Embed Size (px)
DESCRIPTION
Cancer Pain in Children. 13 th Annual Palliative Care Seminar Hector Rodriguez-Cortes, MD Pediatric Hematologist and Oncologist Pediatric Palliative Care and Hospice. Objectives:. Epidemiology of cancer pain Identify the three different pain categories - PowerPoint PPT Presentation
Citation preview
Cancer Pain in Children
13th Annual Palliative Care SeminarHector Rodriguez-Cortes, MD
Pediatric Hematologist and OncologistPediatric Palliative Care and Hospice
Objectives:Epidemiology of cancer pain
Identify the three different pain categories
Identify Treatment and Tumor-Related pain syndromes
Review the Two-step strategy of the WHO guideline
Introduction Cancer:
evokes immediate fear for patients and their families
potentially fatal diseasecan be associated with pain
Symptoms:may be interconnectedtreatment of one symptom may exacerbate
another
FREQUENCY OF CANCER PAIN
Multi-factorial:type of malignanciessites of involvementpresence or absence of metastases
Prevalence of moderate/severe painincreases during the late phases of
malignancy
EPIDEMIOLOGY OF CANCER PAIN IN CHILDREN
Cancer pain: tumor-related treatment-related pattern: surgery, medications
Tumor-related pain: predominates at diagnosis/ early treatment phase May persisted for a median of 10 days after initiation of
treatment.
Examples of tumor-related pain: Brain tumors:
headache/ abnormal neurologic signs Mets w spinal cord compression: back pain
EPIDEMIOLOGY OF CANCER PAIN IN CHILDREN
Treatment-related pain: mucositisantineoplastic therapypostoperative painprocedure-related pain

Breakthrough pain in Children with Cancer
Freidrichsdorf and Postier (2014)Breakthrough Pain Questionnaire for Children
57% of children experienced painPain: major tumor tumor surgery >> tumor/ drug-
relatedYounger children (7-12 year of age) at higher risk
than teenagersPCA

Reason for Breakthrough pain in Children with Cancer
Freidrichsdorf and Postier (2014)
disease progression
infection at the tumor site
development of tolerance
drug interactions
decreasing renal function
somatization and psychological distress.

Pain Mechanisms

PAIN MECHANISMS:Experience of pain:
Subjectivecan be modulated by developmental, familial,
situational, emotional, and other factors. lack of correlation between the extent of tissue
injury and the intensity of pain or suffering.
PAIN MECHANISMS: Terminology
Nociception:sensation of tissue injury or inflammationalerts an individual to potential or ongoing injuryprompts the avoidance or limitation of further injurycan be activated by:
chemical, thermal, or mechanical stimuli lack of it can lead to a variety of medical complications
decubitus ulcers.

Nociception

Somatic pain: Pathophysiology
1. noxious stimuli mechanical,
thermal, or chemical 2. Pain signals are carried
to the dorsal horn of the spinal cord by: A-delta fibers:
mechanical/thermal C fibers: all three
stimulus types3. The signals ascend in
the contralateral spinothalamic and spinoreticular tracts
4. thalamus
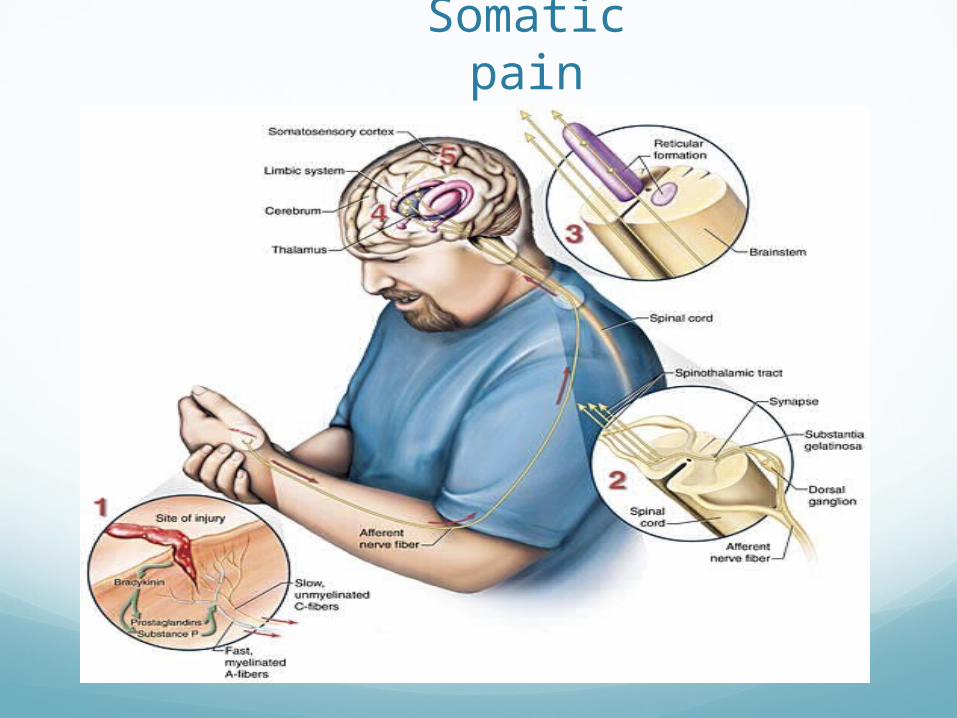
Somatic pain

