Embed Size (px)
Citation preview
Cancer and Aging: Challenges and Opportunitiesacross the Cancer Control Continuum
Supplement to Cancer
Cancer Survivorship and Aging
Nancy E. Avis, PhD1
Gary T. Deimling, PhD2
1 Department of Social Sciences and HealthPolicy, Division of Public Health Sciences, WakeForest University School of Medicine, Winston-Salem, North Carolina.
2 Department of Sociology, Case WesternReserve University, Cleveland, Ohio.
Cancer is primarily a disease of the elderly. Greater than 60% of new cancers
occur in people aged >65 years, and 60% of the current 10 million cancer survi-
vors are aged �65 years. Given these large numbers and the potential vulnerabil-
ity of older adults, older cancer survivors have become an especially important
group to study. This article discusses published research on the physical and
mental functioning of older cancer survivors. In the first part, the authors
reviewed studies of those who are newly diagnosed at the age of �65 years. The
second part reviewed the research regarding long-term (�5 years) cancer survi-
vors who are aged >65 years, but may have been diagnosed at a younger age.
Older survivors are likely to be more affected by cancer in terms of physical than
psychologic function. However, comparisons with individuals without a history of
cancer suggest that older cancer survivors may be faring worse physically and
psychologically than noncancer comparison groups. For older cancer survivors,
cancer occurs against a background of other chronic conditions and normal aging,
and comorbidities and symptoms are important factors to consider. Limitations of
the research were discussed, and recommendations for future research were pro-
vided. In particular, prospective studies with measures of functioning before can-
cer diagnosis and treatment, comparisons with age-matched noncancer
populations, and interventions to reduce the impact of cancer on functioning are
needed. Cancer 2008;113(12 suppl):3519–29. � 2008 American Cancer Society.
KEYWORDS: aging, elderly, oncology, cancer survivors, quality of life.
C ancer is primarily a disease of the elderly. Greater than 60% of
new cancers occur in people aged >65 years.1 The incidence
rate for all sites triples in persons ages 60 years to 70 years, com-
pared with individuals aged 40 to 59 years.2 Moreover, as the pro-
portion of the US population aged �65 years increases, even greater
numbers of older individuals will be diagnosed with cancer.3,4
Improved early detection and treatment have also increased the
number of people who have cancer for an extended period of time.
Of the current 10 million cancer survivors, 60% are aged �65 years,
and >16% of US adults aged �65 years are cancer survivors.5 Given
these large numbers and the potential vulnerability of older adults,
older cancer survivors have become an especially important group
to study.
Survivorship represents a relatively new way of thinking about
cancer as it is experienced by those who are diagnosed and treated
for this disease. In the past, poor survival rates for the majority of
cancers resulted in thinking of cancer as a ‘‘death sentence.’’ How-
ever, improved survival rates have made a survivorship orientation
Sponsored by the National Cancer Institute’sOffice of Cancer Survivorship.
Presented at the Society of Behavioral Medicinepreconference entitled ‘‘Cancer and Aging: Chal-lenges and Opportunities across the Cancer Con-trol Continuum,’’ Washington, DC, March 21,2007.
Address for reprints: Nancy E. Avis, PhD, Divisionof Public Health Sciences, Department of SocialSciences and Health Policy, Wake Forest Univer-sity School of Medicine, Piedmont Plaza II, Sec-ond Floor, Winston-Salem, NC 27157-1063; Fax:(336) 716-7554; E-mail: [email protected]
Received November 7, 2007; accepted January2, 2008.
ª 2008 American Cancer SocietyDOI 10.1002/cncr.23941Published online 3 December 2008 in Wiley InterScience (www.interscience.wiley.com).
3519

more realistic. This, along with the perspective of
cancer as a chronic disease,5,6 has resulted in survi-
vorship becoming a new focus for both the clinicians
who treat cancer patients and the scientists who
study them.
The term ‘‘survivor’’ now refers not only to those
who have lived for an extended period of time after
treatment, but also includes newly diagnosed indivi-
duals as well as those who are in treatment, have
completed treatment, or are in remission. This
change in orientation and language has been
adopted and promoted by the American Cancer Soci-
ety and the National Coalition of Cancer Survivors.
In fact, the National Cancer Institute’s Office of Can-
cer Survivorship defines a survivor as anyone who
has been diagnosed with cancer.7 Taken together, the
definition of a cancer survivor now includes a range
of individuals beginning with those newly diagnosed
to those who have been free of cancer for decades.
This article discusses the physical and mental
functioning of older cancer survivors across a tempo-
ral continuum. The first part reviewed research on
survivors age �65 years who are relatively newly
diagnosed (�3 years) with cancer. The second part
reviewed research on older survivors who represent
long-term survivors. In reviewing the research, we
focused on published research based on samples of
cancer survivors aged >60 years only or research
that specifically compared survivors of different age
categories. We began our search with recently pub-
lished articles identified through PubMed and added
articles cited in these publications. This article did
not attempt to provide an exhaustive review of all
published research on older cancer survivors, but
rather to present a sense of what is currently known
regarding older cancer survivors, the limitations of
this research, and directions for future research.
We should mention several factors that make
comparisons across studies particularly challenging.
One challenge is differing age distributions and cut-
points across studies. The most common cutpoint
for older survivors is 65 years of age, but this is not
used uniformly. Second, samples differ in their time
since diagnosis. Some smaller studies have samples
comprised of survivors with very explicit time inter-
vals from diagnosis (eg, 3 months, 1 year), whereas
other large cohort studies may have wider ranges
(eg, any cancer survivor). Third, some studies control
for important covariates, and others do not. As seen
in this review, these covariates (particularly comor-
bidities and symptoms) are important considerations
in studying older survivors. Fourth, studies involve
different cancer sites. The majority of studies focus
on breast cancer survivors, but others include survi-
vors of multiple cancer sites. As seen in these stu-
dies, quality of life (QOL) issues vary by cancer site.
Despite these challenges, there are some consistent
patterns to the findings, and those patterns are the
focus of this article.
Studies of Newly Diagnosed Older PatientsAlthough many studies have examined the physical
and mental status of newly diagnosed cancer
patients, to our knowledge few have focused specifi-
cally on older patients or on age-related compari-
sons. Even fewer provide comparisons with a general
population. We classified these studies into 2 cate-
gories: 1) those that include older cancer survivors
only or compare older and younger survivors, and 2)
those that provide a comparison between older can-
cer patients with the general population.
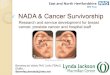
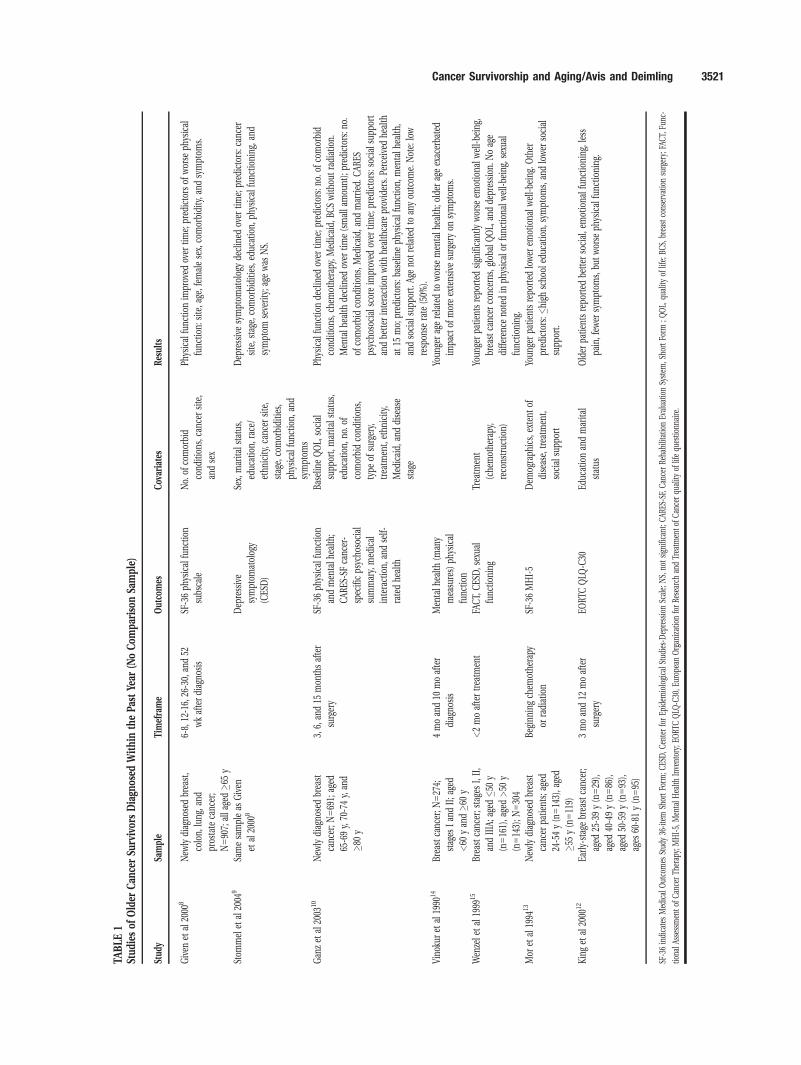
Newly diagnosed older survivors (no comparison group)Given et al8,9 and Ganz et al10 have conducted what
to our knowledge are the largest studies published to
date focusing specifically on older cancer survivors
during the first year after diagnosis (Table 1). The
primary aim of these studies was to examine the tra-
jectory of functioning in the year after diagnosis and
factors related to better functioning. Both studies
assessed functioning with the Medical Outcomes
Study 36-item Short Form (MOS SF-36), but found
somewhat different results in terms of the trajectory
of functioning over time.
