Embed Size (px)
Citation preview

Cancer ProgramStatistical Report 2008
Accredited as a Community Hospital Comprehensive Cancer Center
Cleveland_Cancer Report_2010_FNL.indd 1 5/3/10 12:26 PM

2
I’m proud to present the fifth annual Cancer Program Statistical Report reflecting 2008 data and activities
at Cleveland Clinic in Florida. The Program continues to grow: 878 patients were treated for cancer at our
institution in 2008 compared to 446 in 2004, 500 in 2005, 591 in 2006, and 740 in 2007. We continue to
add physicians and surgeons to our professional staff, who specialize in oncology and bring new and current
expertise to the care of our patients.
Our Cancer Program continues its commitment to provide comprehensive, quality, multidisciplinary, safe,
and patient oriented care to patients diagnosed with cancer. The Program provides clinical services adept
in the prevention, education, early diagnosis, pretreatment evaluation, staging, optimal treatment, rehabilita-
tion, and surveillance for recurrent disease, support services, and end-of-life care for our patients. Patients
referred to Cleveland Clinic for diagnosis, staging, and treatment of their cancers receive the advantages of
inpatient areas dedicated only for the care of cancer patients, an outpatient chemotherapy infusion unit, the
invitation to participate in clinical research trials, and a Cancer Prevention Clinic that offers genetic testing,
family phenotyping, and counseling.
This report will update you on the activity of our cancer services, weekly cancer conferences, quality im-
provement program, cancer registry and database, community outreach programs, patient education and
support groups, and ongoing clinical trials.
The Cancer Committee has chosen to review thyroid cancer in this year’s report. Clinically recognized thyroid
carcinomas constitute less than 1 percent of all human malignancies. However, its incidence has more than
doubled since the 1970’s now making thyroid cancer as prevalent as multiple myeloma, twice as common
as Hodgkin’s disease, and comparable in frequency to cancers of the esophagus, larynx, mouth, and uterine
cervix. Among women, it’s the cancer with the fastest rising number of new cases per year. Thyroid cancer
is the most common endocrine malignancy, comprising 90 percent, and is responsible for more deaths than
all other endocrine cancers combined. At Cleveland Clinic Florida, endocrinologists certified in ultrasound
and radionuclide administration, surgeons expert in endocrine surgery, oncologists, radiation oncologists,
and interventional radiologists work together to ensure the patient receives only the most current and safest
management. Our multidisciplinary approach has resulted in excellent patient outcomes and established
Cleveland Clinic Florida as one of the leaders in the region for the treatment of thyroid disease.
It is my pleasure to present this Report for your review. The Cancer Committee is proud of the strides we
continue to make for our patients ensuring that they continue to receive the best, safest, and most personal-
ized care possible.
Mark E. Sesto, MD, FACS
Cancer Committee Chairman
Cancer Committee Chairman’s Report
Mark E. Sesto, MD, FACS
Cleveland_Cancer Report_2010_FNL.indd 2 5/3/10 12:26 PM

CANCER PROGRAM I STATISTICAL REPORT 2008 3
Mark E. Sesto, MD, FACS, Chairman, General and Oncologic Surgery
Elizabeth Stone, MD, Cancer Liaison Physician, Medical Oncology
Christopher Chen, MD, Quality Control Coordinator, Radiation Oncology
Chieh-Lin Fu, MD, Quality Improvement Coordinator, Hematology
Maria Artze, MD, Radiology
Bruno Bastos, MD, Hematology Oncology
Mariana Berho, MD, Pathology
Viviana Boronat, MD, Clinical Research
Egbert de Vries, MD, Otolaryngology
Margaret Gilot, MD, Breast Surgical Oncology
James Hoffman, MD, Hematology Oncology
Nicolas Muruve, MD, FACS, Urology
Carron Bramwell, Director of Telemetry
Daphne Bautista, Oncology Services
Pablo Davidov, Director of Clinical Research
Lee Ghezzi, Director of Quality Assurance
Mohammed Ibrahim, Pharmacy
Cara Kondaki, LCSW, ACSW, Oncology Social Worker
Kelly Large, CTR, Cancer Registry Coordinator
Kerry Major, Chief Nursing Officer
Mary Ellen Osiecki, Director of Surgical Services, Pain Management
Melinda Scott, Cancer Registry
Sonia Wisdom, MSN, CCRN, Director Medical Surgical Department
Diagnostic Imaging Services
- Digital Mammography
- MRI/Breast MRI
- CT/PET Scanning
Double balloon small bowel enteroscopy
Endoscopic Ultrasound, gastrointestinal
and tracheo-bronchial
Enterostomal Therapy
Hereditary Prevention Clinic/
Genetic Testing
Home Health
Hospice
Invasive Radiology Services
- Stereotactic/Ultrasound Guided Core
Needle Breast Biopsies
Laboratory
Nutritional Services
Oncology Social Services
Outpatient Services
Pain Management
Pastoral Care
Pharmacy
Photodynamic Therapy
Rehabilitation
Special Transportation
Wound Care
- Chemoembolization of Liver Tumors
- CT Guided Radiofrequency Ablation
CANCER COMMITTEE
HOSPITAL SERVICES
The multidisciplinary Cancer Committee provides the leadership for our Cancer Program and assures optimal patient care by en-suring compliance with the American College of Surgeons Cancer Program Standards, and by initiating plans for improvement and change. The Committee is composed of multidisciplinary staff physicians as well as allied health professionals involved in cancer patient care.
Cleveland_Cancer Report_2010_FNL.indd 3 5/3/10 12:26 PM

