Embed Size (px)
Citation preview

Published OnlineFirst January 6, 2011.Cancer Res Kenji Kawada and Makoto Mark Taketo Cancer ProgressionSignificance and Mechanism of Lymph Node Metastasis in
Updated version
10.1158/0008-5472.CAN-10-3277doi:
Access the most recent version of this article at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

1
Review
Significance and Mechanism of Lymph Node Metastasis in Cancer Progression
Kenji Kawada and Makoto Mark Taketo
Abstract
The effect of local therapy, such as surgical lymph node (LN) dissection and radiotherapy,
on the survival of cancer patients has been debated for decades. Several lines of recent
clinical evidence support that LN metastasis plays significant roles in systemic
dissemination of cancer cells, although the effects of surgical LN dissection on survival was
downplayed historically because of controversial data. Molecular studies of LN metastasis
suggest that the microenvironment within LNs, including chemokines and
lymphangiogenesis, can mediate the metastatic spread to the sentinel LNs, and beyond. It
has been demonstrated that chemokine receptor CXCR3 is involved in LN metastasis, and
its inhibition may improve patient prognosis. Although it remains to be determined whether
local therapy is best pursued through LN dissection or through a combination of resection
with radiation, prevention of regional metastases is an important goal in the treatment of
cancer patients to achieve a better survival.
Autors’ affiliation: Departments of Surgery and Pharmacology, Kyoto University Graduate
School of Medicine, Kyoto, Japan
Corresponding Author: Makoto Mark Taketo, Kyoto University Graduate School of Medicine
(Pharmacology), Yoshida-Konoé-cho, Sakyo, Kyoto 606-8501, Japan. Phone: +81-75-753-4391;
Fax, +81-75-753-4402; E-mail, [email protected]
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

2
Patients with advanced cancers have a significant risk of local recurrence and distant metastasis
after surgical resections of the primary tumors. Systemic therapy to prevent distant metastasis
has been emphasized to improve the survival of cancer patients, but the effect of local therapy
has been debated for decades, as reviewed by Punglia et al. (1) and summarized below. The most
frequently used strategy to control local recurrence includes radical resection combined with LN
dissection (lymphadenectomy) and local radiation therapy. Regarding local therapy, three clinical
viewpoints have been proposed. In the early last century, William Halsted proposed that breast
cancer is a local disease that spreads primarily in a predictable, stepwise manner from the
primary tumor to the regional lymphatics and then systemically to distant organs (2). Local
regional LNs are the commonest and earliest site of metastasis of solid tumors, and his idea
provided the justification for radical breast-cancer surgery with extended LN dissection (2). In
reaction to the “Halstedian” theory, the “systemic” theory arose. Bernard Fisher and others
proposed the view that breast cancer is a systemic disease from the beginning and that LN
dissection is merely useful for prognostic information, but does not affect overall survival,
suggesting more important role of hematogenous dissemination to vital organs (liver, lungs etc.)
in metastasis (3). Thus, effective systemic therapies were emphasized in breast-cancer treatment,
which indeed helped to improve the overall survival. As a third hypothesis, the “spectrum”
theory balanced these two opposing strategies (4). Cancer cells develop metastatic potential as
tumors grow through their clinical evolution. Accordingly, the LN involvement is of prognostic
importance not only because it indicates a more malignant tumor biology, but also because
persistent disease in LNs can be the source of subsequent fatal metastases. In fact, results of
some recent clinical trials support this notion. Namely, improved local therapy is causally
associated with better overall survival in several types of cancer as exemplified below.
1) Evidence from clinical trials a) Breast cancer: Two (i.e., Canadian and Danish) prospective randomized trials demonstrated
that, after mastectomy, the addition of radiation therapy and adjuvant chemotherapy not only
decreased local recurrence but also improved overall survival, indicating that local treatment
prevents recurrence from generating fatal metastases (5, 6). A recent meta-analyses also
presented the findings from 78 randomized clinical trials that improved local control during first
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