Given et al studied 907 newly diagnosed breast,
colon, lung, and prostate cancer patients aged �65
years and found that physical functioning improved
over 1 year8 and that symptoms of depression
decreased over 1 year.9 Ganz et al10 followed 691
newly diagnosed breast cancer patients aged �65
years for 15 months and found that both physical
functioning and mental health on the SF-36 declined
over time. It is difficult to determine why these stu-
dies found different patterns of functioning using the
same instrument and similar timeframes. Differences
cannot be explained by cancer site, because Given
et al found improvement among all cancer sites.
Interestingly, Ganz et al found improvement over
time on a cancer-specific psychosocial instrument
(Cancer Rehabilitation Evaluation System). Both stu-
dies, however, found that the number of comorbid
conditions was a significant predictor of changes in
physical and mental health. Given et al8,9 also found
that improvement in physical function was corre-
lated with cancer site, being female, and having
fewer symptoms; a decrease in depressive symptom-
atology was found to be correlated with cancer site,
3520 CANCER Supplement December 15, 2008 / Volume 113 / Number 12
TABLE
1Stud
iesof
Older
Can
cerSu
rvivor
sDiagn
osed
Withinth
ePa
stYe
ar(N
oCom
pariso
nSa
mple)
Stud
ySa
mple
Timeframe
Out
comes
Cov
ariates
Results
Given
etal
2000
8New
lydiag
nosedbrea
st,
colon,
lung
,and
pros
tate
canc
er;
N590
7;alla
ged�6
5y
6-8,
12-16,
26-30,
and52
wkafterdiag
nosis
SF-36ph
ysical
func
tion
subs
cale
No.
ofco
morbid
cond
ition
s,ca
ncer
site,
andsex
Physical
func
tionim
prov
edov
ertim
e;pred
ictors
ofworse
physical
func
tion:
site,a
ge,fem
alesex,
comorbidity,a
ndsymptom
s.
Stom
mel
etal
2004
9Sa
mesampleas
Given
etal
2000
8Dep
ressive
symptom
atolog
y
(CES
D)
Sex,
marita
lstatus,
educ
ation,
race
/
ethn
icity
,can
cersite,
stag
e,co
morbiditie
s,
physical
func
tion,
and
symptom
s
Dep
ressivesymptom
atolog
yde
clined
over
time;
pred
ictors:c
ance
r
site,s
tage
,com
orbiditie
s,ed
ucation,
physical
func
tioning
,and
symptom
seve
rity;a
gewas
NS.
Gan
zet
al20
0310
New
lydiag
nosedbrea
st
canc
er;N
569
1;ag
ed
65-69y,
70-74y,
and
�80y
3,6,
and15
mon
thsafter
surgery
SF-36ph
ysical
func
tion
andmen
talh
ealth
;
CAR
ES-SFca
ncer-
spec
ificps
ycho
social
summary,
med
ical
interaction,
andself-
ratedhe
alth
Baselin
eQOL,
social
supp
ort,marita
lstatus,
educ
ation,
no.o
f
comorbidco
ndition
s,
type
ofsu
rgery,
trea
tmen
t,ethn
icity
,
Med
icaid,
anddisease
stag
e
Physical
func
tionde
clined
over
time;
pred
ictors:n
o.of
comorbid
cond
ition
s,ch
emothe
rapy
,Med
icaid,
BCSwith
outradiation.
Men
talh
ealth
declined
over
time(smalla
mou
nt);pred
ictors:n
o.
ofco
morbidco
ndition
s,Med
icaid,
andmarried
.CAR
ES
psyc
hoso
cial
scoreim
prov
edov
ertim
e;pred
ictors:s
ocials
uppo
rt
andbe
tter
interactionwith
healthca
reprov
iders.
Perceive
dhe
alth
at15
mo;
pred
ictors:b
aselineph
ysical
func
tion,
men
talh
ealth
,
andso
cial
supp
ort.Ag
eno
trelatedto
anyou
tcom
e.Note:
low
resp
onse
rate
(50%
).
Vino
kuret
al19
9014
Brea
stca
ncer;N
527
4;
stag
esIan
dII;a
ged
<60
yan
d�6
0y
4moan
d10
moafter
diag
nosis
Men
talh
ealth
(man
y
mea
sures)
physical
func
tion
Youn
gerag
erelatedto
worse
men
talh
ealth
;older
ageexac
erba
ted
impa
ctof
moreextens
ivesu
rgeryon
symptom
s.
Wen
zele
tal
1999
15Br
east
canc
er;s
tage
sI,II,
andIIIA;a
ged�5
0y
(n516
1),a
ged>50
y
(n514
3);N
530
4
<2moaftertrea
tmen
tFA
CT,
CES
D,s
exua
l
func
tioning
Trea
tmen
t
(che
mothe
rapy
,
reco
nstruc
tion)
Youn
gerpa
tientsrepo
rted
sign
ifica
ntly
worse
emotiona
lwell-be
ing,
brea
stca
ncer
conc
erns
,globa
lQOL,
andde
pression
.Noag
e
diffe
renc
eno
tedin
physical
orfunc
tiona
lwell-be
ing,
sexu
al
func
tioning
.
Mor
etal
1994
13New
lydiag
nosedbrea
st
canc
erpa
tients;
aged
24-54y(n514
3),a
ged
�55y(n511
9)
Beginn
ingch
emothe
rapy
orradiation
SF-36MHI-5
Dem
ograph
ics,
extent
of
disease,
trea
tmen
t,
social
supp
ort
Youn
gerpa
tientsrepo
rted
lower
emotiona
lwell-be
ing.
Other
pred
ictors:�
high
scho
oled
ucation,
symptom
s,an
dlower
social
supp
ort.
King
etal
2000
12Ea
rly-stag
ebrea
stca
ncer;
aged
25-39y(n529
),
aged
40-49y(n586
),
aged
50-59y(n593
),
ages
60-81y(n595
)
3moan
d12
moafter
surgery
EORT
CQLQ
-C30
Educ
ationan
dmarita
l
status
Older
patie
ntsrepo
rted
better
social,e
motiona
lfun
ctioning
,less
pain,few
ersymptom
s,bu
tworse
physical
func
tioning
.
SF-36indica
tesMed
ical
Outco
mes
Stud
y36
-item
ShortFo
rm;C
ESD,C
enterforEp
idem
iologica
lStudies-D
epressionSc
ale;
NS,
notsign
ifica
nt;C
ARES
-SF,
Canc
erRe
habilitation
Evalua
tion
System
,Sho
rtFo
rm;Q
OL,
quality
oflife;
BCS,
brea
stco
nserva
tionsu
rgery;
FACT
,Fun
c-
tiona
lAssessm
ento
fCan
cerTh
erap
y;MHI-5,
Men
talH
ealth
Inve
ntory;
EORT
CQLQ
-C30
,Europ
eanOrgan
izationforRe
search
andTrea
tmen
tofC
ance
rqu
ality
oflifequ
estio
nnaire.