4
The Department of Oncology at Cleveland Clinic Florida continues to strive for compassionate, quality
care using a multidisciplinary, integrated approach. Our commitment to providing innovate social service
programs and strong community outreach, remains a top priority for our team.
We offer interactive support groups for our cancer patient’s and families including “Reel to Real” a movie
support group for our blood cancer patients. The Hematology-Oncology Department, in partnership with
the Leukemia and Lymphoma Society, provide education and support for Leukemia, Lymphoma and My-
eloma patients in our community. Our Breast Cancer Book Club recently celebrated its fourth anniversary.
They remain a strong group and volunteer frequently at Cleveland Clinic to support our breast cancer
initiatives. We have sponsored several American Cancer Society “I Can Cope” programs in the past year,
including “Eating Well for the Cancer Patient” and a “Caring for the Cancer Caregiver” program. We have
also partnered with the International Myeloma Foundation to sponsor two community outreach programs
for updates and education for Multiple Myeloma patients. Our support groups with the American Cancer
Society include monthly “Look Good Feel Better” classes for our chemotherapy patients and a “Man-to-
Man” prostate cancer support group.
In the past year the Oncology Department continued to implement several mentoring programs within
our community. Girl Scout Troop 10182 and 10577 of Weston completed a “Heart to Heart” community
service project to provide personalized decorative tote bags for our chemotherapy infusion suite. Our
Breast Cancer Book Club continued it’s partnership with Girl Scout Troop 95 of Coral Springs, a Cadette
troop in our community. The girls worked with our support group members to begin their Silver Project
which will support the American Cancer Society’s “Look Good Feel Better” programs in Broward County.
The department also was the recipient of an Eagle Scout project from Raymond Gonzales of Boy Scout
Troop 246 to provide new bookshelves in our chemotherapy suite.
With the American Cancer Society, Cleveland Clinic Florida also participated in the annual Relay for Life
and sponsored their kick-off and wrap-up events for the third year in a row. For the last ten years the
Oncology Department has led a team and walked in the Making Strides Against Breast Cancer walk. We
were very proud to be named the #1 team in Broward County for Making Strides Against Breast Cancer,
raising over $10,000 for breast cancer research and support!
Our department continues to sponsor community education outreach programs. In September we initiated
a community outreach table in honor of Prostate Cancer Awareness month, supported by our Man to Man
support group along with the American Cancer Society. During National Breast Cancer Awareness month
in October, several breast cancer survivors ran our fourth annual community outreach table to provide
education on the importance of monthly self-breast exams and yearly mammograms. And, in November,
National Lung Cancer awareness month, we manned our second annual smoking cessation, education and
community referrals table.
The Oncology social worker serves as a link between the cancer patient and the healthcare system, as well
as the community. The Department of Oncology continues to strive for excellence in providing innovative
programs, as well as offering a variety of services, to aide the patient, their family and caregivers with their
long term adjustment to a cancer diagnosis. At Cleveland Clinic Florida our goal is to provide patient- and
family-centered care and put “Patient’s First”.
Community Outreach
Elizabeth Stone, MDMedical Oncologist
Cara S. Kondaki, LCSW, ACSWOncology Social Worker
Cleveland_Cancer Report_2010_FNL.indd 4 5/3/10 12:26 PM