3
5 years resulted in a statistically significant improvement in the overall survival at 15 years, and
that the survival benefit was similar either by extensive surgery or by radiation therapy (7).
With the widespread introduction of the sentinel LN biopsy procedure, the question was
raised about how to deal with potential and additional LN metastases in case of a positive
sentinel LN. Micrometastases in regional LNs were associated with a reduced disease-free
survival with early-stage breast cancer (8). To investigate differences in regional control, survival,
and long-term morbidity between axillary LN dissection and radiation therapy, an international
multicenter phase III trial was initiated in 2001, and is still ongoing (9).
b) Gastric cancer: The need for radical LN dissection for curative treatment of gastric cancer
continues to be debated. Two large randomized trials from the Netherlands and UK that
compared the less extended D1 dissection (lymphadenectomy limited to the perigastric LNs)
with the D2 dissection (lymphadenectomy extended to hepatic, gastric, cardiac and splenic LNs )
failed to show a survival benefit for the D2 procedure (10, 11). In these studies, however, lack of
experience with the surgical skills and postoperative care appeared responsible for the high
morbidity (~45%) and mortality (~12%) of the patients who underwent D2 dissection (Table 1).
The American Intergroup study showed that chemoradiotherapy after no or limited
lymphadenectomy (D0 or D1 dissection) decreased the local recurrence rate and increased
overall survival, suggesting that chemoradiotherapy eliminated the residual LN metastases that
could be removed by D2 dissection (12). In 2006, a prospective randomized trial in Taiwan
showed a significant benefit in overall survival for a D2 dissection over D1 alone, without
increased operative mortality (13). In this trial, all the surgeons had already performed at least 80
D2 operations, and there were no deaths in either group (Table 1). In a surgical trial to compare
two different operative methods, participating surgeons should be experienced equally in both
techniques. These results suggest that adequate local treatment is essential for effective treatment
of gastric cancer.
In 2008, a prospective randomized trial in Japan showed no improvement in overall
survival with D2 dissection plus para-aortic nodal dissection (PAND) as compared with D2 alone.
This trial was performed by experienced surgeons in 24 specialized hospitals with a high volume
of cases, and resulted in very low mortality rates (0.8%) and good long-term survival in both
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

4
groups (14). The result may suggest that para-aortic LN metastasis is a systemic, not local,
disease, and that PAND is an unworthy and excessive procedure against advanced gastric
cancers.
c) Rectal cancer: In the United States, extended LN dissection in rectal cancer was performed in
the 1950s, but the effectiveness of lateral pelvic LN dissection was not accepted because it led to
an increase in blood loss, and urinary and sexual dysfunctions without further survival benefit
(15). Preoperative radiotherapy reduced the relative risk of local recurrence, although without
significant survival improvement (16, 17). Although a recent meta-analysis comparing extended
and non-extended lymphadenectomy of the lateral pelvic LN showed no overall difference in
cancer-specific outcome (18), this study has limitations such as varying protocols, different
levels of surgical expertise, different patient populations and different time periods. In many
Western countries, current standard therapy for lower rectal cancer is total mesorectal excision
(TME) with preoperative radiotherapy.
In Japan, on the other hand, lateral pelvic LN dissection has been performed extensively
along with TME in advanced rectal cancer, which contributed to the reduced local recurrence and
improved survival in retrospective multicentre studies (19). A retrospective analysis suggests that
lateral pelvic LN dissection can be equivalent to the preoperative radiotherapy in terms of the
curative effect for patients with lower rectal cancers (20). It is worth noting that a phase III
prospective randomized trial is ongoing, assessing the effectiveness of lateral pelvic LN
dissection (JCOG 0212).
Similar situations have been reported for lung cancer (21), endometrial cancer (22) and
esophageal cancer (23, 24). In stage I-IIIA non-small cell lung cancer, a meta-analysis of
randomized controlled trials suggests that complete mediastinal LN dissection is associated with
improved survival (21). In endometrial cancer, comparative cohort study reports that para-aortic
LN dissection (PAND) has survival benefits, and that pelvic LN dissection alone might be an
insufficient surgical procedure for patients at intermediate or high risk of recurrence (22). In
adenocarcinoma of the esophagus, one randomized controlled trial suggests that in patients with
1 to 8 metastatic LNs, extended transthoracic esophagectomy with en bloc LN dissection results
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