Cancer Survivorship and Aging/Avis and Deimling 3521
stage, physical functioning, and symptom severity.
Age was found to be related to worse physical func-
tion in the study by Given et al,8,9 but was unrelated
to outcomes in the report by Ganz et al.10
Several studies have compared older and
younger cancer survivors (Table 1). By using various
outcome measures, these studies consistently found
greater psychologic morbidity among younger cancer
patients compared with older survivors.11–15 Possible
explanations for this include cancer being an off-
time event for younger women (most of these studies
focused on breast cancer patients) and younger
women having more family responsibilities, greater
interference with work, more concerns about the
impact of treatment on fertility, and fewer coping or
financial resources.13 Although older cancer patients
may experience less psychologic effects of cancer
than younger survivors, older patients report worse
physical functioning.11,14,16 Despite the consistency
of findings, these studies were limited by the lack of
adjustment for age-related differences in treatment.
It is well established that younger cancer patients
receive more aggressive cancer treatments, which
could have a negative impact on their functioning.17
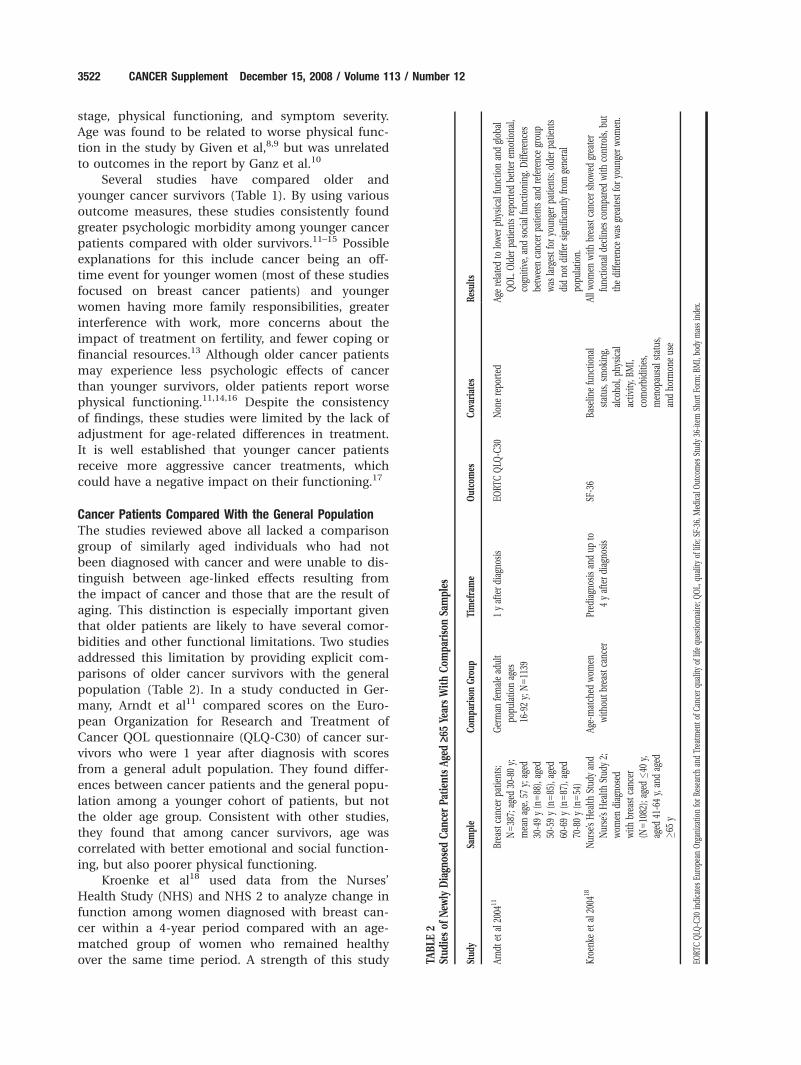
Cancer Patients Compared With the General PopulationThe studies reviewed above all lacked a comparison
group of similarly aged individuals who had not
been diagnosed with cancer and were unable to dis-
tinguish between age-linked effects resulting from
the impact of cancer and those that are the result of
aging. This distinction is especially important given
that older patients are likely to have several comor-
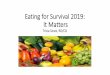
bidities and other functional limitations. Two studies
addressed this limitation by providing explicit com-
parisons of older cancer survivors with the general
population (Table 2). In a study conducted in Ger-
many, Arndt et al11 compared scores on the Euro-
pean Organization for Research and Treatment of
Cancer QOL questionnaire (QLQ-C30) of cancer sur-
vivors who were 1 year after diagnosis with scores
from a general adult population. They found differ-
ences between cancer patients and the general popu-
lation among a younger cohort of patients, but not
the older age group. Consistent with other studies,
they found that among cancer survivors, age was
correlated with better emotional and social function-
ing, but also poorer physical functioning.
Kroenke et al18 used data from the Nurses’
Health Study (NHS) and NHS 2 to analyze change in
function among women diagnosed with breast can-
cer within a 4-year period compared with an age-
matched group of women who remained healthy
over the same time period. A strength of this study TABLE
2Stud
iesof
New
lyDiagn
osed
Can
cerPa
tien
tsAge
d‡6
5Ye
arsWithCom
pariso
nSa
mples
Stud
ySa
mple
Com
pariso
nGro
upTimeframe
Out
comes
Cov
ariates
Results
Arnd
tet
al20
0411
Brea
stca
ncer
patie
nts;
N538
7;ag
ed30
-80y;
mea
nag
e,57
y;ag
ed
30-49y(n588
),ag
ed
50-59y(n585
),ag
ed
60-69y(n587
),ag
ed
70-80y(n554
)
German
femalead
ult
popu
latio
nag
es
16-92y;
N511
39
1yafterdiag
nosis
EORT
CQLQ
-C30
Non
erepo
rted
Agerelatedto
lower
physical
func
tionan
dglob
al
QOL.
Older
patie
ntsrepo
rted
better
emotiona
l,
cogn
itive
,and
social
func
tioning
.Differen
ces
betw
eenca
ncer
patie
ntsan
dreferenc
egrou
p
was
largestforyo
unge
rpa
tients;
olde
rpa
tients
didno
tdiffe
rsign
ifica
ntly
from
gene
ral
popu
latio
n.
Kroe
nkeet
al20
0418
Nurse’sHea
lthStud
yan
d
Nurse’sHea
lthStud
y2;
wom
endiag
nosed
with
brea
stca
ncer
(N510
82);ag
ed�4
0y,
aged
41-64y,
andag
ed
�65y
Age-match
edwom
en
with
outbrea
stca
ncer
Pred
iagn
osis
andup
to
4yafterdiag
nosis
SF-36
Baselin
efunc
tiona
l
status
,smok
ing,
alco
hol,ph
ysical
activ
ity,B
MI,
comorbiditie
s,
men
opau
sals
tatus,
andho
rmon
eus
e
Allw
omen
with
brea
stca
ncer
show
edgrea
ter
func
tiona
ldec
lines
compa
redwith
controls,b
ut
thediffe
renc
ewas
grea
test
foryo
unge
rwom
en.
EORT
CQLQ
-C30
indica
tesEu
rope
anOrgan
izationforRe
search
andTrea
tmen
tofC
ance
rqu
ality
oflifequ
estio
nnaire;Q
OL,
quality
oflife;
SF-36,
Med
ical
Outco
mes
Stud
y36
-item
ShortF
orm;B
MI,bo
dymassinde
x.
3522 CANCER Supplement December 15, 2008 / Volume 113 / Number 12

was the availability of SF-36 scores before diagnosis,
which enabled researchers to compare change in SF-
36 scores from before to after diagnosis. Controlling
for baseline functional status, smoking, alcohol,
physical activity, body mass index, comorbidities,
menopausal status, and hormone use, they found
that all women with breast cancer demonstrated
greater functional declines than the controls. How-
ever, young women who developed breast cancer
demonstrated greater absolute and relative functional
losses in physical role function, bodily pain, social
function, and mental health compared with middle-
aged or older women with breast cancer. Results
showed substantial physical declines in older women
both with and without breast cancer, suggesting that
much of this decline is related to age, rather than
disease or treatment. This research highlights the im-
portance of obtaining functional measures before
treatment.