TYPES OF PAINPain can be divided into 3 categories:
SomaticVisceralNeuropathic
These categories are not mutually exclusive since a patient's pain may have multiple etiologies.

Somatic painTriggered by potential or real injury to tissues
cutaneous burn or an arthritic joint.Pain
tender and localized.constant and sometimes throbbing or aching.it can be acute or chronic.
Bone metastasis is the most common cause of somatic pain

Visceral pain Mechanism is not well characterized.
Pain: Poorly localized less constant it can dull, colicky
Often referred to a distant cutaneous site. diaphragmatic irritation: ipsilateral shoulder passage of a renal stone
Associated: nausea and diaphoresis.
Noxious stimuli that can trigger visceral pain: ischemia, inflammation, torsion, traction, distension, or impaction

Visceral pain

Neuropathic pain Causes:
Peripheral or central in etiology infiltration of neural structures by tumor
fibrosis: radiation injury: surgery
Described as: prolonged, severe, burning, or squeezing It can paroxystic often associated with focal neurologic deficits relatively resistance to opioids
Often associated with symptoms and signs of autonomic instability ( i.e.., tachycardia, sweating)
Example: herniated intervertebral disc, phantom limb pain, degenerative neuropathies such as Guillain-Barre syndrome.

Neuropathic pain Clinical features:
Dysesthesias: abnormal or unfamiliar unpleasant sensations
Allodynia:an exaggerated response to otherwise non-noxious
stimuli, such as light touch of the skin
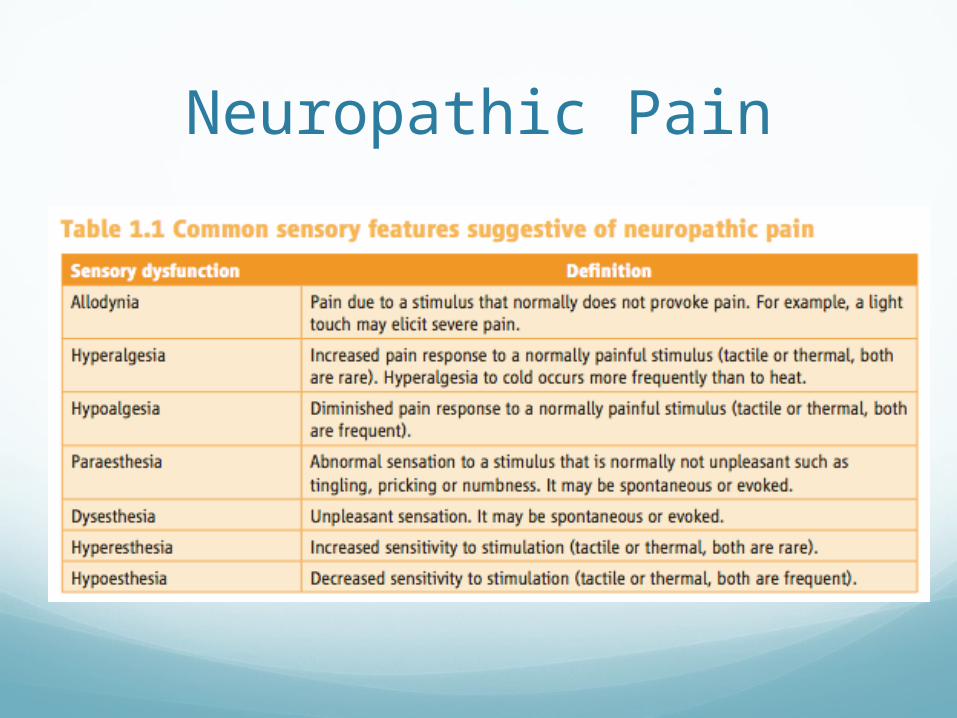
Neuropathic Pain