5
in improved 5-year survival compared with limited transhiatal resection (23). On the other hand,
in pancreatic cancer, 3 randomized controlled trials suggest that extended LN dissection does not
result in survival benefit (25-27). Although there is no doubt that the presence of LN metastases
worsens prognosis of a patient, unambiguous evidence to support LN dissection is still lacking.
For many solid tumors, the role of LN dissection is yet controversial, and may depend on the
tumor type and the stage of patient presentation for diagnosis. Namely, cancers of the breast,
colon and stomach are often diagnosed as local diseases, whereas pancreatic cancer is found after
they have progressed to the systemic diseases. Accordingly, well-designed randomized controlled
trials are required to evaluate the systemic vs. local therapy in a scientific manner.
2) Molecular mechanisms of LN metastasis Cancer metastasis appears to form through a chain of events where organ selectivity by the tumor
cells is largely determined by physical factors (blood and lymph flows) and biological molecules
that are expressed in the tumor microenvironment. As described above, several lines of evidence
are beginning to show that LN metastasis not only provides the prognostic information, but also
plays active roles in developing distant metastases to the vital organs, causing eventual lethality.
However, little is known about its molecular mechanisms. Questions remain whether tumor cells
are trapped by LNs, causing a lag phase in tumor dissemination, whether LN metastases just
serve as evidence of tumor cell transit through the LNs, or whether the LNs promote spreading
of the tumor cells by amplifying them and serving as a launch pad for further systemic metastasis
(28, 29). As the lymph flows into the systemic circulation through the thoracic duct or
lymphovascular shunts, LN metastasis can be regarded as a side loop of the hematogenous
metastasis circuit.
Recent studies suggest that the least efficient steps in metastasis are the survival and
growth of the micrometastatic foci and their persistence that affect colonization, indicating the
importance of interactions between the ‘seed’ (cancer cell) and ‘soil’ (microenvironment). Of the
different components that affect the organ selectivity, instrumental roles have been attributed to
interactions between chemokine receptors on cancer cells and their ligands in the target organs
(30). To date, several sets of chemokines and their receptors have been suggested to play
important roles in the matastatic organ selectivity, and one of the best-studied examples is the
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