SummaryTaken as a whole, research on newly diagnosed older
cancer patients suggests that for older cancer survi-
vors, cancer affects physical functioning more than
psychologic functioning. Whereas older cancer
patients may demonstrate some psychologic impact
of cancer, this tends to be relatively short-lived and
less detrimental than for younger patients. Although
several hypotheses have been put forward as to why
younger cancer survivors have greater psychologic
morbidity, these hypotheses need to be explored fur-
ther and tested. Conversely, older cancer patients
may be more affected by cancer in terms of physical
function. The presence of comorbidities is especially
important and needs to be considered in any study
of older cancer survivors.
Studies of Long-term Cancer SurvivorsThis section focuses specifically on the physical and
psychosocial QOL of older-adult long-term survivors
of cancer (�5 years). The diversity of older adults
included in these studies in terms of age at diagno-
sis, current age, and length of survivorship makes
this literature difficult to synthesize. Studies often
include individuals who range from ages 60 years to
90 years at the time of the study, but may have sur-
vived cancer for �25 years. This results in the inclu-
sion of very different survivor subgroups. As in the
previous section, studies of long-term cancer survi-
vors can be categorized as: 1) those that include only
cancer survivors and 2) those that compare cancer
survivors to those without cancer. We reviewed each
category separately.
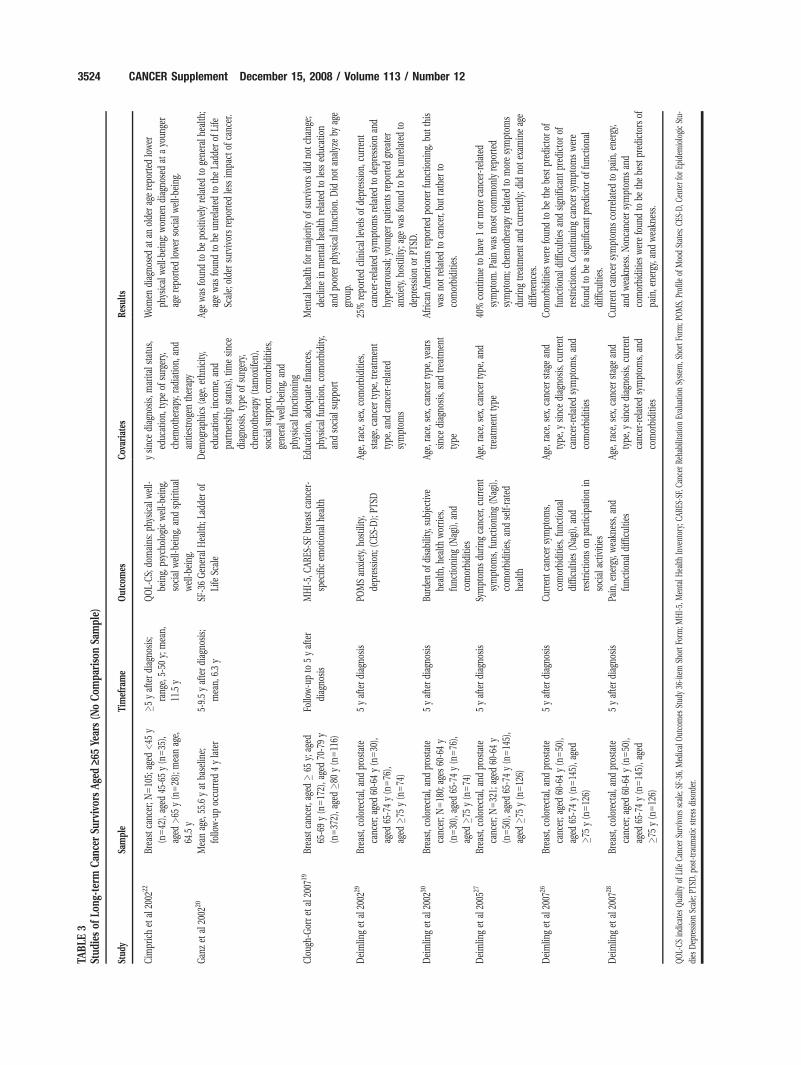
Older adult long-term survivors only (no comparison group)Many of the long-term survivorship studies that
included older adults did not include a comparison
group of similarly aged individuals without a history
of cancer. As with other studies of survivors, the ma-
jority focused on breast cancer survivors. Our review
(Table 3) reflects this pattern.
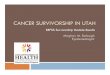
In a study of 316 breast cancer survivors aged
>65 years who were followed for 5 years after diag-
nosis, Clough-Gorr et al19 reported that mental
health did not change for the majority of survivors.
Those survivors who did demonstrate a decline in
mental health had poorer physical function at base-
line. Ganz et al20 found that age was positively
related to general health, and that older breast can-
cer survivors reported less of an impact of cancer on
their lives, a finding also reported by Stava et al.21
Cimprich et al22 compared long-term (�5 years)
breast cancer survivors diagnosed at different ages
(<45 years, 45 to 64 years, and �65 years) and found
that survivors diagnosed at an older age (aged �65
years) reported significantly poorer QOL in the physi-
cal domain, whereas those diagnosed at a younger
age (aged <45 years) demonstrated worse QOL in
the social domain.
Two groups of researchers have conducted stu-
dies focusing on long-term survivors of multiple
types of cancers. Avis et al23,24 studied 242 long-term
(�5 years) survivors of breast, bladder, prostate, col-
orectal, head and neck, or gynecologic cancer.
Approximately Eighty-five percent of this sample was
aged >60 years, and 65% was aged >70 years. The
mean time since diagnosis was 12.6 years. This study
was conducted in the context of developing a QOL
instrument specific to adult cancer survivors, the
Quality of Life in Adult Cancer Survivors (QLACS)
scale. The biggest problems cited by survivors were
sexual problems, fatigue, and family-related concerns
surrounding disease recurrence.23 QOL varied by
cancer site, with prostate and colorectal cancer survi-
vors reporting the best QOL and head and neck and
bladder cancer survivors the worst QOL.
Deimling et al25–30 also conducted a study of
long-term breast, colorectal, and prostate survivors
that specifically examined QOL issues. They studied
321 survivors aged >60 years who were at least 5
years after diagnosis. Their results demonstrated that
nearly 40% of older survivors had at least 1 continu-
ing symptom attributed to cancer or its treatment.
Survivors who had chemotherapy and/or more types
of treatment reported significantly more symptoms
both during treatment and currently. Being African
American or female was found to be significantly
associated with more current symptoms and greater
Cancer Survivorship and Aging/Avis and Deimling 3523
TABLE
3Stud
iesof
Long
-term
Can
cerSu
rvivor
sAge
d‡6
5Ye
ars(N
oCom
pariso
nSa
mple)
Stud
ySa
mple
Timeframe
Out
comes
Cov
ariates
Results
Cim
prichet
al20
0222
Brea
stca
ncer;N
510
5;ag
ed<45
y
(n542
),ag
ed45
-65y(n535
),
aged
>65
y(n528
);mea
nag
e,
64.5
y
�5yafterdiag
nosis;
rang
e,5-50
y;mea
n,
11.5
y
QOL-CS;
domains
:phy
sica
lwell-
being,
psyc
hologicwell-be
ing,
social
well-be
ing,
andsp
iritu
al
well-be
ing.
ysinc
ediag
nosis,
marita
lstatus,
educ
ation,
type
ofsu
rgery,
chem
othe
rapy
,rad
iatio
n,an
d
antie
stroge
ntherap
y
Wom
endiag
nosedat
anolde
rag
erepo
rted
lower
physical
well-be
ing;
wom
endiag
nosedat
ayo
unge
r
agerepo
rted
lower
social
well-be
ing.
