Embed Size (px)
Citation preview

J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
ava i l ab l e a t www.sc i enced i r ec t . com
Review Article
Cancer screening in older adults: What to do when wedon't know
Shabbir M.H. Alibhaia,b,c,d,⁎, Anne M. Horganc
a Department of Medicine, University of Toronto, Canadab Department of Health Policy, Management, and Evaluation, University of Toronto, Canadac Department of Medicine, University Health Network, Canadad Canadian Cancer Society, Canada
A R T I C L E I N F O
⁎ Corresponding author at: Department of MeE-mail address: [email protected]
1879-4068/$ – see front matter © 2011 Elsevidoi:10.1016/j.jgo.2011.03.004
A B S T R A C T
Article history:Received 25 May 2010Received in revised form21 March 2011Accepted 24 March 2011Available online 12 May 2011
More than one-half of new cancers and over 70% of cancer deaths in industrialized nationsoccur in adults age 65 or older. Systematic screening has been associated with reductions incancer-related mortality for a variety of cancers, including breast, cervical, and colorectalcancer. Prostate cancer screening remainsmore controversial despite the recent publicationoftwo large randomized trials of screening. Although guidelines are beginning to address cancerscreening specifically among the growing group of seniors age 70 or older, guidance onestimating remaining life expectancy by explicitly considering competing causes of mortality(e.g. comorbidmedical illness) and functional status in this age group is limited. In this article,key evidence-based guidelines are reviewed for cancer screening in adults and limitations ofscreening studies with respect to older adults are discussed. A framework is reviewed fordeciding how long to continue cancer screening in older adults, which incorporates age andhealth status to provide quantitative estimates of remaining life expectancy.
© 2011 Elsevier Ltd. All rights reserved.
Keywords:Cancer screeningAgedMass screening
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1501.1. Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 150
2. Breast Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1502.1. Issues in Older Women . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1502.2. Potential Harms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
3. Cervical Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1533.1. Issues in Older Women . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 153
4. Colorectal Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1534.1. Issues in Older Adults . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 154
5. Prostate Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1555.1. Issues in Older Men . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 156
6. Other Cancers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 156
dicine, University Health Network, Canada. Tel.: +1 416 340 5125; fax: +1 416 595 5826.a (S.M.H. Alibhai).
er Ltd. All rights reserved.

150 J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
7. Remaining Life Expectancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1568. Discussions with Patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1579. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157Disclosures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157Author Contributions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 157
1. Introduction
The population of adults age 65 or older in Canada and mostindustrialized nations continues to increase, in both absoluteterms and as a proportion of the overall population. In fact, theyconstitute the fastest growing segment of the North Americanpopulation. Just under 60% of all malignancies, and 71% of allcancer-related deaths, occur in people aged 65 or older.1 Adultsaged 65 or older have a 16-fold greater risk of dying from cancerthandoyoungerpeople.2Numerous studies havedemonstratedthat older adults, particularly age 75 or older, often do notundergo cancer screening tests.3,4 For example, in a retrospec-tive cohort studyamongAmericanwomenaged65orolder, 52%,41%, and11%ofwomenaged65–69, 75–79, and85+, respectively,received a screening mammogram.5 As reviewed below, whatthe optimal rate of screening should be for each of these agegroups is considerably more complex and controversial.
Several explanations for declining rates of cancer screeningin older adults can be posited. First and foremost,many cancerscreening guidelines remain silent or discourage screening inadults beyond age 70–75, primarily due to an absence ofevidence in favor of, or against, screening in this older agegroup. Second, remaining life expectancy declines withincreasing age, and any benefits of cancer screening decreasecommensurately. As such, many clinicians and patients maybe reluctant to continue with screening as patients age intotheir eighth decade and beyond. Third, there may beperceptions that the risks or related burdens associated withcancer screening increase with advancing age.
To better understand these issues, this article will brieflyreview the evidence that led to the formulation of majorguidelines for four cancers, breast, colorectal, cervical andprostate, and then discuss issues specific to seniors for eachcancer. Throughout this article the focus will be on averagerisk individuals (i.e. those without genetic conditions orcertain cancers (e.g. breast and colorectal) in first-degreerelatives that increase the risk of developing one or morespecific types of cancer primarily in younger or middle-agedadults). Particular attention will be paid to extrapolatingevidence from studies and guidelines to older adults who arebeyond the recommended age range for screening. This will befacilitated by reviewing a formal framework to considerremaining life expectancy in older adults. We will also brieflydiscuss potential harms associated with screening.
1.1. Methodology
Four malignancies (breast, colorectal, cervical and prostate)were chosen because of their significant burden in older adults(incidence and mortality) in addition to the availability of
evidence and/or guidelines regarding screening. An extensivesearch for explicit, up-to-date English-language screeningguidelines for these cancers was undertaken, with a focus onrecommendations from major medical and professionalsocieties, and governmental sources in North America. Apreference was given to those groups that addressed all fourcancers, those that clearly provided guidance for frequency oftesting, age at initiation and cessation of screening, andpreferred screening modality. Reference is also made torecommendations for specific cancers from specialist organi-zations, e.g. American Urological Association, that are widelycited. Guidelines from seven organizations are included, asshown in Table 1, including the American Cancer Society(ACS), the Canadian Task Force for Preventive Health Care(CTFPHC), and theUnitedStates Preventive Services Task Force(USPSTF). The chosen guidelines highlight the variability inrecommendations and the overall lack of elder-specific detail.The full text of the guidelines can be found on the websites ofeach organization. Evidence tables were created to summarizethe randomized controlled trials (RCTs) specifically for breastand colon cancer, where a number of RCTs exist.
2. Breast Cancer
Breast cancer is the most common non-skin cancer and thesecond highest cause of cancer deaths in Canadian andAmerican women. With increasing age, there is an increasein both breast cancer incidence and mortality.6
The most widely recommended screening maneuver con-sists of clinical breast examination (CBE) and screeningmammography (Table 1). At least eight RCTs have beenconducted on breast cancer screening using mammographywith or without CBE (Table 2).7 For women aged 50 to 69 yr,mammography reduces breast cancer mortality by 26% (95%confidence interval 17–34%).8 Self breast examination has notbeen demonstrated in RCTs to reduce breast cancer mortality9
and is not recommended as a stand-alone screeningmaneuver,although continued breast awareness is recommended.10 Arecent population-based study from Ontario suggested thatmammography plus CBEwas associatedwith improved screen-ing sensitivity and cancer detection rates compared to mam-mography alone, but at a cost of more false positive diagnosesand a greater rate of referral for further diagnostic testing.11
2.1. Issues in Older Women
With aging, breasts become easier to examine becauseglandular tissue is replaced by fat. As a consequence, thesensitivity of mammography increases slightly in older
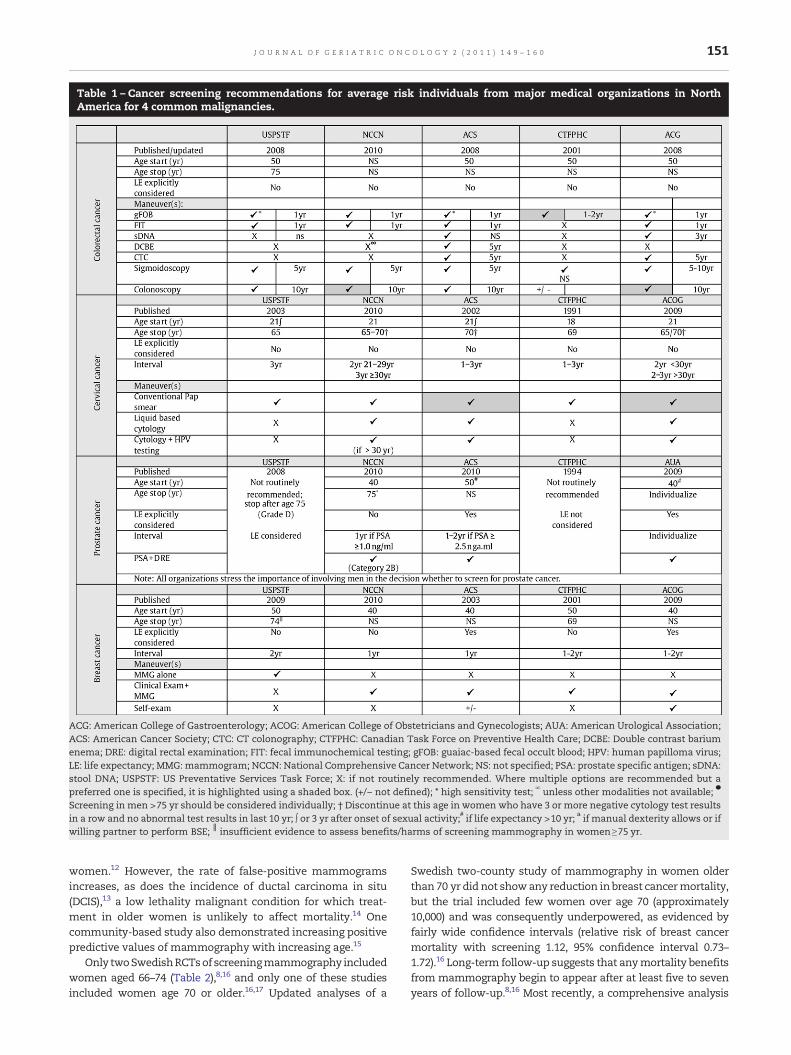
Table 1 – Cancer screening recommendations for average risk individuals from major medical organizations in NorthAmerica for 4 common malignancies.
