Embed Size (px)
Citation preview

Cancer Survivorship: Challenges and Changing ParadigmsScott M. Gilbert, David C. Miller, Brent K. Hollenbeck, James E. Montie and John T. Wei*From the Department of Urology, University of Michigan, Ann Arbor, Michigan, and the Departments of Urology and Health Services,David Geffen School of Medicine, School of Public Health and Jonsson Comprehensive Cancer Center, University of California,Los Angeles, California (DCM)
Purpose: We summarize the potential issues faced by cancer survivors, define a conceptual framework for cancer survivor-ship, describe challenges associated with improving the quality of survivorship care and outline proposed survivorshipprograms that may be implemented going forward.Materials and Methods: We performed a nonsystematic review of current cancer survivorship literature. Given thecomprehensive scope and high profile, the recent report by the Institute of Medicine, From Cancer Patient to Cancer Survivor:Lost in Transition, served as the principal guide for the review.Results: In recognition of the increasing number of cancer survivors in the United States survivorship has become an importanthealth care concern. The recent report by the Institute of Medicine comprehensively outlined deficits in the care provided to cancersurvivors, and proposed mechanisms to improve the coordination and quality of followup care for this increasing number ofAmericans. Measures to achieve these objectives include improving communication between health care providers through asurvivorship care plan, providing evidence based surveillance guidelines and assessing different models of survivorship care.Implementing coordinated survivorship care broadly will require additional health care resources, and commitment from healthcare providers and payers. Research demonstrating the effectiveness of survivorship care will be important on this front.Conclusions: Potential shortcomings in the recognition and management of ongoing issues faced by cancer survivors mayimpact the overall quality of long-term care in this increasing population. Although programs to address these issues havebeen proposed, there is substantial work to be done in this area.
Key Words: survivors, urologic neoplasms, quality of health care
Improvements in cancer directed therapies and manage-ment strategies have led to significant gains in survivalin the last several decades. While additional progress is
necessary, a substantial proportion of adult patients withcancer (an estimated 64%) currently reach 5-year survival,1
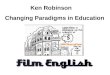
and the number of cancer survivors has increased steadilyfrom 3 million in 1971 to more than 10 million in 2002(fig. 1).2 Accordingly the quality of cancer survivorship hasgained recognition as an important but under studied areaof cancer care. Although few organized and comprehensiveprograms are currently in place, initiatives to improve thequality of care provided to cancer survivors have become apriority of survivorship advocates and policy makers.
Broadly defined, cancer survivorship encompasses the en-tire cancer continuum from initial diagnosis through the re-mainder of life. More explicitly it is focused on the distinctphase of cancer care after active cancer directed treatment, andcomprehensively extends over a range of issues faced by sur-vivors, including the physical, mental and social aspects of thecancer experience.2 For the more than 10 million cancer sur-
Submitted for publication March 21, 2007.Supported by Grant NIH-1-T-32 DKO7782 from the National In-
stitute of Diabetes and Digestive and Kidney Diseases and by theAmerican Urological Association Foundation Research ScholarsProgram (SMG).
* Correspondence: Department of Urology, The University ofMichigan, 1500 E. Medical Center Drive, Women’s Trailer Rm 1013,
Ann Arbor, Michigan 48109-0759 (telephone: 734-615-3040; FAX:734-936-9536; e-mail: [email protected]).0022-5347/08/1792-0431/0THE JOURNAL OF UROLOGY®
Copyright © 2008 by AMERICAN UROLOGICAL ASSOCIATION
431
vivors living in the United States today complications andlong-term consequences related to cancer diagnosis and treat-ment can be a substantial burden. Survivorship care encom-passes these issues broadly, and includes surveillance for theimpacts of cancer and treatment beyond disease recurrence.Accordingly monitoring for late and long-term treatment re-lated effects, assessment of HRQOL impairments, mainte-nance of general health, and management of the social andpsychological facets of cancer recovery such as rehabilitation,adjustment and reintegration into normal daily life are para-mount concerns addressed by cancer survivorship.2
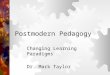
Although survivorship is an area of concern for manyphysicians, policy makers and advocates for quality cancercare, those involved in the treatment of a patient with uro-logical cancer have a particularly important stake in thisdeveloping field. Of the many million cancer survivors livingin the United States men treated for prostate cancer com-prise the second largest group, following only breast cancersurvivors in overall number (fig. 2). In aggregate urologicalmalignancies account for a quarter of the total population ofcancer survivors, and of male cancer survivors greater thanhalf are survivors of prostate, bladder, kidney or testis can-cer.2 The issues faced by urological cancer survivors may besubstantial. In prostate cancer examples range from func-tional and health related quality of life impairments in mentreated for early stage disease3 to significant late term ef-fects such as changes in body composition, bone loss, in-creased fracture risk,4 and development of diabetes and
cardiovascular disease5 in those treated with androgen de-Vol. 179, 431-438, February 2008Printed in U.S.A.