6
CXCL12-CXCR4 axis in breast cancer metastasis to the bone. Regarding the direct role of
chemokines in LN metastasis, recent reports suggest critical roles for CXCR3, CXCR4 and
CCR7 (31-34). Importantly, these three receptors are involved in the recruitment and patterning
of several types of immune cells to LNs, suggesting that cancer cells often acquire these
receptors and are controlled by their ligands in a manner analogous to the immune cell
interactions.
Although early studies to describe chemokine receptors and melanoma or breast cancer
did not detect receptor CXCR3, it has been demonstrated recently that CXCR3 plays the critical
role in LN metastasis of melanoma and colon cancer cells, but not in their hematogenous
metastasis (31, 32). Upon construction of B16F10 mouse melanoma cell derivatives with
reduced CXCR3 expression by antisense RNAs, their metastatic activities have been investigated
after subcutaneous inoculations into mouse footpads. The metastatic frequency of these cells to
popliteal LNs was markedly reduced compared with control B16F10 cells, without affecting
hematogenous metastasis to the lung or liver. In addition, human colon cancer cells were
constructed that expressed CXCR3 cDNA (DLD-1-CXCR3), and compared with controls by
rectal transplantation in nude mice. In 6 weeks, 59% of mice inoculated with DLD-1-CXCR3
showed macroscopic metastases in para-aortic LNs, whereas only 14% of those did with the
control. Metastasis to the liver or lung was rare, and unaffected by CXCR3 expression.
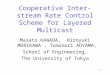
In 92 human colon cancer specimens, expression of CXCR3 was found in 31 (33.7%)
cases, most of which had LN metastasis (32). Importantly, the patients with CXCR3-positive
colon cancer showed significantly shorter survivals than those without CXCR3. The patients
with CXCR4-positive tumors also had a significant poorer prognosis, but its effect was less than
that of CXCR3. In addition, the patients with tumors double positive for CXCR3 and CXCR4
had a significantly poorer prognosis than those with tumors positive only for CXCR4 or the
double negatives (Figure 1). In breast cancer, high CXCR3 expression has also been reported to
be associated with poorer prognosis (35). These results demonstrate that activation of CXCR3
stimulates cancer metastasis preferentially to the draining LNs with poorer prognosis,
implicating a critical role of LN metastasis in overall patient survival (32).
More results have emerged recently in support of the role for CXCR3 in the metastasis
of melanoma and neuroblastoma, and cancers of colon, breast, ovaries, and prostate. Namely,
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

7
several laboratories have provided data that CXCR3 strengthens the invasion-related properties
of cancer (36) and that CXCR3 facilitates lung metastasis of breast and colon cancers (37, 38). In
addition, lymphangiogenesis within the sentinel LNs is also associated with tumor metastasis to
distant sites (39). These results indicate that the microenviornment in LNs, including chemokines
and lymphangiogenesis, can mediate the metastatic spread of tumor cells to the sentinel LNs, and
beyond.
For decades, the oncology community has focused on adjuvant therapies in an effort to
prevent distant metastasis. Although the effects of local recurrence on patient survival was
downplayed, or even denied, prevention of local recurrence is getting to be appreciated as a key
goal for many types of cancer. In the meantime, it is yet to be determined whether regional
treatment of cancer is best pursued through LN dissection or a combination of resection with
radiation. It is also worth noting that economic factors on the health insurance system need to be
evaluated carefully in establishing the therapeutic strategy on metastasis. We should be able to
overcome tumor metastasis with a better understanding of the interplay between the cancer cells
and their microenvironment not only in hematogenous but also LN metastasis.
Acknowledgment. Authors thank Masahiro Aoki for comments on the manuscript. The results
quoted from the authors papers were supported by grants from MEXT, Japan, and by
Littlefield-AACR colon cancer metastasis research grant (to MMT).
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

8
References
1. Punglia RS, Morrow M, Winer ER, et al. “Local therapy and survival in breast cancer” N.
Engl. J. Med.2007.356:2399-405.
2. Halsted WS. “The results of radical operations for the cure of carcinoma of the breast”
Ann.Surg.1907.46:1-19.
3. Fisher B. “Laboratory and clinical research in breast cancer – A personal adventure: The
David A. Karnofsky Memorial Lecture” Cancer Res.1980.40:3863-3874.
4. Hellman S. “Karnofsky Memorial Lecture: natural history of small breast cancers”
J.Clin.Oncol.1994.12:2229-2234.
5. Ragaz J, Jackson SM, Le N, et al. “Adjuvant radiotherapy and chemotherapy in
node-positive premenopausal women with breast cancer” N.Engl.J.Med.1997.337:956-962.
6. Overgaard M, Hansen PS, Overgaar J, et al. “Postoperative radiotherapy in high-risk of
premenopausal women with breast cancer who receive adjuvant chemotherapy”
N.Engl.J.Med.1997.337:949-955.
7. Clarke M, Collins R, Darby S, et al. “Effects of radiotherapy and of differences in the
extent of surgery for early brest cancer on local recurrence and 15-year survival: an overview
of the randomized trials.” Lancet.2005.366:2087-2106.
8. de Boer M, van Deurzen CH, van DijckJA, et al. “Micrometastases or isolated tumor cells
and the outcome of breast cancer” N.Engl.J.Med.2009.361:653-663.
9. Straver ME, Meijnen P, van Tienhoven G, et al. “Role of axillary clearance after a
tumor-positive sentinel node in the administration of adjuvant therapy in early breast cancer”
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