CANCER PROGRAM I STATISTICAL REPORT 2008 5
BREAST Adjuvant Hormonal NSABP B42 8863 Stage I-IIIA ER/PR+completed 5yrs of hormonal therapy: Letrozole/placebo x 5yrsALTTO N063D 8992 Adjuvant lapatinib/trastuzumab in HER2/ErbB2(+) primary breast cancerOncotype Dx Assay PACCT-1 8881 Trial assessing individual options for breast cancer treatment
GI Colorectal. Metastatic CALGB 80405 8902 First line, FOLFOX or FOLFIRI plus Cetuximab or Bevacizumab every 2 weeks. Colon. Adjuvant E 5202 8944 High risk (5-FU, Leucovorin and Oxaliplatin +/- bevacizumab) Low risk (observation)
GU Prostate, High Risk CALGB 90203 9033 Neoadjuvant and Androgen Deprivation prior prostatectomy vs. immediate prostatectomy in high risk clinically localized prostate cancer. Renal Cell, adjuvant CTSU E-2805 8869 May be registered pre or post-surgery. T1b –T4, N0-2: Sunitinib vs. sorafenib vs placebo
LUNG NSCL Early Stages E 1505 8937 Stage IB-IIIA NSCLC chemo +/- bevacizumab
ANCILIARY Bone Loss Prevention CALGB 70604 9113 A Randomized, Phase III Study of Zoledronic Acid in Metastatic CancerPain Associated Neuropathy CALGB 170601 9115 A Phase III Double Blind Trial of Oral Duloxetine for Pain Chemotherapy-Induced Peripheral Neuropathy.
LYMPHOMA
NHL, untreated CALGB 50303 8883 Stage II/III/IV diffuse large B-cell: R-CHOP vs. dose adjusted EPOCH-R
Pharmaceutical Sponsored StudiesMDS Alexion 8810 Examination of PNH, by Level of CD59 on Red and white blood cells, in bone marrow failure syndromes (EXPLORE) ITP Grifols 9004 To assess the safety and the efficacy of a new intravenous immune globulin (IGIV31 Grifols 10%) in patients with idiopathic (immune) thrombocytopenic purpura.MM Novartis 9045 Bone Marker Directed Dosing of ZOMETA (zoledronic acid) for the Prevention of Skeletal Complications in Patients with Advanced Multiple Myeloma.NSCL Eli Lilly 8893 Non-small Cell Lung Cancer: The impact of Ethnic Origin on Patients being Treated Second Line with PemetrexedNSCL ACCORN 9109 A Multi-Center Randomized Phase 2b Study of Cetuximab (Erbitux®) in Combination with Platinum-Based Chemotherapy as First Line Treatment of Patients with Recurrent or Advanced Non-Small Cell Lung CancerBlood-based Assay BioTheme 8895 A Blood-based Diagnostic Assay for Human CancersAnticoagulation Pfizer CV057 9030 A Safety and Efficacy Trial Evaluating the Use of Apixaban for the Extended Treatment of Deep Vein Thrombosis and Pulmonary EmbolismAnticoagulation Pfizer CV056 9032 A Safety and Efficacy Trial Evaluating the Use of Apixaban in the
Treatment of Symptomatic Deep Vein Thrombosis and Pulmonary Embolism (Bristol-Myers Squibb with Pfizer, Inc.)
Oncology And Hematology Clinical Research Protocols
Hematology Studies
Cleveland_Cancer Report_2010_FNL.indd 5 5/3/10 12:26 PM