Neuropathic pain

Pain Assessment

Measuring PainPain:
often under-recognized in cancer patients should be assessed frequently and systematically
Principal barrier to effective pain management: discrepancy between the patient's and physician's
assessments of the pain
Anxiety and depression: may exacerbate, rather than exaggerate, the pain.

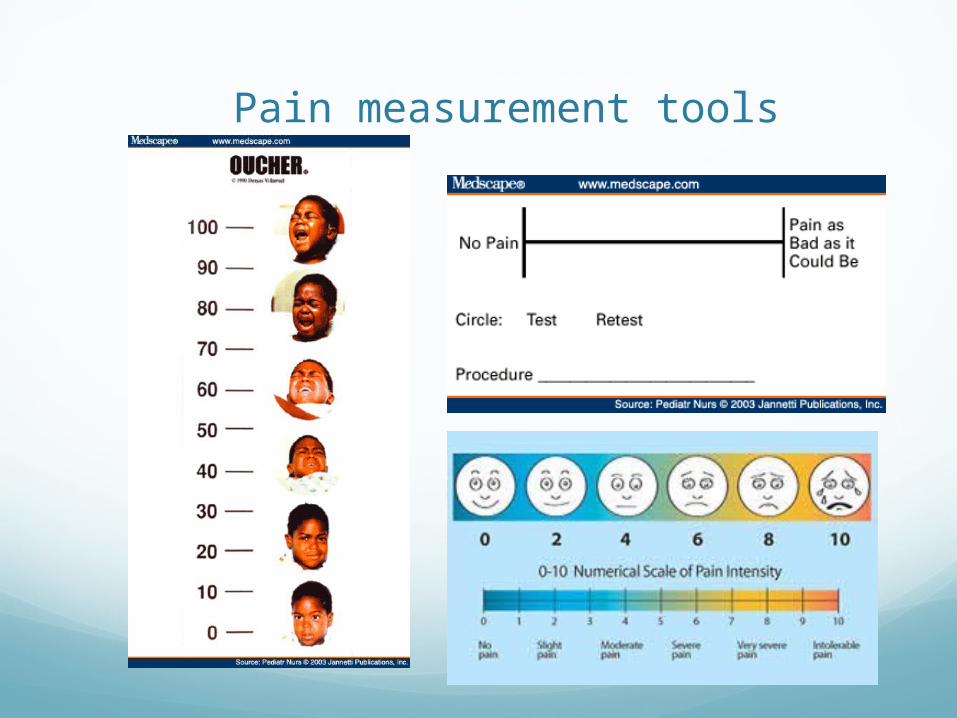
Pain measurement toolsVerbal numerical scale
rating pain from zero for "no pain," to 10 for "the worst imaginable pain"
easily implemented and recorded
10 cm visual analog scale:used, with or without intensity descriptors do not reflect the complexity of the pain
experience
Pain measurement toolsNon-communicate pain:
intensity must be evaluated by other means.nonverbal signs of pain
These include:hypertension, tachycardia, and diaphoresis Agitation or confusionApathy, inactivity, or irritability in patients with
cognitive impairment
Pain measurement tools

