Embed Size (px)
Citation preview

Cancer Treatment:Targeted Agents/ Immunotherapy
Margaret Barton-Burke, PhD, RN, FAAN
Director, Nursing Research
Memorial Sloan Kettering Cancer Center
1
DIsclosures
• MSK Core Grant
• Pfizer Grant
• Pfizer Speakers Bureau
2
Actions of the Immune System
• Defense: Against foreign organisms
• Homeostasis: Destruction of worn or damaged cells
• Surveillance: Identification of foreign or non-self substances
3(Polovich et al., 2014)
Immune System and Cancer
• Cancers survive and metastasize because the immune system does not recognize the cancer cells and destroys them.
• Immunotherapy – encourages the immune system to identify the cancer cells and destroy them.
file:///Users/dr.margaretbarton-burke/Desktop/Treatment.Hormone.Target.pptx
(Tedder & Eggert, 2017) 4
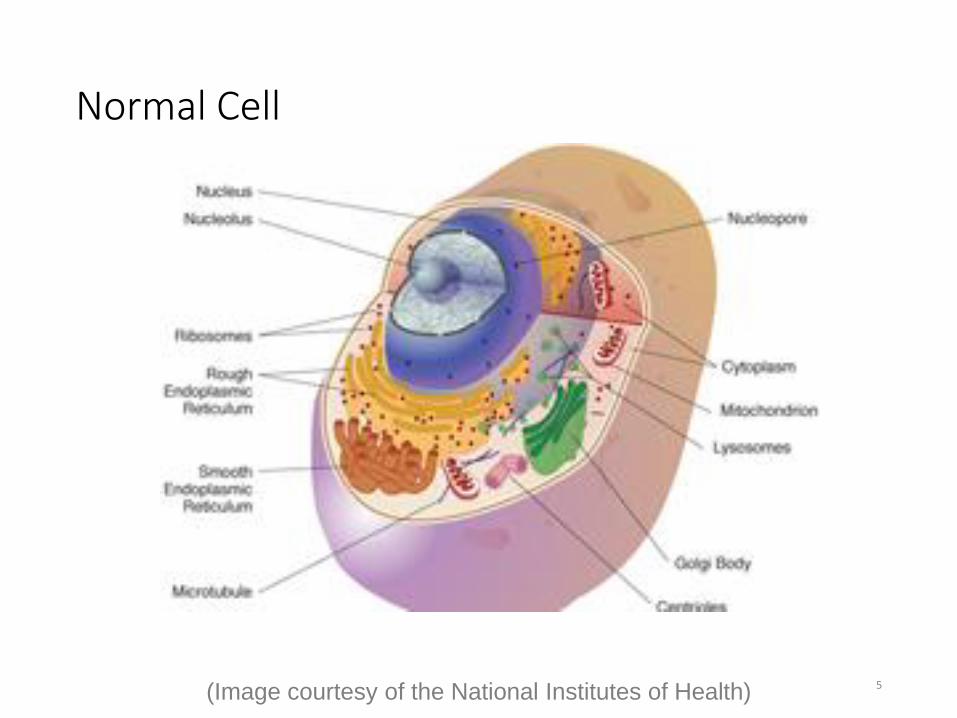
Normal Cell
(Image courtesy of the National Institutes of Health) 5
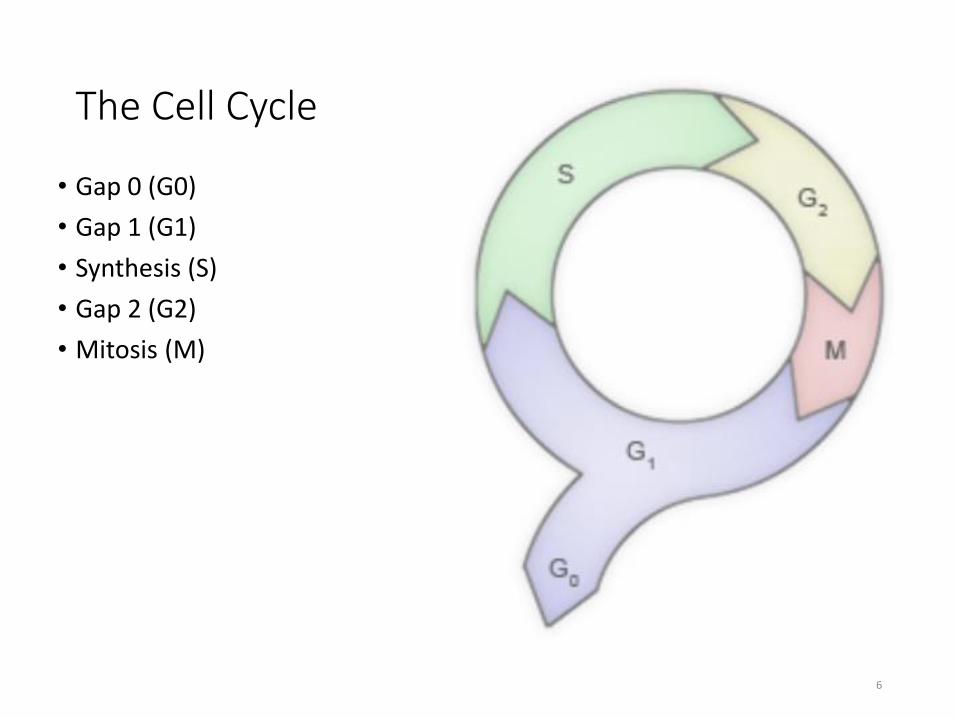
The Cell Cycle
• Gap 0 (G0)
• Gap 1 (G1)
• Synthesis (S)
• Gap 2 (G2)
• Mitosis (M)
6
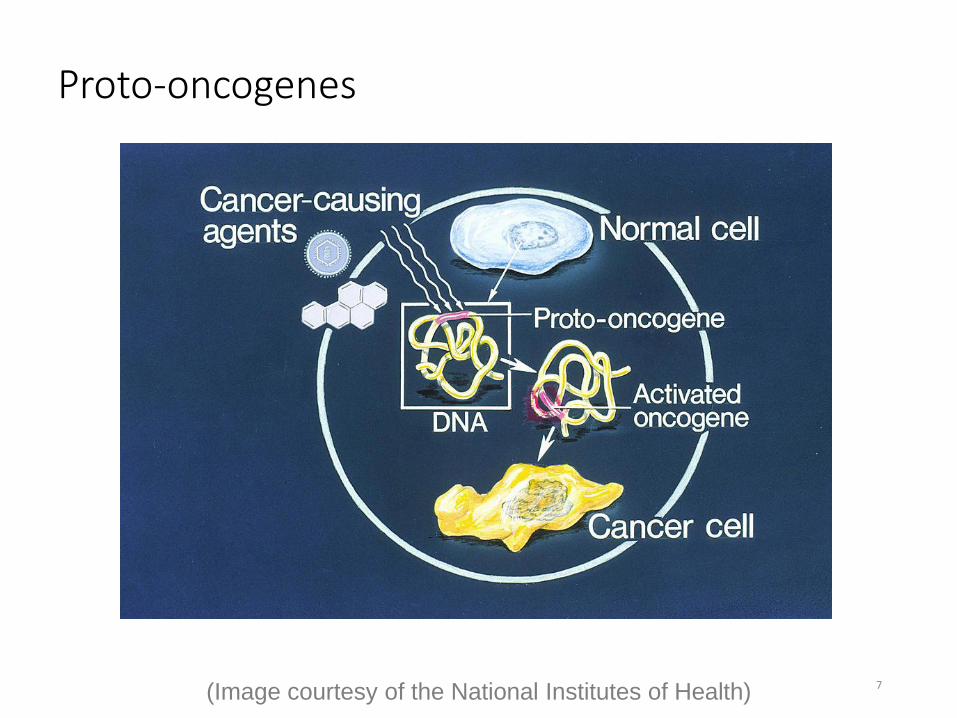
Proto-oncogenes
(Image courtesy of the National Institutes of Health) 7
8
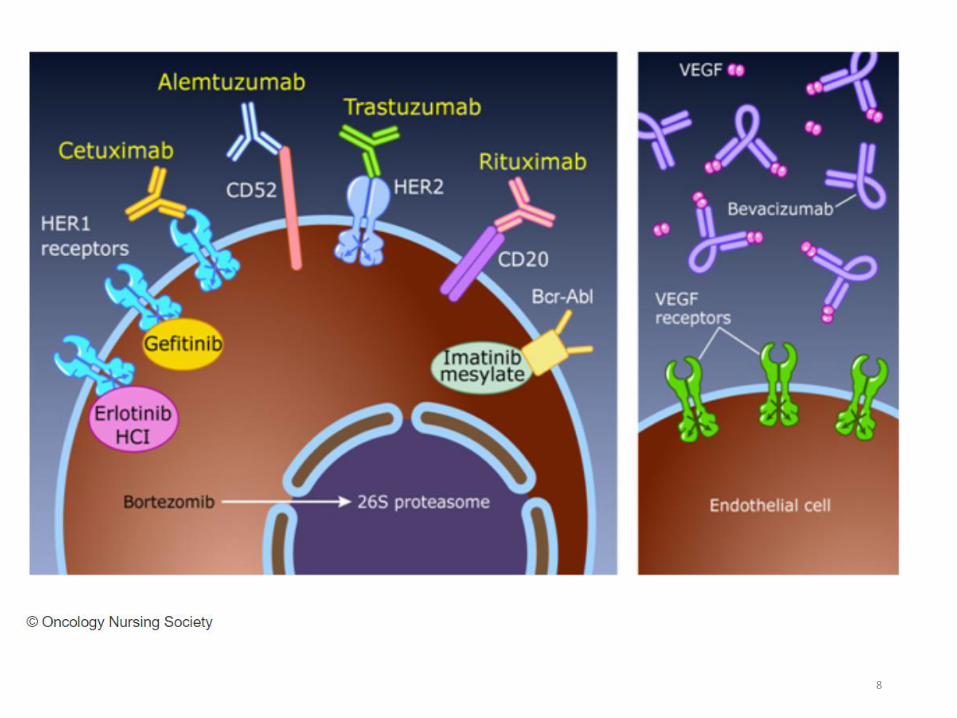
VEGF
• Cancers need blood supply
• Cancers excrete Vascular Endothelial Growth Factor (VEGF)
• VEGF is a signal protein to stimulate growth of blood vessels – process called angiogenesis
• Drugs can block VEGF
9
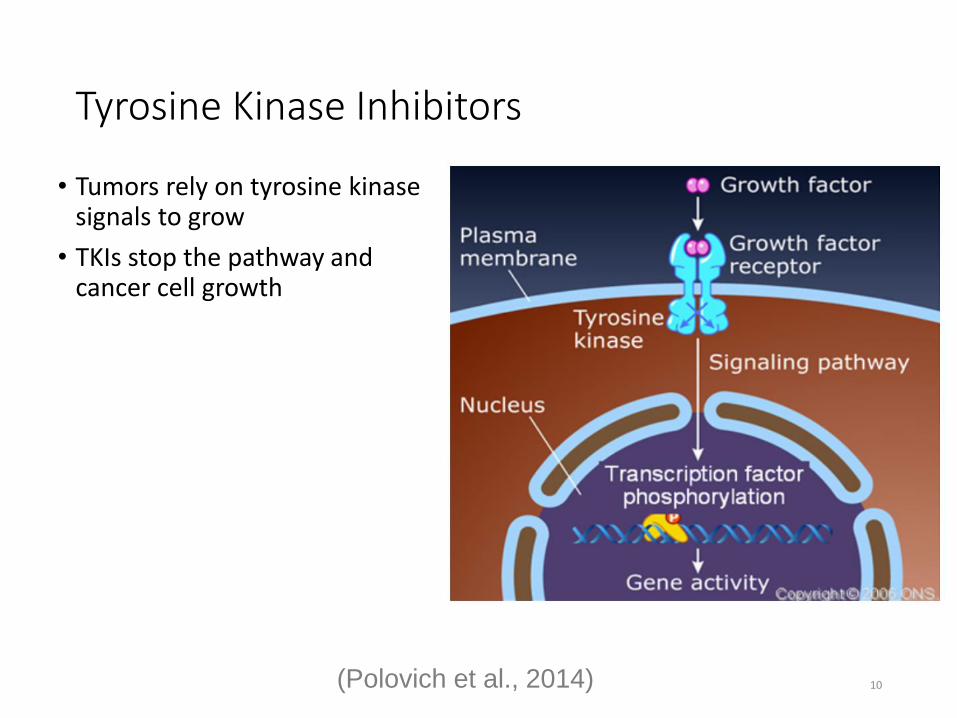
Tyrosine Kinase Inhibitors
• Tumors rely on tyrosine kinase signals to grow
• TKIs stop the pathway and cancer cell growth
10(Polovich et al., 2014)
• Cytokines are a broad class of protein cell regulators produced by the immune system
• Most cytokines possess multiple effects
• Cytokines include