Gan
zet
al20
0220
Mea
nag
e,55
.6yat
baselin
e;
follo
w-upoc
curred
4ylater
5-9.5yafterdiag
nosis;
mea
n,6.3y
SF-36Gen
eral
Hea
lth;L
adde
rof
Life
Scale
Dem
ograph
ics(age
,ethnicity,
educ
ation,
inco
me,
and
partne
rshipstatus
),tim
esinc
e
diag
nosis,
type
ofsu
rgery,
chem
othe
rapy
(tam
oxife
n),
social
supp
ort,co
morbiditie
s,
gene
ralw
ell-be
ing,
and
physical
func
tioning
Agewas
foun
dto
bepo
sitiv
elyrelatedto
gene
ralh
ealth
;
agewas
foun
dto
beun
relatedto
theLa
dder
ofLife
Scale;
olde
rsu
rvivorsrepo
rted
less
impa
ctof
canc
er.
Cloug
h-Gorret
al20
0719
Brea
stca
ncer,a
ged�
65y;
aged
65-69y(n517
2),a
ged70
-79y
(n537
2),a
ged�8
0y(n511
6)
Follo
w-upto
5yafter
diag
nosis
MHI-5,
CAR
ES-SFbrea
stca
ncer-
spec
ificem
otiona
lhea
lth
Educ
ation,
adeq
uate
finan
ces,
physical
func
tion,
comorbidity,
andso
cial
supp
ort
Men
talh
ealth
formajority
ofsu
rvivorsdidno
tch
ange
;
declinein
men
talh
ealth
relatedto
less
educ
ation
andpo
orer
physical
func
tion.
Did
notan
alyzeby
age
grou
p.
Deimlin
get
al20
0229
Brea
st,c
olorec
tal,an
dpros
tate
canc
er;a
ged60
-64y(n530
),
aged
65-74y(n576
),
aged
�75y(n574
)
5yafterdiag
nosis
POMSan
xiety,
hostility,
depression
;(CES
-D);PT
SD
Age,
race
,sex,c
omorbiditie
s,
stag
e,ca
ncer
type
,treatmen
t
type
,and
canc
er-related
symptom
s
25%
repo
rted
clinical
leve
lsof
depression
,current
canc
er-related
symptom
srelatedto
depression
and
hype
rarous
al;y
oung
erpa
tientsrepo
rted
grea
ter
anxiety,
hostility;a
gewas
foun
dto
beun
relatedto
depression
orPT
SD.
Deimlin
get
al20
0230
Brea
st,c
olorec
tal,an
dpros
tate
canc
er;N
518
0;ag
es60
-64y
(n530
),ag
ed65
-74y(n576
),
aged
�75y(n574
)
5yafterdiag
nosis
Burden
ofdisability,
subjec
tive
health,h
ealth
worries,
func
tioning
(Nag
i),an
d
comorbiditie
s
Age,
race
,sex,c
ance
rtype
,yea
rs
sinc
ediag
nosis,
andtrea
tmen
t
type
Africa
nAm
erican
srepo
rted
poorer
func
tioning
,but
this
was
notrelatedto
canc
er,b
utrather
to
comorbiditie
s.
Deimlin
get
al20
0527
Brea
st,c
olorec
tal,an
dpros
tate
canc
er;N
532
1;ag
ed60
-64y
(n550
),ag
ed65
-74y(n514
5),
aged
�75y(n512
6)
5yafterdiag
nosis
Symptom
sdu
ring
canc
er,c
urrent
symptom
s,func
tioning
(Nag
i),
comorbiditie
s,an
dself-rated
health
Age,
race
,sex,c
ance
rtype
,and
trea
tmen
ttype
40%
continue
toha
ve1or
moreca
ncer-related
symptom
.Painwas
mos
tco
mmon
lyrepo
rted
symptom
;che
mothe
rapy
relatedto
moresymptom
s
during
trea
tmen
tan
dcu
rren
tly;d
idno
texam
ineag
e
diffe
renc
es.
Deimlin
get
al20
0726
Brea
st,c
olorec
tal,an
dpros
tate
canc
er;a
ged60
-64y(n550
),
aged
65-74y(n514
5),a
ged
�75y(n512
6)
5yafterdiag
nosis
Current
canc
ersymptom
s,
comorbiditie
s,func
tiona
l
difficu
lties
(Nag
i),an
d
restrictions
onpa
rticipationin
social
activ
ities
Age,
race
,sex,c
ance
rstag
ean
d
type
,ysinc
ediag
nosis,
curren
t
canc
er-related
symptom
s,an
d
comorbiditie
s
Com
orbiditie
swerefoun
dto
bethebe
stpred
ictorof
func
tiona
ldifficultie
san
dsign
ifica
ntpred
ictorof
restrictions
.Con
tinuing
canc
ersymptom
swere
foun
dto
beasign
ifica
ntpred
ictorof
func
tiona
l
difficu
lties.
Deimlin
get
al20
0728
Brea
st,c
olorec
tal,an
dpros
tate
canc
er;a
ged60
-64y(n550
),
aged
65-74y(n514
5),a
ged
�75y(n512
6)
5yafterdiag
nosis
Pain,e
nergy,
wea
kness,
and
func
tiona
ldifficultie
s
Age,
race
,sex,c
ance
rstag
ean
d
type
,ysinc
ediag
nosis,
curren
t
canc
er-related
symptom
s,an
d
comorbiditie
s
Current
canc
ersymptom
sco
rrelated
topa
in,e
nergy,
andwea
kness.
Non
canc
ersymptom
san
d
comorbiditie
swerefoun
dto
bethebe
stpred
ictors
of
pain,e
nergy,
andwea
kness.
QOL-CS
indica
tesQua
lityof
Life
Canc
erSu
rvivorsscale;
SF-36,
Med
ical
Outco
mes
Stud
y36
-item
ShortFo
rm;M
HI-5,
Men
talH
ealth
Inve
ntory;
CARE
S-SF,C
ance
rRe
habilitationEv
alua
tionSy
stem
,Sho
rtFo
rm;P
OMS,
Profile
ofMoo
dStates;C
ES-D
,Cen
terforEp
idem
iologicStu-
dies
Dep
ressionSc
ale;
PTSD
,pos
t-trau
matic
stress
diso
rder.
3524 CANCER Supplement December 15, 2008 / Volume 113 / Number 12

functional difficulty, but this was related to having
more comorbidities and not to cancer-related factors
such as cancer stage at diagnosis or treatment com-
plexity.
In terms of specific symptoms, pain was the
most commonly reported symptom, with 21% attri-
buting this current symptom to their past cancer or
its treatment.27 Although cancer-related factors were
significant correlates of pain, comorbidities and non-
cancer symptoms were stronger correlates. Greater
than 40% of breast cancer survivors and nearly 20%
of prostate cancer survivors reported pain, with breast
cancer survivors reporting the highest levels of pain.
Race was also a significant correlate of pain, with Afri-
can–American women having the highest scores.
Greater than 40% of survivors reported feeling
weakness or lack of energy within the past week,26
with approximately 25% attributing it to cancer.
However, as with other symptoms, the lack of energy
and weakness reported by these older adult survivors
was found to be more strongly related to age-related
factors such as the number of other health problems
rather than cancer.
This study also found important psychosocial
outcomes of cancer. Nearly half of the older adult
long-term survivors reported a range of cancer-
related worries such as fears of disease recurrence,
fears of a new cancer, and fears that symptoms they
experience may represent cancer. Furthermore, these
fears were correlated with the number of cancer-
related symptoms experienced during treatment as
well as current cancer-related or treatment-related
symptoms. Importantly, cancer-related worries were
found to be significant predictors of more general
levels of distress such as anxiety and depression.