DOI:10.1016/j.juro.2007.09.029

CANCER SURVIVORSHIP432
privation therapy. In young men successfully treated fortestis cancer issues related to disease surveillance, fertility,and toxicity associated with radiation therapy and chemother-apy are highly relevant concerns. Similar examples exist forbladder and kidney cancer. Consequently issues related tolong-term cancer survivorship are important in patients diag-nosed with and successfully treated for urological cancers.
Until recently the long-term concerns and cancer relatedissues specific to this prevalent and increasing group havelargely gone unrecognized. Transitioning from a relatively fo-cused cancer control perspective to one inclusive of posttreat-ment surveillance, recovery and rehabilitation is required toadequately address and manage the late and long-term conse-quences of cancer and treatment.6 The rise of prominent sur-vivorship advocacy groups such as the National Coalition ofCancer Survivorship7 and the Lance Armstrong Foundation8
underscore the importance of this challenge. Further supportfrom influential organizations such as the National CancerInstitute and the American Cancer Society has contributed tothe dialogue on survivorship initiatives. However, widespreadimplementation of structured programs has yet to gain trac-tion, and the role and form of survivorship care in the overallapproach to cancer remains ill defined. This review outlines therange of issues faced by cancer survivors, describes a concep-tual framework for cancer survivorship, and reviews severalproposed survivorship programs and potential challenges as-sociated with improving the quality of survivorship care.
DEFINING ANDPRIORITIZING CANCER SURVIVORSHIP
In response to the challenge issued by Mullan, a physician andcancer survivor, to “map the middle ground of survivorship andminimize its medical and social hazards,”9 the Institute ofMedicine established a special committee to examine the med-ical and psychosocial issues faced by the increasing number ofcancer survivors. The resulting report outlined several objec-tives to increase awareness of the needs of cancer survivors,establish survivorship as a distinct phase of cancer care andensure that cancer survivors receive appropriate care duringthis often under recognized phase of the cancer continuum.2 Atotal of 10 recommendations were issued ranging from survi-vor directed interventions to system based approaches (see
FIG. 1. Estimated number of cancer survivors in United States from1971 to 2002.2
Appendix). While some recommendations will likely be achiev-
able without undue effort, some will require systematic re-structuring of the care provided to cancer survivors. Others,such as recommendations to improve opportunities in survi-vorship research, will require a significant commitment fromthe health care community, including funding agencies in-vested in advancing cancer care.
Survivorship Care PlanTo a large extent care after cancer treatment is typicallyfocused on surveillance for disease recurrence. Despite theimportance of this objective, other significant health prob-lems may persist or become apparent later in the course ofthe cancer trajectory. In this setting the success of the initialcancer treatment may be undermined by failing to antici-pate and address later detrimental health effects. Establish-ing a survivorship care plan has been suggested to preventthe disconnect between successful initial cancer therapy andsuboptimal long-term followup care.2
For the majority of cancer survivors in the United Statestoday, followup care is provided by a cancer specialist, and
FIG. 2. Distribution of cancer survivors in United States by cancersite in 2002.2 GU, genitourinary.

CANCER SURVIVORSHIP 433
while intermittent communication between primary care phy-sicians and cancer specialists may take place, coordination offollowup care often varies. As with many other facets of currentfollowup care, the duration and intensity of surveillance mayalso vary widely. In general, ongoing, coordinated survivorshipcare does not extend beyond a relatively short followup andalthough special services are available to cancer survivors,most are underused.10 As a result, potential health problemsmay be missed due to a myopic perspective. The lack of acomprehensive plan outlining the specific needs of cancer sur-vivors may contribute to the incomplete transition of care fromthe cancer specialist to the primary care physician, resulting inlost opportunity to transfer essential information.1 Communi-cation, if present, is often episodic and may fail to incorporatepertinent information which facilitates primary care physicianability to provide high quality and necessary followup care.1 Inthis setting efforts to improve the overall quality of care pro-vided to cancer survivors are needed.