ACG: American College of Gastroenterology; ACOG: American College of Obstetricians and Gynecologists; AUA: American Urological Association;ACS: American Cancer Society; CTC: CT colonography; CTFPHC: Canadian Task Force on Preventive Health Care; DCBE: Double contrast bariumenema; DRE: digital rectal examination; FIT: fecal immunochemical testing; gFOB: guaiac-based fecal occult blood; HPV: human papilloma virus;LE: life expectancy; MMG:mammogram; NCCN: National Comprehensive Cancer Network; NS: not specified; PSA: prostate specific antigen; sDNA:stool DNA; USPSTF: US Preventative Services Task Force; X: if not routinely recommended. Where multiple options are recommended but apreferred one is specified, it is highlighted using a shaded box. (+/− not defined); * high sensitivity test; ∞ unless other modalities not available; ●
Screening in men >75 yr should be considered individually; † Discontinue at this age in women who have 3 or more negative cytology test resultsin a row and no abnormal test results in last 10 yr; ∫ or 3 yr after onset of sexual activity;# if life expectancy >10 yr; a if manual dexterity allows or ifwilling partner to perform BSE; ║ insufficient evidence to assess benefits/harms of screening mammography in women≥75 yr.
151J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
women.12 However, the rate of false-positive mammogramsincreases, as does the incidence of ductal carcinoma in situ(DCIS),13 a low lethality malignant condition for which treat-ment in older women is unlikely to affect mortality.14 Onecommunity-based study also demonstrated increasing positivepredictive values of mammography with increasing age.15
Only twoSwedishRCTsof screeningmammography includedwomen aged 66–74 (Table 2),8,16 and only one of these studiesincluded women age 70 or older.16,17 Updated analyses of a
Swedish two-county study of mammography in women olderthan 70 yr did not showany reduction inbreast cancermortality,but the trial included few women over age 70 (approximately10,000) and was consequently underpowered, as evidenced byfairly wide confidence intervals (relative risk of breast cancermortality with screening 1.12, 95% confidence interval 0.73–1.72).16 Long-term follow-up suggests that anymortality benefitsfrom mammography begin to appear after at least five to sevenyears of follow-up.8,16 Most recently, a comprehensive analysis
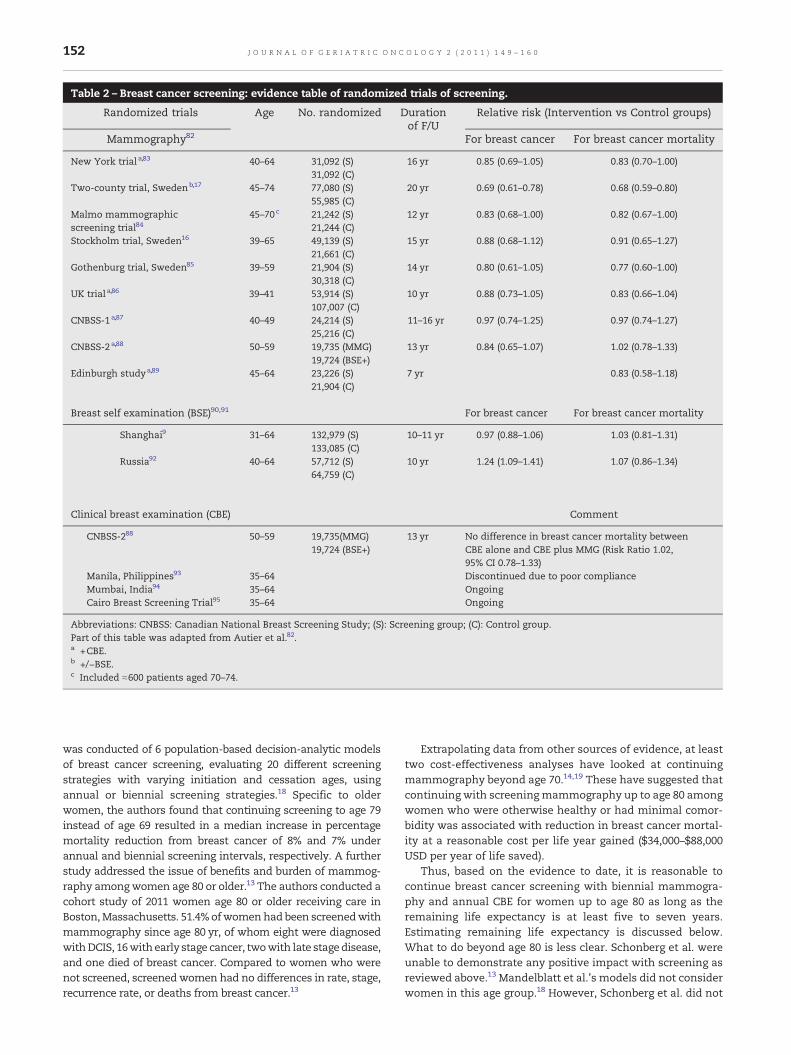
Table 2 – Breast cancer screening: evidence table of randomized trials of screening.
Randomized trials Age No. randomized Durationof F/U
Relative risk (Intervention vs Control groups)
Mammography82 For breast cancer For breast cancer mortality
New York trial a,83 40–64 31,092 (S) 16 yr 0.85 (0.69–1.05) 0.83 (0.70–1.00)31,092 (C)
Two-county trial, Swedenb,17 45–74 77,080 (S) 20 yr 0.69 (0.61–0.78) 0.68 (0.59–0.80)55,985 (C)
Malmo mammographicscreening trial84
45–70c 21,242 (S) 12 yr 0.83 (0.68–1.00) 0.82 (0.67–1.00)21,244 (C)
Stockholm trial, Sweden16 39–65 49,139 (S) 15 yr 0.88 (0.68–1.12) 0.91 (0.65–1.27)21,661 (C)
Gothenburg trial, Sweden85 39–59 21,904 (S) 14 yr 0.80 (0.61–1.05) 0.77 (0.60–1.00)30,318 (C)
UK trial a,86 39–41 53,914 (S) 10 yr 0.88 (0.73–1.05) 0.83 (0.66–1.04)107,007 (C)
CNBSS-1a,87 40–49 24,214 (S) 11–16 yr 0.97 (0.74–1.25) 0.97 (0.74–1.27)25,216 (C)
CNBSS-2a,88 50–59 19,735 (MMG) 13 yr 0.84 (0.65–1.07) 1.02 (0.78–1.33)19,724 (BSE+)
Edinburgh studya,89 45–64 23,226 (S) 7 yr 0.83 (0.58–1.18)21,904 (C)
Breast self examination (BSE)90,91 For breast cancer For breast cancer mortality
Shanghai9 31–64 132,979 (S) 10–11 yr 0.97 (0.88–1.06) 1.03 (0.81–1.31)133,085 (C)
Russia92 40–64 57,712 (S) 10 yr 1.24 (1.09–1.41) 1.07 (0.86–1.34)64,759 (C)
Clinical breast examination (CBE) Comment
CNBSS-288 50–59 19,735(MMG) 13 yr No difference in breast cancer mortality betweenCBE alone and CBE plus MMG (Risk Ratio 1.02,95% CI 0.78–1.33)
19,724 (BSE+)
Manila, Philippines93 35–64 Discontinued due to poor complianceMumbai, India94 35–64 OngoingCairo Breast Screening Trial95 35–64 Ongoing
Abbreviations: CNBSS: Canadian National Breast Screening Study; (S): Screening group; (C): Control group.Part of this table was adapted from Autier et al.82.a +CBE.b +/−BSE.c Included ≈600 patients aged 70–74.