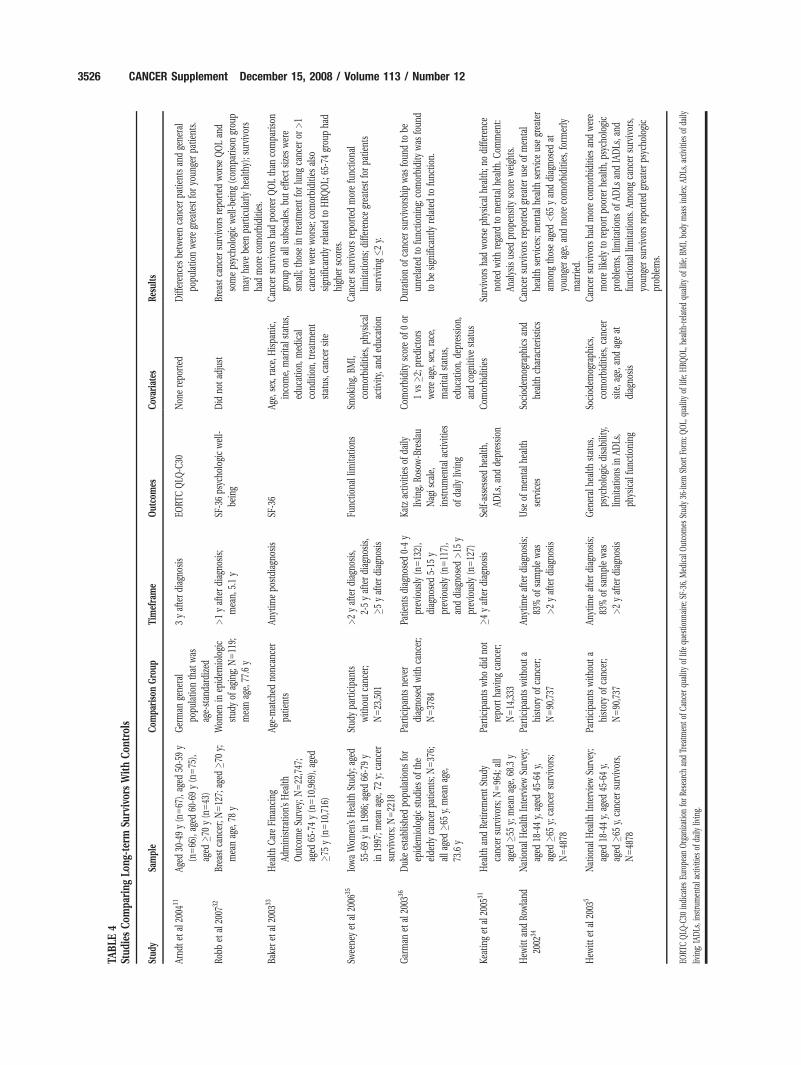
Comparison of long-term survivors to those without acancer historyMost of the long-term physical and mental effects of
cancer reported above are from studies that included
only cancer survivors. To fully understand the impact
of cancer on older persons, it is important to compare
long-term survivors with individuals who have never
had cancer. These studies are presented in Table 4.
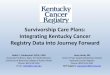
In a study focusing specifically on older adult,
long-term survivors from the Health and Retirement
study, Keating et al31 compared cancer survivors with
a population-based noncancer comparison group
from this same study. Cancer survivors had higher
rates of specific comorbidities such as lung disease,
heart disease, arthritis, incontinence, frequent pain,
and obesity compared with controls. Controlling for
these comorbidities, survivors were still less likely to
report being in excellent health and had more mobil-
ity and activity limitations than those without a his-
tory of cancer. Older long-term cancer survivors did
not exhibit more psychiatric disease or depression,
nor did they exhibit poorer cognitive functioning
compared with those who never had cancer.
Robb et al32 compared SF-36 scores and meas-
ures of psychologic well-being from a sample of
older-adult breast cancer survivors aged �70 years
with the scores of women who had never had cancer.
Their analysis found that cancer survivors reported
poorer physical functioning, bodily pain, more days
per week with fatigue, and worse psychologic well-
being than the comparison group. However, the
comparison group was a sample of women enrolled
in a longitudinal study of healthy aging, and there-
fore may have been particularly healthy.
Using data from the large Health Outcomes
Study, Baker et al33 compared SF-36 scores between
those participants who had a history of cancer with
age-matched participants who did not. They found
that cancer survivors had poorer QOL on all sub-
scales of the SF-36, but the effect sizes were small.
Those who were currently in treatment for lung can-
cer or had >1 cancer were worse off. Comorbidities
were found to be significantly related to health–
related QOL. In what to our knowledge was 1 of the
few studies that further broke down the group of
patients aged >65 years, they found that the patients
ages 65 years to 74 years reported better QOL than
those who were aged >75 years.
Hewitt et al5,34 used data from the National
Health Interview Survey to compare participants
with a history of cancer with those without such a
history. Analyses included survivors ranging from <2
years to those who had survived >20 years. Cancer
survivors had more comorbidities and were more
likely to report poorer overall health and limitations
in activities of daily living. Survivors reported greater
use of mental health services in general; this was
noted particularly for younger women, who also
reported greater psychologic problems. Although
these analyses include both short-term and long-
term survivors, 83% of the sample had been diag-
nosed >2 years previously.
Two studies were able to take advantage of exist-
ing large cohorts in which data were available before
a cancer diagnosis. Sweeney et al35 compared the
functional limitations of female older–adult cancer
survivors (ages 66 years-79 years) from the Iowa
Women’s Health Study with study participants who
had never had cancer. Controlling for baseline char-
acteristics (obesity, smoking, and diabetes) and
comorbidities, they found that 5-year survivors, com-
pared with those without a cancer history, were sig-
Cancer Survivorship and Aging/Avis and Deimling 3525
TABLE
4Stud
iesCom
paring
Long
-term
Survivor
sWithCon
trols
Stud
ySa
mple
Com
pariso
nGro
upTimeframe
Out
comes
Cov
ariates
Results
Arnd
tet
al20
0411
Aged
30-49y(n567
),ag
ed50
-59y
(n566
),ag
ed60
-69y(n575
),
aged
�70y(n543
)
German
gene
ral
popu
latio
nthat
was
age-stan
dardized
3yafterdiag
nosis
EORT
CQLQ
-C30
Non
erepo
rted
Differen
cesbe
twee
nca
ncer
patie
ntsan
dge
neral
popu
latio
nweregrea
test
foryo
unge
rpa
tients.
Robb
etal
2007
32Br
east
canc
er;N
512
7;ag
ed�7
0y;
mea
nag
e,78
y
Wom
enin
epidem
iologic
stud
yof
aging;
N511
9;
mea
nag
e,77
.6y
>1yafterdiag
nosis;
mea
n,5.1y
SF-36ps
ycho
logicwell-
being
Did
notad
just
Brea
stca
ncer
survivorsrepo
rted
worse
QOLan
d
someps
ycho
logicwell-be
ing(com
pariso
ngrou
p
may
have
been
particularly
healthy);s
urvivo
rs
hadmoreco
morbiditie
s.
Bake
ret
al20
0333
Hea
lthCareFina
ncing
Administration’sHea
lth
Outco
meSu
rvey
;N522
,747
;
aged
65-74y(n510
,969
),ag
ed
�75y(n510
,716
)
Age-match
edno
ncan
cer
patie
nts
Anytim
epo
stdiag
nosis
SF-36
Age,
sex,
race
,Hispa
nic,
inco
me,
marita
lstatus,
educ
ation,
med
ical
cond
ition
,treatmen
t
status
,can
cersite
Can
cersu
rvivorsha
dpo
orer
QOLthan
compa
riso
n
grou
pon
alls
ubscales,b
uteffect
sizeswere
small;thos
ein
trea
tmen
tforlung
canc
eror
>1
canc
erwereworse;c
omorbiditie
salso
sign
ifica
ntly
relatedto
HRQ
OL;
65-74grou
pha
d
high
erscores.
Swee
neyet
al20
0635
IowaWom
en’sHea
lthStud
y;ag
ed
55-69yin
1986
;age
d66
-79y
in19
97;m
eanag
e,72
y;ca
ncer
survivors;
N522
18
Stud
ypa
rticipan
ts
with
outca
ncer;
N523
,501
>2yafterdiag
nosis,
2-5yafterdiag
nosis,
�5yafterdiag
nosis
Func
tiona
llim
itatio
nsSm
oking,
BMI,
comorbiditie
s,ph
ysical
activ
ity,a
nded
ucation
Can
cersu
rvivorsrepo
rted
morefunc
tiona
l
limita
tions
;differen
cegrea
test
forpa
tients
surviving�2
y.