The survivorship care plan is a document created bythose primarily responsible for cancer treatment to providedetailed information regarding patient cancer and treat-ment history, define surveillance schedules, identify healthpriorities related to cancer therapy and general health, andindicate how (by whom and in what setting) followup care isprovided. It is tailored to each cancer survivor, modified ac-cording to developing concerns and needs, shared with thepatient, the primary care provider and members of the patientsupport network, and modifiable on completion of active ther-apy. Essential aspects include a comprehensive summary of allcare received, detailed pertinent cancer specific informationsuch as tumor characteristics, and a clear description of whatought to be done during short-term and long-term followup.11
This information is important to survivors and physicians,because a substantial number of patients are not knowledge-able about the treatments they have received.12 Additionalinformation, such as the likely course of recovery, expectedshort-term toxicities related to treatment, outlined strategiesfor ongoing health maintenance and recommended preventa-tive treatments, likely improve the usefulness of the plan andmay translate into better cancer care.11
A second goal of the survivorship care plan is to optimize thecontinuity and coordination of care. Because followup care forpatients with cancer is often complex, involves a number ofhealth care providers and is not universally provided at asingle treatment site, the potential for fragmented and poorlycoordinated care exists. While some motivated cancer survi-vors organize treatment information and serve, in effect, ascoordinators of their own care, this is not the case for all. In facta significant number of patients are not certain which physi-cian is responsible for followup care, indicating that a moresystematic process is needed.13 Consequently health care pro-viders and systems must adapt to the unique challenges oftreating a diverse group of patients who are often mobile, andreceive care from many sources, physicians and locations. Spe-cific provider identification and role definition are needed tooptimize the coordination of the multifaceted aspects of cancercare and surveillance, and avoid unnecessary physician visits,redundant evaluations and inefficient use of limited resources.By serving as a transferable source of information the survi-vorship care plan is designed to address this frequent gap in
care.Developing Evidence Based SurveillanceGuidelines and Posttreatment AssessmentAccording the Institute of Medicine recommendations sur-vivorship care should be founded on evidence based clinicalpractice guidelines, assessment tools and screening instru-ments.2 Although disease surveillance is a standard part ofthe followup care currently provided to cancer survivors,frequency and type of surveillance vary. For many cancersthis variability stems, in part, from a lack of well-defined,evidence based guidelines and may reflect a lack of consen-sus among cancer care providers.14 Close surveillance ismost beneficial in situations in which detection of recurrentdisease results in intervention that prolongs survival. How-ever, this is not the case for all diseases or clinical settings.Although patients and providers appear to value close fol-lowup contact,15,16 early detection of disease recurrence of-ten does not increase the likelihood of salvage.17,18 Further-more, while proponents of early surveillance argue fordetecting and preventing potentially devastating complica-tions related to disease recurrence, it has not been widelysupported by clinical trials to date.19 Given the lack of clin-ical evidence and uncertainty regarding the appropriate fre-quency and intensity of surveillance, further work will berequired to define optimal followup for many cancers, includ-ing urological malignancies.
In the absence of high level clinical evidence, treatmentand surveillance guidelines for many cancers are largelyconsensus based.20 The American Society of Clinical Oncol-ogy has released evidence based guidelines for breast andcolorectal cancer, and comprehensive and detailed consen-sus based guidelines for many other cancers are availablefrom the National Comprehensive Cancer Network. How-ever, the lack of well-defined evidence supporting surveil-lance procedures has resulted in substantial variability infollowup of survivors and, thus, many receive more intensesurveillance than recommended.21,22 More care does not al-ways equate to better care. For example, in breast and colorec-tal cancer evidence based clinical guidelines support limitedsurveillance testing.23–25 However, even in this setting a sig-nificant proportion of survivors do not receive basic recom-mended followup care.22 Given these deficiencies, additionalwork is required to improve the quality of evidence definingsurveillance recommendations and to assure that survivorsreceive optimal followup care. The benefits of this approachmay be substantial. With well conceived evidence based guide-lines variations in clinical practice may decrease, resulting inmore efficient and potentially effective health care delivery.21
Furthermore, well designed and supported clinical guidelinesmay facilitate the delivery of necessary care.11
Surveillance is not restricted to disease recurrence. Thenumber of cancer survivors older than 65 years is increasingsteadily and an additional challenge is expanding surveil-lance to include noncancer health problems in this agingpopulation. In many cancer survivors overall health may beas important as cancer specific concerns, and although pa-tients with cancer are exposed to many health resources andprofessionals, they may not always receive the same qualityof care for chronic medical problems during active cancertreatment and surveillance.26,27 To provide high qualitycare cancer specialists may have to partner with primarycare physicians to ensure that cancer and general healthissues are addressed appropriately. The survivor experience
may facilitate this objective, as many survivors become more
CANCER SURVIVORSHIP434
health conscious after successful therapy. This period hasbeen referred to as a teachable moment in which attentiveand motivated survivors can be encouraged to change healthbehaviors meaningfully.28 As a result many care providersadvocate modifiable health behaviors such as smoking ces-sation, changes in diet, decreased alcohol consumption andincreased physical activity in the survivorship care plan. Inaddition, many survivorship advocates argue for broadeningsurvivorship care to include psychosocial issues and eco-nomic consequences after cancer treatment.2
APPLIED MODELS FORDELIVERING SURVIVORSHIP CARE
Conceptually survivorship begins with established care af-ter cancer diagnosis. In this setting treatment options arediscussed and implemented if appropriate. After treatmenta period of surveillance is typical to detect short and inter-mediate term complications, followed by a transition tolonger term care. This period of survivorship care should beinclusive, and encompass cancer specific issues, generalhealth concerns and less commonly assessed areas of poten-tial impairment (fig. 3). It is often the weak link in presentcare.2 Several models have been proposed to provide qualitysurvivorship care. Although approaches vary, all modelshave a common goal of improving the quality of care forcancer survivors by delivering comprehensive, coordinatedand tailored followup. Because cancer survivors comprise alarge and diverse group, individual needs vary considerablyand can be summarized by 4 commonly applied models forcancer survivorship.