152 J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
was conducted of 6 population-based decision-analytic modelsof breast cancer screening, evaluating 20 different screeningstrategies with varying initiation and cessation ages, usingannual or biennial screening strategies.18 Specific to olderwomen, the authors found that continuing screening to age 79instead of age 69 resulted in a median increase in percentagemortality reduction from breast cancer of 8% and 7% underannual and biennial screening intervals, respectively. A furtherstudy addressed the issue of benefits and burden of mammog-raphy amongwomen age 80 or older.13 The authors conducted acohort study of 2011 women age 80 or older receiving care inBoston,Massachusetts. 51.4% ofwomenhad been screenedwithmammography since age 80 yr, of whom eight were diagnosedwithDCIS, 16withearly stage cancer, twowith late stagedisease,and one died of breast cancer. Compared to women who werenot screened, screened women had no differences in rate, stage,recurrence rate, or deaths from breast cancer.13
Extrapolating data from other sources of evidence, at leasttwo cost-effectiveness analyses have looked at continuingmammography beyond age 70.14,19 These have suggested thatcontinuing with screeningmammography up to age 80 amongwomen who were otherwise healthy or had minimal comor-bidity was associated with reduction in breast cancer mortal-ity at a reasonable cost per life year gained ($34,000–$88,000USD per year of life saved).
Thus, based on the evidence to date, it is reasonable tocontinue breast cancer screening with biennial mammogra-phy and annual CBE for women up to age 80 as long as theremaining life expectancy is at least five to seven years.Estimating remaining life expectancy is discussed below.What to do beyond age 80 is less clear. Schonberg et al. wereunable to demonstrate any positive impact with screening asreviewed above.13 Mandelblatt et al.'s models did not considerwomen in this age group.18 However, Schonberg et al. did not

153J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
attempt to stratify women on the basis of remaining lifeexpectancy.13 A careful discussion with women in this agegroup who have a life expectancy of at least 5–7 yr (see below)about continuing screening, keeping in mind the increasedpossible risks/harms, may be reasonable.
2.2. Potential Harms
Screening for any cancer is associated with at least 3potentially important harms: false-positive screening results,unnecessary subsequent procedures, and overdiagnosis. Inthe recent comprehensive analysis by Mandelblatt et al.,stopping annual screening at age 79 instead of age 69 led toan additional 240 false-positive results per 1000womenand anadditional unnecessary 16 biopsies per 1000women. Althoughnumerical data were not provided, the risk of overdiagnosis(i.e. finding tumors that did not lead to morbidity or excessmortality in the patient's remaining lifetime) increased withage, mostly because of increasing rates of competing causes ofmortality (i.e. greater comorbidity in older women). In anotherstudy, the incidence of DCIS has increased by awhopping 750%in the last 20 yr, primarily due to enhanced detection bymammography.20 Specific to women age 80 or older, Schon-berg et al. reported an 11% rate of false-positive screeningmammograms leading to 19 benign breast biopsies, threewomen experienced a false-negativemammogram, and sevenwomen were diagnosed with DCIS.13 Model-based analyseshave suggested these potential harms can be significantlyreducedwithminimal impact onmortality reduction and earlydetection of breast cancer by reducing the screening intervalfrom annual to biennial.18 An important fourth additionalharm is false-negative results, which can lead to falsereassurance and later detection of cancers. This does notseem to be an issue in older women undergoing mammogra-phy, at least in the study by Schonberg et al.13
Beyond potential clinical harms, adverse economic conse-quences of screening need to be considered. These can includecosts associated with unnecessary screening or subsequentconfirmatory testing, costs associated with treatment ofoverdiagnosed, asymptomatic tumors, out-of-pocket costsassociated with follow-up visits for patients and caregivers,etc. Few data are available from extant cost-effectivenessmodels for these outcomes.19
3. Cervical Cancer
Cervical cancer is the third most common gynecologicmalignancy and twelfth most common cancer overall amongwomen in Canada.6 Similar statistics are noted in the UnitedStates.21 Although the incidence and mortality rates ofinvasive cervical cancer have been declining in Canada andthe United States since 196021,22 both the incidence andmortality increase with age, with the probability of developingcervical cancer being 1 in 648 for women aged ≤ 39 yr; 1 in 374for women 40–59 yr; 1 in 755 for women 60–69 yr; and 1 in 552in those ≥ 70 yr.23 About one-half of all cases are diagnosed inwomen who have never been screened.24
Although no RCTs have directly demonstrated a reductionin cervical cancer mortality with screening, there is a large
body of evidence from cohort and case–control studiessupporting the effectiveness of screening.25 The Papanicolaou(Pap) test is the standard screening test for cervical cancer(Table 1). Newer cytologic techniques, such as using liquid-based thin-layer slide preparation, may be associated withhigher sensitivity and may therefore require less frequentscreening intervals.24 Testing for HPV as an adjunct to cervicalsmear testing has recently been included as a potentialscreening modality in a number of guidelines, having beenshown in multiple studies to be more sensitive than cervicalcytology alone in detecting cervical histopathology.26–28 Poorspecificity limits it as a stand-alone primary screeningmodality while the combination results in the identificationof large numbers of cervical intraepithelial neoplasia (CIN)disease, precancerous disease that often spontaneouslydisappears, especially in younger women.29–31 None of thesemodalities have been adequately evaluated in older women.
3.1. Issues in Older Women
Cervical cancer screening decreases with increasing age, withCanadian data suggesting that 40–45% of women aged 60–69have not had a Pap test in the last three years.32 US datasuggested that 28–64% of women age 65 or older have neverhad a Pap test or have not had one done in the past threeyears,33 although more recent data suggest cervical cancerscreening may have improved in older American women.34
Interestingly, all 5 guidelines that we included recommendstopping screening in average risk women (i.e., those withoutprior abnormal cytology results or who are positive for humanpapillomavirus) by the age of 70 (Table 1).24 Since cervicalcancer is rare among average risk women over age 70 whohave been screened in the past,35 it appears reasonable to stopscreening at age 70 in these women. Although this guideline isan expert-based recommendation, it is supported by adecision-analytic model.24,36
4. Colorectal Cancer
Colorectal cancer is the second and third most common causeof cancer death in men and women, respectively,6 and theprevalence of colorectal cancer increases markedly amongpersons beyond 50 yr of age.
Several different screening maneuvers have been consid-ered, including the fecal occult blood test (FOBT), sigmoidos-copy, double contrast barium enema (DCBE), and colonoscopy(Table 3a and 3b). The strongest evidence exists for FOBT. RCTshave demonstrated that annual screening with the FOBT isassociated with a 15–33% reduction in colorectal cancermortality and a 17–20% reduction in incidence.37–40 Retrospec-tive case–control studies have shown that flexible sigmoidos-copy reduces mortality from colorectal cancer.41 A smallerRCT demonstrated reduced incidence of colorectal cancer butno reduction in cancer mortality was noted,42 whereas asecond RCT showed a trend toward reduced cancer mortalitybut no change in incidence.43 Most recently, a just-publishedlarge RCT of one-time flexible sigmoidoscopy demonstrated23% and 31% reduction in colorectal cancer incidence andmortality, respectively.44 A second large RCT of flexible
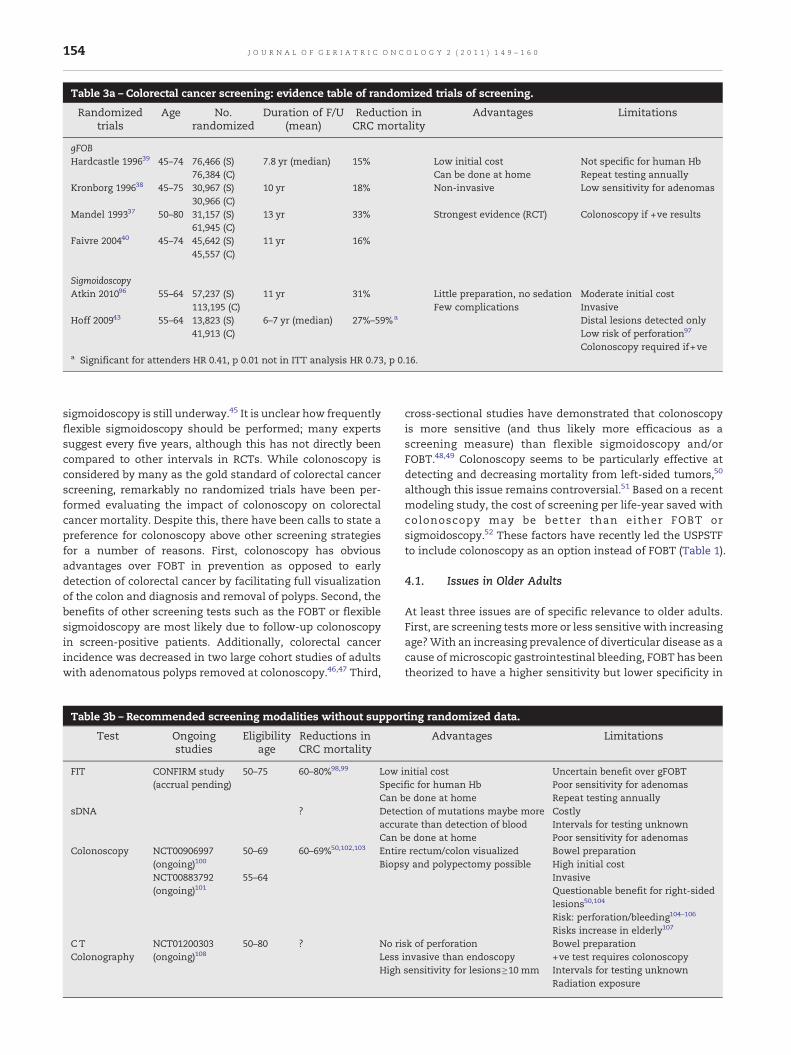
Table 3a – Colorectal cancer screening: evidence table of randomized trials of screening.