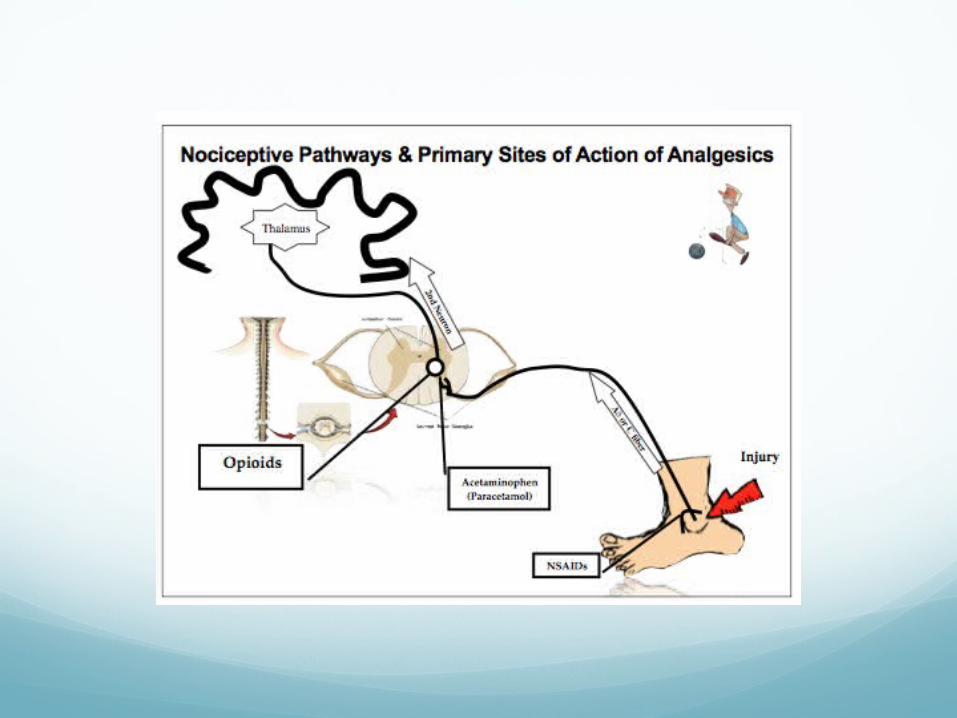
Pain Management
Principles for the pharmacological management of pain.
WHO: 1986dosing at regular intervalsusing the appropriate route of administration adapting treatment to the individual child
WHO: 2012using a two-step strategy
Principles for the pharmacological management of pain.
WHO: 1986dosing at regular intervals
steady blood level: reducing peaks and troughsusing the appropriate route of administration
Least invasive route (often chosen by the child)Transdermal patches: long onset time
adapting treatment to the individual childFrequently assessment, reassessment and
modification
Principles for the pharmacological management of pain.
WHO: 1986
WHO: 2012: two-step strategychoice depends on the child’s level of pain.
MildModerate to severe pain

Three-step vs. Two-step approach
Difference: three-step analgesic ladder:
use of codeine as a weak opioidtreatment of moderate pain
two-step approach: low doses of strong opioid
Two-step: more effective strategy for persisting pain.