Shared Care ModelThe shared care model, as implied, involves care shared andcoordinated between 2 or more health care providers indifferent specialties or locations. Because this approach hasimproved outcomes and facilitated effective management ofchronic diseases such as diabetes and chronic renal disease,it is used extensively throughout the United States.29,30 The
FIG. 3. Conceptual model of current follo
success of the shared care approach is regular personalcommunication, and periodic knowledge transfer betweenspecialists and primary care physicians. Although addi-tional assessment is necessary, the shared care model maybe beneficial in improving the quality of survivor care. In-volving more than 1 physician in the care of cancer survivorsappears to increase the likelihood of quality care. For example,a study revealed that patients with colorectal cancer treated byan oncologist and a primary care physician were significantlymore likely to receive recommended care compared to thosetreated by either physician alone.27 Although experience withthe shared care model in cancer care is limited in the UnitedStates, several European and Canadian studies indicate thatthis model may be appropriate for cancer survivors.19,31,32
Because the shared care model uses existing resources, itmay be more easily implemented than other survivorshipmodels. In addition, application of a survivorship care planmay increase physician communication and coordination ofcare, and direct re-referral to the cancer specialist when lateterm effects and concerns arise. A care manager to serve asan intermediary between the oncologist and primary carephysician has also been proposed as a potential refine-ment.33 Advances in technology may also improve the effec-tiveness and efficiency of the shared care model. For exam-ple, increasing use of electronic medical systems mayimprove information transfer and physician communication.Successful shared care reintegrates the primary care physi-cian into the overall care of the cancer survivor when gen-eral medical and health maintenance needs may be over-shadowed by cancer specific concerns.1
Risk Based Followup CareWhile some survivors will not require nor desire close fol-lowup care, those at high risk for health detriment requiremore intense surveillance and care. In childhood can-cers34,35 and breast cancer36,37 a risk based approach hasbeen used to address differential surveillance requirementsbased on severity of disease, treatment characteristics and
wup care and cancer survivorship2

CANCER SURVIVORSHIP 435
risk of detrimental health effects, and to provide appropriatecare at the individual level.38 A principal component of therisk based approach is that the survivorship followup plan isadaptable and can be tailored to the specific needs of eachcancer survivor. Typically nurses have been the coordinatorsof such risk based long-term followup clinics.35,39 In child-hood cancers these programs promote continuity40 and ef-fectively manage cancer related symptoms.41 The success ofthis model will depend on several factors including identify-ing, redirecting and retraining a segment of health careproviders, such as nurses, to serve as coordinators.2
Cancer Specific Survivorship ClinicsDedicated survivorship clinics are designed to provide a rangeof services and comprehensive care to cancer survivors in asingle clinical setting. In many ways this approach representsan extension of long-term followup programs to managethe needs of childhood cancer survivors after completion oftherapy.42 Several resources are brought together in long-termfollowup clinics. Care is generally coordinated by an oncologynurse practitioner, a multidisciplinary approach consisting ofsurgical, medical and radiation oncologists as well as re-constructive surgeons is generally used, and many programsuse social workers and psychiatric services. The central prin-ciples such as risk based assessment, and care coordinationand continuity are transferable, and may contribute substan-tially to improved care in adult cancer survivors. Disease spe-cific cancer survivorship programs were first initiated in breastcancer to address treatment related effects such as lymph-edema, changes in body image, depression, weight control and,less commonly, cardiac disease. Other disease focused pro-grams have been initiated but are not as well established. Thestructure, available resources and objectives vary according todisease and clinic design. However, few adult cancer survivorsare currently followed in this setting.