oInterferonsoInterleukinsoHematopoietic growth factors
11
Cytokines
(Polovich et al., 2014)
Hematopoietic Growth Factors
• Action: Stimulate the differentiation, proliferation, maturation, and functioning of hematopoietic cells
• Used to decrease the severity of toxicities/side effects from treatment
• Examples:
oErythropoietin – epoetin alfa, darbepoetinoG-CSF – filgrastim (Neupogen), pegfilgrastim (Neulasta)
12(Polovich et al., 2014)
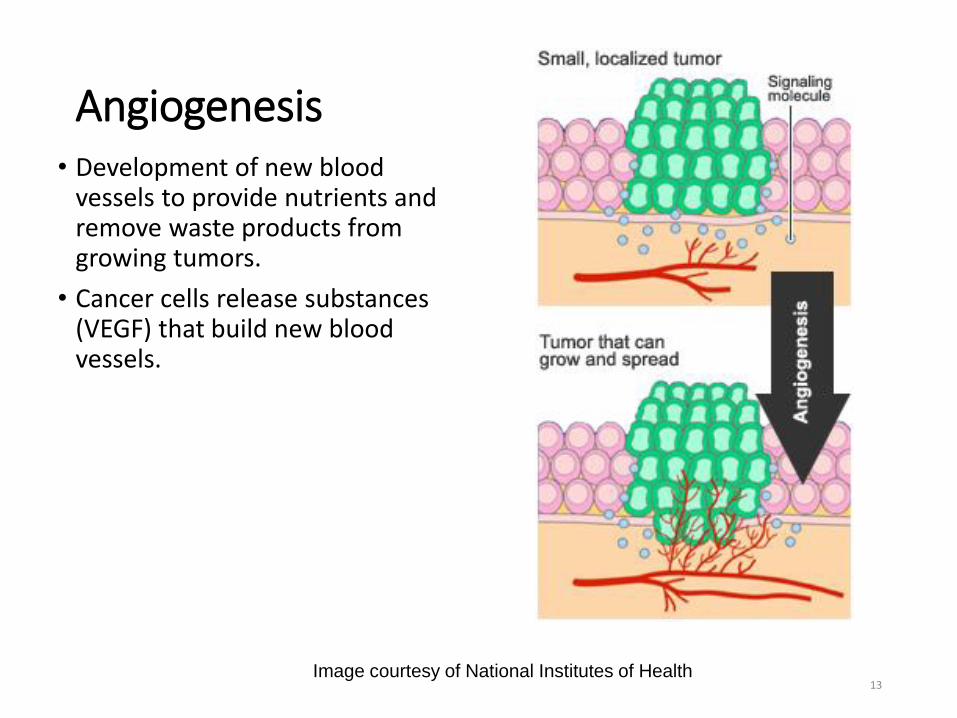
Angiogenesis• Development of new blood
vessels to provide nutrients and remove waste products from growing tumors.
• Cancer cells release substances (VEGF) that build new blood vessels.
Image courtesy of National Institutes of Health13
Major Types of Treatment for Cancer
SURGERY
RADIOTHERAPY
CHEMOTHERAPY, IMMUNOTHERAPY,
HORMONAL THERAPY
PALLIATIVE CARE
14

Targeted Therapies
15
Confusing Language
• Mabs
• Mibs
• Mids
• Nabs
• Nabs
• Car-T cells
16
Targeted Therapy
• Target molecular pathways within the cell
• New targets are being identified
• Many are oral agents
• Improved bone marrow recovery
17(Polovich et al., 2014)
Types of Targeted Therapy
Small molecule inhibitors
• Tyrosine kinase inhibitorsoBCR-ABL kinase inhibitors
oCDK – cyclin-dependent kinase inhibitors
o EGFR - epidermal growth factor receptor inhibitors
oVEGF – vascular endothelial growth factor inhibitors
• mTOR inhibitors
• PARP inhibitors
• Proteasome inhibitors
• Checkpoint inhibortors
18(Polovich et al., 2014)
Tyrosine Kinase Inhibitors
Side effects determined by receptor
• Rash
• Fluid retention
• Nausea and vomiting
• Diarrhea
• Fatigue
19(Polovich et al., 2014)
Imatinib Mesylate
• Inhibits BCR-ABL tyrosine kinase created by the Ph+ genetic abnormality