9
J.Clin.Oncol.2010.28:731-737.
10. Bonenkamp JJ, Hermans J, Sasako M, et al. “Extended lymph-node dissection for gastric
cancer” N.Engl.J.Med.1999.340:908-914.
11. Cuschieri A, Weeden S, Fielding J, et al. “Patient survival after D1 and D2 resections for
gastric cancer: long-term results of the MRC randomized surgical trial” Br J
Cancer.1999.79:1522-1530.
12. Macdonald JS, Smalley SR, Benedetti J, et al. “Chemoradiotherapy after surgery compared
with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction”
N.Engl.J.Med.2001.345:725-730.
13. Wu CW, Hsiung CA, Lo SS, et al. “Nodal dissection for patients with gastric cancer: a
randomized controlled trial” Lancet Oncol.2006.7:309-315.
14. Sasako M, Sano T, Yamamoto S, et al. “D2 lymphadenectomy alone or with para-aortic
nodal dissection for gastric cancer” N.Engl.J.Med.2008.359:453-62
15. Stearns MW Jr, and Deddish MR. “Five-year results of abdominopelvic lymph node
dissection for carcinoma of the rectum” Dis Colon Rectum.1959.2:169-172.
16. Kapiteijn E, Marijnen CA, Nagtegaal ID, et al. “Preoperative radiotherapy combined with
total mesorectal excision for resectable rectal cancer” N.Engl.J.Med.2001.345:638-646.
17. Sebag-Montefiore D, Stephens RJ, Steele R, et al. “Preoperative radiotherapy versus
selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and
NCIC-CTG C016): a multicentre randomized traial” Lancet.2009.373:811-820.
18. Georgiou P, Tan E, Gouvas N, et al. “Extended lynphadenectomy versus conventional
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

10
surgery for rectal cancer: a meta-analysis” Lancet Oncol. 2009. 10:1053-1062.
19. Kobayashi H, Mochizuki H, Kato T, et al. “Outcomes of surgery alone for lower rectal
cancer with and without pelvic sidewall dissection” Dis Colon Rectum.2009.52:567-576.
20. Watanabe T, Tsurita G, Muto T, et al. “Extended lymphadenectomy and preoperative
radiotherapy for lower rectal cancers” Surgery.2002.132:27-33.
21. Wright G, Manser RL, Byrnes G, et al. “Surgery for non-small cell lung cancer: systematic
review and meta-analysis of randomized controlled trials” Thorax.2006.61:597-603.
22. Todo Y, Kato H, Kaneuchi M, et al. “Survival effect of para-aortic lymphadenectomy in
endometrial cancer (SEPAL study) : a retrospective cohort analysis” Lancet. 2010.375:1165-72.
23. Omloo JM, Lagarde SM, Hulscher JB, et al. “Extended transthoracic resection compared
with limited transhiatal resection for adenocarcinoma of the mid/distal esophagus: Five-year
survival of a randomized clinical trial” Ann Surg.2007.246:992-1000.
24. Jamieson GG, Lamb PJ and Thompson SK. “The role of lymphadenectomy in esophageal
cancer” Ann Surg.2009.250:206-209.
25. Pedrazzoli S, DiCarlo V, Dionigi R, et al. “Standard versus extended lymphadenectomy
associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head
of the pancreas” Ann Surg.1998.228:508-517.
26. Yeo CJ, Cameron JL, Lillemoe KD, et al. “Pancreaticoduodenectomy with or without distal
gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocaccinoma,
part2” Ann Surg.2002.236:355-368.
27. Farnell MB, Pearson RK, Sarr MG, et al. “A prospective randomized trial comparing
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