Institution Based Survivorship ProgramsComprehensive survivorship programs are being developedat several academic cancer centers. In contrast to diseasespecific survivorship clinics these institution based pro-grams provide coordinated and tailored care to survivors ofall cancers in a single clinical setting. In theory institutionbased programs limit the redundancy inherent in operatingseveral cancer specific clinics. While potentially more com-plex, this approach uses shared clinical and research re-sources and expertise, and may ultimately prove to be moreefficient than several separate disease specific clinics.1 Re-solving recognized challenges such as ensuring flexibility inhow survivors navigate and use program resources will re-quire innovation and novel thought. There is increasinginterest and support for this model, as indicated by thenetwork of cancer centers funded through the Lance Arm-strong Foundation.8 In the coming years additional clinicalexperience, systems development and research will providefurther insight into this developing model.
SURVIVORSHIP CAREIN UROLOGICAL CANCERS
Although optimal surveillance procedures have not beencompletely defined for survivors of urological cancers, sev-
eral health concerns and impairments have emerged as ar-eas of necessary care. For prostate cancer survivors issues ofsurvivorship range from routine health related quality of lifeassessment, and management of urinary incontinence, sex-ual dysfunction and bowel complaints, to the many sideeffects associated with androgen deprivation therapy suchas decreased bone mineral density and increased risk ofskeletal fracture. Bladder cancer survivors treated with cys-tectomy experience changes in urinary and bowel functionafter urinary diversion, and long-term health concerns in-cluding downstream consequences related to gastrointesti-nal malabsorption, HRQOL impairments and changes inbody image may be under recognized. For bladder cancersurvivors treated for nonmuscle invasive disease, surveil-lance frequency and detection of recurrent disease are im-portant considerations. Concerns for testis cancer survivorsmay focus on disease recurrence and preservation of fertil-ity. However, other important processes of surveillanceshould be considered, such as assessing the remaining testisfor tumor development and monitoring for secondary malig-nancies in those treated with radiation and chemotherapy.In survivors of kidney cancer surveillance for renal functionand disease recurrence are 2 common concerns. However,without effective salvage therapy or evidence based surveil-lance guidelines followup imaging may be more commonlyobtained than warranted. These examples are not meant tobe a complete list of concerns faced by survivors of urologicalcancers. Instead they underscore the many issues and un-certainties regarding optimal and necessary survivorshipcare in this population.
The care of urological cancer survivors may be improvedin several ways. An important first step may be widespreadimplementation and application of survivorship care plans.As discussed, common use of a survivorship care plan facil-itates physician communication, provides a guide for fol-lowup care, and helps coordinate disease and health surveil-lance. In prostate cancer survivors treated with ADTinformation related to disease severity, previous local treat-ments if any, type, frequency and duration of ADT, sideeffects related to the hypogonadal state, and potential risksassociated with prolonged ADT exposure such as metabolicchanges and bone mineral density loss guides care giversregarding treatment history, associated symptoms and po-tential downstream health risks. Evidence based surveil-lance practices are an additional area requiring consider-ation. In several cases, such as cystoscopic surveillance forsuperficial bladder cancer and radiographic imaging surveil-lance for renal cell carcinoma, the effectiveness, optimalfrequency and duration of surveillance have not yet beendetermined. In the absence of evidence based guidelinesclinicians may base surveillance on consensus based guide-lines such as those provided by the National ComprehensiveCancer Network and the American Urological Association.43
Program development and advancement in the form ofdisease specific and institution based survivorship clinicsmay serve as a logical next step to systematically improvesurvivorship care. While few organized programs are cur-rently in place for prostate cancer survivors, the high rate ofcancer control obtainable with treatment, and the functionaland health related quality of life impairments associatedwith different therapies have resulted in a prevalent groupof survivors who may benefit from structured, coordinatedand tailored survivorship care. Although efforts are cur-
rently under way, these programs are in the earliest stages
CANCER SURVIVORSHIP436
of development. Determining how patients respond to morestructured and coordinated followup care and, more impor-tantly, if these approaches improve patient outcomes, arerelevant issues that may be addressed through concomitantclinical research in the setting of survivorship clinics.
SURVIVORSHIP RESEARCH
While efforts and clinical initiatives to improve cancer sur-vivor care are in the early stages of development, an equallyimportant initiative is to promote and advance survivorshipresearch. This is a potentially fertile area of translationalresearch that will further facilitate the quality of care pro-vided to cancer survivors. A number of important questionsregarding survivorship remain to be answered. Although thebenefits of survivorship care are intuitive, coordinated andcomprehensive care has not been tested empirically, andthere is a potential for increased resource expenditure with-out concurrent improvement in outcomes. Consequently sur-vivorship models should be compared quantitatively andobjectively. Defining optimal, evidence based surveillancepractices is an additional research priority. As indicated inbreast and colorectal cancer, more testing does not alwayslead to improved outcomes. In the majority of cancers, in-cluding urological malignancies, questions regarding fre-quency, type and intensity of followup care have not beenadequately addressed. Given the limited amount of researchand knowledge currently available to push survivorship careforward, the Institute of Medicine has identified this as apriority in its recommendations.