6
The Cancer Registry plays an integral role in the success of the Cleveland Clinic Flor-ida Cancer Program, providing data management services to meet mandatory state cancer reporting requirements, as well as those of the American College of Surgeons Commission on Cancer. The Cancer Registry maintains data on all cancer patients seen since January 1, 2004 and the data is made available to the medical staff for special studies, audits and research. Certified tumor registrars prepare anabstract for each patient using information from their medical record. Data includesdemographic information, diagnostic findings, histology, stage of disease, type oftreatment and survival information. The Registry also monitors follow-up of ourpatients through a lifetime tracking record.
The Cancer Committee physicians assist the Cancer Registry with quality control by chart review and are also the key members of weekly Cancer Conferences. Various types of malignancies are selected for presentation at Cancer Conference on the ba-sis of complexity, unusual manifestation of the disease or special interest.
The Conference format includes a complete presentation of medical history, physical findings, clinical course, radiographic studies and pathologic interpretation. Cancer Conferences are approved for one hour of Category 1 Continuing Medical Education credit. A total of forty Cancer Conferences were held in 2008 in a facility-wide format. A total of ninety-one cases were presented. The number of cases presented repre-sents 11% of the 2008 analytic caseload.
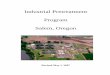
In 2008, a total of 878 new tumors were diagnosed and or treated in our hospital. The top five primary sites include Prostate, Breast, Lung & Bronchus, Colon & Rectum, and Thyroid. The following figure compares Cleveland Clinic’s percentage of cases to the rest of Florida, as well as the United States.
These figures were obtained from the 2008 Cancer Facts and Figures, published by the American Cancer society and may represent estimates.
Cancer Registry Report 2008
Kelly Large, CTRCancer Program Coordinator
Prostate
Breast
Colon & Rectum
Bronchus & Lung 8.1% 17.0% 15.0%
14.7% 10.7% 10.4%
8.5% 11.6% 12.7%
19.2% 11.2% 13.0%
Cleveland_Cancer Report_2010_FNL.indd 6 5/3/10 12:26 PM

CANCER PROGRAM I STATISTICAL REPORT 2008 7
Clinically recognized thyroid carcinomas constitute less than 1 percent of all human malignancies. The annual incidence of thyroid cancer varies worldwide from 0.5 to 10 per 100,000. However, to place its incidence in perspective, thyroid carcinoma is as prevalent as multiple myeloma, twice as common as Hodgkin’s disease, and com-parable in frequency to cancers of the esophagus, larynx, mouth, and uterine cervix. The incidence of thyroid cancer has more than doubled since the 1970’s. In 2009, ap-proximately 37,200 new cases will be diagnosed. Among women, it’s the cancer with the fastest rising number of new cases per year. Thyroid cancer is the most common endocrine malignancy, comprising 90 percent, and is responsible for more deaths than all other endocrine cancers combined.
Most patients with thyroid cancer first present with a thyroid nodule noted on exami-nation or found incidentally by an imaging study. Thyroid nodules are common with a prevalence of 4 to 7 percent in the United States. The vast majority are benign and do not require surgical treatment. The challenge in the evaluation and management of thy-roid nodules is to distinguish between the patients at high risk for cancer from those with benign disease who can be observed. It is particularly important to elicit a history of irradiation to the head and neck in childhood (papillary carcinoma) or iodine defi-ciency (follicular carcinoma). A linear relationship has been noted for the subsequent development of thyroid cancer following childhood exposure to external beam radio-therapy over a range of 5 to 1,000 cGy. In the past, these doses were achieved in children treated for tonsilar, thymic, or adenoid enlargement and for acne. In addition, nuclear accidents have exposed children to the deleterious effects of ionizing radia-tion. Certain familial syndromes are associated with thyroid cancer. Medullary thyroid cancer (MTC) occurs in Multiple Endocrine Neoplasia (MEN) IIA, MEN IIB, and familial MTC. Familial papillary carcinoma has been associated with Gardner’s syndrome.
The accuracy of ultrasound-guided fine needle aspiration cytology (FNA) has markedly diminished the role of other thyroid imaging studies in the initial evaluation of thyroid nodules. Imaging (ultrasound, radionuclide scintigraphy, CT, MRI, and PET) continues to play an important role in the evaluation of hyper-functioning nodules, locally inva-sive lesions, large fixed nodules, vocal cord paralysis, and in the follow-up of thyroid cancer. At Cleveland Clinic Florida, the Departments of Endocrinology and Pathology collaborate allowing for immediate review of the material obtained at biopsy by a cy-topathologist with expertise in the area of thyroid disease to determine if the sample is adequate for interpretation and rendering a reliable diagnosis. This approach allows for higher diagnostic accuracy and the fewest number of needle passes.
Thyroid Cancer 2008 Data
Vineeth Mohan, MDEndocrinologist
Mark E. Sesto, MD, FACS Cancer Committee Chairman
Cleveland_Cancer Report_2010_FNL.indd 7 5/3/10 12:26 PM

