-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
1/48
Felicia Marie Knaul, PhDHarvard Global Equi ty I ni tiative,
Global Task F orce on Expanded Access to
Cancer Care and Control in LM ICs
Tmatelo a Pecho A:C. Mxico
Mexican Health F oundation
Bethesda,
January 14th, 2014
Cancer Prevention Fellowship Program
2013-2014 Cancer Prevention and
Control Colloquia SeriesNational Cancer Institute
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
2/48
Evidence-basedAdvocacy
Advocacy-inspired Evidence
Action:
projects, programs, policies
Duality:
evidence and advocacy
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
3/48
Harvard, Breast Cancer in Developing Countries, Nov 4, `09
Nobel Amartya Sen,Cancer survivor diagnosed in
India 60 years ago
Drew G. FaustPresident of Harvard
University 22+ year BCsurvivor
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
4/48
January, 2008
June, 2007
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
5/48
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
6/48
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
7/48
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
8/48
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
9/48
to evidence
From anecdote
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
10/48
Global Task Force on Expanded
Access to Cancer Care and
Control in Developing Countries
= global health + cancer care
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
11/48
Global Task Force on
Expanded Access to
Cancer Care and Control
35 members:
Global health + Cancer care
Technical Advisory Committee: 60+
Private Sector Engagement Group
Priority areas and Working groups: Ped Onc, Pain &
Palliation, Womens
cancers, Survivorship, Economics of cancer
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
12/48
Closing the Cancer Divide:An Equity Imperative
I: Shouldbe done
II: Could be doneIII: Can be done
M1. Unnecessary
M2. Unaffordable
M3. Impossible
M4: Inappropriate
Expanding access to cancer care and control in LMICs:
1: Innovative Delivery
2: Access: Affordable Meds, Vaccines & Techs3: Innovative
Financing: Domestic and Global
4: Evidence for Decision-Making
5: Stewardship and Leadership
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
13/48
#2 cause of death in wealthy countries
#3 in upper middle-income#4 in lower middle-income
and # 8 in low-income countriesMore than 85% of pediatric cancer
cases and 95% of
deaths occur in developing countries.
For children & adolescents
5-14 cancer is
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
14/48
Mirrors the epidemiological transition
LMICs increasingly face both infection-
associated cancers, and all other cancers.
The Cancer TransitionDouble burden for health systems
Cancers increasingly only of the poor, are
not the only cancers affecting the poor
LMICs account for >90% of cervical and 70%
of breast cancer deaths. Both are leading killers
especially of young - women.
C t iti i M i
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
15/48
Cancer transition in Mexico:
Breastand Cervicalmortality
0
4
8
12
16
1955 1990 2010Mortalityrateadjustedbyage
Oaxaca(Poorest)
Nuevo Len(Wealthiest)
Source: Knaul et al., 2008. Reproductive Health Matters, and
updated by Knaul, Arreola-Ornelas and Mndez.
0
10
20
30
1980 20100
10
20
1980 2010
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
16/48
Cancer is a disease of both rich and poor;
yet it is increasingly the poor who suffer:
1. Exposure to risk factors
2. Preventable cancers (infection)
3. Death and disability fromtreatable cancer
4. Stigma and discrimination
5. Avoidable pain and suffering
The Cancer Divide:
An Equity Imperative
Fac
ets
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
17/48
Adults
Leukaemia
All
cancers
Source: Knaul, Arreola, Mendez. estimates based on IARC,
Globocan, 2010.
Children
LOW
INCOM
HIGH
INCOME
Sur
vival
inequa
lity
gap
LOW
INCOM
HIGH
INCOME
100%
Facet 3: The Opportunity to Survive
(M/I) Should Not Be Defined by Income
In Canada, almost 90% of children with
leukemia survive.
In the poorest countries only 10% survive.
Russia
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
18/48
Non-methadone, Morphine
Equivalent opioid consumption perdeath from HIV or cancer in
pain:
Poorest 10%: 54 mg
Richest 10%: 97,400 mg
US/Canada: 270,000 mg
Latin America
N.America
Africa
Asia
injustice:
the pain divide
Data: http://www.treatthepain.com/methodology
Calculations: HGEI/FunsaludKnaul et al. Eds Closing the Cancer
Divide.
India
http://www.treatthepain.com/methodologyhttp://www.treatthepain.com/methodology
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
19/48
The night of my high school prom visiting my father,
Sigmund Knaul, at Mount Sinai Hospital, Toronto a fewweeks
before his death from cancer. May 1984.