Outcomes metrics are also expanding, and increasingly cli-nicians and researchers appreciate the importance of cancerrelated outcomes other than survival. As therapy has becomemore effective and life has been prolonged, treatment relatedcomplications, health impairment and health related quality oflife have become more relevant and important outcomes. Qual-ity of life research and survivorship experiences are interre-lated, because both are measures of how patients treated forcancer function and experience life after treatment. To datesurvivorship research in prostate cancer has been largelybased on HRQOL measurement and comparison, and severallongitudinal population based cohort studies have estimatedthe burden of disease and treatment using HRQOL as theprimary measure.44 Future research on preventing and man-aging prevalent conditions and complications in cancer survi-vors would be beneficial. The results from such research maybe used to guide followup survivorship care,45 guideline devel-opment and health policy.46
Survivorship research will benefit from directed efforts toincrease long-term health assessment in randomized clinicaltrials and observational studies. Indeed the long-term na-ture of many survivorship issues requires substantial fore-sight and investment in longitudinal measures and datacollection. Although some researchers have advocated incor-porating long-term complication and health related qualityof life measures into randomized clinical trials,46 existingresources such as the National Cancer Institute supportedCancer Care Outcomes Research and Surveillance Consor-tium and the Cancer Research Network may be an informa-tive and efficient starting point.47,48 Regardless, the successof the survivorship research initiative may ultimately be
based on commitment to these endeavors.CONCLUSIONS
As the number of individuals treated successfully for cancerhas increased, health issues that extend beyond the imme-diate posttreatment and early surveillance phase of followupcare have become more relevant. The number of cancersurvivors in the United States will continue to increase, par-ticularly in light of changes in the age structure projected incoming years. The cancer experience may result in healthimpairments that have previously gone unrecognized after suc-cessful cancer treatment. Furthermore, the followup care pro-vided to the majority of cancer survivors varies, and in manyinstances evidence guiding the type and intensity of surveil-lance is lacking. Substantial improvement in the quality of careprovided during the survivorship phase may be realized withinitiatives to improve the coordination of care, and monitorlong-term and late complications of cancer and treatment. Al-though early in development, structured and coordinated sur-vivorship care is gaining acceptance. Measures such as provid-ing a survivorship care plan at discharge from active cancertreatment may be realized without undue effort. However,greater challenges, such as ensuring efficient use of health careresources, implementing effective models of survivorship care,improving the quality of evidence supporting surveillanceguidelines, providing additional opportunities for high impactsurvivorship research and evaluating the overall effectivenessof survivorship care will ultimately determine the evolving roleof survivorship care.
APPENDIX
Institute of Medicine RecommendationSummary Adapted From Hewitt et al2
Recommendation 1 Raise awareness of the needs of cancer survivors,establish cancer survivorship as a distinct phaseof cancer care and act to ensure the delivery ofappropriate survivorship care.
Recommendation 2 Provide a comprehensive care summary andfollowup plan (survivorship care plan) that isclearly and effectively explained to all patientscompleting active cancer therapy.
Recommendation 3 Use systematically developed evidence basedclinical practice guidelines, assessment toolsand screening instruments to help identify andmanage late effects of cancer and its treatment.
Recommendation 4 Develop quality of survivorship care measuresand implement quality assurance programs tomonitor and improve the care that all cancersurvivors receive.
Recommendation 5 Test models of coordinated, interdisciplinarysurvivorship care in diverse communities andacross systems of care.
Recommendation 6 Develop comprehensive cancer control plans thatinclude consideration of survivorship care, andpromote the implementation, evaluation andrefinement of existing state cancer control plans.
Recommendation 7 Expand and coordinate efforts to provideeducational opportunities to health care providersto equip them to address the health care andquality of life issues facing cancer survivors.
Recommendation 8 Act to eliminate discrimination and minimizeadverse effects of cancer on employment, whilesupporting cancer survivors with short-term andlong-term limitations in ability to work.
Recommendation 9 Act to ensure that all cancer survivors haveaccess to adequate and affordable healthinsurance with the assistance of insurers andhealth care payors.
Recommendation 10 Increase funding support of survivorshipresearch and expand mechanisms for itsconduct to better guide effective survivorship
care.