Garman
etal
2003
36Duk
eestablishe
dpo
pulatio
nsfor
epidem
iologicstud
iesof
the
elde
rlyca
ncer
patie
nts;
N537
6;
alla
ged�6
5y,
mea
nag
e,
73.6
y
Participan
tsne
ver
diag
nosedwith
canc
er;
N537
84
Patie
ntsdiag
nosed0-4y
prev
ious
ly(n513
2),
diag
nosed5-15
y
prev
ious
ly(n511
7),
anddiag
nosed>15
y
prev
ious
ly(n512
7)
Katz
activ
ities
ofda
ily
living,
Rosow-B
reslau
Nag
isca
le,
instrumen
tala
ctivities
ofda
ilyliv
ing
Com
orbidity
scoreof
0or
1vs
�2;p
redictors
wereag
e,sex,
race,
marita
lstatus,
educ
ation,
depression
,
andco
gnitive
status
Durationof
canc
ersu
rvivorsh
ipwas
foun
dto
be
unrelatedto
func
tioning
;com
orbidity
was
foun
d
tobe
sign
ifica
ntly
relatedto
func
tion.
Keatinget
al20
0531
Hea
lthan
dRe
tirem
entStud
y
canc
ersu
rvivors;
N596
4;all
aged
�55y;
mea
nag
e,68
.3y
Participan
tswho
didno
t
repo
rtha
ving
canc
er;
N514
,333
�4yafterdiag
nosis
Self-assessed
health,
ADLs
,and
depression
Com
orbiditie
sSu
rvivorsha
dworse
physical
health;n
odiffe
renc
e
notedwith
rega
rdto
men
talh
ealth
.Com
men
t:
Analysis
used
prop
ensity
scoreweigh
ts.
Hew
ittan
dRo
wland
2002
34Nationa
lHea
lthInterview
Survey
;
aged
18-44y,
aged
45-64y,
aged
�65y;
canc
ersu
rvivors;
N548
78
Participan
tswith
outa
historyof
canc
er;
N590
,737
Anytim
eafterdiag
nosis;
83%
ofsamplewas
>2yafterdiag
nosis
Use
ofmen
talh
ealth
services
Sociod
emog
raph
icsan
d
health
charac
teristics
Can
cersu
rvivorsrepo
rted
grea
terus
eof
men
tal
health
services;m
entalh
ealth
serviceus
egrea
ter
amon
gthos
eag
ed<65
yan
ddiag
nosedat
youn
gerag
e,an
dmoreco
morbiditie
s,form
erly
married
.
Hew
ittet
al20
035
Nationa
lHea
lthInterview
Survey
;
aged
18-44y,
aged
45-64y,
aged
�65y,
canc
ersu
rvivors,
N548
78
Participan
tswith
outa
historyof
canc
er;
N590
,737
Anytim
eafterdiag
nosis;
83%
ofsamplewas
>2yafterdiag
nosis
Gen
eral
health
status
,
psyc
hologicdisability,
limita
tions
inAD
Ls,
physical
func
tioning
Sociod
emog
raph
ics,
comorbiditie
s,ca
ncer
site,a
ge,a
ndag
eat
diag
nosis
Can
cersu
rvivorsha
dmoreco
morbiditie
san
dwere
morelik
elyto
repo
rtpo
orer
health,p
sych
olog
ic
prob
lems,
limita
tions
ofAD
Lsan
dIADLs
,and
func
tiona
llim
itatio
ns.A
mon
gca
ncer
survivors,
youn
gersu
rvivorsrepo
rted
grea
terps
ycho
logic
prob
lems.
EORT
CQLQ
-C30
indica
tesEu
rope
anOrgan
izationforRe
search
andTrea
tmen
tofC
ance
rqu
ality
oflifequ
estio
nnaire;S
F-36
,Med
ical
Outco
mes
Stud
y36
-item
ShortF
orm;Q
OL,
quality
oflife;
HRQ
OL,
health-related
quality
oflife;
BMI,bo
dymassinde
x;AD
Ls,a
ctivities
ofda
ily
living;
IADLs
,ins
trum
entala
ctivities
ofda
ilyliv
ing.
3526 CANCER Supplement December 15, 2008 / Volume 113 / Number 12

nificantly more likely to report functional limitations
such as an inability to do housework, walk a half
mile, or walk up/down stairs. Using data from the
Duke Established Populations for Epidemiologic stu-
dies of the Elderly, Garman at al36 found that func-
tion decline was significantly correlated with the
presence of comorbidities rather than cancer per se
among participants aged �65 years.
SummaryThe research regarding long-term cancer survivors is
noteworthy for the consistency of findings that can-
cer survivors have more comorbidities and poorer
functioning (independent of comorbidities) than
noncancer survivors. The consistency of this research
is in contrast to that of newly diagnosed older
patients, in whom the effects of cancer due to age
are not as apparent. It thus appears that age-related
differences may arise over time. This may be the
result of the late effects of cancer and its treatment,
consequences of underlying risk factors for cancer
(eg, smoking and diet), or the interaction of cancer
and aging. This highlights the importance of studying
the late effects of cancer and developing interven-
tions to prevent loss of functioning with age.
Summary and Future Research DirectionsThe literature suggests that older cancer survivors
are likely to be more affected by cancer in terms of
physical compared with psychologic function. Physi-
cal domains also may be more important to older
persons, for whom impairments in mobility may
mean the difference between independent and
assisted living. The literature has consistently shown
that older breast cancer survivors are less likely to
have psychologic morbidity than younger survivors.
However, comparisons with noncancer patients in
some studies suggest that older cancer survivors may
be faring worse psychologically than noncancer sur-
vivors. In the context of older cancer survivors, it is
important to consider the impact of an acute cancer
episode on a background of other chronic conditions
and deterioration in physical functioning that is part
of normal aging. To our knowledge, very few studies
to date have measures of functioning before a cancer
diagnosis and treatment, thus making it difficult to
determine the direct impact of cancer.
Limitations of ResearchThe majority of studies reviewed herein focused on
breast cancer survivors. This is largely a result of the
large numbers of long-term breast cancer survivors.
However, the extent to which these findings can be
generalized to men, cancers that progress more
quickly, and cancers with different patterns of treat-
ment is unknown. Another limitation is that most
studies do not report effect sizes, which is particu-
larly important for some of the studies that deter-
mined statistical significance with large sample sizes.
Studies comparing older and younger cancer sur-
vivors do not take treatment characteristics beyond
type of surgery or adjuvant therapy into account.
This is an important consideration because older per-
sons tend to receive less aggressive treatment because
of the greater likelihood of estrogen receptor–positive
tumors, the presence of comorbid conditions, and
lower functional status,17 and more aggressive treat-
ment may impact QOL. To truly understand the impact
of age on cancer survivorship, it is important to control
for type of treatment received.
Although many studies control for comorbidities,
others do not. The long-term effects of cancers that
are common among older adults often coexist along
with other health problems associated with aging.
Thus, older adults may experience this dual vulner-
ability. Over a decade ago, Havlik et al37 identified
comorbidities as a significant issue among cancer
survivors and found them to increase with advancing
age. Recently, others have also identified the pre-
sence of comorbidities among older survivors as 1 of
the key issues to be addressed by research on cancer
and aging.38
Finally, it should be noted that few articles report
effect sizes, but in those that do, the effect size is of-
ten modest. This is noted especially in studies with
large sample sizes, in which small effects can be sta-
tistically significant.
The following approaches to futureresearch are suggested:
� Any study of older cancer survivors needs to con-
sider comorbidities and their interaction with a
cancer diagnosis. As observed in the studies
described herein, comorbidities are important
determinants of QOL.
� Comparisons with age-matched noncancer popula-
tions are critical for understanding the impact of
cancer on older persons. These comparisons are
particularly important in the context of other func-
tional declines that occur with aging and are not
attributable to cancer.
� Prospective studies that measure physical and
mental health functioning before treatment are
needed to assess changes in functioning resulting
from treatment.
� Age groupings of older survivors need to be broken
down further into young-old and old-old. To our
Cancer Survivorship and Aging/Avis and Deimling 3527
knowledge, the majority of research published to
date combined all survivors aged >65 years. How-
ever, some research has shown age differences
even among those aged �60 years.8,29,33 The gen-
eral gerontologic literature would recommend
separating the young-old from the old-old, because
research has shown that there are important
health, functioning, and psychosocial differences
among age groupings of older adults.
� It is important to identify subgroups of older survi-
vors at greatest risk. This may include those who
have poor functioning at the time of diagnosis, low
social support, or comorbidities. Cancer site and
type of treatment may also be important.