The First Step: mild painRecommendations:
Paracetamol and ibuprofenchoice for first step (mild pain) widely available in child-appropriate dosage forms
oral liquidsrelatively inexpensive
ANALGESIC MEDICATIONS: Non-opioids Acetaminophen:
inhibits prostaglandin synthesis
lacks the sedative effects minimal anti-inflammatory
effect no side effects such as
gastritis and inhibition of platelet
Aspirin and NSAIDs in cancer patients: risk for bleeding
Aspirin: irreversible inhibition of
platelet
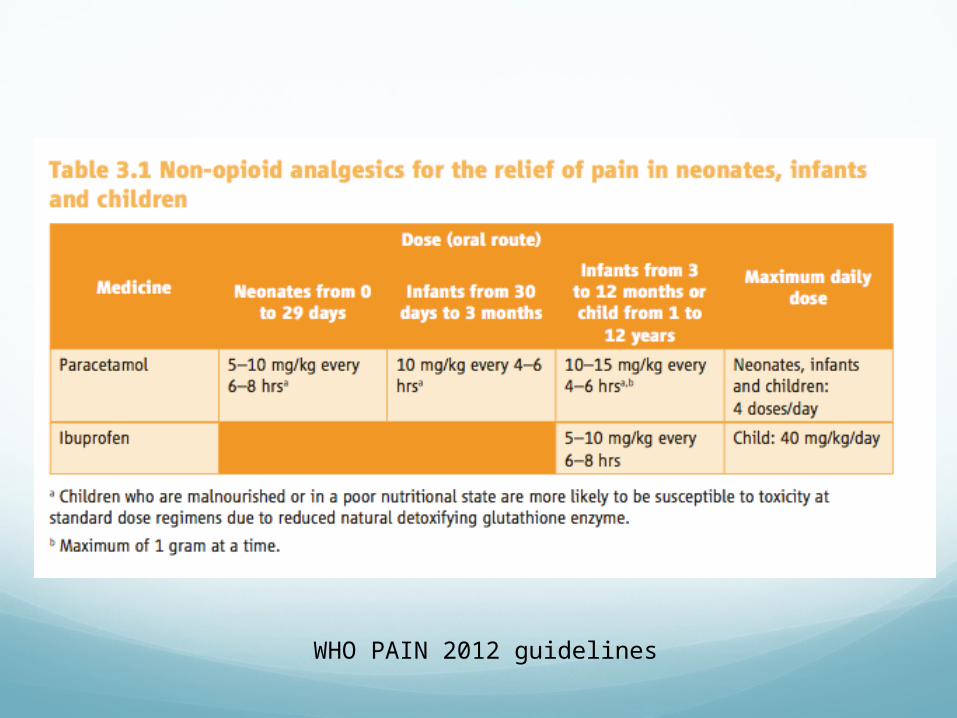
WHO PAIN 2012 guidelines

The Second Step: Moderate to Severe pain
Recommendations:
Morphinedrug of choiceother strong opioids
intolerable side-effects.
Administer opioid analgesics in the first step:clinical judgementcareful considerations of the disability caused
by pain

Strong Opioids Morphine:
first choice metabolize in the liver widely used
It can be administered: oral, rectal, IV, SQ, epidural, intrathecal, or
intraventricular
Starting dose for immediate-release oral morphine 0.1 mg/kg q4 hours.
Very young infants should receive a reduced dose due delayed clearance

Strong Opioids:Hydromorphone:
oral, IV, SQ, epidural, and intrathecal used if there are dose-limiting side effects
from morphine. 5-8 times as potent as morphine.
Fentanyl:transdermal, oral transmucosal, and IV50-100 times more potent than morphinevery rapid onset: high lipid solubility shorter duration of action after IV
administration: used in patients with dose-limiting side
effects: pruritus

Strong Opioids:Meperidine
no advantages over morphine major drawback: can cause dysphoria, excitation, and
convulsions, particularly in patients with impaired renal clearance
Methadone synthetic opioid that has a prolonged duration of action its potency is similar to morphine. convenient as a long-acting medication in patients who are
unable to swallow slow-release morphine tablets
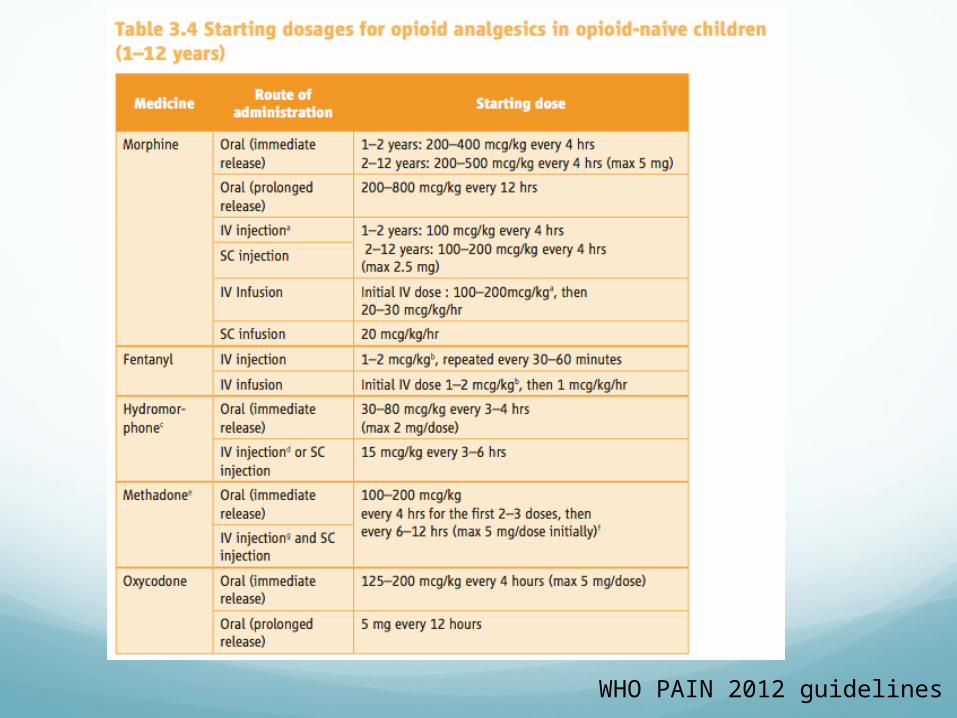
WHO PAIN 2012 guidelines