• Oral route
• Indicated for CML, ALL, MDS and GIST
• Side effects: edema and fluid retention; GI irritation
• Take with food and glass of water
20(Polovich et al., 2014)
Antiangiogenic Agents
•Action: Target the neovasculature of tumors to halt their growth, prevent tumor invasion, and preclude metastatic spread
•Side Effects: bleeding, peripheral neuropathy, deep vein thrombosis (DVT), hypertension
•Examples: oBevacizumab (anti-VEGF)oThalidomide and Lenalidomide – Miscellaneous biologic
response modifiers that have antiangiogenic properties
21(Polovich et al., 2014)
Bevacizumab
•Anti-VEGF antibody•Also called an angiogenesis inhibitor•Binds to and inhibits activity of VEGF therefore
blocking proliferation and formation of new blood vessels. •Used in colorectal, NSCLC, glioblastoma, renal cell •Avoid use for at least 28 days after major surgeryoSurgical incision should be completely healed
•Do not use 28 days before surgery
22(Polovich et al., 2014)

Immunotherapy
23(Image courtesy of National Cancer Institute)
Types of Immunotherapy
• Monoclonal antibodies
• Radioimmunotherapy
• Vaccines
• Cytokines
• Adoptive T-cell transfer
• Checkpoint inhibitors
24(Polovich et al., 2014)
Introduction to Immunotherapy
• Immunotherapy: a treatment that restores or enhances the immune system's natural ability to fight cancer
• Immunotherapy has been described as a way to “fire up the immune system's response to cancer”
25
Monoclonal Antibodies (mAbs)
• Target tumor-specific antigens on cell surfaces of some cancer cells
• Chimeric (70% human/30% foreign), humanized (90% human), fully humanized (100% human)
• mAbs are a passive (meaning they do not result in any immunologic memory) but specific (meaning they target specific cancer cells) class of immunotherapy