CANCER SURVIVORSHIP 437
Abbreviations and Acronyms
ADT � androgen deprivation therapyHRQOL � health related quality of life
IOM � Institute of Medicine
REFERENCES
1. Oeffinger KC and McCabe MS: Models for delivering survivor-ship care. J Clin Oncol 2006; 24: 5117–5124.
2. Hewitt M, Greenfield S and Stovall E: From Cancer Patient toCancer Survivor: Lost in Transition. Washington, D. C.:The National Academies Press 2006.
3. Miller SC, Sanda MG, Dunn RL, Montie JE, Pimentel H,Sandler HM et al: Long-term outcomes among localizedprostate cancer survivors: health-related quality-of-lifechanges after radical prostatectomy, external radiation andbrachytherapy. J Clin Oncol 2005; 23: 2772.
4. Shahinian VB, Kuo YF, Freeman JL and Goodwin JS: Risk offracture after androgen deprivation for prostate cancer.N Engl J Med 2005; 352: 154.
5. Keating NL, O’Malley AJ and Smith MR: Diabetes and cardio-vascular disease during androgen deprivation therapy forprostate cancer. J Clin Oncol 2006; 24: 4448.
6. Grunfeld E: Looking beyond survival: how are we looking atsurvivorship? J Clin Oncol 2006; 24: 5166.
7. National Coalition of Cancer Survivorship. Available at http://www.canceradvocacy.org/. Accessed February 2007.
8. Lance Armstrong Foundation. Available at http://www.livestrong.org/. Accessed February 2007.
9. Mullan F: Seasons of survival: reflections of a physician withcancer. N Engl J Med 1985; 313: 270.
10. Tesauro GM, Rowland JH and Lustig C: Survivorship re-sources for post-treatment cancer survivors. Cancer Pract2002; 10: 277.
11. Earle CC: Failing to plan is planning to fail: improving thequality of care with survivorship care plans. J Clin Oncol2006; 24: 5112.
12. Makaryus AN and Friedman EA: Patients’ understanding oftheir treatment plans and diagnosis at discharge. MayoClin Proc 2005; 80: 991.
13. Miedema B, MacDonald I and Tatemichi S: Cancer follow-upcare. Patients’ perspectives. Can Fam Physician 2003; 49:890.
14. Johnson FE: Overview. In: Cancer Patient Follow-Up. Editedby FE Johnson and KS Virgo. St. Louis: Mosby 1997; p 4.
15. Impact of follow-up testing on survival and health-relatedquality of life in breast cancer patients. A multicenter ran-domized controlled trial. The GIVIO investigators. JAMA1994; 271: 1587.
16. Muss HB, Tell GS, Case LD, Robertson P and Atwell BM:Perceptions of follow-up care in women with breast cancer.Am J Clin Oncol 1991; 14: 55.
17. Fong Y, Cohen AM, Fortner JG, Enker WE, Turnbull AD, CoitDG et al: Liver resection for colorectal metastases. J ClinOncol 1997; 15: 938.
18. NIH consensus conference. Ovarian cancer. Screening, treat-ment and follow-up. NIH Consensus Development Panel onOvarian Cancer. JAMA 1995; 273: 491.
19. Grunfeld E, Levine MN, Julian JA, Coyle D, Szechtman B,Mirsky D et al: Randomized trial of long-term follow-up forearly-stage breast cancer: a comparison of family physi-cians versus specialist care. J Clin Oncol 2006; 24: 848.
20. National Comprehensive Cancer Network: Clinical PracticeGuidelines in Oncology. Available at http://www.nccn.org/professionals/physician_gls/default.asp. Accessed January
2007.21. Elston Lafata J, Simpkins J, Schultz L, Chase GA, JohnsonCC, Yood MU et al: Routine surveillance care after cancertreatment with curative intent. Med Care 2005; 43: 592.
22. Cooper GS, Johnson CC, Lamerato L, Poisson LM, Schultz L,Simpkins J et al: Use of guideline recommended follow-upcare in cancer survivors: routine of diagnostic indications?Med Care 2006; 44: 590.
23. Smith TJ, Davidson NE, Schapira DV, Grunfeld E, Muss HB,Vogel VG 3rd et al: American Society of Clinical Oncology1998 update of recommended breast cancer surveillanceguidelines. J Clin Oncol 1999; 17: 1080.
24. Bast RC Jr, Ravdin P, Hayes DF, Bates S, Fritsche H Jr,Jessup JM et al: 2000 update of recommendations for theuse of tumor markers in breast and colorectal cancer: clin-ical practice guidelines of the American Society of ClinicalOncology. J Clin Oncol 2001; 19: 1865.
25. Desch CE, Benson AB 3rd, Somerfield MR, Flynn PJ, KrauseC, Loprinzi CL et al: Colorectal cancer surveillance: 2005update of an American Society of Clinical Oncology practiceguideline. J Clin Oncol 2005; 23: 8512.