TramadolCentrally acting analgesic with opioid effects
Control of moderate to moderately severe pain
Food does not affect its rate of absorption
Dosing:17 years of age and over:
Starting dose: 25 mg/day q AM and titrated in 25 mg increments as separate doses every 3 days to reach 100 mg/day (25 mg q.i.d.).
may be increased by 50 mg as tolerated every 3 days to reach 200 mg/day (50 mg q.i.d.).
How supplied: 50 mg tab

Codeine Excluded for pain relief from the two-steps
Codeine
“weak” opioid
widely available
previously recommended to control moderate pain.
well-known safety but efficacy problemsgenetic variability in biotransformation.
Codeine:prodrug
enzyme CYP2D6:converted into its active metabolite morphine.
efficacy depends on the amount of active metabolite.
variable expressions of the enzymes inter-individual and inter-ethnic differences Fetus: absent or less than 1% Children less < 5 year: 25% of the adult values
Excluded medicine for pain relief:
Codeine Poor metabolizers:
vary in ethnic groups from 1% to 30% ineffectiveness
Rapid metabolizer: metabolize codeine quickly and extensivelyrisk of severe opioid toxicity,
high and uncontrolled conversion into morphine.

SYNDROMES OF PEDIATRIC CANCER PAIN
Treatment-Related Syndromes
Tumor-Related Syndromes

Treatment-Related Syndromes: Mucositis
Optimal management is not well established.
S/P BMT: more intense and
prolonged that chemotherapy-related.
Therapy: topical therapies: sodium
bicarbonate, hydrogen peroxide, nystatin, viscous lidocaine, dyclonine,
systemic therapies: opioids and systemic antifungal agents.

Treatment-Related Syndromes: Graft-Versus-Host Disease
May be associated with severe abdominal pain.
GVHD is the next most common cause of pain after an allogeneic BMT
Pain due to GVHD frequently requires the administration of opioids