• Used in combination with chemotherapy/radiation has shown significantly improved response rates
26(Polovich et al., 2014)
Rituximab
• Chimeric anti-CD20 antibody
• Binds to CD20 antibody on the surface of normal and malignant B lymphocytes
• Indications: lymphomas, leukemias, rheumatoid arthritis
• Infusion-related hypersensitivity, myelosuppression
• Tumor lysis syndrome can occur in high risk patients
27(Polovich et al., 2014)
Trastuzumab
• Humanized, monoclonal anti-HER2 antibody
• Infusion-related hypersensitivity
• Cardiac toxicity
• Used following completion of doxorubicin and cyclophosphamide in breast cancer patients
28(Polovich et al., 2014)
Vaccines
• Cancer vaccines trigger an immune response against a patient's cancer
• Molecular targets or genes that differentiate a patient's normal cells from tumor cells must be identified
• There are two types of vaccines used for cancer management:o Those intended to prevent cancer (preventive vaccines)
o Those intended to treat cancer (therapeutic cancer vaccines)
29(Polovich et al., 2014)
Preventive Vaccines
• Certain cancers are thought to be caused by viruses; therefore vaccines may help reduce the risk of cancer developmentoGardasil protects against various types of human papillomavirus (HPV)
oCervarix vaccine is targeted at preventing HPV and cervical cancer
oHep B vaccine is targeted to prevent hepatocellular carcinoma
30(Polovich et al., 2014)
Therapeutic Vaccines
• Designed to treat existing cancers. oDelay or stop cancer cell growth
oCause tumor shrinkage
oPrevent cancer from recurring
o Eliminate cancer cells that have not been killed by other treatment methods