8
Thyroid Cancer 2008 Data
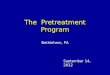
In 2008, 476 FNAs were performed by the phy-sicians in the Department of Endocrinology. The Cancer Committee directed a review comparing the 2008 FNA results to the surgical pathology re-sults, in patient’s who had both, for informational and quality purposes.
Of the twenty two FNAs interpreted as ‘benign’, none were found to be malignant on the final sur-gical pathology (100 percent accuracy). Of the twenty two FNAs interpreted as ‘malignant’, only two were found to be benign on the final surgical pathology (90 percent accuracy), one was follicu-lar hyperplasia (multinodular goiter) and the other a follicular adenoma. Of the twenty one FNAs inter-preted as ‘follicular neoplasm’, nine were benign (43 percent), six were follicular adenomas (28 per-cent), and six were cancers (28 percent), slightly higher than the expected 10 to 20 percent gener-ally accepted in the literature.
The Cleveland Clinic Florida data is consistent with national trends seen with thyroid cancer with a high incidence in younger patients and preponderance of relatively smaller papillary carcinomas.
Cleveland_Cancer Report_2010_FNL.indd 8 5/3/10 12:26 PM

CANCER PROGRAM I STATISTICAL REPORT 2008 9
The staging of thyroid cancer is unique in that histologic diagnosis and the age of the patient is included because of their prognostic importance. At least eight systems have been proposed and to a lesser or greater extent validated. It is recommended that the TNM staging system introduced by the International Union Against Cancer (IUCC) and pro-moted by the American Joint Committee on Cancer (AJCC), the American Cancer Society (ACS), the National Coopera-tive Cancer Network (NCCN), and the American College of Surgeons be adopted as the international staging system.
Thyroid cancer is best managed with a multidisciplinary, in-tegrated, and patient-centered approach. At Cleveland Clinic Florida, endocrinologists certified in ultrasound and radionu-clide administration, surgeons expert in endocrine surgery, oncologists, radiation oncologists, and interventional radi-ologists work together to ensure the patient receives only the most current and safest management. Treatment of well-differentiated thyroid cancer consists of partial or total thyroidectomy, nodal dissection when clinically indicated, iodine-131 administration, and thyrotropin (TSH) suppres-sion with thyroid hormone. There is controversy regarding whether total or partial thyroidectomy is performed. Propo-nents of lesser surgery argue that demonstration of a sur-vival advantage with total thyroidectomy in low-risk patients is difficult and the risk of permanent hyperparathyroidism (hypocalcemia) and recurrent laryngeal nerve injury is sig-nificantly higher than the reported two percent, particularly when surgery is performed by less experienced surgeons.
The rationale for total thyroidectomy includes improved abil-ity to use post-operative I-131 ablative therapy as well as lowering the dose required. It allows for monitoring of recur-rences with I-131 scans and serum thyroglobulin measure-ment. It removes multifocal disease, improves survival in subsets of patients, and decreases recurrence rates and the risk of developing the often fatal pulmonary metasta-ses. Finally, it also reduces the small risk of a differentiated cancer degenerating into one that is undifferentiated. Our endocrinologists and surgeons prefer total thyroidectomy for all patients with well-differentiated thyroid cancer at our institution.
Cleveland_Cancer Report_2010_FNL.indd 9 5/3/10 12:26 PM

10
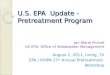
In 2008, Cleveland Clinic Florida surgeons performed the most total thyroidectomies of all the South Florida Hospitals.
For thyroid surgeries performed from 2004 through 2008, the average length of stay (ALOS), complications, and mortality for patients undergoing a unilateral thyroidectomy were 1.0 days, 0.0%, 0.0% comparing favorably to the accepted 1.2 days, 1.60%, and 0.10% values. The ALOS, complications, and mortality for patients undergoing a total thyroidectomy were 1.2 days, 1.7%, also comparing favorably to the accepted 1.3 days, 2.90%, and 0.10% values. (Compiled from the Solucient Hospital Database.)
Thyroid Cancer 2008 Data
These figures were compiled from the Solucient Hospital Database.
Cleveland_Cancer Report_2010_FNL.indd 10 5/3/10 12:26 PM