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
20/48
Challenge and disprove the
myths about cancer
M1. Unnecessary
M2. UnaffordableM3. Inappropriate
M4: Impossible
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
21/48
The costs of inaction are huge:
Invest I NactionTobacco is a huge economic risk: 3.6% lower
GDP
Total economic cost of cancer, 2010: 2-4% of global GDP
Prevention and treatment offers
potential world savings of
$ US 130-940 billion
1/3-1/2 of cancer deaths are avoidable:2.4-3.7 million
deaths,
of which 80% are in LIMCs
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
22/48
The costs to close the cancer divide
are and may be less than many fear:
All but 3 of 29 LMIC priority cancer chemo and
hormonal agents are off-patent
Pain medication is cheap
Prices drop: HepB and HPV vaccines
Delivery & financing innovations are
underutilized & undeveloped so that purchasing
is fragmented and procurement is unstable
PAHO 2013 Strategic Fund for NCDs
includes key cancer drugs
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
23/48
Challenge and disprove the
myths about cancerM1. Unnecessary
M2. UnaffordableM3. InappropriateM4: Impossible
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
24/48
Women and mothers in LMICs
face many risks through the life cycle
Women 15-59, annual deathsDiabetes
120,889
Breast
cancer
166,577
Source: Estimates based on data from WHO: Global Health
Observatory, 2008 and Murray et al Lancet 2011.
Cervical
cancer
142,744
Mortality
in
childbirth
342,900
-35%in 30
year
= 430, 210 deaths
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
25/48
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
26/48
The Diagonal Approach to
Health System StrengtheningRather than focusing on either
disease-specific vertical orhorizontal-systemic programs, harness
synergies that
provide opportunities to tackle disease-specific priorities
while addressing systemic gaps and optimize available
resources
Diagonal strategies major benefits:X = > parts
Bridge disease divides using a life cycle response
avoids the false dilemmas between disease silos -
CD/NCD- that continue to plague global health
Generate positive externalities: e.g. womens cancer
programs fight gender discrimination; pain control 4all
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
27/48
Diagonal Strategies:
Positive Externalities
Promoting prevention and healthy lifestyles:
Reduce risk for cancer and other diseases
Reducing stigma for womens cancers:Contributes to reducing
gender discrimination.
Investing in treatment produces champions
Pain control and palliationReducing barriers to access is
essential for
cancer, for other diseases, and for surgery.
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
28/48
Applies a diagonal
approach to avoid
the false dilemmasbetween disease silos
-CD/NCD- thatcontinue to plague
global health
Closing the Cancer Divide:A BLUEPRINT TO EXPAND ACCESS IN
LMICs
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
29/48
Challenge and disprove the
myths about cancer
M1. Unnecessary
M2. UnaffordableM3. Inappropriate
M4: Impossible
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
30/48
Huge steps in the transition thru reform toward
Universal Health Coverage in many countries
Examples:
Brazil
China
Colombia
Chile
EEUU(Affordable Care Act)
El Salvador
Peru
South Af r ica
Taiwan
Mexico: Seguro Popular de Salud
Yetoften in thecontext of rapid,
profound,
polarized andcomplex
epidemiologicaltransition or
battlingfragmented health
systems
2003 REFORM: ELIMINATE SEGMENTATION IN ACCESS TO
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
31/48
2003 REFORM: ELIMINATE SEGMENTATION IN ACCESS TO
HEALTH INSURANCE BY GENERATING A SYSTEM FOR SOCIAL
PROTECTION IN HEALTH THAT INCLUDES PUBLICALLY
FUNDED HEALTH INSURANCE FOR FAMILIES EXCLUDED
FROM SOCIAL SECURITY
Social Security
Public and private,Formal sector workers
and their families:
Ministry of Health
with residual funding
Poor, informal sector,non-salaried, rural
areas:~50% ofpopulation
1943
2001/3: Pilot of PHI
2003: Law
Jan. 1, 2004: SSPH
2010: Universalcoverage of PHI
System for SocialProtection in Health
Seguro
Popular
Frenk et al., 2004.
R f 2003 d SPSS
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
32/48
Personal health
services
Public Health
Goods
Stewardship
Information, Research and
Development of Human
Resources
High specialty
interventions
Essential Health
Services
Fund for
personal health
services
Community Healthservices
FUNDS
SeguroPopu
lar
Fund for communityhealth services
MOH Budget
Fund for
catastrophic illness
Reform 2003 and SPSS:
New financial arquitecture
Source: (Frenk et al, 2006)
Fund for next
genderations
i i i C C
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
33/48
DiagonalizingCancer Care:
Financing & Delivery1. Financing: Integrate cancer care
into
national insurance and social security
programs2. Delivery: Harness platforms by integrating
breast and cervical cancer prevention, screening
and survivorship care into MCH, SRH,
HIV/AIDS, social welfare and anti-poverty
programs.