Randomizedtrials
Age No.randomized
Duration of F/U(mean)
Reduction inCRC mortality
Advantages Limitations
gFOBHardcastle 199639 45–74 76,466 (S) 7.8 yr (median) 15% Low initial cost Not specific for human Hb
76,384 (C) Can be done at home Repeat testing annuallyKronborg 199638 45–75 30,967 (S) 10 yr 18% Non-invasive Low sensitivity for adenomas
30,966 (C)Mandel 199337 50–80 31,157 (S) 13 yr 33% Strongest evidence (RCT) Colonoscopy if +ve results
61,945 (C)Faivre 200440 45–74 45,642 (S) 11 yr 16%
45,557 (C)
SigmoidoscopyAtkin 201096 55–64 57,237 (S) 11 yr 31% Little preparation, no sedation Moderate initial cost
113,195 (C) Few complications InvasiveHoff 200943 55–64 13,823 (S) 6–7 yr (median) 27%–59%a Distal lesions detected only
41,913 (C) Low risk of perforation97
Colonoscopy required if+vea Significant for attenders HR 0.41, p 0.01 not in ITT analysis HR 0.73, p 0.16.
154 J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
sigmoidoscopy is still underway.45 It is unclear how frequentlyflexible sigmoidoscopy should be performed; many expertssuggest every five years, although this has not directly beencompared to other intervals in RCTs. While colonoscopy isconsidered by many as the gold standard of colorectal cancerscreening, remarkably no randomized trials have been per-formed evaluating the impact of colonoscopy on colorectalcancer mortality. Despite this, there have been calls to state apreference for colonoscopy above other screening strategiesfor a number of reasons. First, colonoscopy has obviousadvantages over FOBT in prevention as opposed to earlydetection of colorectal cancer by facilitating full visualizationof the colon and diagnosis and removal of polyps. Second, thebenefits of other screening tests such as the FOBT or flexiblesigmoidoscopy are most likely due to follow-up colonoscopyin screen-positive patients. Additionally, colorectal cancerincidence was decreased in two large cohort studies of adultswith adenomatous polyps removed at colonoscopy.46,47 Third,
Table 3b – Recommended screening modalities without suppor
Test Ongoingstudies
Eligibilityage
Reductions inCRC mortality
FIT CONFIRM study(accrual pending)
50–75 60–80%98,99 LowSpecCan b
sDNA ? DetecaccurCan b
Colonoscopy NCT00906997(ongoing)100
50–69 60–69%50,102,103 EntirBiops
NCT00883792(ongoing)101
55–64
C TColonography
NCT01200303(ongoing)108
50–80 ? No riLessHigh
cross-sectional studies have demonstrated that colonoscopyis more sensitive (and thus likely more efficacious as ascreening measure) than flexible sigmoidoscopy and/orFOBT.48,49 Colonoscopy seems to be particularly effective atdetecting and decreasing mortality from left-sided tumors,50
although this issue remains controversial.51 Based on a recentmodeling study, the cost of screening per life-year saved withcolonoscopy may be better than either FOBT orsigmoidoscopy.52 These factors have recently led the USPSTFto include colonoscopy as an option instead of FOBT (Table 1).
4.1. Issues in Older Adults
At least three issues are of specific relevance to older adults.First, are screening testsmore or less sensitive with increasingage?With an increasing prevalence of diverticular disease as acause of microscopic gastrointestinal bleeding, FOBT has beentheorized to have a higher sensitivity but lower specificity in
ting randomized data.
Advantages Limitations
initial cost Uncertain benefit over gFOBTific for human Hb Poor sensitivity for adenomase done at home Repeat testing annuallytion of mutations maybe moreate than detection of blood
Costly
e done at homeIntervals for testing unknownPoor sensitivity for adenomas
e rectum/colon visualized Bowel preparationy and polypectomy possible High initial cost
InvasiveQuestionable benefit for right-sidedlesions50,104
Risk: perforation/bleeding104–106
Risks increase in elderly107
sk of perforation Bowel preparationinvasive than endoscopy +ve test requires colonoscopysensitivity for lesions≥10 mm Intervals for testing unknown
Radiation exposure

155J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
older adults, but rigorous clinical data are lacking. Second, arescreening tests less safe? A major complication of flexiblesigmoidoscopy and colonoscopy is bowel perforation. It occursin about one in 10,000 adults with flexible sigmoidoscopy53
and about one in 3000 with colonoscopy.54 It is even rarer withDCBE and approaches zero risk with CT colonography(0.005%).55 A recent Medicare-based study examined compli-cation rates after outpatient colonoscopy, and confirmed thatboth increasing age and comorbidity were associated withgreater risks of adverse events within 30 days. The risk ofperforation was 0.6 per 1000 procedures, and the risk of deathwas approximately 0.1% overall (53 of 53,200 colonoscopies)among patients aged 66 to 95.56 Thus, although complicationsof colonoscopy increase with age, the absolute rates remainquite low and are unlikely to affect the choice of one screeningtest over another. Third, when should screening stop? Whilestudies have generally included adults up to age 79–85, benefitfrom screening appears within 5–10 yr of follow-up.38,39 Thus,screening is likely to be of limited benefit and may be harmfulin individuals with a remaining life expectancy of less thanfive years.
As a consequence of recently published data, the USPSTFrevised its guidelines in 2008 to indicate an upper age limit of75 yr above which colorectal cancer screening was no longerroutinely recommended, and discouraged at age 86 or higher,due to limited benefits and increased risk of harms.57 Again,however, these guidelines fail to consider remaining lifeexpectancy, which is influenced by more than chronologicalage.Noneof theothermajor guidelineswe reviewed featuredanupperage, although theACSguidelines suggesteddiscontinuingscreening once life expectancy is less than 10 yr (Table 1).
5. Prostate Cancer
Prostate cancer is the most common cancer in both Canadianand American men and the second or third most commoncause of cancer mortality.6,21 The prevalence increases withage, and the median age at diagnosis is 68 yr.6,21 Althoughmortality from prostate cancer also increases with age, therisk of dying from prostate cancer is about 3% for a man aged60 or older.25
Prostate cancer screening remains controversial in variousage groups. Until last year, this was primarily because therewere no high-quality RCTs that either supported or refutedscreening for prostate cancer. Given the slow growth of manytumors, the risk of overdetection (i.e., identifying tumors thatare indolent and unlikely to be clinically important during aman's remaining life) is high.58 Not only is treatmentassociated with significant long-term side effects such asincontinence, impotence, and bowel injury, there is only oneRCT that has demonstrated that aggressive treatment oflocalized prostate cancer improves survival.59,60
In 2009, preliminary results of two large RCTs examining thebenefits and risks of screening for prostate cancer werepublished.61,62 Despite these new data, prostate cancer screeningremains controversial, for reasons that are discussed below.
