Embed Size (px)
Citation preview

Cancer Pain Management
DR. PRADEEP JAIN
Sr. Consultant
Department of Anaesthesiology,
Pain & Perioperative Medicine
Sir Ganga Ram Hospital
New Delhi - 110 060

Global Crusade Against Pain
Chronic Pain is a Disease State

Pain Management A Team Approach
physician
NURSING
PHARMACY
SOCIALWORKER
SPIRITUALGUIDANCE
CASEMANAGER
DIETICIAN
PHYSICALREHAB

Pain Management
Children with cancer do not need to suffer
unrelieved pain
Effective pain management and palliative care are
major priorities of the WHO cancer programme,
together with primary prevention early detection &
treatment of curable cancers
Analgesic therapies are essential in controlling
pain and should be combined with appropriate
psychosocial, physical & supportive approaches

Pain in Cancer
In the developed world, the major
sources of pain in children’s are due to
diagnostic and therapeutic procedures.
In the developing world, most pain is
disease related

Why to Relieve Pain
CHILDREN Irritable, anxious & restless in response to pain
Develop mistrust & fear of hospitals, medical staff
and treatment procedures
Experience night terrors, flashbacks, sleep
disturbance and eating problem
Children with uncontrolled pain may feel victimized,
depressed, isolated ,lonely and their capacity to
cope with cancer treatment may be impaired

PATIENTS AND CLOSE RELATIVES
Distrustful towards the medical system
Experience depression & guilt about
being unable to prevent the pain
HEALTH CARE WORKERS
It numbs their compassion, creates guilt
Encourages denial that children are
suffering
Why to Relieve Pain

Management Strategies
Assess the child
Conduct physical examination
Determine primary cause of pain
Evaluates secondary causes
(environmental and internal )
Develop treatment plan
Analgesic drugs and non analgesic therapies
Implement Plan
Assess regularly and revise plan as necessary

• QUESTT
Q – Question the child
U – Use pain rating scales
E – Evaluate child’s behavior
S – Secure parent’s involvement
T – Take cause of pain into account
T – Take earliest action
Pain Assessment

Pain Assessment
PRE VERBAL
- Physiological changes
- Behavioral response –facial expression, body movement and type
of cry
PRE-SCHOOLERS
The various self-reporting scales are:
–The Oucher Scale
–Happy-Sad Face Scale
–Eland’s Colour Scale
–Poker Chip Tool
–Ladder Scale
–Linear Analogue Scale
SCHOOL AGED CHILDRENS
VAS and modified Mcgill Pain Questionnaire

Neonatal Pain Assessment Scale
Krecheal SW, Bildner J CRIES: a new neonatal postoperative
pain management score. Initial testing of validity and
reliability. Pediatric Anesthesia 1995;5:53-61

Pain Assessment Scales
The Wong Baker Scale
0
No Pain
10
Max. PainVAS

Approach to pain management
Flexibility is the key to managing cancer pain
Placebo should not be used in management of
cancer pain
Drug treatment is the main stay in cancer pain
management
Effective (70 - 80%)
Inexpensive

Non Opioid Drugs
• Mild to moderate pain
• Adjunct to balanced pain management
• Pharmacokinetics similar in infants aged over 6 months to adults
• Very little efficacy & safety data for infants available
• Paracetamol - tablet, syrup, suppositoriesdose 10-15mg/kg orally 6 hr
• Ibuprofen - tablet, syrupdose 10-20mg/kg orally 6 hr
• Diclofenac - orally 1mg/kg 8-12 hr
• Ketarolac - i/v 0.2-0.5 mg/kg

Morphine
Name derives from the Greek, Morpheus, the God of dreams, while opium is the Greek word for juice.
Oldest analgesic known to man Land mark in the development of
pain control Dried exudate of the opium poppy ‘’
papaver somini ferum”.

Guidelines for Analgesic Drug Therapy
“By the ladder”
“By the clock”
“By the appropriate route”
“By the child”

“By the ladder”

Morphine in Cancer Pain Management
“By the clock”
at fixed interval of time
dose titrated against the patients pain - gradually
increasing until the patient is comfortable
next dose before the effect of previous dose worn
off
prn means pain relief negligible
making patients earn their analgesia is as
unacceptable as making diabetic earn their insulin

Morphine in Cancer Pain Management
“By Mouth”
Treatment of choice
Tablets every 4 hourly
Slow release tablets
MST - 12 hourly
MXL - 24 hourly A simple aqueous solution of the sulfate or hydrochloride salt every 4 hours

Morphine in Cancer Pain Management
“By The Child ”
No standard doses.
No fixed upper dose limit (analgesic celing effect)
The “right” dose is the dose that relieves the pain
Range 5mg to >1000 mg

Morphine
Drug of choice
Oral, S/C, I/V, rectally, epidural and Intrathecal
Oral dose 0.15 –0.3mg/kg every 4 hour
Intermittent I/V 50-100 g /kg
Continuous I/V or S/C 15-30 g /kg/h
Controlled release oral preparation
< 6 months of age dose decrease to 1/3

