incidence and severity ofconsiderably lower for the capecitabine group than for toxicities’.the three fluorouracil-based therapy subgroups and the
fluorouracil-based therapy combined group ($US2156 Survival maximisedvs $US7508, $US14 406, $US12 542 and $US10 865, The model showed that capecitabine plus docetaxelrespectively). Capecitabine was also associated with would maximise quality-adjusted survival amonglower total direct costs relating to cancer care than the patients with breast cancer, and delay time to diseasecomparative therapies [see table].* This resulted in a progression. However, mean total direct medical costsfavourable cost-effectiveness ratio for capecitabine were higher in the capecitabine plus docetaxel arm thancompared with the fluorouracil cohort as a whole, as in the docetaxel monotherapy arm ($US20 701 vswell as for capecitabine compared with each $US19 839 per patient).† This extra cost was due mainlyfluorouracil-based treatment subgroup. to the extra acquisition cost of capecitabine when used
in combination with docetaxel; docetaxel monotherapy‘Best cost solution’cost $US13 292 per patient, while docetaxel plusTotal per-patient costs associated with chemotherapy capecitabine cost $US10 167 plus $US4635 per patient,and supportive care were ‘substantially lower’ with respectively. However, the researchers note that most ofcapecitabine, compared with combined fluorouracil- the acquisition cost of capecitabine (> 90%) is offset bybased, therapy ($US3264 vs $US10 112), note the
1
Inpharma 6 Jul 2002 No. 13451173-8324/10/1345-0001/$14.95 Adis © 2010 Springer International Publishing AG. All rights reserved
Single Article
Capecitabine – continuedthe lower cost associated with docetaxel when used as
* Costs included those for all cancer-related services andcombination therapy. Mean costs associated with hospitalisations, chemotherapy, reimbursement, adverse events andadverse event-related hospitalisations were lower for supportive care.the capecitabine plus docetaxel monotherapy arm, ** One of the researchers was affiliated with Roche Pharmaceuticals,compared with the docetaxel arm ($US5167 vs US, which provided funding for the study.$US5861). † Costs included those for infusions, drug acquisition, physician
consultations, and hospitalisations and other treatments associated‘Highly cost-effective’ with adverse events. Costs were discounted at a rate of 3% per annum.Compared with docetaxel alone, capecitabine plus
1. Baran RW, et al. Clinical and economic outcomes associated with metastaticdocetaxel cost an additional $US5520 per quality- colorectal cancer in managed care populations: capecitabine (Xeloda Rm) versuscomparison therapies. Value in Health 5: 199-200 (plus poster), May-Jun 2002.adjusted life-year gained, proving the capecitabine plus
2. Hornberger J, et al. Economic evaluation of capecitabine-docetaxel combinationdocetaxel combination to be ‘highly cost-effective in thetreatment of metastatic breast cancer: a micro-simulation study. Value in Health
treatment of women with metastatic breast cancer’, say 5: 129 (plus oral presentation), May-Jun 2002.800888209the researchers.
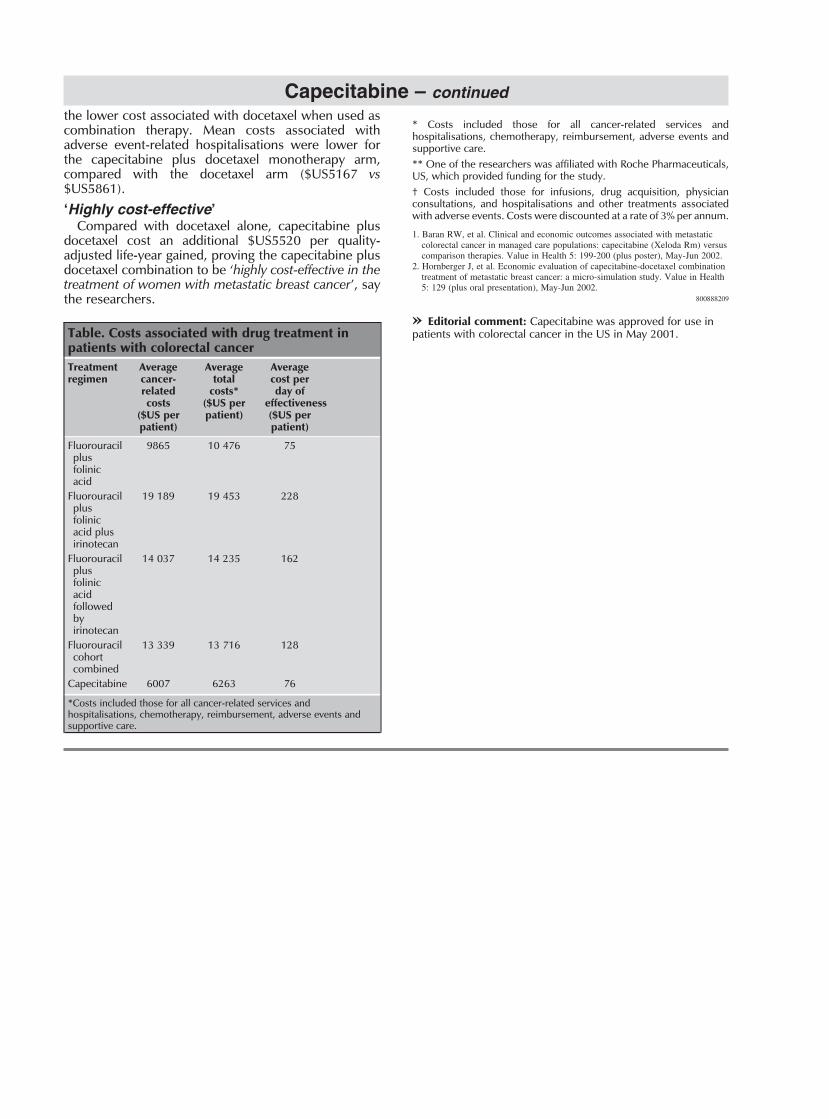
» Editorial comment: Capecitabine was approved for use inTable. Costs associated with drug treatment in patients with colorectal cancer in the US in May 2001.patients with colorectal cancerTreatment Average Average Averageregimen cancer- total cost per
related costs* day ofcosts ($US per effectiveness
($US per patient) ($US perpatient) patient)
Fluorouracil 9865 10 476 75plusfolinicacid
Fluorouracil 19 189 19 453 228plusfolinicacid plusirinotecan
Fluorouracil 14 037 14 235 162plusfolinicacidfollowedbyirinotecan
Fluorouracil 13 339 13 716 128cohortcombined
Capecitabine 6007 6263 76
*Costs included those for all cancer-related services andhospitalisations, chemotherapy, reimbursement, adverse events andsupportive care.
2
1173-8324/10/1345-0002/$14.95 Adis © 2010 Springer International Publishing AG. All rights reservedInpharma 6 Jul 2002 No. 1345