Both RCTs reported interim data after 7–9 yr of follow-up.The first RCT, part of the massive US Prostate, Lung, Colorectal,andOvarian (PLCO) Cancer Screening Trial, enrolled 76,693men
ages 55–74 to annual screeningwith a PSA test and digital rectalexamination (DRE).61 Compliancewas over 85% in the screeningarm, but screening in the control arm (due to provider choice)went from 40% at baseline to 52%, significantly weakening thelikelihood of finding any benefit of screening because ofcontamination (leading to dramatically reducedpower). Neitherbiopsies nor treatment were mandated if the PSA was above aspecific threshold. After a median of 11 yr of follow-up, therewere 92 deaths fromprostate cancer in screenedpatients and 82in the control group (rate ratio 1.11, 95% confidence interval (CI)0.83 to 1.50).
In contrast, in theEuropeanstudy, 182,000menages55–69 in7European countries (with the majority coming from 2 countries)were offered PSA screening every 2–4 yr; most centers did notinclude DRE.62 Additionally, a biopsy was mandated if the PSArose above 3.0 ng/mL, in contrast to the US study, but notreatment was mandated if the biopsy was positive. After amedianof9 yrof follow-up, 5990prostatecancerswerediagnosedin the screening group compared to 4307 among controls. Moreimportantly, 214 prostate cancer deaths occurred in the screenedgroup compared to 326 in the control group (rate ratio 0.80, 95%CI0.67 to 0.95). Mortality curves did not separate between screenedand unscreened groups until at least 10 yr of follow-up. Theabsolute difference in prostate cancer deaths is about 0.71 per1000 men screened. Follow-up continues in both trials.
Interpretation of the 2 studies is challenging and contro-versial.63 It is abundantly clear that screening is associatedwitha significantly greater detection rate of prostate cancer and asignificant risk of overdetection,58 but the 2 RCTs differ withrespect to whether early detection improves cancer-specificmortality.
Prior to the publication of these 2 trials, both the CTFPHCand the USPSTF concluded that there is insufficient evidenceto recommend for or against screening for prostate cancerwhereas the American Urological Association recommendedscreening be considered from age 40 onwards (Table 1). TheACS recently revised its recommendations based on the 2RCTs; it now recommends that men age 50 or older who haveat least a 10-year life expectancy be provided an opportunity tomake an informed choice about screening for prostate cancerwith a PSA test with or without DRE.64
The incidence of prostate cancer is quite low in men underthe age of 50 with no risk factors (such as African Americanethnicity or a positive family history of prostate cancer; forthesemen, screening discussions should bemade earlier). TheDRE has a sensitivity of 59% in asymptomatic men.65 Althoughit is inexpensive and simple to perform, it picks up fewercancers than PSA testing and its reproducibility is low.66 ThePSA test has a sensitivity of about 73% and specificity of 85%.66
These performance characteristics vary depending on the PSAcut-off that is used and the age of the patient. Adjusting thePSA cut-off on the basis of age or using free to total PSA ratio,PSA density, or other permutations of the test alter sensitivityand specificity somewhat but none of these measures hasbeen associated with reductions in prostate cancer mortality.None of these enhancements beyond a simple PSA level arerecommended by the ACS.64 Another important confoundingfactor in screening considerations is that 15% of men with anormal PSA (<3 ng/mL) and normal DRE have a diagnosis ofprostate cancer on systematic prostate biopsy.67

156 J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
5.1. Issues in Older Men
In the situationwhereamiddle-agedmanandhisphysicianhaveagreed to start screeningwith annual PSA andDRE, when shouldhe stop? An important factor to consider is lead time bias. Thisrefers to picking up subclinical disease earlier (as a consequenceof screening) and consequently making long-term survivalappear better without actually altering the natural history ofthedisease. In thecaseofprostate cancer screening, thishasbeenestimated at 7–12 yr.58,68,69Why is this relevant? The only RCT todemonstrate an impact on survival with aggressive treatmentrequired about eight years of follow-up,59 and only 5% of patientshad screen-detected disease.70 In other words, the vast majorityof men had clinically diagnosed disease. This means that forscreening to be useful, a man would probably need to have aremaining life expectancy of 15–20 yr (lead time+median follow-up time from the Scandinavian RCT).
Somewhat surprisingly, the USPSTF recently revised itsguidelines to recommend not screening for prostate cancer inmen age 75 or older, citing low likelihood of benefit andsignificant risks of overdetection and harm fromovertreatment.71 This recommendation was made prior to thepublication of the 2 RCTs reviewed above, which led many toquestion what evidence led the USPSTF to alter its recommen-dation. From a geriatric oncology perspective, the new recom-mendation is troubling, since there is virtually no directevidence, new or old, examining screening in men age 75 orolder. Even if indirect evidence fromdecision-analyticmodelsorrecommendations from other guidelines are considered, theseindirect lines of evidence argue that screening is reasonable ifremaining life expectancy is at least 10 yr, which it is for manymen age 75 or older.75 Clearly this issue remains controversialeven after the publication of the two recent RCTs, although itwould have been more rational to use a life expectancy cutoffrather than an absolute age cutoff for when to stop screening,even though determining remaining life expectancy in practiceis not straightforward (see below).
6. Other Cancers
At present, neither the CTFPHC nor the USPSTF recommendscreening for ovarian or uterine cancer in women and lung orskin cancer in both sexes due to lack of data demonstratingreductions in cancer-specific mortality. No guidelines onscreening for these diseases are provided by NCCN. Screeningfor these cancers have been reviewed in detail elsewhere.However, the ACS recommends self-examination of the skinby all adults and skin examination within the context of aperiodic health visit, and no upper age limit is provided.25,72
That being said, no studies have demonstrated reduction inskin cancer mortality from regular screening by either thepatient or a health care professional.
7. Remaining Life Expectancy
Critical to the discussion of whether to continue screening inadults beyond age 70–75, where guidelines and the primary
evidence are generally silent, is considering and estimatingthe patient's remaining life expectancy. Clearly age is a factor,with the average 65-year-old expected to live longer than theaverage 70- or 75-year-old. Yet there is tremendous heteroge-neity in the older population. Estimating remaining lifeexpectancy is not an easy or precise science, yet decisionsare made at the bedside or in the office after implicitlyconsidering remaining life expectancy on a daily basis. Beyondage, both comorbidity (the presence of one or more medicalillnesses) and functional status (independent or dependent inbasic or instrumental activities of daily living) impact onremaining life expectancy.73,74 Almost a decade ago Walterand Covinsky presented a compelling framework that at-tempts to integrate these factors when considering cancerscreening in older adults.75 In general, based on actuarial lifetables and large longitudinal studies, individuals in excellenthealth tend to live about 25% longer than someone of equalage who is in average health. Conversely, individuals in poorhealth tend to live about 30–50% shorter than the averageperson. Similarly, several studies have demonstrated that, incommunity-dwelling older adults, dependence in one ormore76 or two or more77 instrumental activities of daily living(IADLs) is associated with at least a 50% greater risk of dying inthe next three, five, or ten years, adjusted for age, sex, and avariety of sociodemographic and clinical factors, includingcomorbidity.76,77 Walter has gone on to develop a model thatpredicts one-year survival after hospitalization in olderadults78 and demonstrated the impact of both age andcomorbidity on 5-year survival in older adults undergoingscreening for colorectal cancer.79 However, published lifeexpectancy models for older adults incorporating factorsbeyond age and gender rarely extend beyond the 1- to 5-yeartime horizon,76,80 whereas screening decisions usually entailthinking beyond this time frame.Moreover, Ganguli et al. havepublished the only model incorporating age, comorbidity,functional status, and other factors in community-dwellingolder adults that extends follow-up out to 10 yr, but theirmultivariable proportional hazards model has not beenindependently validated. Other important factors that mayaffect long-term survival include frailty, cognitive impair-ment, and physical activity.76,77
Sowhat is a clinician to do?Walter andCovinsky's frameworkremains seminal in assisting clinicians in thinking about factorsbeyond age and gender, but it does not explicitly considercomorbidity, functional status, frailty, cognition, or other vari-ables separately.75 What it does is stratify life expectancyestimates into quartiles using actuarial life tables.81 While it isreasonable to assume that individuals in the highest (best)quartile of life expectancy have no to minimal comorbidity andexcellent functional status, there are no working definitions ofaverage or poor health. Integrating various published prognosticmodels, it is tempting to approximate average health as havingmild comorbidity (e.g., with controlled hypertension, osteoarthri-tis, or similar conditions) and reasonable functional indepen-dence, this may be no better than the clinician's expert opinion.Stated differently, while there is no question that comorbidity,functional dependence, andother factors influence remaining lifeexpectancy, there is presently no validated prediction tool to helpa clinician do this. In our own geriatric oncology practices, wehave defined average health as having mild comorbidity (e.g.