Treatment-Related Syndromes: Phantom Limb Pain
Common among children after amputation of an extremity
Incidence/severity decrease with time after amputation
Prior treatment with chemo increased the risk after subsequent amputation.
Therapy: tricyclic anti-depressants opioids seen to be ineffective early and frequent use of a limb
prosthesis may reduce the duration and severity
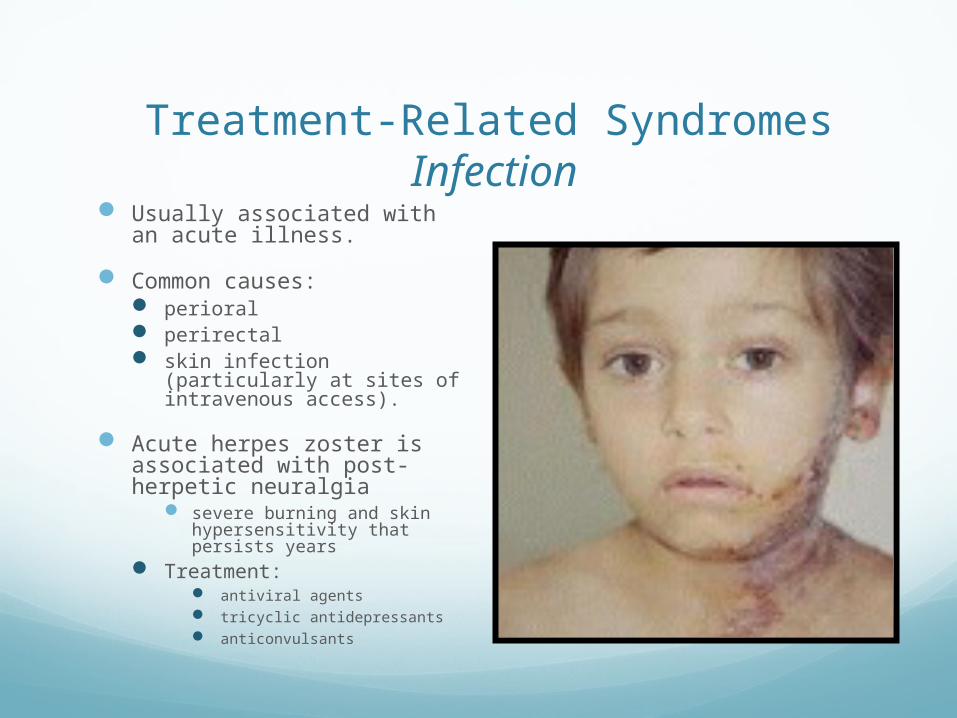
Treatment-Related Syndromes Infection
Usually associated with an acute illness.
Common causes: perioral perirectal skin infection (particularly at
sites of intravenous access).
Acute herpes zoster is associated with post-herpetic neuralgia
severe burning and skin hypersensitivity that persists years
Treatment: antiviral agents tricyclic antidepressants anticonvulsants

Treatment-Related Syndromes Antineoplastic Therapy—Related Pain
Peripheral venous injection: thrombophlebitis associated with local pain leucovorin, thiotepa
Intrathecal chemotherapy: arachnoiditis and meningeal irritation
syndrome (i.e., headache, nuchal rigidity; fever, nausea, and vomiting).
Chemotherapy: Vesicants:
local necrosis Irritants:
burning or inflammation without necrosis.
painful vincristine neuropathy.

Treatment-Related Syndromes Procedure—Related Pain
Needle Puncture: major source of distress must be adequately
prepared before their first needle puncture to minimize their fear and anxiety.
Topical treatments: local anesthetics: EMLA skin cooling and EMLA can
produce vasoconstriction, which may occasionally make venous cannulation more difficult.

Lumbar PunctureBone Marrow Aspiration
Lumbar puncture: puncture of the skin by the
spinal needle or by contact with bone
Spinal headache: cerebrospinal fluid leak. (epidural blood patch)
BMA/Bx: needle through the periosteum suctioning of the marrow
Treatment: EMLA or other topical conscious sedation:
Propofol

Tumor-Related SyndromesTumor commonly causes pain from involvement:
Bone: Somatic pain Viscera: Visceral pain Nerves: Neuropathic pain
Bone metastases: cause pain by stimulation of nerve endings in the
endosteum by the destroyed bone tissue periosteum is more sensitive than bone marrow and
cortex

BONE PAIN Tumor involvement of bone is the most common
cause of cancer pain
Type of tumors: Neuroblastoma, ostesarcoma, Ewing sarcoma: Breast, lung, prostate, and multiple myeloma:
high incident of bone metastatic cancer
Common sites: Vertebral, skull, humerus, ribs, pelvis, and femur.
Pain due to bone metastases has an important negative impact on quality of life

Bone Pain:Pathophysiology
Caused by imbalance between bone formation (mediated by osteoblasts) and resorption, which is mediated by osteoclasts.
Purely somatic unless a pathologic fracture or tumor extension disrupts a nerve.
Avascular necrosis steroid treatment
Osteoradionecrosis may develop months or years after irradiation.
Pseudorheumatism may result from the rapid withdrawal of corticosteroids reinstitution of steroid treatment followed by slow
withdrawal confirms the diagnosis by relieving the arthralgias and myalgias