• The purpose of cancer vaccines is to induce T cells to mount long-lasting, tumor-specific responses.
• One example is sipuleucel-T vaccine, which is an FDA-approved agent that treats prostate cancer.
31(Polovich et al., 2014)
Adoptive T-cell Transfer
• T cells play a primary role in how the immune system fights cancer.
• T-cell transfer involves collecting T cells from a patient and engineering them to recognize specific antigens on the surface of cancer cells, then infusing them back into the patient.
• CAR T-cell therapy most popular way that T-cells are being engineered.
• Two CAR T therapies are FDA-approved and more are in clinical trials.
32(Polovich et al., 2014)
Breast Cancer with VEGF (red)
(Image courtesy of the National Institutes of Health) 33
Summary
34
References
35
References• American Cancer Society. (2015). Global Cancer Facts & Figures 3rd
Edition. Retrieved from https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/global-cancer-facts-and-figures/global-cancer-facts-and-figures-3rd-edition.pdf
• Mahon, S.M. (2017). Cancer epidemiology and prevention. In Eggert, J. (Ed.) Cancer Basics (2nd Ed.). Pittsburgh, PA: Oncology Nursing Society, 39-61.
• National Cancer Institute (NCI). (2015). What is Cancer? Retrieved from https://www.cancer.gov/about-cancer/understanding/what-is-cancer
• National Cancer Institute (NCI). (2017). Metastatic Cancer. Retrieved from https://www.cancer.gov/types/metastatic-cancer#how-cancer-spreads
• Polovich, M., Olsen, M. & LeFebvre, K.B. (2014). Chemotherapy and Biotherapy Guidelines and Recommendations for Practice. Pittsburgh, PA: Oncology Nursing Society
• Tedder, M. & Eggert, J. (2017). Biology of Cancer. In Eggert, J. (Ed.) Cancer Basics (2nd Ed.). Pittsburgh, PA: Oncology Nursing Society, 3-22.
36