157J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
controlledhypertension, osteoarthritis, etc.) and independence inIADLs. Similarly, we equate poor healthwith one ormore seriouscomorbidities (e.g., prior myocardial infarction in the last twoyears,moderate to severe chronic obstructive pulmonary diseaseusing regular bronchodilators, and congestive heart failure withat least one hospitalization in the last year) and dependence inone or more IADLs. We have adopted these definitions afterconsulting published prognostic models as well as severalcomorbidity measures, notably the Charlson Index, the Index ofCoexistent Diseases, and the Adult Comorbidity Evaluation 27(ACE 27). Whether these definitions accurately reflect thequartiles of health in Walter and Covinsky's article remains tobe established. Readers may particularly find it useful to use aconvenient web-based comorbidity scoring system (http://oto2.wustl.edu/clinepi/calc.html) for theACE27.74AlthoughtheACE27has only been validated in cancer patients, it has been shown tohaveprognostic impact onoverall survival acrossabroad rangeoftumors, andmoderate to severecomorbidity is associatedwithanadjusted hazard ratio of mortality of 1.86 and 2.56, respectively.74
These estimates are similar to those of other studies examiningtheprognostic impactof comorbidityand functional statusabove,lending support to its use by clinicians. However, we mustemphasize that it has not been validated for the purpose ofestimating life expectancy in older adults considering cancerscreening.
8. Discussions with Patients
Although not the focus of our review, it is important torecognize that having discussionswith patients aboutwhen tostop screening are difficult for clinicians. Beyond the impre-cision of models for estimating life expectancy and thelimitations in evidence noted above, they force us to confrontthe notion of a patient's proximate mortality and requiresignificantly more effort and time than ordering a repeatscreening test. Beyond the principles in the frameworkoutlined by Walter and Covinsky,75 and some principles onwhen to consider recommending termination of screening bythe USPSTF (Appendix X of the procedure manual), there is aneed for educational toolkits and/or decision aids which maybe a way to facilitate such discussions. However, we are notaware of any such decision aids that specifically deal with thenotion of stopping (rather than starting or not starting)screening for any of the cancers we have reviewed. This isan important area for future research and development.
9. Summary
Cancer remains a major cause of morbidity and mortality inolder adults. This situation is likely to worsen given thedemographic imperative and improving survival rates after anew cancer diagnosis. Cancer screening is an important toolfor decreasing the incidence of and mortality from cancer inolder adults. In particular, systematic screening for colorectalcancer in both sexes, breast cancer and cervical cancer inwomen, and possibly prostate cancer inmen lead to decreasedmortality from the respective cancers. Guidelines on cancerscreening have been reviewed, in order to provide a scientific
basis for when to stop screening in adults over age 70–75. For agiven patient, along with their values and preferences, it isimportant to consider remaining life expectancy, which can beestimated using age and health status. It is hoped that thisinformation and the tables in this article will help inform amore rational discussion between the physician and theirolder patient about when to stop cancer screening. Validatedlong-term prognostic models and educational resources tohelp physicians with such discussions are urgently needed.
Disclosures
Drs. Alibhai andHorganhaveno financial conflicts of interest todeclare with respect to this article and related subject matter.
Author Contributions
Conception and Design, Data collection, analysis and inter-pretation of data, manuscript writing, approval of finalversion: Dr. Alibhai.
Data collection, analysis and interpretation of data, man-uscript writing, approval of final version: Dr. Horgan.
R E F E R E N C E S
1. Kinsella K, Velkoff VA. An aging world: 2001. U.S. CensusBureau P95/01-1. Washington (DC): U.S. Government PrintingOffice; 2001.
2. Ries LAG, Eisner MP, Kosary CL, Hankey BF, Miller BA, Clegg L,et al, editors. SEER Cancer Statistics Review, 1975–2000.Bethesda, MD: National Cancer Institute; 2003.
3. Sawaya GF, Brown AD, Washington AE, Garber AM. Clinicalpractice. Current approaches to cervical-cancer screening.N Engl J Med 2001;344:1603–1607.
4. Jerant AF, Franks P, Jackson JE, Doescher MP. Age-relateddisparities in cancer screening: analysis of 2001BehavioralRiskFactor Surveillance System data. Ann Fam Med 2004;2:481–487.
5. Bynum JP, Braunstein JB, Sharkey P, Haddad K, Wu AW. Theinfluence of health status, age, and race on screeningmammography in elderly women. Arch Intern Med 2005;165:2083–2088.
6. Canadian Cancer Society: Canadian Cancer Statistics 2010.Toronto, 2010.
7. Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancerscreening: a summary of the evidence for the U.S. PreventiveServices Task Force. Ann Intern Med 2002;137:347–360.
8. Kerlikowske K, Grady D, Rubin SM, Sandrock C, Ernster VL.Efficacy of screening mammography. A meta-analysis. JAMA1995;273:149–154.
9. Thomas DB, Gao DL, Ray RM, Wang WW, Allison CJ, ChenFL, et al. Randomized trial of breast self-examination inShanghai: final results. J Natl Cancer Inst 2002;94:1445–1457.
10. Baxter N. Preventive health care, 2001 update: should womenbe routinely taught breast self-examination to screen forbreast cancer? Cmaj 2001;164:1837–1846.
11. Chiarelli AM, Majpruz V, Brown P, Theriault M, Shumak R,Mai V. The contribution of clinical breast examination to theaccuracy of breast screening. J Natl Cancer Inst 2009;101:1236–1243.
158 J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
12. Kerlikowske K, Grady D, Barclay J, Sickles EA, Ernster V. Effectof age, breast density, and family history on the sensitivity offirst screening mammography. JAMA 1996;276:33–38.
13. Schonberg MA, Silliman RA, Marcantonio ER. Weighing thebenefits and burdens of mammography screening amongwomen age 80 years or older. J Clin Oncol 2009;27:1774–1780.
14. Kerlikowske K, Salzmann P, Phillips KA, Cauley JA, CummingsSR. Continuing screeningmammography inwomen aged 70 to79 years: impact on life expectancy and cost-effectiveness.JAMA 1999;282:2156–2163.
15. Kerlikowske K, Grady D, Barclay J, Sickles EA, Eaton A, ErnsterV. Positive predictive value of screening mammography byage and family history of breast cancer. JAMA 1993;270:2444–2450.
16. Nystrom L, Andersson I, Bjurstam N, Frisell J, Nordenskjold B,Rutqvist LE. Long-term effects of mammography screening:updated overview of the Swedish randomised trials. Lancet2002;359:909–919.
17. Tabar L, Vitak B, ChenHH, Duffy SW, YenMF, Chiang CF, et al.The Swedish Two-County Trial twenty years later. Updatedmortality results and new insights from long-term follow-up.Radiol Clin North Am 2000;38:625–651.
18. Mandelblatt JS, Cronin KA, Bailey S, Berry DA, de Koning HJ,Draisma G, et al. Effects of mammography screening underdifferent screening schedules: model estimates of potentialbenefits and harms. Ann Intern Med 2009;151:738–747.
19. Mandelblatt J, Saha S, Teutsch S, Hoerger T, Siu AL, Atkins D,et al. The cost-effectiveness of screening mammographybeyond age 65 years: a systematic review for the U.S.Preventive Services Task Force. Ann Intern Med 2003;139:835–842.
20. Ernster VL, Ballard-Barbash R, Barlow WE, Zheng Y, WeaverDL, Cutter G, et al. Detection of ductal carcinoma in situ inwomen undergoing screening mammography. J Natl CancerInst 2002;94:1546–1554.
21. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancerstatistics, 2009. CA Cancer J Clin 2009;59:225–249.
22. Franco EL, Duarte-Franco E, Ferenczy A. Cervical cancer:epidemiology, preventionand the roleofhumanpapillomavirusinfection. Cmaj 2001;164:1017–1025.
23. http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/documents/document/acspc-026238.pdf ACS-CFFA.
24. Saslow D, Runowicz CD, Solomon D, Moscicki AB, Smith RA,Eyre HJ, et al. American Cancer Society guideline for the earlydetection of cervical neoplasia and cancer. CA Cancer J Clin2002;52:342–362.
25. Brawley OW, Kramer BS. Cancer screening in theory and inpractice. J Clin Oncol 2005;23:293–300.
26. Cuzick J, Clavel C, Petry KU, Meijer CJ, Hoyer H, Ratnam S,et al. Overview of the European and North American studieson HPV testing in primary cervical cancer screening. Int JCancer 2006;119:1095–1101.