11
standard pancreatoduodenectomy with pancreatoduedenectomy with extended lymphadenectomy
in respectable pancreatic head adenocarcinoma” Surgery.2005.138:618-30.
28. Sleeman JP and Thiele W. “Tumor metastasis and the lymphatic vasculature”
Int.J.Cancer.2009.125:2747-2756.
29. Joyce JA, and Pollard JW. “Microenvironmental regulation of metastasis”
Nat.Rev.Cancer.2009.9:239-252.
30. Balkwill F. “Cancer and the chemokine network” Nat Rev Cancer.2004.4:540-550.
31. Kawada K, Sonoshita M, Sakashita H, et al. “Pivotal role of CXCR3 in melanoma cell
metastasis to lymph nodes” Cancer Res.2004.64.4010-4017.
32. Kawada K, Hosogi H, Sonoshita M, et al. “Chemokine receptor CXCR3 promotes colon
cancer metastasis to lymph nodes” Oncogene.2007.26.4679-4688.
33. Müller A, Homey B, Soto H, et al. “Involvement of chemokine receptors in breast cancer
metastasis” Nature.2001.410:50-56.
34. Wiley HE, Gonzalez EB, Maki W, et al. “Expression of CC chemokine receptor-7 and
regional lymph node metastasis of B16 murine melanoma” J Natl Cancer
Inst.2001.93:1638-1643.
35. Ma X, Norsworthy K, Kundu N, et al. “CXCR3 expression is associated with poor survival
in breast cancer and promotes metastasis in a murine model” Mol Cancer Ther.2009.8:490-498.
36. Zipin-Roitman A, Meshel T, Sagi-Assif O, et al. “CXCL10 promotes invasion-related
properties in human colorectal carcinoma cells” Cancer Res.2007.67:3396-405.
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

12
37. Walser TC, Rifat S, Ma X, et al. “Antagonism of CXCR3 inhibits lung metastasis in a
murine model of metastatic breast cancer” Cancer Res.2006.66:7701-7.
38. Cambien B, Karimdjee BF, Richard-Fiardo P, et al. “Organ-specific inhibition of metastatic
colon carcinoma by CXCR3 antagonism” Br J Cancer.2009.100:1755-64.
39. Hirakawa S, Brown LF, Kodama S, et al. “VEGF-C-induced lymphangiogenesis in sentinel
lymph nodes promotes tumor metastasis to distant sites” Blood.2007.109:1010-1017.
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

13
Table 1. Four randomized controlled trials of gastric cancer
No. of 5-year perioperative perioperative participating patients survival rate morbidity mortality surgeons/hospitals
Taiwan trial (13) single hospital 3 experienced surgeons
D2 /D3 111 59.5 %* 17 %** 0 %
D1 110 53.6 % 7 % 0 %
Dutch trial (10) 80 hospitals
D2 331 47 % 43 % ** 10 % **
D1 380 45 % 25 % 4 %
UK trial (11) 33 surgeons
D2 200 33 % 46 % ** 13 % ***
D1 200 35 % 28 % 6.5 %
Japan trial (14) 24 hospitals
D3 (D2+PAND) 259 70 % 28.1 % 0.8 %
D2 263 69 % 20.9 % 0.8 %
* P < 0.05 compared with D1 (log-rank test)
** P < 0.01 compared with D1 (Fisher’s exact test)
*** P < 0.05 compared with D1 (Fisher’s exact test)
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

14
Legend to Figure 1. Survival curve (Kaplan and Meier estimates) by expression of CXCR3 and
CXCR4 in colon cancer (27).
on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277

on April 23, 2014. © 2011 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on January 6, 2011; DOI: 10.1158/0008-5472.CAN-10-3277