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
34/48
Mexicos 2003: major health reform
created Seguro Popular
Horizontal Coverage:
Beneficiaries
VerticalCoverage
Diseasesa
ndInterventions:
Benef
itsPackage
Affiliation: 2004: 6.5 m
2012: 54.6 m
Benefit package: 2004: 113
2012: 284+57
Evolution of vertical coverage:
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
35/48
Evolution of vertical coverage:
cumulative # of covered interventions,
2004-2012
Notes:
SP = Seguro Popular
MING = Medical Insurance for a New Generation (Children born
after December 1, 2006 and until they are 5 years of age)
FPCHE = Fung for Protection against Catastrophic Health
Expenditure
EPHS =Essential Personal Health Services
EPI = Expanded Programme of Immunisations
CBP= Community-based package
0
50
100
150
200
250
300
350
400
450
500
2004 2005 2006 2007 2008 2009 2010 2011 2012
63 65 65 65 65 65 65 65 65
6 6 8 6 12 1212 12 13
22
83
176 184189 189 198 198
206
6
6
1720
49 4949 57
57
110
108 116128
128131
MING
EPHS
EPI
CBP
FPCHE
Numberofinterv
entions
Seguro Popular
284 interventions
MING + SP
FPCHE
57interventions
CAUSES 91
FPCHE 6
CAUSES 284
FPCHE 57
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
36/48
Accelerated, universal, vertical coverage by disease
with an effective package of interventions
2004/6: HIV/AIDS, cervical cancer, ALL in
children
2007: All pediatric cancers; Breast cancer2011: Testicular and
Prostate cancer and NHL
2012: Ovarian (colorectal) cancer
Key aspect of Seguro Popular:
diagonal, financial protection for
catastrophic illness
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
37/48
Seguro Popular and cancer:
Evidence of impactBreast cancer adherence to treatment:
2005: 200/600
2010: 10/900
Since the incorporation of childhood
cancers into the Seguro Popular30-month survival: 30% to almost
70%
adherence to treatment: 70% to 95%.
The human faces of
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
38/48
The human faces of
Seguro Popular:
Guillermina Avila
&Abish Romero
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
39/48
Health System
Functions
Stage of Chronic Disease Life Cycle /components CCC
Primary
Prevention
Secondary
preventionDiagnosis Treatment
Survivorship/
Rehabilitation
Palliation/
End-of-life care
Stewardship
Financing
Delivery
Resource
Generation
Responding to the challenge of chronicity:
Health system functions
by care-control continuum
Effective financial coverage of a
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
40/48
Effective financial coverage of a
chronic disease: breast cancer
Mexico: Large and exemplary investment in financialprotection
for breast cancer prevention and treatment,
yet..a low survival rate.
Strengthen early detection, survivorship and palliation:
diagonalize delivery
Cancer Control-Care continuum
Primary
Prevention
Early
Detection Diagnosis Treatment Survivorship Palliation
Delivery and financial protection challenges:
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
41/48
Benefits:coveredin
terventions
Delivery and financial protection challenges:
Seguro Popular in Mexico
ACCELERATED VERTICAL COVERAGE for Catastrophic
Illnesses included in the Fund: breast cancer, AIDS
Community and Public Health Services
Poor Rich
CHILDREN: Health insurance for a New Generation
Package of essential personal
services
Beneficiaries
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
42/48
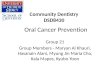
% diagnosed in Stage 4 by state# 2 killer of
women 30-54
5-10% detected
in Stage 0-1
Poor
municipalites:50% Stage 4; 5x
the rate for r ich
Breast Cancer: Delivery failure
Poor
RIch
i
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
43/48
Juanita:Advanced metastatic breast
cancer is the result of a series
of missed opportunities
Di li i D li 1
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
44/48
Diagonalizing Delivery 1:
Integration of cervical & breast cancer educati
into anti-poverty programs, Oportunidades
Include information in
manuales for communityworkers
1.5 million promoters
> 90% of poor Mexicanhouseholds: 5.8 million
families
Diagonalizing Delivery 2:
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
45/48
Diagonalizing Delivery 2:
Training primary care providers in
early detection of breast cancerPromoters (+4000), Nurses &
MDs (+1400)
medical students (+750)
Nuevo Leon, Jalisco, Morelos, PueblaSignificant increase in
knowledge, especially in CBE
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
46/48
The ?s that keep me up at night
and
worry me throughout the days:
1) Why has/should breast cancer become
such an emblematic and powerfulmessage?
1) Is it right or fair to advocate only on
behalf of ones own disease?
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
47/48
Be an
optimistoptimalist
-
8/13/2019 Cancer Prevention Fellowship Program 2013-2014 Cancer
Prevention and Control Colloquia Series National Cancer
Institute
48/48