27. Koliopoulos G, ArbynM,Martin-Hirsch P, KyrgiouM, PrendivilleW, Paraskevaidis E. Diagnostic accuracy of humanpapillomavirus testing in primary cervical screening: asystematic review and meta-analysis of non-randomizedstudies. Gynecol Oncol 2007;104:232–246.
28. Mayrand MH, Duarte-Franco E, Rodrigues I, Walter SD,Hanley J, Ferenczy A, et al. Human papillomavirus DNAversus Papanicolaou screening tests for cervical cancer.N Engl J Med 2007;357:1579–1588.
29. Cuzick J, Szarewski A, Cubie H, Hulman G, Kitchener H,Luesley D, et al. Management of women who test positive forhigh-risk types of human papillomavirus: the HART study.Lancet 2003;362:1871–1876.
30. Arbyn M, Buntinx F, Van Ranst M, Paraskevaidis E,Martin-Hirsch P, Dillner J. Virologic versus cytologic triage ofwomen with equivocal Pap smears: a meta-analysis of the
accuracy to detect high-grade intraepithelial neoplasia. J NatlCancer Inst 2004;96:280–293.
31. Ronco G, Giorgi-Rossi P, Carozzi F, Confortini M, Dalla PalmaP, Del Mistro A, et al. Efficacy of human papillomavirustesting for the detection of invasive cervical cancers andcervical intraepithelial neoplasia: a randomised controlledtrial. Lancet Oncol 2010;11:249–257.
32. Cervical Cancer Screening in Canada: 1998 SurveillanceReport. Ottawa: Public Health Agency of Canada; 1998.
33. Mandelblatt JS, HammondDB. Primary care of elderlywomen: isPap smear screening necessary?Mt Sinai J Med 1985;52:284–290.
34. Ostbye T, Greenberg GN, Taylor Jr DH, Lee AM. Screeningmammography and Pap tests among older American women1996–2000: results from the Health and Retirement Study(HRS) and Asset and Health Dynamics Among the Oldest Old(AHEAD). Ann Fam Med 2003;1:209–217.
35. Stenkvist B, Bergstrom R, Eklund G, Fox CH. Papanicolaousmear screening and cervical cancer. What can you expect?JAMA 1984;252:1423–1426.
36. Mandelblatt JS, Lawrence WF, Womack SM, Jacobson D, Yi B,Hwang YT, et al. Benefits and costs of using HPV testing toscreen for cervical cancer. JAMA 2002;287:2372–2381.
37. Mandel JS, Bond JH, Church TR, Snover DC, Bradley GM,Schuman LM, et al. Reducingmortality from colorectal cancerby screening for fecal occult blood. Minnesota Colon CancerControl Study. N Engl J Med 1993;328:1365–1371.
38. Kronborg O, Fenger C, Olsen J, Jorgensen OD, Sondergaard O.Randomised study of screening for colorectal cancer withfaecal-occult-blood test. Lancet 1996;348:1467–1471.
39. Hardcastle JD, Chamberlain JO, Robinson MH, Moss SM, AmarSS, Balfour TW, et al. Randomised controlled trial offaecal-occult-blood screening for colorectal cancer. Lancet1996;348:1472–1477.
40. Faivre J, Dancourt V, Lejeune C, Tazi MA, Lamour J, Gerard D,et al. Reduction in colorectal cancer mortality by fecal occultblood screening in a French controlled study. Gastroenterology2004;126:1674–1680.
41. Walsh JM, Terdiman JP. Colorectal cancer screening: scientificreview. JAMA 2003;289:1288–1296.
42. Thiis-Evensen E, Hoff GS, Sauar J, Langmark F, Majak BM,Vatn MH. Population-based surveillance by colonoscopy:effect on the incidence of colorectal cancer. Telemark PolypStudy I. Scand J Gastroenterol 1999;34:414–420.
43. Hoff G, Grotmol T, Skovlund E, Bretthauer M. Risk ofcolorectal cancer seven years after flexible sigmoidoscopyscreening: randomised controlled trial. BMJ 2009;338:b1846.
44. Atkin WS, Edwards R, Kralj-Hans I, Wooldrage K, Hart AR,Northover JM, et al. Once-only flexible sigmoidoscopyscreening in prevention of colorectal cancer: a multicentrerandomised controlled trial. Lancet 2010;375:1624–1633.
45. Prorok PC, Andriole GL, Bresalier RS, Buys SS, Chia D,Crawford ED, et al. Design of the Prostate, Lung, Colorectaland Ovarian (PLCO) Cancer Screening Trial. Control Clin Trials2000;21:273S–309S.
46. Winawer SJ, Zauber AG, Ho MN, O'Brien MJ, Gottlieb LS,Sternberg SS, et al. Prevention of colorectal cancer bycolonoscopic polypectomy. The National Polyp StudyWorkgroup. N Engl J Med 1993;329:1977–1981.
47. Citarda F, Tomaselli G, Capocaccia R, Barcherini S, Crespi M.Efficacy in standard clinical practice of colonoscopicpolypectomy in reducing colorectal cancer incidence. Gut2001;48:812–815.
48. Imperiale TF, Wagner DR, Lin CY, Larkin GN, Rogge JD,Ransohoff DF. Risk of advanced proximal neoplasms inasymptomatic adults according to the distal colorectalfindings. N Engl J Med 2000;343:169–174.
49. LiebermanDA,DeGarmoPL, FleischerDE, EisenGM,HelfandM.Patterns of endoscopy use in the United States. Gastroenterology2000;118:619–624.
159J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
50. Baxter NN, Goldwasser MA, Paszat LF, Saskin R, Urbach DR,Rabeneck L. Association of colonoscopy and death fromcolorectal cancer. Ann Intern Med 2009;150:1–8.
51. Brenner H, Hoffmeister M, Arndt V, Stegmaier C, AltenhofenL, Haug U. Protection from right- and left-sided colorectalneoplasms after colonoscopy: population-based study. J NatlCancer Inst 2010;102:89–95.
52. Sonnenberg A, Delco F, Inadomi JM. Cost-effectiveness ofcolonoscopy in screening for colorectal cancer.Ann Intern Med2000;133:573–584.
53. Winnan G, Berci G, Panish J, Talbot TM, Overholt BF,McCallum RW. Superiority of the flexible to the rigidsigmoidoscope in routine proctosigmoidoscopy. N Engl J Med1980;302:1011–1012.
54. Nelson DB, McQuaid KR, Bond JH, Lieberman DA, Weiss DG,Johnston TK. Procedural success and complications oflarge-scale screening colonoscopy. Gastrointest Endosc2002;55:307–314.
55. Pickhardt PJ. Incidence of colonic perforation at CTcolonography: review of existing data and implications forscreening of asymptomatic adults. Radiology 2006;239:313–316.
56. Warren JL, Klabunde CN, Mariotto AB, Meekins A, Topor M,BrownML, et al. Adverse events after outpatient colonoscopyin the Medicare population. Ann Intern Med 2009;150:849–857,W152.
57. Screening for colorectal cancer: U.S. Preventive Services TaskForce recommendation statement. Ann Intern Med 2008;149:627–637.
58. Etzioni R, Penson DF, Legler JM, di Tommaso D, Boer R, GannPH, et al. Overdiagnosis due to prostate-specific antigenscreening: lessons from U.S. prostate cancer incidencetrends. J Natl Cancer Inst 2002;94:981–990.
59. Bill-Axelson A, Holmberg L, RuutuM, HaggmanM, AnderssonSO, Bratell S, et al. Radical prostatectomy versus watchfulwaiting in early prostate cancer. N Engl J Med 2005;352:1977–1984.
60. Alibhai SM, Klotz LH. A systematic review of randomizedtrials in localized prostate cancer. Can J Urol 2004;11:2110–2117.
61. Andriole GL, Grubb III RL, Buys SS, Chia D, Church TR, FouadMN, et al. Mortality results froma randomized prostate-cancerscreening trial. N Engl J Med 2009;360:1310–1319.
62. Schroder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S,Nelen V, et al. Screening and prostate-cancer mortality in arandomized European study. N Engl J Med 2009;360:1320–1328.
63. Barry MJ. Screening for prostate cancer–the controversy thatrefuses to die. N Engl J Med 2009;360:1351–1354.
64. Wolf AM,Wender RC, Etzioni RB, Thompson IM, D'Amico AV,Volk RJ, et al. American Cancer Society guideline for the earlydetection of prostate cancer: update 2010. CA Cancer J Clin2010;60:70–98.
65. Hoogendam A, Buntinx F, de Vet HC. The diagnostic valueof digital rectal examination in primary care screening forprostate cancer: a meta-analysis. Fam Pract 1999;16:621–626.