26. Earle CC, Burstein HJ, Winer EP and Weeks JC: Quality ofnon-breast cancer health maintenance among elderlybreast cancer survivors. J Clin Oncol 2003; 21: 1447.
27. Earle CC and Neville BA: Under use of necessary care amongcancer survivors. Cancer 2004; 101: 1712–1719.
28. Ganz PA: A teachable moment for oncologists: cancer survi-vors, 10 million strong and growing! J Clin Oncol 2005; 23:5458.
29. Renders CM, Valk GD, de Sonnaville FF, Twisk J, KriegsmanDM, Heine RJ et al: Quality of care for patients with type 2diabetes mellitus: a long-term comparison of two qualityimprovement programmes in The Netherlands. Diabet Med2003; 20: 846.
30. Jones C, Roderick P, Harris S and Rogerson M: An evaluationof a shared primary and secondary care nephrology servicefor managing patients with moderate to advanced CKD.Am J Kidney Dis 2006; 47: 103.
31. Braun TC, Hagen NA, Smith C and Summers N: Oncologistsand family physicians: using a standardized letter to im-prove communication. Can Fam Physician 2003; 49: 882.
32. Nielsen JD, Palshof T, Mainz J, Jensen AB and Olesen F:Randomized controlled trial of a shared care programme fornewly referred cancer patients: bridging the gap betweengeneral practice and hospital. Qual Saf Health Care 2003;12: 263.
33. Oxman TE, Dietrich AJ, Williams JW Jr and Kroenke K: Athree-component model for reengineering systems for thetreatment of depression in primary care. Psychosomatics2002; 43: 441.
34. Hewitt M, Weiner SL and Simone JV: Childhood Cancer Sur-vivorship: Improving Care and Quality of Life. Washington,D. C.: The National Academies Press 2003.
35. Oeffinger KC: Longitudinal risk-based health care for adultsurvivors of childhood cancer. Curr Probl Cancer 2003; 27:143.
36. Ganz PA, Desmond KA, Leedham B, Rowland JH, MeyerowitzBE and Belin TR: Quality of life in long-term, disease-freesurvivors of breast cancer: a follow-up study. J Natl CancerInst 2002; 94: 39.
37. Ganz PA, Greendale GA, Petersen L, Kahn B and Bower JE:Breast cancer in younger women: reproductive and latehealth effects of treatment. J Clin Oncol 2003; 21: 4184.
38. Wallace WH, Blacklay A, Eiser C, Davies H, Hawkins M,Levitt GA et al: Developing strategies for long term followup of survivors of childhood cancer. BMJ 2001; 323: 271.
39. Hollen PJ and Hobbie WL: Establishing comprehensive spe-cialty follow-up clinics for long-term survivors of cancer.Providing systematic physiological and psychosocial sup-
port. Support Care Cancer 1995; 3: 40.
CANCER SURVIVORSHIP438
40. Smith ED, Walsh-Burke K and Crusan C: Principles of train-ing social workers in oncology. In: Psycho-Oncology. Editedby JC Holland. New York: Oxford University Press 1998.
41. Cox K and Wilson E: Follow-up for people with cancer: nurse-led services and telephone interventions. J Adv Nurs 2003;43: 51.
42. Oeffinger KC, Eshelman DA, Tomlinson GE and BuchananGR: Programs for adult survivors of childhood cancer.J Clin Oncol 1998; 16: 2864.
43. American Urological Association Clinical Guidelines. Avail-able at www.auanet.org/guidelines/. Accessed June 2007.
44. Potosky AL, Harlan LC, Stanford JL, Gilliland FD, HamiltonAS, Albertsen PC et al: Prostate cancer practice patternsand quality of life: the Prostate Cancer Outcomes Study.
J Natl Cancer Inst 1999; 91: 1719.45. Giesler RB, Given B, Given CW, Rawl S, Monohan P, Burns Det al: Improving the quality of life of patients with prostatecancer: a randomized trial testing the efficacy of a nurse-driven intervention. Cancer 2005; 104: 752.
46. Ayanian JZ and Jacobsen PB: Enhancing research on cancersurvivors. J Clin Oncol 2006; 24: 5149.
47. Ayanian JZ, Chrischilles EA, Fletcher RH, Fouad MN,Harrington DP, Hahn KL et al: Understanding cancertreatment and outcomes: the Cancer Care Outcomes Re-search and Surveillance Consortium. J Clin Oncol 2004; 22:2992.
48. Wagner EH, Green SM, Hart G, Field TS, Fletcher S, GeigerAM et al: Building a research consortium of large healthsystems: the Cancer Research Network. J Natl Cancer Inst
Monogr 2005; p 3.