� Greater emphasis is needed on recruiting older
persons into clinical trials. Relatively few elderly
persons are accrued to clinical trials because of
concerns that older patients cannot tolerate or will
not benefit from treatment17or restrictive inclu-
sion/exclusion criteria.39 These criteria need to be
carefully evaluated to ensure that older persons are
not excluded unnecessarily.
� Interventions are needed to reduce the impact of
cancer on functioning. Existing behavioral inter-
ventions that have shown benefits among cancer
survivors in general need to be applied to older
patients. In some instances, this may mean adjust-
ing the modality or specifics of the intervention
(eg, exercise).
A more detailed discussion of the implications
for future research is provided in the article by Bel-
lizzi et al in this issue.40
REFERENCES1. Yancik R, Ries LA. Cancer in older persons: an interna-
tional issue in an aging world. Semin Oncol. 2004;31:128-
136.
2. American Cancer Society. Cancer Facts & Figures 2002.
Atlanta, GA: American Cancer Society; 2002.
3. Edwards BK, Howe HL, Ries LA, et al. Annual report to the
nation on the status of cancer, 1973-1999, featuring impli-
cations of age and aging on U.S. cancer burden. Cancer.
2002;94:2766-2792.
4. Yancik R. Cancer burden in the aged: an epidemiologic
and demographic overview. Cancer. 1997;80:1273-1283.
5. Hewitt M, Rowland JH, Yancik R. Cancer survivors in the
United States: age, health, and disability. J Gerontol A Biol
Sci Med Sci. 2003;58:82-91.
6. Rao AV, Demark-Wahnefried W. The older cancer survivor.
Crit Rev Oncol Hematol. 2006;60:131-143.
7. About Cancer Survivorship Research: Survivorship Defini-
tions. National Cancer Institute Office of Survivorship. Be-
thesda, MD: National Cancer Institute; 2005. Available
at http://dccps.nci.nih.gov/ocs/definitions.html. Accessed
November 6, 2006.
8. Given CW, Given B, Azzouz F, et al. Comparison of changes
in physical functioning of elderly patients with new diag-
noses of cancer. Med Care. 2000;38:482-493.
9. Stommel M, Kurtz ME, Kurtz JC, et al. A longitudinal analy-
sis of the course of depressive symptomatology in geriatric
patients with cancer of the breast, colon, lung, or prostate.
Health Psychol. 2004;23:564-573.
10. Ganz PA, Guadagnoli E, Landrum MB, et al. Breast cancer
in older women: quality of life and psychosocial adjust-
ment in the 15 months after diagnosis. J Clin Oncol.
2003;21:4027-4033.
11. Arndt V, Merx H, Sturmer T, et al. Age-specific detriments
to quality of life among breast cancer patients 1 year after
diagnosis. Eur J Cancer. 2004;40:673-680.
12. King MT, Kenny P, Shiell A, et al. Quality of life 3 months
and 1 year after first treatment for early stage breast can-
cer: influence of treatment and patient characteristics.
Qual Life Res. 2000;9:789-800.
13. Mor V, Malin M, Allen S. Age differences in the psychoso-
cial problems encountered by breast cancer patients. J Natl
Cancer Inst Monogr. 1994;(16):191-197.
14. Vinokur AD, Threatt BA, Vinokur-Kaplan D, et al. The process
of recovery from breast cancer for younger and older patients.
Changes during the first year.Cancer. 1990;65:1242-1254.
15. Wenzel LB, Fairclough DL, Brady MJ, et al. Age-related dif-
ferences in the quality of life of breast carcinoma patients
after treatment. Cancer. 1999;86:1768-1774.
16. Yancik R, Wesley MN, Ries LA, et al. Effect of age and
comorbidity in postmenopausal breast cancer patients
aged 55 years and older. JAMA. 2001;285:885-892.
17. Crivellari D, Aapro M, Leonard R, et al. Breast cancer in
the elderly. J Clin Oncol. 2007;25:1882-1890.
18. Kroenke CH, Rosner B, Chen WY, et al. Functional impact
of breast cancer by age at diagnosis. J Clin Oncol. 2004;22:
1849-1856.
19. Clough-Gorr KM, Ganz PA, Silliman RA. Older breast can-
cer survivors: factors associated with change in emotional
well-being. J Clin Oncol. 2007;25:1334-1340.
20. Ganz PA, Desmond KA, Leedham B, et al. Quality of life in
long-term, disease-free survivors of breast cancer: a follow-
up study. J Natl Cancer Inst. 2002;94:39-49.
21. Stava CJ, Lopez A, Vassilopoulou-Sellin R. Health profiles
of younger and older breast cancer survivors. Cancer. 2006;
107:1752-1759.
22. Cimprich B, Ronis DL, Martinez-Ramos G. Age at diagnosis
and quality of life in breast cancer survivors. Cancer Pract.
2002;10:85-93.
23. Avis NE, Smith KW, McGraw S, et al. Assessing quality of
life in adult cancer survivors (QLACS). Qual Life Res.
2005;14:1007-1023.
24. Avis NE, Ip E, Long FK. Evaluation of the Quality of Life in
Adult Cancer Survivors (QLACS) scale for long-term cancer
survivors in a sample of breast cancer survivors. Health
Qual Life Outcomes. 2006;4:92.
25. Deimling GT, Bowman KF, Sterns S, et al. Cancer-related
health worries and psychological distress among older
adult, long-term cancer survivors. Psychooncology. 2006;15:
306-320.
26. Deimling GT, Sterns S, Bowman KF, et al. Functioning and
activity participation restrictions among older adult, long-
term cancer survivors. Cancer Invest. 2007;25:106-116.
27. Deimling GT, Sterns S, Bowman KF, et al. The health of
older-adult, long-term cancer survivors. Cancer Nurs.
2005;28:415-424.
3528 CANCER Supplement December 15, 2008 / Volume 113 / Number 12

28. Deimling GT, Bowman KF, Wagner LJ. The effects of
cancer-related pain and fatigue on functioning of older
adult, long-term cancer survivors. Cancer Nurs. 2007;30:
421-433.
29. Deimling GT, Kahana B, Bowman KF, et al. Cancer survi-
vorship and psychological distress in later life. Psychoon-
cology. 2002;11:479-494.
30. Deimling GT, Schaefer ML, Kahana B, et al. Racial differ-
ences in the health of older adult long term cancer survi-
vors. Psychosocial Oncol. 2002;20:71-94.
31. Keating NL, Norredam M, Landrum MB, et al. Physical and
mental health status of older long-term cancer survivors.
J Am Geriatr Soc. 2005;53:2145-2152.
32. Robb C, Haley WE, Balducci L, et al. Impact of breast can-
cer survivorship on quality of life in older women. Crit Rev
Oncol Hematol. 2007;62:84-91.
33. Baker F, Haffer SC, Denniston M. Health-related quality of
life of cancer and noncancer patients in Medicare mana-
ged care. Cancer. 2003;97:674-681.
34. Hewitt M, Rowland JH. Mental health service use
among adult cancer survivors: analyses of the National
Health Interview Survey. J Clin Oncol. 2002;20:4581-
4590.
35. Sweeney C, Schmitz KH, Lazovich D, et al. Functional lim-
itations in elderly female cancer survivors. J Natl Cancer
Inst. 2006;98:521-529.
36. Garman KS, Pieper CF, Seo P, et al. Function in elderly can-
cer survivors depends on comorbidities. J Gerontol A Biol
Sci Med Sci. 2003;58:M1119-M1124.
37. Havlik RJ, Yancik R, Long S, Ries L, Edwards B. The
National Institute on Aging and the National Cancer Insti-
tute SEER collaborative study on comorbidity and early di-
agnosis of cancer in the elderly. Cancer. 1994;74(7 suppl):
2101-2106.
38. Berger N, Savvides P, Koroukian S, et al. Cancer in the
elderly. Trans Am Clin Climatol Assoc. 2006;117:147-156.
39. Lewis JH, Kilgore ML, Goldman DP, et al. Participation of
patients 65 years of age or older in cancer clinical trials.
J Clin Oncol. 2003;21:1383-1389.
40. Bellizzi KM, Mustian KM, Palesh O, Diefenbach M. Cancer
survivorship and aging: moving the science forward. Can-
cer. 2008;113 (suppl): Pages.
Cancer Survivorship and Aging/Avis and Deimling 3529