66. Harris R, Lohr KN. Screening for prostate cancer: an update ofthe evidence for the U.S. Preventive Services Task Force. AnnIntern Med 2002;137:917–929.
67. Thompson IM, Ankerst DP, Chi C, Lucia MS, Goodman PJ,Crowley JJ, et al. Operating characteristics of prostate-specificantigen in men with an initial PSA level of 3.0 ng/ml or lower.JAMA 2005;294:66–70.
68. Draisma G, Boer R, Otto SJ, van der Cruijsen IW, Damhuis RA,Schroder FH, et al. Lead times and overdetection due toprostate-specific antigen screening: estimates from theEuropean Randomized Study of Screening for ProstateCancer. J Natl Cancer Inst 2003;95:868–878.
69. Tornblom M, Eriksson H, Franzen S, Gustafsson O, Lilja H,Norming U, et al. Lead time associated with screening forprostate cancer. Int J Cancer 2004;108:122–129.
70. Frankel S, Smith GD, Donovan J, Neal D. Screening forprostate cancer. Lancet 2003;361:1122–1128.
71. Screening for prostate cancer: U.S. Preventive Services TaskForce recommendation statement. Ann Intern Med 2008;149:185–191.
72. Smith RA, Cokkinides V, Eyre HJ. American Cancer SocietyGuidelines for the Early Detection of Cancer, 2005. CA Cancer JClin 2005;55:31–44; quiz 55–36.
73. Albertsen PC, Fryback DG, Storer BE, Kolon F, Fine J. Theimpact of co-morbidity on life expectancy among men withlocalized prostate cancer. J Urol 1996;156:127–132.
74. Piccirillo JF, Tierney RM, Costas I, Grove L, Spitznagel Jr EL.Prognostic importance of comorbidity in a hospital-basedcancer registry. JAMA 2004;291:2441–2447.
75. Walter LC, Covinsky KE. Cancer screening in elderly patients:a framework for individualized decision making. JAMA2001;285:2750–2756.
76. Fried LP, Kronmal RA, Newman AB, Bild DE, Mittelmark MB,Polak JF, et al. Risk factors for 5-year mortality in older adults.JAMA 1998;279:585–592.
77. Ganguli M, Dodge HH, Mulsant BH. Rates and predictors ofmortality in an aging, rural, community-based cohort: therole of depression. Arch Gen Psychiatry 2002;59:1046–1052.
78. Walter LC, Brand RJ, Counsell SR, Palmer RM, Landefeld CS,Fortinsky RH, et al. Development and validation of aprognostic index for 1-year mortality in older adults afterhospitalization. JAMA 2001;285:2987–2994.
79. Walter LC, Lindquist K, Nugent S, Schult T, Lee SJ, CasadeiMA, et al. Impact of age and comorbidity on colorectal cancerscreening among older veterans. Ann Intern Med 2009;150:465–473.
80. Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development andvalidation of a prognostic index for 4-year mortality in olderadults. JAMA 2006;295:801–808.
81. National Center for Health Statistics. Life Tables of the UnitedStates. In; 1997.
82. Autier P, Hery C, Haukka J, Boniol M, Byrnes G. Advancedbreast cancer and breast cancer mortality in randomizedcontrolled trials on mammography screening. J Clin Oncol2009;27:5919–5923.
83. Gotzsche PC, Nielsen M. Screening for breast cancer withmammography. Cochrane Database Syst Rev 2006:CD001877.
84. Andersson I, Nystrom L. Mammography screening. J NatlCancer Inst 1995;87:1263–1264.
85. Bjurstam N, Bjorneld L, Warwick J, Sala E, Duffy SW, NystromL, et al. The Gothenburg Breast Screening Trial. Cancer2003;97:2387–2396.
86. Moss SM, Cuckle H, Evans A, Johns L, Waller M, Bobrow L.Effect of mammographic screening from age 40 years onbreast cancer mortality at 10 years' follow-up: a randomisedcontrolled trial. Lancet 2006;368:2053–2060.
87. MillerAB, ToT,BainesCJ,Wall C.TheCanadianNationalBreastScreening Study-1: breast cancer mortality after 11 to 16 yearsof follow-up. A randomized screening trial of mammographyin women age 40 to 49 years. Ann Intern Med 2002;137:305–312.
88. Miller AB, To T, Baines CJ, Wall C. Canadian National BreastScreening Study-2: 13-year results of a randomized trial inwomen aged 50–59 years. J Natl Cancer Inst 2000;92:1490–1499.
89. Roberts MM, Alexander FE, Anderson TJ, Chetty U, DonnanPT, Forrest P, et al. Edinburgh trial of screening for breastcancer: mortality at seven years. Lancet 1990;335:241–246.
90. Kosters JP, Gotzsche PC. Regular self-examination or clinicalexamination for early detection of breast cancer. CochraneDatabase Syst Rev 2003:CD003373.
91. Screening for breast cancer: recommendations and rationale.Ann Intern Med 2002;137:344–346.

160 J O U R N A L O F G E R I A T R I C O N C O L O G Y 2 ( 2 0 1 1 ) 1 4 9 – 1 6 0
92. Semiglazov VF, Moiseenko VM, Manikhas AG, Protsenko SA,Kharikova RS, Popova RT, et al. Role of breast self-examinationin early detection of breast cancer: Russia/WHO prospectiverandomized trial in St. Petersburg. Cancer Strategy 1999;1:145–151.
93. Pisani P, Parkin DM, Ngelangel C, Esteban D, Gibson L, MunsonM, et al. Outcome of screening by clinical examination of thebreast in a trial in the Philippines. Int J Cancer 2006;118:149–154.
94. http://cancercontrol.cancer.gov/grants/abstract.asp?applid=6965060 NCICcrAa.
95. Boulos S, Gadallah M, Neguib S, Essam E, Youssef A, Costa A,et al. Breast screening in the emergingworld: high prevalenceof breast cancer in Cairo. Breast 2005;14:340–346.
96. Atkin W, Kralj-Hans I, Wardle J, Duffy S. Colorectal cancerscreening. Randomised trials of flexible sigmoidoscopy. BMJ2010;341:c4618.
97. Gatto NM, Frucht H, Sundararajan V, Jacobson JS, Grann VR,Neugut AI. Risk of perforation after colonoscopy andsigmoidoscopy: a population-based study. J Natl Cancer Inst2003;95:230–236.
98. Saito H, Soma Y, Koeda J, Wada T, Kawaguchi H, Sobue T,et al. Reduction in risk of mortality from colorectal cancer byfecal occult blood screening with immunochemicalhemagglutination test. A case-control study. Int J Cancer1995;61:465–469.
99. Saito H, Soma Y, NakajimaM, Koeda J, Kawaguchi H, KakizakiR, et al. A case-control study evaluating occult bloodscreening for colorectal cancer with hemoccult test and an
immunochemical hemagglutination test. Oncol Rep 2000;7:815–819.
100. http://clinicaltrials.gov/ct2/results?term=NCT00906997.101. http://www.clinicaltrials.gov/ct2/results?
term=NCT00883792.102. Whitlock EP, Lin JS, Liles E, Beil TL, Fu R. Screening for
colorectal cancer: a targeted, updated systematic review forthe U.S. Preventive Services Task Force. Ann Intern Med2008;149:638–658.
103. Muller AD, Sonnenberg A. Protection by endoscopy againstdeath from colorectal cancer. A case-control study amongveterans. Arch Intern Med 1995;155:1741–1748.
104. Levin TR, Zhao W, Conell C, Seeff LC, Manninen DL, ShapiroJA, et al. Complications of colonoscopy in an integratedhealth care delivery system. Ann Intern Med 2006;145:880–886.
105. Rabeneck L, Paszat LF, Hilsden RJ, Saskin R, Leddin D,Grunfeld E, et al. Bleeding and perforation after outpatientcolonoscopy and their risk factors in usual clinical practice.Gastroenterology 2008;135:1899–1906, 1906 e1891.
106. AroraG,MannalitharaA,SinghG,GersonLB,TriadafilopoulosG.Risk of perforation from a colonoscopy in adults: a largepopulation-based study. Gastrointest Endosc 2009;69:654–664.
107. Lin OS, Kozarek RA, Schembre DB, Ayub K, Gluck M, DrennanF, et al. Screening colonoscopy in very elderly patients:prevalence of neoplasia and estimated impact on lifeexpectancy. JAMA 2006;295:2357–2365.
108. http://clinicaltrials.gov/ct2/results?term=NCT01200303.