Bone PainDiagnosis
Plain x-rays may show lytic or blastic lesions. CT scan may further define the morphology
Bone scans: more sensitive than plain x-ray, but may be negative
with purely osteolytic lesions
MRI: less sensitive than x-ray or CT for cortical bone
destruction may show marrow edema and soft tissue extension

Bone Pain: lesion

BACK PAIN Cancer:
<1 percent of back pain But 98% of known cancer patients who present with back pain will have
evidences of metastases.
Thoracic spine, is the most common site of bony metastasis
Symptoms: High cervical spine: posterior headache (? tension headache) C7 to T1 refer to the interscapular region T12 or L1: refer pain to the flank, iliac crest, or sacroiliac joint Sacral destruction: saddle distribution
Loss of motor function, hyperreflexia or hyporeflexia, or bowel or bladder dysfunction are suggestive of myelopathy. prompt immediate intervention
BACK PAINDiagnostic evaluation:
Plain radiographs will detect appx.70 % MRI or CT/myelography should be added if plain films
are normal and there is a high suspicion of tumor.
Bone scan: appropriate when suspicion of tumor is low and the X-
ray is normal sensitivity of bone scan is high, especially for
osteoblastic lesions and fracture.
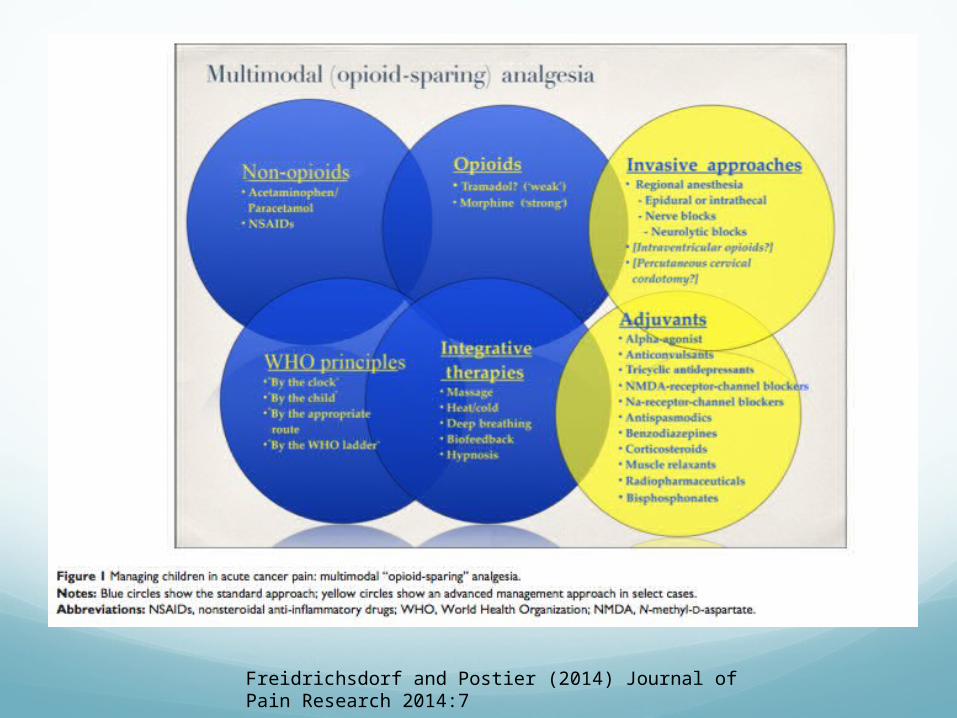
Freidrichsdorf and Postier (2014) Journal of Pain Research 2014:7

References Overview of cancer pain, Z.H Bajwa, C. A. Warfield,UpToDate: July
17, 2007
Cancer pain syndromes, Z.H Bajwa, C. A. Warfield,UpToDate: July 17, 2007
Pain Assessment and Management in Infants With Cancer, Bonnie Stevens, PhD* Pediatr Blood Cancer 2007;49:1097—1101
Symptom Management in Supportive Care; P.A. Pizzo, D. Poplack, Principles and Practice of Pediatric Oncology , 4th edition
WHO guidelines on the pharmacological treatment of persisting pain in children with medical illnesses 2012.
Freidrichsdorf and Postier (2014), Management of breakthrough pain in children with cancer, Journal of Pain Research 2014:7 117-123