CANCER PROGRAM I STATISTICAL REPORT 2008 11
The long-tem prognosis for patients with differentiated thyroid cancer is generally favorable. Ten-year survival for patients with papillary or mixed papillary/follicular cancer is 92 percent and fol-licular cancer 72 percent. Tumor recurrence, however, may occur in up to 20 percent. By 2006, over 400,000 people in the United States were living with the diagnosis of thyroid cancer, a number that will continue to grow given the rising numbers of new cases and excellent prognosis. Life-long follow-up is essential.
Surveillance includes serum thyroglobulin determinations, whole-body scanning with I-131, and recently, because disease often first recurs in regional cervical lymph nodes, dedicated ultrasound of the neck. Specific ultrasound characteristics of metastatic lymph nodes and the use of ultrasound guided FNA of suspicious nodes for cytologic confirmation has authenticated the proce-dure’s usefulness. Over the past few years, the use of recombi-nant thyroglobulin stimulating hormone (rh TSH) has revolution-ized the management of thyroid cancer patients. No longer do patients need to discontinue their thyroid replacement hormones prior to surveillance testing thus avoiding periods of severe hy-pothyroidism and its associated symptoms. The technique also improves the sensitivity of serum thyroglobulin testing. The diag-nostic accuracy of serum thyroglobulin testing while remaining on replacement therapy is 36 percent with a false negative rate of 64 percent. RhTSH-stimulated levels > 2 ng/ml while the patient remains on replacement therapy has a sensitivity of 100 percent, a negative predictive value of 100 percent, and a false positive rate of only 9 percent.
Persistent or recurrent disease is treated by surgical resection, I-131 administration, or external beam radiotherapy. Very high cu-mulative doses of I-131 (1,000 mCi) have been associated with a small but significant increase in bladder and breast cancer. Acute myelogenous leukemia has also been reported.
Vineeth Mohan, MDDepartment of Endocrinology
Mark Sesto, MDDepartment of Surgery
References:1. Jemal A, Thomas A, Murray T, et al. Cancer statistics, 2002. CA Cancer J Clin 2002; 52: 23-47
2. McHenry CR. What’s new in general surgery: Endocrine surgery. J Am Coll Surg 2002; 195: 364
3. Gemsejager E, Perren A, Seifert B, et al. Lymph node surgery in papillary thyroid carcinoma. J Am Coll Surg 2002; 197: 182
4. Cobin RH, Gharib H. AACE/AAES medical/ surgical guidelines for clinical practice: Management of thyroid carcinoma. Endocrine practice 2001; 7: 202
5. Chen H, Nicol TL, Udelsman R. Follicular lesions of the thyroid: Does frozen section evaluation alter operative management? Ann Surg 1995; 222: 101
6. Mazzaferri EL, Kloos R. Is diagnostic iodine-131 scanning with recombinant human TSH useful in the follow-up of differentiated thyroid cancer after thyroid ablation? J Clin Endocrinol Metab 2002; 87: 1490-1498
Cleveland_Cancer Report_2010_FNL.indd 11 5/3/10 12:26 PM

2950 Cleveland Clinic Blvd. I Weston, FL 33331
Nonprofit
Organization
U.S. Postage
PAID
Ft. Lauderdale, FL
PERMIT NO. 4163
Cleveland Clinic, located in Weston and West Palm Beach, Florida,
is a not-for-profit, multi-specialty, academic medical center that
integrates clinical and hospital care with research and education.
Cleveland Clinic has nearly 170 physicians with expertise in 35
specialties. The medical campus is fully integrated and includes
diagnostic centers, outpatient surgery, and a 24-hour emergency
department located in the state-of-the-art hospital, which was
named one of the nation’s 100 Top Hospitals® in cardiovascular
care by Thomson Reuters in 2007 and 2008. Cleveland Clinic
Florida is 1 of only 13 hospitals in the nation recognized at the
Gold level by the American Heart Association for performance
in all three categories of the Get with the Guidelines program:
Coronary Artery Disease, Heart Failure & Stroke. Cleveland Clinic
Florida is an integral part of Cleveland Clinic in Ohio, where pro-
viding outstanding patient care is based upon the principles of
cooperation, compassion and innovation. Physicians at Cleveland
Clinic are experts in the treatment of complex conditions that are
difficult to diagnose. For more information about Cleveland Clinic
Florida, visit www.clevelandclinicflorida.org.
Cleveland_Cancer Report_2010_FNL.indd 12 5/3/10 12:26 PM