Fentanyl
More potent then morphine
Hepato-renal compromise
< histamine release
Muscular rigidity
Only opioid with transdermal preparation
Oral Trans mucosal preparation
Sufentanyl nasal spray, Aerosol preparation

Pediatric Cancer Pain Management
Adjuvant drugs
May be necessary for one of the
three reasons:
To treat the adverse effects of
analgesic:
To enhance pain relief
To treat concomitant
psychological disturbances:

Intrathecal Drug Delivery
Morphine most commonly used
Epidural or Intrathecal administration
Epidural percutaneous catheter
Tunneled subcutaneous catheter

Procedure Related Pain General Principles
Prophylaxis should involve both pharmacological
and non pharmacological approaches
The specific approaches used should be tailored to
the individual
Children must be adequately prepared for all
invasive and diagnostic procedures
To be done in specially designated treatment
rooms

Algorithms for Pain Management During Procedures
PAINLESS PROCEDURE (CT, MRI)
Individualized preparation
chloral hydrate 1 hour before procedure
Pentobarbital
MILD PAINFUL PROCEDURE (I/V CANNULATION)
Parental presence
Local anaesthetics
– Topical anaesthetics
– Buffered lidocaine
Behavioural techniques e.g. bubble-blowing, distraction

Algorithms for Pain Management During Procedures
MODERATELY PAINFUL PROCEDURE (L.P.)
Benzodiazepines
SEVERE PAINFUL PROCEDURES (B.M
ASPIRATION, BIOPSY)
No venous access – oral midazolam with
morphine, I/M Ketamine
Venous access – midazolam with fantanyl,
morphine,Ketamine, propofol and N2O
GA

Oral Transmucosal Fentanyl
Sedation
100,200,300 ug
Dose:10-15ug/kg
Onset 20 mins
Nausea/vomiting common

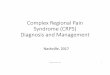
EMLA Application
1. Applying: Don’t rub the cream
2. Covering: Allow a thick layer
3. Timing: Let it be undistributed
4. Removing: 60 min after application
1.
4.
2.
3.

Nitrous Oxide Analgesia
Provide good analgesia, sedation and amnesia without resulting in loss of consciousness known as relative analgesia
Bone marrow aspiration, lumbar, puncture, venous cannulation and wound dressings
Administration– Demand system
(entonox )
– Constant flowdevices(quantiflex apparatus/ anaesthesia machine)

Programmable Electronic Devices
Programmable Electronic Devices
• Interfaced with microprocessorInterfaced with microprocessor
• Flexibility in programmingFlexibility in programming
• Comprehensive display & memory of eventsComprehensive display & memory of events
• Security features prevent temperingSecurity features prevent tempering
• Event logEvent log
• Multiple applicationMultiple application
• Interfaced with microprocessorInterfaced with microprocessor
• Flexibility in programmingFlexibility in programming
• Comprehensive display & memory of eventsComprehensive display & memory of events
• Security features prevent temperingSecurity features prevent tempering
• Event logEvent log
• Multiple applicationMultiple application

Disposable Fixed Programme DevicesDisposable Fixed Programme Devices
• Light weight - Maximum portabilityLight weight - Maximum portability
• Non Electronic - No programmingNon Electronic - No programming
• Hydrostatic positive pressure Elastomeric Hydrostatic positive pressure Elastomeric
energyenergy
• Flow restrictor - Flow rates are presetFlow restrictor - Flow rates are preset
• SimplicitySimplicity
• Minimal patient & nursing trainingMinimal patient & nursing training
• Light weight - Maximum portabilityLight weight - Maximum portability
• Non Electronic - No programmingNon Electronic - No programming
• Hydrostatic positive pressure Elastomeric Hydrostatic positive pressure Elastomeric
energyenergy
• Flow restrictor - Flow rates are presetFlow restrictor - Flow rates are preset
• SimplicitySimplicity
• Minimal patient & nursing trainingMinimal patient & nursing training

PEDIATRIC PO PAIN RELIEF
PCA
Morphine loding dose 50 g/ Kg
Infusion rate 15 g/ Kg/ hr
PCEA
Bupivicaine Bolus 0.5 ml/ Kg ( 0.25% )
Infusion rate - ( 0.125% ) 0.1 - 0.5 ml/ Kg / hr
Fentanyl 2 g/ ml + 0.125% Bupivicaine - 0.1 - 0.5 ml/ Kg / hr
Morphine 20 - 50 g/ Kg



Non Drug Pain Therapy
Supportive Support and empower the child
and family
Cognitive Influence thought
Behavioural Changes behaviour
Physical Affects sensory system
Integral Part of Cancer Pain Treatment

Freedom from pain should be
seen as a right of every cancer
patient and access to pain
therapy as a measure of
respect of this right
Cancer Pain

Conclusion
Nothing would have a greater impact on
the quality of life of children with cancer
than the dissemination and
implementation of the current principles
of palliative care, including pain relief &
symptom control

SGRH
Thank You….